

SUMMARY
Between 1992 and 2004, a total of 49 819 confirmed hepatitis C infections have been reported to the Health Protection Agency (HPA) by laboratories in England and Wales; the annual number of reports increased from 241 in 1991 to 8149 in 2004. Most reports with a known risk factor were in injecting drug users (87%, 12 438/14 221), but 71% (35 598/49 819) of the total had no reported identified risk. The age-sex distribution of the latter cases was similar to that in injecting drug users. Using names to assign ethnicity, individuals with South Asian names had an older age distribution and a different risk factor profile from non-South Asians. Using published age-specific prevalence data from 1996, it was estimated that around 281 764 cases of hepatitis C infection exist in England and Wales, and that only 17% of these cases have been reported to the HPA. Surveillance reports continue to provide important information regarding trends in hepatitis C infection in specific risk groups.
INTRODUCTION
Over recent years, hepatitis C virus (HCV) infection has emerged as a major public health problem, and is now known to be a major cause of chronic hepatitis [1]. Chronic complications of hepatitis C infection include cirrhosis, liver failure and primary liver cancer [2].
The World Health Organization (WHO) estimates that there are 170 million persons chronically infected with HCV worldwide with an estimated global prevalence of 3%. A marked variation in prevalence exists between countries [3]. In most developed countries the prevalence of anti-HCV ranges between 0·4% and 2%. Higher prevalence levels have been seen in parts of Eastern Europe and in Africa. Egypt has one of the highest levels reported, with between 20% and 25% of both urban and rural populations being infected [4].
Acute symptomatic hepatitis C infection is rare and ∼80% of individuals who acquire the virus become chronically infected [5]. An undetermined proportion of chronic infections are asymptomatic [6]. Transmission of the virus occurs most effectively via injecting drug use and by the transfusion of contaminated blood or blood products [7]. Universal screening of blood donors, viral inactivation of blood products and improvements in infection control measures have significantly decreased exposure to the virus. In most developed countries infection is now largely confined to high-risk groups such as injecting drug users (IDUs) [6, 8], where the prevalence of HCV infection ranges from 30% to 98% [9–17]. In the United Kingdom, groups where the prevalence of HCV has been found to be low include antenatal women [18, 19] organ donors [20] and genitourinary medicine clinic attendees [21].
Surveillance of hepatitis C in England and Wales began in the early 1990s. The aim of this surveillance is to monitor trends in incidence and prevalence, to determine the major risk factors associated with infection in England and Wales, and to inform health-care planning, prevention and control strategies.
This paper describes the features of confirmed cases of hepatitis C infection reported to the Health Protection Agency (HPA) between 1992 and 2004 by laboratories in England and Wales.
METHODS
Reports of laboratory-confirmed hepatitis C infections from the national surveillance system were analysed. Since 1990, HCV testing has been performed in around 300 public health and NHS laboratories in England and Wales.
A laboratory case is confirmed by the detection of antibody to hepatitis C virus (anti-HCV) or HCV RNA in serum. Current available laboratory assays are unable to differentiate between acute and chronic hepatitis C infection.
Since the second half of 1990, a number of laboratories in England and Wales have reported confirmed cases of HCV infections to the Public Health Laboratory Service, Communicable Disease Surveillance Centre (now part of the Health Protection Agency) using a surveillance form or an electronic reporting system [22]. The form allows for the collection of demographic details, risk factors for infection and information on whether the infection was acquired overseas. Evidence for an acute infection or seroconversion is also requested. Reports received electronically include minimal risk factor information.
Reported names are held temporarily on the laboratory surveillance database in agreement with guidance on confidential patient information [23]. Ethnicity is not reported through the routine laboratory surveillance system. ‘Nam Pehchan’ software was used to assign South Asian ethnicity based on the names that were present on the database [24]. Statistical significance was measured using χ2 or Kruskal–Wallis tests as appropriate.
Age-specific estimates of the burden of disease were obtained by applying 1996 published age-specific prevalence data [25] to 2003 age-specific mid-year resident population estimates for England and Wales (Office for National Statistics) [26]. Laboratory reports were adjusted to reflect age in 2004 (for example a 26-year-old with a laboratory report in 1992 will be 38 years old in 2004 and hence in the 35–44 years age group) and compared to the age-specific estimated burden.
RESULTS
A total of 49 819 confirmed cases of hepatitis C infection were reported to the HPA between 1992 and 2004. The cumulative totals when plotted indicated an increase year on year (Fig. 1).
Fig. 1.

Cumulative reports of HCV infection 1992–2004.
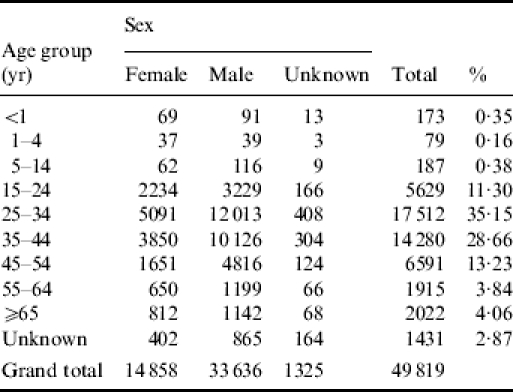
Of the cumulative total, 67·5% (33 636/49 819) of these infections occurred in males. Females accounted for 29·8% (14 858/49 819) of infections, while gender was not reported in 2·7% (1325/49 819) of the reports. The ratio of HCV infection between males and females was 2·3:1. The majority, 63·8% (31 792/49 819), of infections were described in those aged between 25 and 44 years (Table 1). A total of 439 cases of hepatitis C infection were reported in children aged <15 years throughout this period, of these, 173 were in infants aged <1 year. Of these 173, only 70 were reported as being HCV RNA positive.
Table 1.
Laboratory-confirmed reports of hepatitis C infection, England and Wales: 1992–2004 by age and sex
Information relating to risk factor was present in 28·5% (14 221/49 819) of the reports received. The most commonly reported risk factor for infection was injecting drug use accounting for 87·5% of those with a reported risk (Table 2). The male to female ratio of IDUs was 2·8:1 (8997 males, 3231 females), and the majority of cases were reported in the 25–44 years age group (72·2%, 8982/12 438). Being institutionalized (largely in prison) was reported in 3·6% (509/14 221) of cases without any other exposure history. Of the 303 (2·1%) reports attributed to blood transfusion, 26 cases had reported acquiring infection abroad. Thirty seven per cent (87/234) of the reports specifying sexual exposure were sexual contacts of known HCV-positive individuals and 10 had partners who were reported as IDUs. Vertical transmission accounted for 45 (0·3%) reports with risk factor information and of these, only 15 had HCV RNA detected. Other reported settings or routes of transmission included; acquiring infection in a household setting, 0·25% (35/14 221); or having an organ or tissue transplant, 0·22% (31/14 221). A total of 19 cases reported acquiring their infection occupationally. Of these, six were health-care workers, only two of whom had acquired their infection via documented needle-stick injuries.
Table 2.
Risk factor distribution by South Asian and non-South Asian name
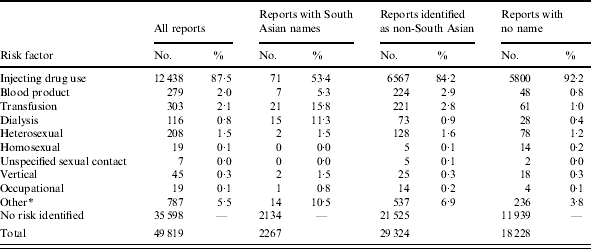
% represents the percentage of reports with risk factor information.
Being institutionalized (largely in prison) was reported in 509/787 of cases in the ‘other’ exposure category.
In children aged <15 years, 24·1% (106/439) of reports had risk factor information. The main routes of acquisition in this group were: vertical transmission 42·4% (45/106); being in receipt of blood products 21·7% (23/106); receiving a transfusion 14·2% (15/106) and injecting drug use 10·4% (11/106). In those children without risk factor information, 9·3% (31/333) had information that one or both parents were IDUs. Of those children aged <1 year, 26·6% (46/173) had information on risk factors. Of these, the majority (35/46) had acquired their infection through vertical transmission, followed by familial transmission (5/46). Of those without a named route of transmission, 17·3% (22/127) had information that one or both parents were IDUs.
A total of 35 598 (71·5%) reports did not have any risk factor information; the male to female ratio was 2·1:1 (23 384 males, 11 127 females). The majority of these cases 61·4% (21 843/35 598) were aged between 25 and 44 years and the age distribution was fairly similar to that amongst IDUs.
Reports were received from all regions in England and Wales. The highest rates were observed in the North West and South West regions (12·5 and 11·8/100 000 respectively) (Table 3). The proportion of reports with risk factor information varied by region, with the South West and South East regions having the greatest proportion of reports with risk factor information (46·6% and 45·1% respectively), and the North West and West Midlands regions reporting the lowest proportion (13·1% and 13·6% respectively). Of reports with a known risk factor, the proportion where the route of transmission specified injecting drug use was high in all regions, ranging from 72% to 94%.
Table 3.
Reports of HCV infection by region and year
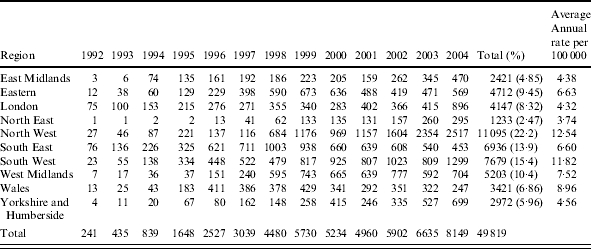
Calculated using 2003 mid-year population estimates.
Data on acute cases and seroconversions has been collected since 1996 and 1997 respectively, however, the information is rarely reported. A total of 364 individuals had a documented hepatitis C seroconversion or acute infection. Of these, 212 had risk factor information, the majority of these were IDUs (89·6%, 190/212), Heterosexual exposure accounted for 2·4% (5/212), followed by being in receipt of a blood transfusion 1·4% (3/212), however, there is no information about whether the infection was acquired abroad.
During this 13-year period, 295 individuals reported that their infection was acquired abroad. Of these cases, 82·2% (243/295) reported the country where the infection was acquired. The most commonly reported countries were: Pakistan 10·2% (25/243), Italy 9·9% (24/243), and Spain 7·8% (19/243). Of those individuals who had acquired their infection abroad and who had a reported risk factor, injecting drug use (48·1%, 52/108) was the most frequently reported risk, followed by transfusion (24·1%, 26/108), heterosexual exposure (7·4%, 8/108) and being in receipt of blood products (4·6%, 5/108).
Approximately two thirds (31 591/49 819) of laboratory reports had a name recorded. Of these, 7·2% (2267/31 591) were of South Asian origin, the majority of which were identified as having names of Moslem religious and Urdu linguistic origin (57·1%, 1294/2267). The male to female ratio was 1·59:1 (males 1285, females 809). The distribution of ages in the South Asian ethnic group were skewed towards the older age groups (Fig. 2) and were found to significantly differ from that of the non South Asians (Kruskal–Wallis test P<0·001). Ninety-four per cent (2134/2267) of reports in South Asians lacked any risk factor information (Table 2). However, of those reports with risk information, the most commonly reported risk factor was injecting drug use (53·4%, 71/133), followed by receiving a transfusion (15·8%, 21/133); having dialysis (11·3%, 15/133); and being in receipt of blood products (5·3%, 7/133) (Table 2). The proportion of these reports with risk factor information that were acquired though injecting drug use was significantly lower than in the non-South Asians (P<0·001).
Fig. 2.

Age distribution of HCV reports by age and ethnicity. ——, South Asian; , no name; ····▴····, non-South Asian; – –◆– – , total.
, no name; ····▴····, non-South Asian; – –◆– – , total.
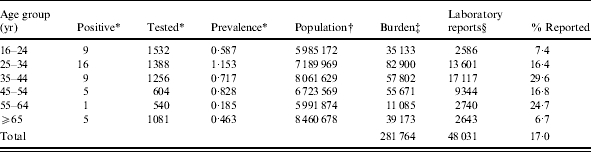
Based on population prevalence data from 1996 [25] and mid-year 2003 population estimates, [26] it was estimated that around 281 764 hepatitis C cases exist in adults (aged ⩾16 years) in England and Wales. The population prevalence data is based on testing of residual sera submitted to 16 laboratories in England and Wales for diagnostic tests. A comparison with the cumulative number of reports received in this age group since 1992, suggests that only 17% (48 031/281 764) of cases have been reported (Table 4).
Table 4.
Estimated age-specific numbers of chronic infections and proportion of cases reported England and Wales by 2004
DISCUSSION
The number of laboratory reports of hepatitis C infection has increased annually since testing commenced. This is probably mainly due to changes in testing and reporting rather than an increase in the incidence of hepatitis C infection. It is assumed that most of the infections identified by surveillance are prevalent infections acquired at some time in the past. Laboratory reports of HCV reflect current laboratory testing patterns rather than the incidence of infection. Acute infections or seroconversions would be expected to be a better reflection of incidence, but the number of such infections identified and reported is small. The age and sex distributions observed were consistent with those previously reported [22]. The majority of infections are confined to individuals aged between 25 and 44 years and injecting drug use is the most common risk factor associated with infection. Other risks such as being in receipt of blood products or in receipt of a transfusion are much less common. Although a substantial proportion of reports are received without attached risk factor information, the age-sex profile of these cases suggests that many of these may also be occurring in IDUs. This emphasizes the importance of IDUs in the transmission of hepatitis C. Studies in IDUs have yielded different estimates of the prevalence of HCV infection [9–13]. Sharing of blood-contaminated injecting paraphernalia has been shown to contribute to the spread of the infection [27], and cross-sectional surveys have shown that the prevalence of hepatitis C increases with increasing number of years of injecting, which is likely to reflect cumulative exposure [12, 28]. Studies of IDUs conducted in Europe, New Zealand, Australia and the United States have found anti-HCV prevalence to be >50%, increasing to 80% after 2–3 years of injecting [12, 28], and that infection is acquired rapidly after initiation of injecting [28]. England and Wales has a relatively low prevalence of hepatitis C infection in IDUs compared to other developed countries [29]. Harm reduction interventions throughout the 1980s and 1990s aimed at IDUs, has contributed to the lower prevalence of HCV infection amongst this group in England and Wales compared to other industrialized countries [17].
The results indicate that trends both between and within regions varied considerably over time. Differences between regions are difficult to interpret as they may reflect different levels of testing and/or reporting. The largest number of reports were received from the North West region. There was variability in the reporting of risk factor by region with the North West and West Midlands reporting the smallest proportion of reports with risk factor information, although the proportion of reports mentioning injecting drug use as the route of transmission exceeded 80% in most regions.
Laboratory reports of hepatitis C infection in children are rare; the majority of children having acquired the infection as a result of vertical transmission. In children aged <1 year, maternal anti-HCV will be present and so vertical transmission can only be confirmed by the detection of HCV RNA. The estimated risk of mother-to-infant transmission is <6% [30–32], and this may explain why RNA detection was only reported in 40% of children aged <1 year over the period.
Prior to the introduction of viral inactivation of blood products (1985), and the screening of blood donors (1991), some recipients of blood and blood products were inadvertently infected. The risk of HCV infectious donations entering the blood supply in England has decreased since 1993, and is currently estimated to be 1 in 30 million as a result of testing all donations for HCV RNA [33]. These interventions have greatly reduced the risk of hepatitis C being acquired by such routes in the United Kingdom and is reflected by the small proportion of reports with transfusion as a route of transmission. Transfusion may still represent a significant risk in developing countries or countries where donor screening has not been routinely implemented.
Although the risk of transmission following a single percutaneous exposure from a hepatitis C antibody-positive source is estimated to be 1·8% (0–7%), health-care workers are at increased risk of HCV infection compared with the general population [34]. Only six of the 19 occupationally acquired infections were in health-care workers, only two of which were detected following documented needle-stick injuries. Current guidelines recommend that all source patients (subject to appropriate consent) should be tested for evidence of hepatitis C infection and follow-up testing conducted in the health-care worker [35]. The HPA is currently undertaking the active surveillance of documented needle-stick injuries to health-care workers. Since 1997, as part of this surveillance scheme, nine seroconversions following percutaneous exposure to a HCV-positive source patient have been documented [36].
One of the main limitations of the use of routine surveillance data is the large proportion of reports without any risk factor information. For the majority of infections, the date of acquisition is not known and the diagnosis is often made late in the course of the disease. Exposure to the virus may have occurred many years in the past, making the probable route of acquisition difficult to assign. Enhanced surveillance of hepatitis C was piloted in seven laboratories in England and Wales [37]. Detailed clinical and epidemiological information was obtained from the requesting clinician or general practitioner (GP). This sentinel laboratory-based surveillance demonstrated that most risk factors could in fact be identified and information on acquisition risk was available for 86% of reports. This suggests that the large proportion of reports with no risk factor information is due to the fact that they are not reported by the clinician/GP who requests the hepatitis C test from the laboratory, rather than because they are truly unknown.
Of the reports with names, 7·2% were found to be of South Asian origin. Based on the 2001 census, ∼4·0% of the England and Wales population are from an Indian, Pakistani or Bangladeshi ethnic group [38] suggesting that individuals of this ethnic origin may be at higher risk of infection. The older age distribution and the lower proportion of cases with known risk factors observed in individuals with South Asian names is interesting. One possible explanation is that individuals who acquired infection in their country of origin many years ago are now presenting with chronic liver disease and being tested. Failure to collect information on ethnicity in routine surveillance data could be masking important risk factors or inequality of access to preventive or health-care services. Studies to determine the prevalence of infection in ethnic minority groups may lead to better tailoring of prevention programmes and treatment services.
Based on published prevalence data we estimated that around 281 764 anti-HCV-positive adults in England and Wales have been exposed to the virus. This estimate is based on testing of residual sera submitted to 16 laboratories for diagnostic tests and may not be truly reflective of the general population prevalence. Despite this, we believe that a substantial proportion of hepatitis C infections have not been diagnosed and reported to the HPA. The level of under-reporting to national surveillance is not known, but the low rate of reports from London, where prevalence is expected to be highest and where the proportion of IDUs who report being tested [39] is amongst the highest, suggests that under-reporting is a major problem in London. Assuming that reporting is not influenced by age, our estimates suggest that older infected individuals are less likely to be identified than younger individuals and that more effort is required to identify ex-IDUs who may be infected. The Hepatitis C Action Plan for England was recently published, setting out proposals to raise awareness about hepatitis C amongst the general population [29]. It aims to increase HCV testing, to strengthen prevention activities in IDUs and to identify persons already infected with hepatitis C so they can be managed effectively. Laboratory reports of confirmed hepatitis C infection are likely to continue to increase further in the next few years as a result of these initiatives.
The data clearly indicate that the burden of infection is greatest in IDUs. Since the infection is often sub-clinical [40] and many individuals are likely to be unaware of their condition, this may be contributing to ongoing transmission in populations, particularly in IDUs. Since a vaccine to prevent HCV infection does not yet exist, the greatest impact is most likely to be achieved by sustaining and improving efforts on primary prevention strategies in IDUs. Laboratory surveillance continues to provide important information regarding trends of hepatitis C infection in specific groups.
ACKNOWLEDGEMENTS
We thank Mrs Anjna Mistry for managing the surveillance databases and also the laboratory staff who contribute to the national surveillance of hepatitis C. We also thank Mr Nick Andrews for reading the manuscript and for his statistical advice.
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Di Bisceglie AM et al. Long-term clinical and histopathological follow-up of chronic posttransfusion hepatitis. Hepatology. 1991;14:969–974. doi: 10.1016/0270-9139(91)90113-a. [DOI] [PubMed] [Google Scholar]
- 2.Alter H. Natural History and clinical aspects of hepatitis C virus infection. Antiviral Therapy. 1996;1:15–20. [Google Scholar]
- 3.Anon. Hepatitis C: global update. Weekly Epidemiology Record. 1997;72:341–344. [Google Scholar]
- 4.Alter MJ. Epidemiology of hepatitis C in the West. Seminars in Liver Disease. 1995;15:5–14. doi: 10.1055/s-2007-1007259. [DOI] [PubMed] [Google Scholar]
- 5.Gish RG, Lau JYN. Hepatitis C virus: eight years old. Viral Hepatitis Review. 1997;3:17–37. [Google Scholar]
- 6.Anon. Global surveillance and control of hepatitis C. Journal of Viral Hepatitis. 1999;6:35–47. [PubMed] [Google Scholar]
- 7.MacDonald M, Crofts N, Kaldor J. Transmission of hepatitis C virus: rates, routes and cofactors. Epidemiology Review. 1996;18:137–148. doi: 10.1093/oxfordjournals.epirev.a017921. [DOI] [PubMed] [Google Scholar]
- 8.Koretz RL, Stone O, Gitnick GL. The long-term course of non-A, non-B post transfusion hepatitis. Gastroenterology. 1980;79:898. [PubMed] [Google Scholar]
- 9.Van den Hoek JAR et al. Prevalence incidence and risk factors for hepatitis C infection among drug users in Amsterdam. Journal of Infectious Disease. 1990;162:823–826. doi: 10.1093/infdis/162.4.823. [DOI] [PubMed] [Google Scholar]
- 10.Donahue JG et al. Antibody to hepatitis C virus among cardiac surgery, homosexual men and intravenous drug users in Baltimore, Maryland. American Journal of Epidemiology. 1991;134:1206–1211. doi: 10.1093/oxfordjournals.aje.a116023. [DOI] [PubMed] [Google Scholar]
- 11.Guadagnino V et al. Anti-hepatitis C antibody prevalence among intravenous drug addicts in the Catanzaro area. Archives of Virology. 1992;4:335–336. doi: 10.1007/978-3-7091-5633-9_78. [DOI] [PubMed] [Google Scholar]
- 12.Garfein RS et al. Viral infections in short-term injection drug users: the prevalence of the hepatitis C, hepatitis B, human deficiency and human T-lymphotropic viruses. American Journal of Public Health. 1996;86:655–661. doi: 10.2105/ajph.86.5.655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Memon MI, Memon MA. Hepatitis C: an epidemiological review. Journal of Viral Hepatitis. 2002;9:84–100. doi: 10.1046/j.1365-2893.2002.00329.x. [DOI] [PubMed] [Google Scholar]
- 14.Majid A et al. Molecular epidemiology of hepatitis C virus infection amongst intravenous drug users in rural communities. Journal of Medical Virology. 1995;46:48–51. doi: 10.1002/jmv.1890460111. [DOI] [PubMed] [Google Scholar]
- 15.Serfaty MA et al. Risk factors and medical follow-up of drug users tested for hepatitis C – can the risk of transmission be reduced? Drug and Alcohol Review. 1997;16:339–347. doi: 10.1080/09595239700186721. [DOI] [PubMed] [Google Scholar]
- 16.Lamden KM et al. Hepatitis B and hepatitis C infections: risk factors among drug users in Northwest England. Journal of Infection. 1998;17:260–269. doi: 10.1016/s0163-4453(98)92045-x. [DOI] [PubMed] [Google Scholar]
- 17.Hope VD et al. Prevalence of Hepatitis C among injection drug users in England and Wales: is harm reduction working? American Journal of Public Health. 2001;91:38–42. doi: 10.2105/ajph.91.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Balogun MA et al. The prevalence and genetic diversity of hepatitis C infection in antenatal clinic attenders in two regions of England. Epidemiology and Infection. 2000;125:705–712. doi: 10.1017/s0950268800004696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ward C et al. Prevalence of hepatitis C among pregnant women attending an inner London obstetric department: uptake and acceptability of named antenatal testing. Gut. 2000;47:165–166. doi: 10.1136/gut.47.2.277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wreghitt TG et al. Transmission of hepatitis C virus by organ transplantation in the United Kingdom. Journal of Hepatology. 1994;20:768–772. doi: 10.1016/s0168-8278(05)80148-5. [DOI] [PubMed] [Google Scholar]
- 21.Balogun MA et al. A national survey of genitourinary medicine clinic attenders provides little evidence of sexual transmission of hepatitis C virus infection. Sexually Transmitted Infections. 2003;79:301–306. doi: 10.1136/sti.79.4.301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ramsay ME et al. Laboratory surveillance of hepatitis C virus infection in England and Wales: 1992–1996. Communicable Disease and Public Health. 1998;1:89–94. [PubMed] [Google Scholar]
- 23.Department of Health. http?//www.dh.gov.uk/PolicyAndGuidance/InformationPolicy/PatientConfidentialityAndCaldicottGuardians/fs/en http?//www.dh.gov.uk/PolicyAndGuidance/InformationPolicy/PatientConfidentialityAndCaldicottGuardians/fs/en
- 24.Harding S, Dews H, Simpson SL. The potential to identify South Asians using a computerized algorithm to classify names. Population Trends. 1999;97:46–49. [PubMed] [Google Scholar]
- 25.Balogun MA et al. The prevalence of Hepatitis C in England and Wales. Journal of Infection. 2002;45:219–226. doi: 10.1053/jinf.2002.1059. [DOI] [PubMed] [Google Scholar]
- 26.ONS. UK: Office for National Statistics; 2003. [Google Scholar]
- 27.Hagan H et al. Sharing of Drug Preparation Equipment as a Risk Factor for Hepatitis C. American Journal of Public Health. 2001;91:42–46. doi: 10.2105/ajph.91.1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Di Bisceglie AM. Hepatitis C. Lancet. 1998;351:351–355. doi: 10.1016/S0140-6736(97)07361-3. [DOI] [PubMed] [Google Scholar]
- 29.Department of Health. Hepatitis C Action Plan for England. London: Department of Health; 2004. [Google Scholar]
- 30.Anon. The scientific challenge of hepatitis C. Science. 1999;285:26–30. doi: 10.1126/science.285.5424.26. [DOI] [PubMed] [Google Scholar]
- 31.European Association for the Study of the Liver. International consensus conference on hepatitis C. Journal of Hepatology. 1999;30:956–961. [PubMed] [Google Scholar]
- 32.Yeung LTF, King SM, Roberts EA. Mother to infant transmission of hepatitis C virus. Hepatology. 2001;34:223–229. doi: 10.1053/jhep.2001.25885. [DOI] [PubMed] [Google Scholar]
- 33.Soldan K et al. Estimation of the risk of hepatitis B virus, hepatitis C virus and human immunodeficiency virus infectious donations entering the blood supply in England, 1993–2001. Vox Sanguinis. 2003;84:274–286. doi: 10.1046/j.1423-0410.2003.00296.x. [DOI] [PubMed] [Google Scholar]
- 34.CDC. Recommendations for follow-up of health-care workers after occupational exposure to hepatitis C virus. Morbidity and Mortality Weekly Report. 1997;46:603–606. [PubMed] [Google Scholar]
- 35.Ramsay ME. Guidance on the investigation and management of occupational exposure to hepatitis C. Communicable Disease and Public Health. 1999;2:258. [PubMed] [Google Scholar]
- 36.Health Protection Agency. Centre for Infections; England and Wales and Northern Ireland: 2005. [Google Scholar]
- 37.Balogun MA et al. Risk factors, clinical features and genotype distribution of diagnosed hepatitis C virus infections: a pilot for a sentinel laboratory-based surveillance. Communicable Disease and Public Health. 2003;6:34–39. [PubMed] [Google Scholar]
- 38.Office for National Statistics; General Register Office for Scotland; Northern Ireland Statistics and Research Agency. 2001. http://www.statistics.gov.uk/STATBASE/Expodata/Spreadsheets/D7666.xls http://www.statistics.gov.uk/STATBASE/Expodata/Spreadsheets/D7666.xls
- 39.Health Protection Agency. London: Health Protection Agency; 2004. [Google Scholar]
- 40.Harris HE et al. Clinical course of hepatitis C virus during the first decade of infection. British Medical Journal. 2002;324:1–5. doi: 10.1136/bmj.324.7335.450. [DOI] [PMC free article] [PubMed] [Google Scholar]