

SUMMARY
Lack of access to safe water and sanitation contributes to diarrhoea moribidity and mortality in developing countries. We evaluated the impact of household water treatment, latrines, shallow wells, and rainwater harvesting on diarrhoea incidence in rural Kenyan children. We compared diarrhoea rates in 960 children aged <5 years in 556 households in 12 randomly selected intervention villages and six randomly selected comparison villages during weekly home visits over an 8-week period. On multivariate analysis, chlorinating stored water [relative risk (RR) 0·44, 95% confidence interval (CI) 0·28–0·69], latrine presence (RR 0·71, 95% CI 0·54–0·92), rainwater use (RR 0·70, 95% CI 0·52–0·95), and living in an intervention village (RR 0·31, 95% CI 0·23–0·41), were independently associated with lower diarrhoea risk. Diarrhoea risk was higher among shallow well users (RR 1·78, 95% CI 1·12–2·83). Chlorinating stored water, latrines, and rainwater use all decreased diarrhoea risk; combined interventions may have increased health impact.
INTRODUCTION
There is a strong association between poverty and lack of access to safe water and sanitation [1]. The World Health Organization (WHO) estimates that over one billion people worldwide lack access to improved water supplies [2]. Many millions more rely on water sources that, although improved, are still contaminated, or are located outside the home, necessitating transport and storage before use, which frequently results in faecal contamination [3, 4]. Consumption of faecally contaminated water is an important route of transmission for enteric pathogens [5]. The consequence of the lack of water and sanitary infrastructure in the developing world is a high burden of diarrhoeal diseases, which result in about two million deaths per year [6].
In 2000, the UN established a Millennium Development Goal (MDG) for Water to halve the proportion of the world's population without access to safe water by 2015. Achievement of the MDG for Water will require the provision of access to safe water to 300 000 persons per day, every day, by 2015 [7], but will still leave hundreds of millions of people exposed to unsafe water sources. In sub-Saharan Africa, the MDG for Water will probably not be met [8]. It is clear that inexpensive, innovative solutions to the problem of safe water are needed for the short to medium term.
To address the need for safe water, the Centers for Disease Control and Prevention (CDC) and the Pan American Health Organization/WHO developed a simple, inexpensive, household-based strategy, called the Safe Water System (SWS) with three components: point-of-use water disinfection using locally produced sodium hypochlorite solution; safe water storage; and behaviour change techniques [9]. Field trials have shown that use of the SWS reduces the risk of diarrhoea by 25-85% [10–14].
In October 1999, we implemented the SWS in collaboration with CARE Kenya in a programme that also provided latrines and improved water supplies, including shallow wells and rainwater collection, in rural western Kenya [15]. To determine the impact of the SWS, latrines, and improved water supplies on diarrhoea incidence in children aged <5 years, we conducted an evaluation of this programme from March to May 2001.
METHODS
Setting
CARE Kenya's Water, Sanitation, and Education for Health (WASEH) programme promoted latrine building, rainwater collection, and shallow well construction in 72 rural villages with a population of 45 000 people in Nyanza Province, Kenya. These communities are populated mainly by members of the Luo tribe, whose livelihoods depend on fishing and subsistence farming. Household compounds are dispersed, typically located ⩾100 m from the nearest neighbour. The SWS project was incorporated into the WASEH programme because in many communities ground water was contaminated, too deep to access, or too salty to drink.
Study design
Because the WASEH programme involved the implementation of a public health intervention using community-wide implementation strategies, the only feasible approach to evaluating the health impact was through a quasi-experimental design. For the evaluation, WASEH villages included communities that could, and others that could not, access ground water to determine whether access to ground water would be a factor that might influence acceptance of the SWS. For a comparison group, we selected nearby villages that were participating in a sustainable agricultural project that did not have a water and sanitation component. These villages are culturally and linguistically similar to WASEH villages.
To measure the health impact of the SWS and other interventions we conducted weekly active diarrhoea surveillance for a period of 8 weeks from March to May 2001, which coincided with the rainy season.
Sample selection
The median number of households per village in this region was about 90. We calculated that 12 intervention villages and six comparison villages would be adequate to detect a ⩾30% difference in diarrhoea incidence in children aged <5 years, assuming that children aged <5 years resided in 50% of households and had a weekly diarrhoea incidence rate of 12% (a conservative estimate based on previous surveys). We estimated a 25% dropout rate, and aimed for a confidence level of 95%; we added 20% to the sample size to account for a design effect. Using a random numbers table, we selected an intervention group of six (27%) of 22 WASEH project villages without access to ground water and six (12%) of 50 WASEH villages with probable access to ground water, and a comparison group of six (10%) of 60 neighbouring villages in the sustainable agriculture project.
SWS intervention elements
Water disinfection solution
A commercial bleach producer (Jet Chemicals, Nairobi, Kenya) prepared a 1·0% sodium hypochlorite solution for the project, packaged it in 500-ml containers with an 8-ml screw cap that doubled as a dosing device, and labelled the bottles with the brand name, Klorin, and dosing instructions in Luo (the local language) and pictograms. One bottle of Klorin was sufficient to treat 1250 l, enough to last a family of six for 2 months. Community health workers sold Klorin in project villages for 45 Kenya shillings (US$ 0·33) per bottle (slightly more than the cost of four single-use bags of laundry detergent), which covered the cost of production of each bottle, plus enough to provide health workers a small commission from each sale as an incentive; promotion, distribution, and evaluation costs were not recovered.
Storage containers
Because the local population had strong aesthetic and cultural preferences for clay pots, we had a local pottery collective produce clay pots (hereafter referred to as modified clay pots) for safe storage that included a spigot, narrow mouth, and fitted ceramic lid [16]. The collective produced 20-l and 40-l pots which community health workers sold for US$2.40 and US$ 2.90, respectively, keeping a small commission for each sale as an incentive. We also promoted locally available 20-l plastic jerry cans as a low-cost, alternative safe water storage vessel.
Behaviour change techniques
We implemented the project with a two-stage community mobilization approach. We first oriented local government officials, community management committees, and leaders of women's groups to the project to gain their support, and then trained community volunteers to use participatory hygiene and sanitation transformation (PHAST) methodology [17] to promote the SWS, hygiene, and sanitation in community meetings, community management committees, and during home visits.
From August 2000 to May 2001, we also implemented a social marketing campaign to promote the SWS in WASEH programme villages and to commercialize the products, with the aim of economic sustainability [15]. Social marketing activities included: (1) focus groups to develop a brand name (Klorin) and logo; (2) demonstrations of the SWS by project staff at area markets; and (3) promotional activities including street theatre, puppet shows, and a district-wide soccer tournament during which the SWS was advertised.
WASEH programme elements
Latrines
WASEH promoted latrines with cement sanitary platforms (‘sanplat’) and ventilated improved pit (VIP) latrines, each of which was lined with cement trapezoidal blocks and had a superstructure made of bricks or tree branches. Communities were taught about the link between sanitation and health and were offered the opportunity to participate in the programme. Interested persons were provided training in manufacture of cement platforms and blocks, and construction of both types of latrine. The programme paid for 40% of latrine costs and community members paid 60% of costs and provided the labour.
Shallow wells
All wells were dug by hand with a diameter of 1 m and a depth of 15–30 m. All were reinforced with concrete rings and were fitted with Afridev hand pumps (http://www.arihantdeepwellpumps.com/afridev.html) for lifting water.
Rainwater harvesting
Although rainwater harvesting was promoted, particularly in communities lacking accessible ground water, no specific technologies were used. While some households had masonry collection tanks, most set out all available collection vessels, such as buckets and barrels, whenever it rained.
PHAST
During the implementation of the SWS in intervention communities, we also used PHAST methodology to train community volunteers in comparison villages to promote improved hygiene, using the same material as the WASEH programme, but leaving out the SWS content. After the conclusion of the evaluation, we implemented the SWS in the comparison villages according to a pre-existing plan.
Baseline data
Although the WASEH programme was already in progress at the time of the introduction of the SWS component of the project, before implementing the SWS we conducted a survey to determine ‘baseline’ conditions at the time of our intervention. We systematically selected 50% of households in the 12 intervention and six comparison villages, using a random rotating start in each village. To determine baseline demographic characteristics, sanitary conditions, drinking water handling and storage practices, and ownership of common household items, we developed a questionnaire that was translated into Luo and administered in March 2000. To estimate socio-economic status, we assigned the median market price in Kenyan shillings to each household item reported in the baseline survey, summed the value of all household items, and converted the value to US$ using a conversion factor of 72 Kenyan shillings per US$.
Follow-up data
At the onset of the long rains, in late March 2001, we established a system of active diarrhoea surveillance among all children aged <5 years in the 12 intervention and six comparison villages. During weekly household visits over 8 weeks, interviewers obtained reports of the occurrence of diarrhoea (defined as ⩾3 loose stools in a 24-h period) from caregivers, including onset and recovery dates, in resident children over the preceding 7 days. At each visit, the interviewers determined the current water source; assessed the drinking water storage vessel type and latrine status through direct observation; and verified sodium hypochlorite use by measurement of detectable (>0·1 mg/l) free chlorine levels in stored water using the N,N-diethyl-phenylenediamine (DPD) colorimetric method (Free and Total Chlorine kit; Hach Co., Loveland, CO, USA).
Statistical analysis
Statistical analysis was performed using SAS version 8.0 (SAS Institute Inc., Cary, NC, USA). Diarrhoea episodes reported on consecutive visits were counted as one episode unless a beginning and resolution date were reported and there were >2 diarrhoea-free days between episodes. To assess the quality of active diarrhoea surveillance data, we performed an exploratory outlier analysis of diarrhoea incidence among children by village to determine whether outcome measures from any given village differed substantially from the results of aggregated data. To assess the association between diarrhoea and confirmed use of Klorin solution (defined as the presence of free chlorine residuals in stored water), presence of a household latrine, water source, type of storage container, and demographic covariables, we constructed generalized linear models using generalized estimating equations to control for intra- and inter-personal correlation between outcomes. To account for the effect of use and non-use of different water and sanitation interventions, we performed analyses comparing diarrhoea predictors between intervention and comparison households, and between using and non-using households in intervention villages. To examine the effect of covariables on associations between the use of interventions and disease, we performed a subset analysis linking baseline demographic and socioeconomic data to the SWS evaluation, excluding households that had moved away or in which children had reached 5 years of age or died.
Ethical review
The Institutional Review Board (IRB) of the Centers for Disease Control and Prevention determined that, because this work represented programme evaluation of a proven public health practice and disease surveillance, IRB regulations did not apply. Nevertheless, written informed consent was obtained from each participant head of household, and confidentiality was assured by maintaining data collection forms in a locked cabinet and irreversibly removing personal identifiers from databases.
RESULTS
Baseline
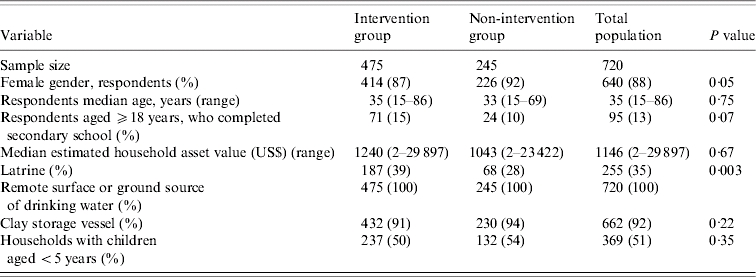
The 50% sample selected for the baseline survey included 720 households; no household refused to participate. The median age of respondents was 35 years (range 15–69); 640 (88%) were female (see Table 1). Among 626 respondents aged ⩾18 years, 95 (13%) had completed secondary school. The median estimated household asset value was US$1146 (range 2–29 897); there was no difference between intervention and comparison villages. All 720 households retrieved drinking water from a remote surface (river or pond) or ground water (borehole or shallow well) source and stored water in the home; 92% stored their drinking water in a traditional, wide-mouthed clay vessel. Latrines were present in 39% of intervention households and 28% of comparison households (P=0·003). Children aged <5 years resided in 369 (51%) households; the age distribution of children was similar between intervention and comparison groups.
Table 1.
Selected baseline demographic characteristics, water handling, and storage practices of households by intervention group
Follow-up
For the follow-up evaluation, we included all households in intervention and comparison villages with children aged <5 years. By exploratory outlier analysis, diarrhoea incidence among children in two intervention villages was significantly lower than in the other 10 villages in the intervention group. On subsequent investigation, there was a strong suspicion that data were being fabricated by two enumerators and these two villages were excluded from further analysis; including results from these two villages in the analysis would have overestimated the protective effect of the interventions. A total of 366 households in 10 intervention villages and 189 households in six comparison villages, with 618 and 342 children aged <5 years, respectively, were included in the analysis of data from the active diarrhoea surveillance system. The median age of children was 30 months (range 1–59 months) in intervention and comparison villages at the initiation of active surveillance. The median number of completed visits per household during the 8-week surveillance period was eight (range 1–8) in both groups of villages.
During weekly household visits, households in intervention villages more frequently reported that their primary water source was a shallow well, borehole, or rainwater than comparison households (Table 2). Intervention households more frequently reported using improved storage containers than comparison households; the vast majority of households in both groups used traditional clay pots (Table 2). Intervention households were also more likely to have residual chlorine in their stored water (43% of visits vs. 0%, P=undefined) and to possess a latrine (49% of visits vs. 27%, P<0·001).
Table 2.
Number of households with children aged <5 years, and water/sanitation conditions at the time of prospective diarrhoea surveillance at childrens' households
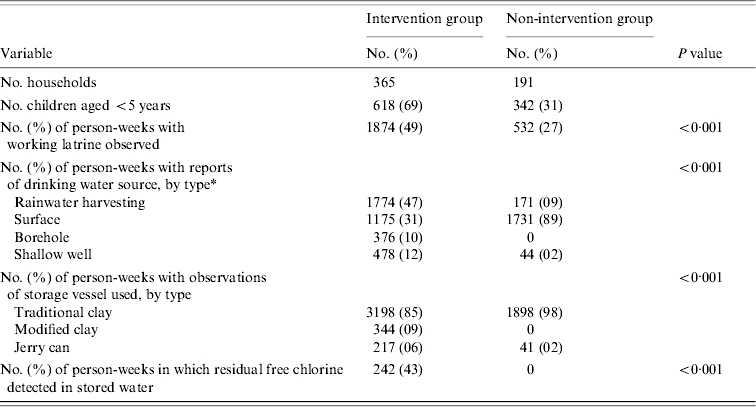
Surface water includes lake, river and dam water.
Over the 8-week follow-up period, at least one household case of diarrhoea in children aged <5 years was reported by intervention group respondents during 131 (8·0%) of 1643 home visits, and by comparison group respondents during 302 (22·6%) of 1336 visits. The crude household diarrhoea rate in intervention households was 65% lower than in comparison households.
On multivariate analysis, living in an intervention village household [relative risk (RR) 0·31, 95% CI 0·23–0·41], use of Klorin (RR 0·44, 95% CI 0·28–0·69), presence of a latrine (RR 0·71, 95% CI 0·54–0·92), and use of rainwater sources (RR 0·70, 95% CI 0·52–0·95) were each independently associated with a lower risk of diarrhoea in children aged <5 years (Table 3). The type of water storage vessel did not appear to affect risk. Drinking water from shallow wells increased the risk of diarrhoea in children when compared to consuming water from surface water sources. There was no evidence of clustering of diarrhoea by village.
Table 3.
Relative risk of diarrhoea in children aged <5 years by intervention status and by water and sanitation intervention employed, determined by multivariate analysis
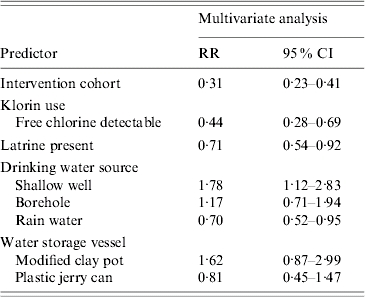
RR, Relative risk; CI, confidence interval.
When risk factors for diarrhoea in children aged <5 years were examined within the intervention cohort in a multivariate model, Klorin use (RR 0·42, 95% CI 0·26–0·67), and presence of a latrine (RR 0·58, 95% CI 0·38–0·88) were independently associated with a reduced risk of diarrhoea; use of shallow well water was independently associated with an increased diarrhoea risk (Table 4). There was no evidence of clustering of diarrhoea by village.
Table 4.
Relative risk of diarrhoea in children aged <5 years, by water and sanitation intervention employed in the intervention cohort, determined by multivariate analysis
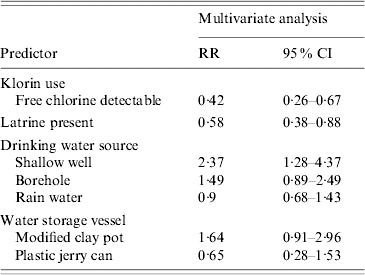
RR, Relative risk; CI, confidence interval.
Of the original 369 households with children aged <5 years in the baseline survey, 176 remained available for prospective diarrhoea surveillance, accounting for 32% of the cohort. An analysis of this subset seeking potential predictors of diarrhoea, such as mother's age, education status, and socio-economic status, did not identify additional covariables that modified the association of different interventions with diarrhoea risk.
DISCUSSION
This evaluation of the health impact of the SWS was the first in a rural African setting and demonstrated that SWS use was associated with a substantially lower risk of diarrhoea in children aged <5 years living in an impoverished region with unsafe water sources. The magnitude of the protective effect was consistent with the results of randomized controlled trials of the SWS in populations on three continents that differed in environmental conditions, culture, language, and prevalent water handling, sanitation, and hygiene practices [10–14]. This evaluation differed from previous studies because it measured effectiveness in a ‘real world’ setting, employing an implementation approach that required participants to purchase disinfectant solution and safe storage containers [15]. The finding that 43% of households were observed to have residual chlorine in stored water was substantially higher than results from household surveys in similar programmes elsewhere [18–20] and, as a measure of the population's willingness to purchase and use Klorin, indicated a moderate degree of programmatic success.
The protective effect of Klorin was independent of the impact of several other simultaneously promoted interventions, which included latrines, boreholes, and rainwater collection. The health impact of Klorin was equivalent to that of the other interventions, in contrast to what the dominant water and sanitation paradigm would have predicted: that sanitation, hygiene, and increased water supply would reduce diarrhoea more than improvements in water quality [21, 22]. That paradigm was based on literature reviews published in 1985 and 1991, at which time few studies on the health impact of point-of-use water quality interventions had been conducted. Since 1992, however, a number of published reports have demonstrated that point-of-use water quality interventions prevent contamination of stored water [23–29] and a recent Cochrane review indicated that they also reduce diarrhoea risk [30]. Another recent Cochrane review documented that the health impact of point-of-use water treatment is similar in magnitude to the impact of sanitation and hygiene interventions [31]. The growing weight of evidence of the efficacy of point-of-use interventions suggests that a new paradigm for the effect of environmental interventions on diarrhoeal disease is needed to take into account the high-risk zone between collection and consumption of drinking water that was not considered previously [32].
Multivariate models used in this evaluation revealed apparent synergy between the different interventions. Although the use of Klorin, latrines, or rainwater collection were each independently protective against disease, living in intervention villages showed a lower risk of diarrhoea than any individual intervention. This finding suggests that combined interventions might improve the general village environment and have greater impact than single interventions. A recent Cochrane review [31] suggested that the impact of multiple interventions may not be additive, but the results of this evaluation suggest that further investigation of combined interventions is warranted. A recently published modelling exercise suggested that, because of multiple diarrhea transmission pathways, the health impact of water quality interventions would be minimal in the absence of sanitation and hygiene interventions [33]. Although the conclusions of the modelling exercise are not borne out by existing data [30], the findings of this evaluation support the authors' contention that combined interventions that block several routes of diarrhoea transmission should more effectively reduce diarrhoea risk.
We did not attempt to evaluate hygiene behaviour in this evaluation because reported behaviour is notoriously unreliable [34] and we had inadequate resources to measure hand-washing behaviour objectively. In addition, volunteers in comparison villages incorporated the same PHAST hygiene and sanitation training into their promotional activities as did volunteers in the intervention villages, so the exposure to hygiene education was similar, although of shorter duration. Additional research is needed to determine the impact of improved hygiene combined with point-of-use water treatment; two recent evaluations suggest that the point-of-use water treatment and hand washing can be effectively co-promoted [35, 36].
In this evaluation, the use of improved containers exhibited no health benefit. This finding may have resulted from the relatively low numbers of participants who adopted the improved containers. Other studies have demonstrated a beneficial impact of narrow-mouthed, covered containers on the quality of stored water and on health [3, 25], but in those studies, the source water quality was good and the containers prevented contamination. In the case of this evaluation, the source water was contaminated, so disinfection was central to the impact of the intervention. Results of this evaluation suggest that chlorine disinfection may be a more effective barrier to recontamination of stored water than safe storage.
This evaluation had several important limitations. First, the quasi-experimental design raises the concern of a low effective number of observations if households within a given village are not independent of each other in the risk of transmission of diarrhoeal pathogens. In this case, however, the populations of these villages were dispersed, with households tending to be situated a distance of ⩾100 m from each other. These households were therefore not exposed to the immediate environment of other households, which mitigates the risk of exposure to pathogens. This is supported by the lack of evidence of disease clustering by village.
A second concern of quasi-experimental designs is whether the intervention and comparison communities are similar enough to make valid inferences from differences in outcomes. Furthermore, it is possible that confounding from variables that are not measured may influence outcomes. In the case of this evaluation, however, all communities were in the same geographical region, with the same language and cultural practices and economic activities. The differences in effect of the different interventions were consistent between and within the intervention and comparison groups, and the impact of Klorin, in particular, was similar in magnitude and direction to results obtained from studies in other geographic and cultural settings [10–14]. In this sense, the findings are robust.
A third limitation is the absence of baseline diarrhoea data. If baseline diarrhoea rates between children in intervention and comparison communities had been different, diarrhoea data collected subsequently could have been biased. This limitation was mitigated by the finding, noted above, that the effects of the interventions within the intervention village population were similar to the effects measured between intervention and comparison populations.
A fourth limitation is that, because of budgetary constraints, diarrhoeal outcomes were only measured during an 8-week period in the rainy season, when waterborne diseases were more likely to occur. It is possible, as two literature reviews have suggested, that there is an attenuation of the effect of point-of-use water interventions over time [30, 37]. Other research, however, suggests that utilization of such interventions may be enhanced over time with continued promotion [13]. Further research addressing this issue is needed.
Finally, because this evaluation assessed the effectiveness of an intervention in real-world conditions, in which the SWS was ‘grafted’ into an existing water and sanitation project, there was a potential for confounding between the effects of the different interventions, or for one intervention to reinforce the effect of another. The use of each intervention was, however, objectively verifiable, which enabled the stratification of households by intervention used and, consequently, for the independent effect of each intervention to be measured. The consistency in magnitude and direction of evaluation results, and their consistency with research findings in other settings, suggests that the findings are valid.
Since the completion of this evaluation, the social marketing campaign has continued with the disinfection solution rebranded as ‘WaterGuard.’ The solution is more concentrated, with a smaller bottle (150 ml vs. 500 ml) and lower price (20 Kenya shillings), and the programme has expanded nationally. Over one million bottles were sold in Kenya in 2006. Despite the robust sales, research in Kenya and elsewhere indicates that challenges remain in equity of access and consistent utilization of SWS products that must be purchased, and used daily [18–20, 38].
Results of this evaluation of the effectiveness of the SWS in the improvement of water quality and prevention of disease provide evidence for its utility as a tool in the armamentarium of strategies to prevent diarrhoea. Outcomes of this evaluation also suggest that added benefit can be obtained by combining the SWS with other water, sanitation, and hygiene interventions. Further study of this promising model is warranted. Inexpensive innovations that improve water quality, hygiene, and sanitation at the household level may help to reduce the burden of disease that impedes the development of communities in the developing world.
ACKNOWLEDGEMENTS
Funding for this evaluation was provided by the Woodruff Foundation through the CARE-CDC Health Initiative.
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Blakely T et al. The global distribution of risk factors by poverty level. Bulletin of the World Health Organization. 2005;83:118–132. [PMC free article] [PubMed] [Google Scholar]
- 2.WHO, United Nations Children's Fund (UNICEF), Water Supply and Sanitation Council Global Water Supply and Sanitation Assessment 2000 ReportNew York, NY: UNICEF; 2000, pp. 1–6. 77–79. [Google Scholar]
- 3.Hammad ZH, Dirar HA. Microbiologicalal examination of sebeel water. Applied Environmental Microbiology. 1982;43:1238–1243. doi: 10.1128/aem.43.6.1238-1243.1982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Han AM et al. Contamination of drinking water during collection and storage. Tropical & Geographical Medicine. 1989;41:138–140. [PubMed] [Google Scholar]
- 5.Black R, Lanata C, Blaser MJ, Smith PD, Ravdin JI. Infections of the Gastrointestinal Tract. New York: Raven Press Ltd; 1995. Epidemiology of diarrhoeal diseases in developing countries; pp. 13–36. , pp. [Google Scholar]
- 6.Parashar UD, Bresee JS, Glass RI. The global burden of diarrhoeal disease in children. Bulletin of the World Health Organization. 2003;81:236. [PMC free article] [PubMed] [Google Scholar]
- 7.UNESCO 2007. http://www.unesco.org/water/wwap/facts_figures/mdgs.shtml#goal7. http://www.unesco.org/water/wwap/facts_figures/mdgs.shtml#goal7 . World Water Assessment Programme . ). Accessed 16 March 2007.
- 8.World Health Organization/UNICEF. Meeting the MDG Drinking Water and Sanitation Target: The Urban and Rural Challenge of the Decade. Geneva: WHO Press; 2006. pp. 6–14. , pp. [Google Scholar]
- 9.CDC Safe Water Systems for the Developing World: A Handbook for Implementing Household-Based Water Treatment and Safe Storage Projects SWSAtlanta: Centers for Disease Control and Prevention; 2000 [Google Scholar]
- 10.Quick RE et al. Diarrhoea prevention in Bolivia through point-of-use water treatment and safe storage: a promising new strategy. Epidemiology and Infection. 1999;122:83–90. doi: 10.1017/s0950268898001782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Semenza JC et al. Water distribution system and diarrhoeal disease transmission: a case study in Uzbekistan. American Journal of Tropical Medicine and Hygiene. 1998;59:941–946. doi: 10.4269/ajtmh.1998.59.941. [DOI] [PubMed] [Google Scholar]
- 12.Quick R et al. Diarrhoea prevention through household-level water disinfection and safe storage in Zambia. American Journal of Tropical Medicine and Hygiene. 2002;66:584–589. doi: 10.4269/ajtmh.2002.66.584. [DOI] [PubMed] [Google Scholar]
- 13.Luby SP et al. Delayed effectiveness of home-based interventions in reducing childhood diarrhoea, Karachi, Pakistan. American Journal of Tropical Medicine and Hygiene. 2004;71:420–427. [PubMed] [Google Scholar]
- 14.Lule JR et al. Effect of home-based water chlorination and safe storage on diarrhoea among persons with human immunodeficiency virus in Uganda. American Journal of Tropical Medicine and Hygiene. 2005;73:926–933. [PubMed] [Google Scholar]
- 15.Makutsa P et al. Challenges in implementing a point-of-use water quality intervention in rural Kenya. American Journal of Public Health. 2001;91:1571–1573. doi: 10.2105/ajph.91.10.1571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ogutu P et al. Seeking safe storage: a comparison of drinking water quality in clay and plastic vessels. American Journal of Public Health. 2001;91:1610–1611. doi: 10.2105/ajph.91.10.1610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sawyer R, Simpson-Hebert M, Wood S.PHAST Step-by-Step Guide: A Participatory Approach for the Control of Diarrhoeal Disease. WHO/EOS/98.3ed. Geneva: World Health Organization; 1998 [Google Scholar]
- 18.Dunston C et al. Collaboration, cholera, and cyclones: how a pilot project to improve point-of-use water quality grew to national scale in less than a year. American Journal of Public Health. 2001;91:1574–1576. doi: 10.2105/ajph.91.10.1574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Safe water systems: an evaluation of the Zambia Clorin program. http://www.ehproject.org/PDF/Others/Zambia%20Report%20Format.pdf. 2007. http://www.ehproject.org/PDF/Others/Zambia%20Report%20Format.pdf ). Accessed 23 October .
- 20.CDC http://who.int/household_water/resources/Freeman.pdf. 2007. http://who.int/household_water/resources/Freeman.pdf . Removing barriers to point of use water treatment products through social marketing and entrepreneurship: a case study in western Kenya ( ). Accessed 23 October .
- 21.Esrey SA, Feachem RG, Hughes JM. Interventions for the control of diarrhoeal diseases among young children: improving water supplies and excreta disposal facilities. Bulletin of the World Health Organization. 1985;63:757–772. [PMC free article] [PubMed] [Google Scholar]
- 22.Esrey SA et al. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bulletin of the World Health Organization. 1991;69:609–621. [PMC free article] [PubMed] [Google Scholar]
- 23.Quick RE et al. Narrow-mouthed water storage vessels and in situ chlorination in a Bolivian community: a simple method to improve drinking water quality. American Journal of Tropical Medicine and Hygiene. 1996;54:511–516. doi: 10.4269/ajtmh.1996.54.511. [DOI] [PubMed] [Google Scholar]
- 24.Luby S et al. A low-cost intervention for cleaner drinking water in Karachi, Pakistan. International Journal of Infectious Diseases. 2001;5:144–150. doi: 10.1016/s1201-9712(01)90089-x. [DOI] [PubMed] [Google Scholar]
- 25.Roberts L et al. Keeping clean water clean in a Malawi refugee camp: a randomized intervention trial. Bulletin of the World Health Organization. 2001;79:280–287. [PMC free article] [PubMed] [Google Scholar]
- 26.Mong Y et al. Impact of the safe water system on water quality in cyclone-affected communities in Madagascar. American Journal of Public Health. 2001;91:1577–1579. doi: 10.2105/ajph.91.10.1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McGuigan K et al. Solar disinfection of drinking water contained in transparent plastic bottles: characterizing the bacterial inactivation process. Journal of Applied Microbiology. 1998;84:1138–1148. doi: 10.1046/j.1365-2672.1998.00455.x. [DOI] [PubMed] [Google Scholar]
- 28.McGuigan K, Joyce TM, Conroy RM. Solar disinfection: use of sunlight to decontaminate drinking water in developing countries. Journal of Medical Microbiology. 1999;48:785–787. doi: 10.1099/00222615-48-9-785. [DOI] [PubMed] [Google Scholar]
- 29.Crump JA et al. Effect of point-of-use disinfection, flocculation and combined flocculation-disinfection on drinking water quality in western Kenya. Journal of Applied Microbiology. 2004;97:225–231. doi: 10.1111/j.1365-2672.2004.02309.x. [DOI] [PubMed] [Google Scholar]
- 30.Clasen Tet al. Interventions to improve water quality for preventing diarrhoea [Review]. The Cochrane Library2006http://thecochranelibrary.com). Accessed 16 March 2007.
- 31.Fewtrell L et al. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis. Lancet Infectious Diseases. 2005;5:42–52. doi: 10.1016/S1473-3099(04)01253-8. [DOI] [PubMed] [Google Scholar]
- 32.Clasen TF, Cairncross S. Household water management: refining the dominant paradigm. Tropical Medicine and International Health. 2005;9:187–191. doi: 10.1046/j.1365-3156.2003.01191.x. [DOI] [PubMed] [Google Scholar]
- 33.Eisenberg JNS, Scott JC, Porco T. Balancing water sanitation and hygiene interventions to reduce diarrheal disease burden. American Journal of Public Health. 2001;97:1–7. doi: 10.2105/AJPH.2006.086207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tiballs J. Teaching hospital medical staff to handwash. Medical Journal of Australia. 1996;164:395–398. doi: 10.5694/j.1326-5377.1996.tb124899.x. [DOI] [PubMed] [Google Scholar]
- 35.Luby S et al. Combining water treatment and hand washing for diarrhoea prevention: a cluster randomized controlled trial. Tropical Medicine and International Health. 2006;11:479–489. doi: 10.1111/j.1365-3156.2006.01592.x. [DOI] [PubMed] [Google Scholar]
- 36.Parker A et al. Sustained high levels of stored drinking water treatment and retention of hand washing knowledge in rural Kenyan households following a clinic-based intervention. Epidemiology and Infection. 2006;134:1029–1036. doi: 10.1017/S0950268806005954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Arnold BF, Colford JM. Treating water with chlorine at point-of-use to improve water quality and reduce child diarrhea in developing countries: a systematic review and meta-analysis. American Journal of Tropical Medicine and Hygiene. 2007;76:354–364. [PubMed] [Google Scholar]
- 38.Stockman LJ et al. Awareness and use of WaterGuard among mothers in Malawi: lessons learned from a national survey, 2005. Emerging Infectious Diseases. 2007;13:1077–1080. doi: 10.3201/eid1307.070767. [DOI] [PMC free article] [PubMed] [Google Scholar]