

SUMMARY
Rapid notification of infectious diseases is essential for prompt public health action and for monitoring of these diseases in the Irish population at both a local and national level. Anecdotal evidence suggests, however, that the occurrence of notifiable infectious diseases is seriously underestimated. This study aims to assess the level of hospitalization for notifiable infectious diseases for a 6-year period in one health board region in Ireland and to assess whether or not there was any under-reporting during this period. All hospital in-patient admissions from 1997 to 2002 inclusive with a principal diagnosis relating to ‘infectious and parasitic diseases’ (ICD codes 001–139) of residents from a health board region in Ireland were extracted from the Hospital In-Patient Enquiry System (HIPE). All notifiable infectious diseases were identified based on the 1981 Irish Infectious Disease Regulations and the data were analysed in the statistical package, JMP. These data were compared with the corresponding notification data. Analysis of the hospital in-patient admission data revealed a substantial burden associated with notifiable infectious diseases in this health board region: there were 2758 hospitalizations by 2454 residents, 17 034 bed days and 33 deaths. The statutory notification data comprises both general practitioner and hospital clinician reports of infectious disease. Therefore, only in cases where there are more hospitalizations than notifications can under-reporting be demonstrated. This occurred in nine out of 22 notifiable diseases and amounted to an additional 18% of notifications (or 572 cases) which were ‘missed’ due to hospital clinician under-reporting. The majority of these under-reported cases were for viral meningitis (45%), infectious mononucleosis (27%), viral hepatitis C unspecified (15%) and acute encephalitis (5·8%). This study has highlighted the extent of under-reporting of hospitalized notifiable infectious diseases, in a health board region in Ireland, which is a cause for concern from a surveillance point of view. If this under-reporting is similar in other health boards, then it would appear that the epidemiology of some notifiable diseases is incomplete both regionally and nationally. This under-reporting negatively impacts on the effectiveness of the notification process as a ‘real-time’ surveillance tool and an early warning system for outbreaks.
INTRODUCTION
The 1981 Irish Infectious Disease Regulations [1] specify that as soon as a medical practitioner suspects that a patient is suffering from or is a carrier of a specified infectious disease, they must immediately notify the relevant medical officer of health. These data are collated regionally by the Public Health Department in each health board and nationally by the Health Protection Surveillance Centre (HPSC). The notification process is essential for activating prompt public health action, providing an early warning for outbreaks and monitoring disease incidence [2]. These data are used to inform and evaluate national and regional intervention programmes, for example, immunization policy. Furthermore, the information allows for collaboration with European and other international bodies on the monitoring and control of communicable disease. It is generally believed, however, that there is inadequate reporting of infectious diseases through the notification process [3]. It is a difficult task to accurately quantify the level of under-notification and clearly this has implications for disease surveillance and mounting appropriate public health responses.
Retrospective data on the occurrence of infectious diseases in hospitalized patients is available through the Hospital In-Patient Enquiry System (HIPE). HIPE is the only source of standardized national morbidity data available for acute hospital services in Ireland [4] and is the responsibility of the HIPE and National Perinatal Reporting System (NPRS) Unit at the Economic and Social Research Institute (ESRI). HIPE collects demographic, clinical and administrative data for each episode of hospital care. These data are taken from the patients' medical charts. Coding of the diagnoses and procedures is performed by using the International Classification of Diseases (ICD), 9th Revision – Clinical Modification and is carried out by a trained coder. Over 60 acute Irish public hospitals report on ~950 000 records annually using HIPE. The advantage of using HIPE is that the data are routinely collected and are standardized.
The HIPE dataset presents a valuable means of retrospectively assessing notifiable infectious disease hospitalizations. Indeed, these hospitalizations represent the most severe illnesses due to notifiable diseases and therefore warrant an extra onus on hospital clinicians to notify. The aim of this study, therefore, was to determine for one health board region in Ireland, the level of hospitalizations due to notifiable infectious diseases and to compare these hospitalizations with notifications for the same period to examine whether or not there was any substantial under-reporting of these diseases by hospital clinicians.
METHODS
The North Eastern Health Board (NEHB) has a population of 344 956 according to the 2002 census, which represents ~9% of the total national population and includes the counties of Cavan, Louth, Meath and Monaghan (Fig. 1). The regional NEHB population demographics have been shown to be similar to the national population demographics [5]. The health-care needs of this region are serviced by five acute hospitals (all of which contribute data to HIPE) and approximately 150 general practitioners. Overall, this health board region represents an ideal study cohort. All hospital in-patient admissions for NEHB residents from 1997 to 2002 with a principal diagnosis relating to ‘infectious and parasitic diseases’ (ICD codes 001-139) were extracted from HIPE. The HIPE datasets for the years from 1997 to 2002 were provided by ESRI. Only the principal diagnosis (the primary reason for admission) was selected in order to best represent new incident cases of disease and in order to eliminate co-existing or historical conditions from the analysis. All notifiable infectious diseases in the HIPE dataset were identified based on the 1981 Infectious Disease Regulations.
Fig. 1.

Map of Ireland (showing NEHB counties in white).
In cases where patients had more than one hospitalization for the same condition all duplicates were removed based on a first occurrence per patient basis. This was done in order to assess the number of notifications that should have arisen due to hospitalization events. Patients who were re-admitted to the same hospital with the same principal diagnosis were eliminated from the data using medical record numbers. Similarly patients who were transferred between hospitals were eliminated from the data using the patient's date of birth, sex, county, diagnosis and a hospital admission date within 1 day of discharge from a previous hospital. In order to protect the privacy of patients, where there were less than five cases, the data was aggregated into a category called ‘Others’.
Notification data on all notifiable infectious diseases for NEHB residents were provided by the Department of Public Health, NEHB and the HPSC. All data were analysed in the statistical package, JMP (SAS Institute, Cary, NC, USA).
RESULTS
During the 6-year period between 1997 and 2002 there were 2758 notifiable infectious disease hospitalizations among 2454 NEHB residents (Table). These notifiable disease hospitalizations represented 31·3% of all infectious disease hospitalizations for NEHB residents and 0·82% of total hospitalizations for NEHB residents. The most common notifiable disease admission was for gastroenteritis in children aged <2 years (28·3%), followed by viral meningitis (11·1%) and tuberculosis (10·4%).
Table.
Hospitalizations and notifications for NEHB residents between 1997 and 2002
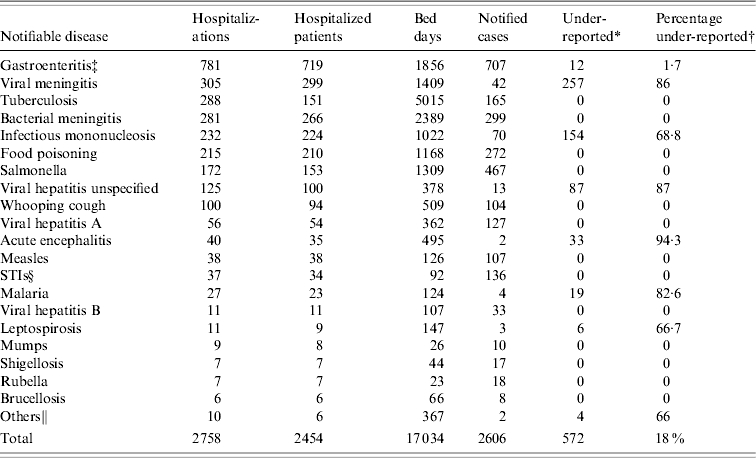
The number of under-reported cases is calculated by subtracting the number of notified cases from the number of hospitalized patients with the corresponding infectious disease.
The percentage under-reported is calculated by dividing the number under-reported by the number of notified cases plus the number under-reported.
Gastroenteritis in children aged <2 years.
Notifiable sexually transmissible infections: ano-genital warts, candidiasis, chancroid, Chlamydia trachomatis, genital herpes simplex, gonorrhoea, granuloma inguinale, lymphogranuloma venereum, molluscum contagiosum, non-specific urethritis, Pediculosis pubis, syphilis, trichomoniasis.
Includes the notifiable diseases of Typhoid/Paratyphoid. Further breakdown of figures could not be given due to data protection issues.
A total of 17 034 bed days were taken up by this cohort of patients hospitalized with a principal diagnosis of a notifiable disease. Overall, tuberculosis patients took up the highest number of bed days (5015 days) and also had the highest average length of stay per patient (33·2 days). Bacterial meningitis patients took up the second highest number of bed days (2389 days) and had an average length of stay of 9 days per patient. There were 33 deaths among patients hospitalized with notifiable diseases. The highest number of deaths occurred among bacterial meningitis patients (n=11) followed by tuberculosis patients (n=8) and acute encephalitis patients (n=8).
The notification data, between 1997 and 2002, revealed that there were 2606 cases of infectious diseases notified for NEHB residents (Table). Assuming all hospitalized notifiable diseases will also be notified then comparison of the number of notified cases with the number of hospitalized patients for the same 6-year period highlights under-reporting by hospital clinicians in the NEHB. Only in cases were there are more hospitalizations than notifications can under-reporting be established. This occurred for nine out of 22 infectious diseases and should have generated and extra 572 notifications (Table). This would bring the total number of notifications for this 6-year period from 2606 to 3174. In other words, 18% of notifications overall, which should have been generated during this period, were not reported.
The most frequently under-reported notifiable infectious disease was viral meningitis. There were 299 NEHB residents hospitalized on 305 occasions with a principal diagnosis of viral meningitis. The majority of patients were in the 0–9 years age group (42·3%). These patients took up 1409 bed days. The majority (69%) of these hospitalized cases occurred in 2000 and 2001 (Fig. 2a). Despite this ‘hospital activity’ there were only 42 notifications – a disparity of 257 cases – which corresponds to an under-reporting of 86%. With this level of under-reporting, the dramatic rise in the incidence of hospitalized viral meningitis patients during 2000 and 2001 was obscured. There was also extensive under-reporting of hospitalized infectious mononucleosis cases. In total, there were 224 NEHB residents hospitalized on 232 occasions with a principal diagnosis of infectious mononucleosis. These patients had a median age of 16 years (range 0–69 years) with the most common age group affected being 15–19 years (54%). These infectious mononucleosis patients took up, in total, 1022 bed days. There were, however, only 70 notifications reported between 1997 and 2002 – a disparity of 154 cases (Fig. 2b). The third most under-reported disease was ‘viral hepatitis unspecified’ (including hepatitis C). There were 100 NEHB residents hospitalized on 125 occasions and the majority of patients (39%) had a principal diagnosis of chronic hepatitis C without hepatic coma. These patients had a median age of 36·5 years (range 1–86 years) and the most common age group affected was 50–54 years (14·5%). In total these patients took up 378 bed days. Yet, there were only 13 notifications reported – a disparity of 87 cases (Fig. 2c).
Fig. 2.

Hospitalizations and notifications of (a) viral meningitis, (b) infectious mononucleosis, (c) viral hepatitis unspecified and (d) acute encephalitis between 1997 and 2002.
There was a total of 35 NEHB residents hospitalized on 40 occasions with acute encephalitis. These patients had a median age of 42 years (range 0–88 years) and the most common age group affected was 0–4 years (22·6%). The majority of these patients (54·3%) had a principal diagnosis of viral encephalitis not otherwise specified or not elsewhere classifiable. Of cases where an aetiology was recorded the largest proportion of patients (17%) were diagnosed with herpes simplex meningo-encephalitis. Overall, these hospitalizations for acute encephalitis peaked in 2000 and began to decline thereafter (Fig. 2d). There were, however, only two notifications for acute encephalitis and surprisingly both notifications occurred in 2001, the year after the peak in encephalitis hospitalizations. This corresponds to a meagre notification rate of 6% (under-reporting of 94%) and paints the starkest of pictures considering there were eight deaths in this cohort. The under-reporting of typhoid and paratyphoid cases is another cause for concern. All cases identified in HIPE had a principal diagnosis of paratyphoid B and all cases were in the 15–19 years age group. There were, however, no corresponding notifications for these hospitalized paratyphoid cases. Failure to notify these diseases has implications for public health since contact tracing and further preventative measures cannot occur.
Other diseases for which under-reporting was identified include malaria (n=19, 82·6% under-reporting), gastroenteritis in children aged <2 years (n=12, 1·7% under-reporting), leptospirosis (n=6, 66·7% under-reporting).
DISCUSSION
Under-reporting has been demonstrated in various countries for specific notifiable infections including bacterial meningitis [6–8], encephalitis [9], gastroenteritis [10, 11], hepatitis A [12], B [13–15] and C [14, 16], Legionnaires' disease [17], malaria [18], pertussis [19–21], tuberculosis [22, 23] and viral meningitis [24]. Some of these studies have also used comparisons with hospital in-patient admission/discharge systems to identify incomplete notification. For example, under-reporting of viral hepatitis C by 79% between 1993 and 2000 was identified by Strauss et al. [6] using the Austrian Hospital Discharge Register. Another study [7] comparing the English Hospital Episode Statistics to notifications of viral encephalitis from 1989 to 1998, concluded that there was a ‘disparity which implies that almost all (97%) hospitalized cases were not formally reported’.
This study, however, is the first comprehensive report in which all hospitalized notifiable diseases from a single statutory list has been examined for under-reporting. This was achieved by comparing hospital in-patient admission data with the notification data for the same period. In essence, over the 6-year period between 1997 and 2002 in the NEHB region, 18% of notifications (or 572 cases) which should have been generated were ‘missed’ due to hospital clinician under-reporting. These under-reported notifiable infectious diseases include infections for which immediate public health action must be taken (typhoid/paraptyphoid), infections for which enhanced surveillance is required (leptospirosis, malaria) and infections which do not require immediate public health intervention (gastroenteritis, acute encephalitis, viral hepatitis unspecified, viral meningitis, infectious mononucleosis). Clearly, the phenomenon of under-reporting spans the list of notifiable diseases and is not limited to less severe infections or those for which surveillance would be considered less important.
In fact, the under-reporting of 18% of notifications may be a conservative estimate for a number of reasons. First, only patients with a principal diagnosis of a notifiable infectious disease were analysed in this study in order to best represent new incident cases of disease. This approach may have overlooked some hospital in-patients with a notifiable infectious disease in a second, third, fourth, fifth or sixth diagnosis that would also have generated notifications. Second, for some diseases, e.g. gastroenteritis, patients may be susceptible to repeat bouts of the disease and these repeat hospitalizations have not been included in the analysis. Finally, patients that attend only Accident and Emergency departments and are not admitted to hospital are not included in the HIPE dataset. Thus, these patients if not reported by the attending clinician represent yet another source of under-reporting. Under-reporting of hospitalized patients with a notifiable infectious disease, therefore, is likely to occur to a much wider extent than demonstrated by this study.
If the level of under-reporting identified in the NEHB is similar in other health boards in Ireland, then it would appear that, nationally, the epidemiology of some notifiable diseases is being obscured and this casts doubt on the effectiveness of the notification process as a surveillance tool and an early warning system for outbreaks. Furthermore, these hospitalization data represent the most severe of cases and also represent only a proportion of the total cases occurring in the larger community. Although not in the scope of this study, it is likely that there is also substantial under-reporting of notifiable diseases by general practitioners [25, 26]. These facts make it extremely difficult to get a true measure of the overall infectious disease incidence in the Irish population.
But what contributes to under-reporting? Various studies cite that excess work and lack of time [25], lack of familiarity of the list of statutory notifiable diseases [26–28], lack of understanding of the importance of notification [3, 29] and concern regarding confidentiality [29] contributes to poor clinician reporting. Seneviratne et al. [30] proposed that a lack of feedback on the outcome of notification investigations is perceived by clinicians as no useful action has been taken and this in turn leads to further apathy about the process. These researchers found however, that the appointment of a ‘notification nurse’ and having a specific ward register for infectious diseases improved notifications significantly. However, Figueiras et al. [31], suggest that these are ‘external facilitating factors’ and the most important hurdle to overcome is the clinicians' attitude to the notification process itself. These attitudes and lack of motivation can only be tackled through enhanced educational programmes including undergraduate courses and continuing medical education (CME) courses. Indeed, this study has highlighted a group of notifiable diseases that particularly warrants educational intervention and regional feedback.
Surveillance systems must be flexible in order to monitor changes in disease incidence so that public health measures can be promptly implemented. More timely hospital in-patient admission statistics would provide a comprehensive addition to the current surveillance system. However, many of the diagnoses for infectious diseases in HIPE are non-specific in that the responsible aetiological agent is not recorded. This may be due to a number of reasons including the extent to which an illness is investigated and the availability of appropriate diagnostic techniques and computerized records. With the ever-changing pattern of disease over time and the emergence of infections, the recording of more detailed diagnosis in HIPE will become more important and will aid in the understanding of disease and outbreak epidemiology.
On 1 January 2004, the 1981 Irish Infectious Disease Regulations [1] were amended in order to update the list of notifiable diseases and to make microbiology laboratories legal notifiers. These changes together with the imminent roll out of a national Computerised Infectious Disease Reporting (CIDR) system [32] will go some way to addressing the problem of under-reporting in Ireland. However, some diseases, e.g. viral encephalitis, will still only be diagnosed clinically and therefore it is essential to provide education and feedback to relevant health-care workers on the importance of the notification process. Furthermore, studies like this one may provide a baseline for comparing the effectiveness of the new reporting system into the future.
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Infectious Disease Regulations, 1981 1981. . SI No. 390 of . (amended by SI No. 268 of 1985, SI No. 288 of 1988, SI No. 384 of 1996, SI No. 151 of 2000 and SI No. 707 of 2003).
- 2.National Disease Surveillance Centre 2001. . Review of notifiable diseases and the process of notification. Dublin: National Disease Surveillance Centre,
- 3.Harvey I. Infectious disease notification – a neglected legal requirement. Health Trends. 1991;23:73–74. [PubMed] [Google Scholar]
- 4.Department of Health and Children Dublin: Economic and Social Research Institute; 2002. . Activity in acute public hospitals in Ireland 1990–1999. [Google Scholar]
- 5.Department of Public Health, North Eastern Health Board 2004. . Health status report of the people of the north east,
- 6.Meyer CN et al. Adult bacterial meningitis: aetiology, penicillin susceptibility, risk factors, prognostic factors and guidelines for empirical antibiotic treatment. Clinical Microbiology and Infection. 2004;10:709–717. doi: 10.1111/j.1469-0961.2004.00925.x. [DOI] [PubMed] [Google Scholar]
- 7.Harvey I, Kaul S, Peters TJ. Auditing and improving notification and chemoprophylaxis in bacterial meningitis. Journal of Epidemiology and Community Health. 1992;46:329–331. doi: 10.1136/jech.46.4.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Goldacre MJ, Miller DL. Completeness of statutory notification for acute bacterial meningitis. British Medical Journal. 1976;2:501–503. doi: 10.1136/bmj.2.6034.501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Davison KL et al. Viral encephalitis in England, 1989–1998: what did we miss? Emerging Infectious Diseases. 2003;9:234–240. doi: 10.3201/eid0902.020218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Flint JA et al. From stool to statistics: reporting of acute gastrointestinal illnesses in Canada. Canadian Journal of Public Health. 2004;95:309–313. doi: 10.1007/BF03405138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barrett P, Lau YK. Incompleteness of statutory notification of bacterial gastro-intestinal infection. Public Health. 1996;111:183–185. doi: 10.1016/s0033-3506(97)00580-5. [DOI] [PubMed] [Google Scholar]
- 12.Lerman Y et al. How valid is the official data from the Health Department on reported morbidity in Israel? Hepatitis A as an example. Harefuah. 1999;136:441–445. [PubMed] [Google Scholar]
- 13.Poulos RG, Ferson MJ. Enhanced surveillance of acute hepatitis B in south-eastern Sydney. Communicable Disease Intelligence. 2004;28:392–395. doi: 10.33321/cdi.2004.28.44. [DOI] [PubMed] [Google Scholar]
- 14.Hagan H et al. Case-reporting of acute hepatitis B and C among injection drug users. Journal of Urban Health. 2002;79:579–585. doi: 10.1093/jurban/79.4.579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Abdool Karim SS, Abdool Karim Q. Under-reporting in hepatitis B notifications. South African Medical Journal. 1991;79:242–244. [PubMed] [Google Scholar]
- 16.Strauss R, Fulop G, Pfeifer C. Hepatitis C in Austria 1993–2000: reporting bias distort HCV epidemiology in Austria. Eurosurveillance. 2003;8:113–118. doi: 10.2807/esm.08.05.00412-en. [DOI] [PubMed] [Google Scholar]
- 17.Smith A et al. Legionnaires' disease in Ireland – a cause for concern? Irish Medical Journal. 2002;95:308–310. [PubMed] [Google Scholar]
- 18.Davidson RN et al. Under-reporting of malaria, a notifiable disease, in Britain. Journal of Infection. 1993;26:348–349. doi: 10.1016/0163-4453(93)96241-h. [DOI] [PubMed] [Google Scholar]
- 19.Beard SM, Finn A. Do we need to boost pertussis immunization within the existing UK vaccination schedule? Journal of Public Health Medicine. 2000;22:349–356. doi: 10.1093/pubmed/22.3.349. [DOI] [PubMed] [Google Scholar]
- 20.Andrews R, Herceg A, Roberts C. Pertussis notifications in Australia, 1991 to 1997. Communicable Disease Intelligence. 1997;21:145–148. doi: 10.33321/cdi.1997.21.30. [DOI] [PubMed] [Google Scholar]
- 21.Jenkinson D. Whooping cough: what proportion of cases is notified in an epidemic? British Medical Journal (Clinical Research Edition) 1983;287:185–186. doi: 10.1136/bmj.287.6386.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pillaye J, Clarke A. An evaluation of completeness of tuberculosis notification in the United Kingdom. BMC Public Health. 2003;6:31. doi: 10.1186/1471-2458-3-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.van Loenhout-Rooyackers JH et al. Pyrazinamide use as a method of estimating under-reporting of tuberculosis. International Journal of Tuberculosis and Lung Disease. 2001;5:1156–1160. [PubMed] [Google Scholar]
- 24.Brabazon ED et al. Trends in viral meningitis hospitalisations and notifications in the North Eastern Health Board (1997–2001): a cause for concern? Irish Medical Journal. 2004;97:306–308. [PubMed] [Google Scholar]
- 25.Dinis J. Mandatory notification of communicable diseases: what physicians think. Acta Medica Portuguesa. 2000;13:33–38. [PubMed] [Google Scholar]
- 26.Durrheim D, Thomas J. General practice awareness of notifiable infectious diseases. Public Health. 1994;108:273–278. doi: 10.1016/s0033-3506(94)80006-5. [DOI] [PubMed] [Google Scholar]
- 27.Abdool Karim SS, Dilraj A. Reasons for under-reporting of notifiable conditions. South African Medical Journal. 1996;86:834–836. [PubMed] [Google Scholar]
- 28.Spedding RL, Jenkins MG, O'Reilly SA. Notification of infectious diseases by junior doctors in accident and emergency departments. Journal of Accident and Emergency Medicine. 1998;15:102–104. doi: 10.1136/emj.15.2.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Collins G. Notification of infectious diseases (SHB) Infoscan. 1997;7(4) [Google Scholar]
- 30.Seneviratne SL, Gunatilake SB, de Silva HJ. Reporting notifiable diseases: methods for improvement, attitudes and community outcome. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1997;91:135–137. doi: 10.1016/s0035-9203(97)90199-1. [DOI] [PubMed] [Google Scholar]
- 31.Figueiras A et al. Influence of physicians attitudes on under-notifying infectious diseases: a longitudinal study. Public Health. 2004;118:521–526. doi: 10.1016/j.puhe.2003.12.015. [DOI] [PubMed] [Google Scholar]
- 32.National Disease Surveillance Centre 2003. p. 114. . Annual Report . : Computerised Infectious Disease Reporting System, p.