

SUMMARY
Contacts of leprosy patients have a higher risk of developing clinical leprosy. Being a contact is defined socially, but with the introduction of geographical information systems (GIS) in infectious disease epidemiology, it is necessary to relate spatial distance to social distance. We measured the distances between patients and their socially defined contacts in northwest Bangladesh. Contact categories differ in mean distance to the index patients. Sixty-seven per cent of the high-risk contacts lived within 10 metres (m), while all low-risk contacts lived >10 m from the index patient. Classification based on intervals of spatial distance creates categories that contain contacts of different socially defined categories, illustrated by a category of people living between 10 m and 20 m consisting of 47% of high-risk contacts and 52% low-risk contacts. Classification of contacts based on the spatial distance, as performed with GIS techniques, produces other groups than with social definitions.
Contacts of leprosy patients have an increased risk of developing clinical leprosy themselves compared to non-contacts. Several risk factors add to this increased risk of which contact intensity is one important factor (reviewed in [1]). The contact intensity with patients is described using socially defined distances such as household member, neighbour and social contact.
Remote sensing (RS) and geographical information systems (GIS) are increasingly used in infectious disease epidemiology in general [2], and in recent years have also been introduced into leprosy research [3]. GIS techniques are used to classify contact based upon the actual distance (in metres) to an index patient. However, the relationship between such a classification based upon the actual distance and socially defined distances such as household member or neighbour are unknown. In this short report we aim to shed light on this issue.
We first studied whether a socially defined group has a certain typical distance, and second investigated the quantitative difference between direct (or Euclidean) distance and the walking distance. The latter was done because in the study area people live in small groups of houses (compounds). The houses contain one or several rooms. Some houses contain two separate households in different rooms. These households share a roof, but not the kitchen. A neighbour can live either on the same compound or on the next compound. A neighbour by definition lives under another roof. To take this organization of the houses into account, we investigated the direct distance – as would be done with GIS analysis – and the walking distance, which was defined as the distance an adult would take to walk from one house to another.
The study was in northwest Bangladesh, which is a densely populated, highly endemic area for leprosy, and was part of a larger study (the COLEP study) [4]. We measured the distance between the houses of patients and the houses of contacts. Contacts were categorized socially based upon the topological position of the house in which they lived, sharing of a kitchen or by the intensity of contact [4]:
those living under the same roof and using the same kitchen (KR);
those living under a separate roof, but using the same kitchen (K);
those living under the same roof, but not using the same kitchen (R);
next-door neighbours (N1);
neighbours of the neighbours (N2);
social contacts, who stay in the same room at least 4 h a day for 5 days a week (S).
The COLEP study included 1037 newly detected index leprosy patients, with a group of about 20 contacts each. From the index patients we randomly selected 40 patients and their contact groups. Of the selected groups, seven had partially or completely moved since intake into the COLEP study. These groups were excluded from the measurements. The remaining 33 groups contained 758 contacts living in 273 houses. We measured the distance between the front door of the index patients' houses and the front door of the houses of contacts. Distances were not measured beyond 100 m, and for the calculation of the mean distance this cut-off value was used. The results are shown in Table 1.
Table 1.
Risk of leprosy and distance (in metres) between the front door of an index patient and the front door of contacts for each contact category
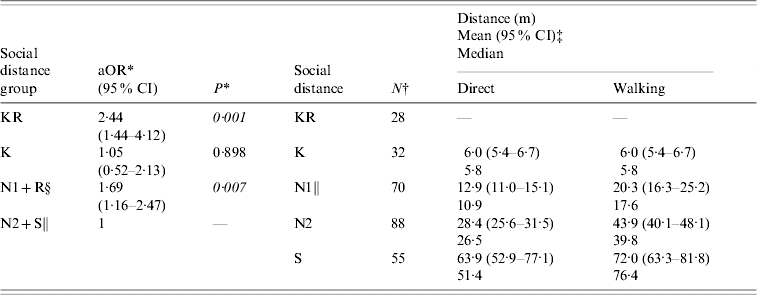
aOR, Adjusted odds ratio; CI, confidence interval.
For explanation of Social distance group abbreviations see text.
From [5], adjusted for age, sex, WHO leprosy classification of index patient, genetic relationship, presence of BGC scar, seropositivity for PGL-I antibodies against M. leprae.
Number of measurements in each category.
Mean and 95% CI were calculated for the log-transformed data. The figures have been back-transformed for an easier interpretation.
Contact categories were grouped [5].
There were no R contacts in the sample of contact groups in this study.
We found that 250 of the 273 houses of contacts (92%) were within the cut-off value of 100 m of the index patient (Table 2). The remaining 8% of contacts outside the 100-m range were all social (S) contacts. The measurements in Table 1 showed an increase in the mean distance for contact categories in the order KR, K, N1, N2, and S (Kruskal–Wallis test for trend, P<0·001). The socially defined contact categories KR and N1 can be grouped into a high-risk group based upon the findings of Moet et al. [5] (we assume K to be high risk as well, although this was not found in Moet et al. because of the small numbers; see [5]). Of the contacts living within 10 m of the index patient, all were within the socially defined high-risk group. However, of the 70 houses in the high-risk N1 category, 42 (60%) were beyond 10 m of the index patient. Of the 143 houses in the socially defined low risk group (N2+S), none were within 10 m of the index patient. A categorization based upon direct distance could be made, with the distance category ‘within 10 metres’ coinciding largely with the established high-risk contact group, and the distance ‘beyond 10 metres’ with the low-risk group.
Table 2.
Comparison of classification by social distance group and spatial distance, in 10-m intervals up to 50 m and classes of 50–100 m and ⩾100 m (absolute number of houses and rounded percentage of socially defined distance for each actual distance category)
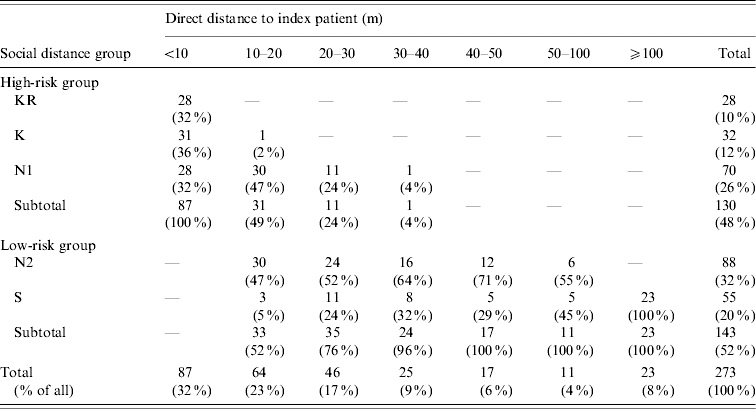
For explanation of Social distance group abbreviations see text.
However, classification based upon distance is not the same as socially defined categories. If one would have classified contact by distance categories with several 10-m intervals, the category 10–20 m would contain 47% N1, 47% N2 and 5% S contacts (see Table 2), mixing groups with different risks as found in [5], possibly resulting in a dilution of risk estimates. It is exactly these types of classifications that are made in analyses with GIS techniques.
However, the socially defined categorization also has its limitations as. It cannot be ruled out, for instance, that a N1 neighbour living further away has less contact than a N1 neighbour living nearby. Therefore, defining contact categories socially may as in Moet et al. [5] dilute risk estimates in another way.
The difference in classifying socially or by distance is further illustrated when we consider the measurements for walking distance, which can be related to the effort of making contact. The walking and direct distances were equal as long as both houses were situated on the same compound. In this way we could determine that 36% of the N1 lived on the same compound, while all N2 and S lived on other compounds. The N1 group thus is heterogeneous in terms of location on the same compound.
Classifying contact based upon spatial distance is not the same as a classification based upon definitions of social distance. The best classification would render the most homogeneous groups concerning risk of leprosy. Which one of these classifications is better for leprosy, cannot be determined by these data and is open for debate. Our result can differ when the population is distributed differently over dwellings, e.g. urban areas, or areas with a lower population density. In general our findings show that when contact is categorized either using GIS techniques or socially, infectious disease epidemiologists should keep in mind that they may be mixing individuals with different contact intensities and thus, risk of infection.
ACKNOWLEDGEMENTS
We thank the American Leprosy Missions and The Leprosy Mission International for financial support of the COLEP study.
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Moet FJ et al. Risk factors for the development of clinical leprosy among contacts, and their relevance for targeted interventions. Leprosy Review. 2004;75:310–326. [PubMed] [Google Scholar]
- 2.Cromley EK, McLafferty SL. GIS and Public Health. New York: Guilford; 2002. Analyzing the risk and spread of infectious diseases; pp. 188–209. , pp. [Google Scholar]
- 3.Bakker MI et al. Population survey to determine risk factors for Mycobacterium leprae transmission and infection. International Journal of Epidemiology. 2004;33:1329–1336. doi: 10.1093/ije/dyh266. [DOI] [PubMed] [Google Scholar]
- 4.Moet FJ et al. A study on transmission and a trial of chemoprophylaxis in contacts of leprosy patients: design, methodology and recruitment findings of COLEP. Leprosy Review. 2004;75:376–388. [PubMed] [Google Scholar]
- 5.Moet FJ et al. Physical distance, genetic relationship, age, and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosy. Journal of Infectious Diseases. 2006;193:346–353. doi: 10.1086/499278. [DOI] [PubMed] [Google Scholar]