

SUMMARY
The purpose of this study was to assess the association between human T-lymphotropic virus 1 (HTLV-1) and a lifetime history of active tuberculosis (TB) among relatives of HTLV-1-infected patients. We reviewed clinical charts of all relatives of HTLV-1-infected index cases who attended our institute in Lima from 1990–2004. The data of 1233 relatives was analysed; 394 (32·0%) were HTLV-1 positive. Eighty-one subjects (6·6%) had a history of active TB, including 45/394 (11·4%) HTLV-1-positive and 36/839 (4·3%) HTLV-1-negative relatives (P<0·001). On multivariate analysis, three factors were associated with TB history: HTLV-1 infection (adjusted OR 2·5, 95% CI 1·6–3·9), age (adjusted OR 1·3, 95% CI 1·1–1·5 per 10-year age increase) and relation to the index case (adjusted OR 2·6, 95% CI 1·3–5·1, for siblings vs. spouses of index cases). In conclusion, HTLV-1 infection may increase the susceptibility to active TB. In populations where both infections are frequent, such an association could affect the dynamics of TB.
INTRODUCTION
Human T-lymphotropic virus 1 (HTLV-1) is a retrovirus that produces a lifelong infection [1]. Worldwide, an estimated 20 million people are infected [2]. The majority of carriers remain asymptomatic. HTLV-1 nonetheless causes morbidity and mortality in endemic areas, because in 2–5% of the carriers, infection is associated with severe diseases such as adult T-cell leukaemia/lymphoma and HTLV-1-associated myelopathy/tropical spastic paraparesis. Furthermore, HTLV-1-infected individuals are at increased risk of developing specific infections: associations of HTLV-1 with strongyloidiasis, infective dermatitis, scabies, leprosy, and kidney or bladder infections have been reported [1, 3, 4]. HTLV-1 can be transmitted through blood transfusion, exchange of contaminated needles or syringes, sexual intercourse, and from mother to child [1]. Because of the latter two routes of transmission, HTLV-1 tends to cluster within families. In Peru, it is estimated that 1–3% of the healthy adult population carry HTLV-1 [5, 6].
Peru is also endemic for tuberculosis (TB). Although the TB incidence rate has decreased after the extensive implementation of the WHO programme of Directly Observed Treatment, Short Course Strategy (DOTS) in 1990, Peru still has one of the highest TB incidence rates of the Americas, with an estimated 172 cases/100 000 in 2005 [7].
The adverse impact of HIV on the incidence and outcome of TB is well known [8]. There is less information on the effects of HTLV-1 infection on TB. In Japan, HTLV-1-infected people show a reduced delayed-type hypersensitivity response to purified protein derivative (PPD) of Mycobacterium tuberculosis, whereas the response to phytohaemagglutinin is normal [9, 10]. In a study of former blood donors in the United States, HTLV-1 carriers responded normally to antigens of mumps and Candida albicans [11]. Furthermore, high frequencies of HTLV-1 infection among TB patients have been reported in Japan, Nigeria and Brazil [12–14]. On the other hand, in studies in Senegal and Papua New Guinea, few TB patients were HTLV-1 infected [15, 16].
Fewer studies started with HTLV-1-infected individuals and looked at the occurrence of TB. In one Japanese report, TB history was more frequent among HTLV-1-infected than among seronegative men [17]. In another Japanese study, chest X-ray findings compatible with old pulmonary TB were more frequent among HTLV-1 carriers than among non-carriers [18].
In order to assess the association between HTLV-1 and a lifetime history of active TB, we conducted a cross-sectional study among family members of HTLV-1-infected subjects attending a referral centre in Lima, Peru.
METHODS
Setting
At the Institute of Tropical Medicine Alexander von Humboldt in Lima, we provide HTLV-1 screening and clinical follow-up to patients with presumptive diagnoses of HTLV-1-associated diseases. Also HTLV-1-positive candidate blood donors are being referred to our institute for counselling. Each time a new case of HTLV-1 infection is documented (‘index case’), we offer free HTLV-1 screening to their blood relatives as well as their partners. The routine evaluation of index cases and their relatives includes a standardized interview by trained health-care workers and HTLV-1 testing. During the study period, enzyme immunoassays (EIA; Sanofi Diagnostics Pasteur, Marnes-la-Coquette, France; Bio-Rad Laboratories, Hercules, CA, USA; or Cambridge Biotech, Worcester, MA, USA) were used as screening tests. Most of the reactive samples (62%) were confirmed with Western blot (Genelabs Diagnostics, Singapore) or line immunoassay (Innogenetics, Ghent, Belgium). Not all reactive samples underwent confirmatory testing because of some financial limitations during the study period.
Study population
For this study, we reviewed the clinical charts of all relatives of HTLV-1-infected index cases and included the data of those relatives screened between January 1990 and January 2004. Children aged <3 years were not included because at that age, the EIA results are neither entirely reliable nor definitive, especially because prolonged breastfeeding is common in this population. We excluded data of relatives with indeterminate serology or without information on TB history.
Data collection
The clinical charts contained demographic information, data on medical and HTLV-1 risk factor history, and included questions on TB history. We considered that if someone had ever received TB treatment, he or she had a history of active TB. All clinical charts had been filled out at the first contact with an index case's relative, before interviewer and respondent were aware of the HTLV-1 status. A blank copy of these charts is available on request.
Statistical analysis
The frequency of a history of TB in HTLV-1-negative relatives was compared to that in HTLV-1-positive relatives and index cases using χ2 tests. Through bivariate analyses, we assessed the crude association between a lifetime history of active TB and the following variables: HTLV-1 status; age at the time of HTLV testing; sex; ethnicity; history of blood transfusion and of drug abuse; relation to the index case and reason for HTLV-1 testing of the index case. Ethnicity was defined as Andean if both parents or all four grandparents were born in the Andean region.
Multivariate analysis was done using the generalized estimating equation method, in order to adjust for the effect of potential confounding factors and at the same time to account for correlation between family members [19]. All variables with a P value of <0·2 on bivariate evaluation were included in the model. To check whether the lack of HTLV-1 confirmation tests could influence the results, we repeated the analysis excluding all subjects with unconfirmed positive EIA results.
Data were stored in Microsoft Access and analysed with SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, USA) and R 2.5.0 [20].
HIV
Until 2004, HIV tests were not part of the routine evaluation of people who came for HTLV-1 screening at our institute. To check the frequency of HIV among the relatives who were included in this study and had a history of TB according to their clinical charts, we visited these people and invited them to participate in a follow-up study. After informed consent, trained health-care workers interviewed these subjects and took a new sample, which was then tested for HIV using a microparticle chemoilluminometric immunoassay (Bayer Healthcare, Lima, Peru).
Ethical considerations
The study protocol was approved by the Institutional Review Board of the Universidad Peruana Cayetano Heredia and the study was conducted following the guidelines of this university with respect to human participants' protection.
RESULTS
A total of 1305 relatives were tested for HTLV-1. Four hundred and ten of 665 (61·7%) index cases had brought at least one family member. Family studies started more frequently with female than with male index cases and more frequently with diseased than with healthy index cases (Table 1). Twenty-seven relatives were excluded because of indeterminate HTLV-1 serology; 32 because of missing information on TB; and 13 children were not included because they were aged <3 years when tested. The remaining 1233 relatives, from 398 families, were included. In addition to the index case, the median number of participants per family was two (interquartile range 1–4, range 1–23).
Table 1.
Characteristics of index cases with and without family studies
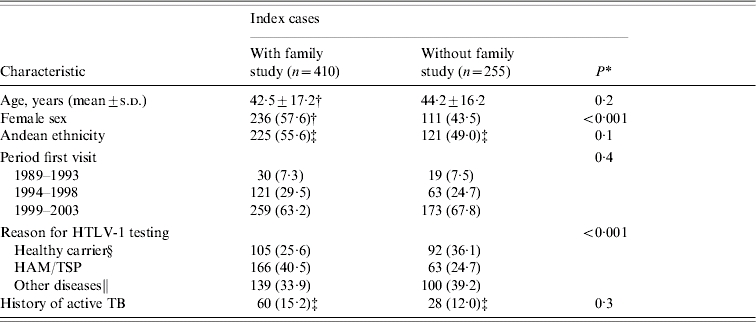
s.d., Standard deviation; HAM/TSP, HTLV-1-associated myelopathy/tropical spastic paraparesis.
t test for age and Pearson χ2 test for the other variables.
Data are presented as absolute numbers and percentages (within parentheses), except for age, which is expressed as mean±s.d. in years.
Data of some index cases were missing; percentages were calculated on available data.
A total of 185 were blood donors; 8 were found positive during a general health check up and 4 tested positive during a HTLV-1 surveillance study.
Other diseases: 110 strongyloidiasis; 52 infective dermatitis; 31 other dermatological problems; 20 adult T-cell leukaemia/lymphoma; 14 uveitis; 12 diverse other diseases.
The mean age (±s.d.) of the relatives was 36 (±18) years; 777 (63·0%) were female. In total, 475 (38·5%) were children of index cases; 236 (19·1%) siblings; 161 (13·1%) parents; and 200 (16·2%) spouses. A total of 161 relatives (13·1%) had more distant relationships with index cases. HTLV-1 screening tests were positive in 394 family members (32·0%); in 248 (62·9%), the diagnosis of HTLV-1 infection was confirmed with Western blot or line immunoassay.
Eighty-one relatives (6·6%) reported a history of TB: 36/839 (4·3%) HTLV-1-negative and 45/394 (11·4%) HTLV-1-positive individuals (χ2 test, P<0·001). Among the index cases, 60/395 (15·2%) had a history of TB (χ2 test: P<0·001 compared to HTLV-1-negative, and P=0·1 compared to HTLV-1-positive relatives). Sixteen of the 45 patients (36%) with HTLV-1 and TB were children or siblings of infected subjects.
The comparison between relatives with and without a history of active TB is shown in Table 2. Forty-five of 81 relatives (56%) with TB history were HTLV-1 positive, compared to 349/1152 relatives (30%) without TB history [odds ratio (OR) 2·9, 95% confidence interval (CI) 1·8–4·5]. People with a history of TB were older (OR 1·3, 95% CI 1·1–1·5 per 10-year age increase) and more frequently of Andean ethnicity (OR 1·9, 95% CI 1·2–3·1). They also reported more often that they had received a blood transfusion (OR 2·5, 95% CI 1·4–4·4).
Table 2.
Characteristics of all relatives with and without history of active TB; bivariate and multivariate analyses
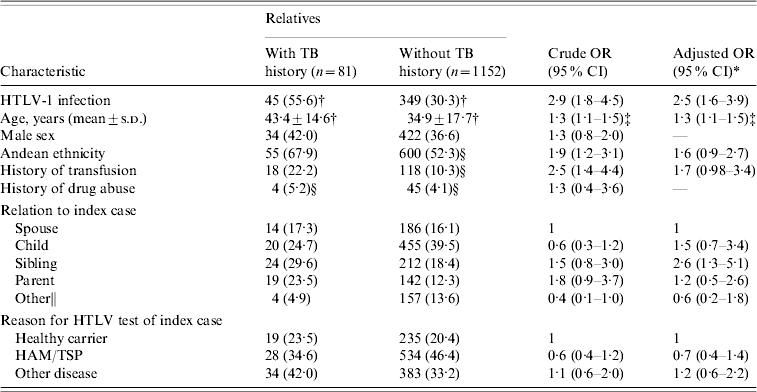
s.d., Standard deviation; OR, odds ratio; CI, confidence interval; HAM/TSP, HTLV-1-associated myelopathy/tropical spastic paraparesis.
Generalized estimating equation including the following variables: HTLV-1 infection, age, ethnicity, transfusion history, relation to the index case, reason for HTLV test of index case and family code.
Data are presented as absolute numbers and percentages (within parentheses), except for age, which is expressed as mean±s.d. in years.
OR per 10-year age increase.
Data of some relatives were missing; percentages were calculated on available data.
Other: 29 grandchildren, 3 grandparents, 15 uncles/aunts, 20 nephews/nieces, 17 cousins, 23 siblings by marriage, 18 stepchildren, 15 parents by marriage, 21 more distant relations.
On multivariate analysis, three factors were significantly associated with a lifetime history of active TB: HTLV-1 status (adjusted OR 2·5, 95% CI 1·6–3·9 for seropositive versus seronegative relatives), age (adjusted OR 1·3, 95% CI 1·1–1·5 per 10-year age increase) and relation to the index case (adjusted OR 2·6, 95% CI 1·3–5·1 for siblings compared to spouses) (Table 2). When we repeated the same analysis excluding all relatives with unconfirmed EIA-positive samples, the association between TB history and HTLV-1 infection remained significant (adjusted OR 2·2, 95% CI 1·2–3·8).
From June 2006 to January 2007, we organized home visits to the relatives who according to their clinical charts had a history of TB. Thirty-seven out of 81 subjects (46%) were found. The remaining relatives were not able to be contacted at home on at least two occasions (n=18), had moved to an unknown address (n=15), died (n=4), or lived outside Lima (n=3); for four relatives, the address registered on the chart did not exist. Among those who died, the cause of death according to the relatives was: myocardial infarct, bladder cancer, cerebral trauma, and TB.
Twenty-three of the 37 relatives who were found (62%; 13 HTLV-1 positive and 10 HTLV-1 negative) were willing to undergo HIV screening; they were all HIV negative. Three subjects did not want to participate because they already knew their HIV status: two HTLV-negative subjects had been tested a few months before our visit and were HIV negative and one HTLV-1-infected subject reported a diagnosis of HIV infection in 2003.
On interview, the 23 participants in the follow-up study confirmed that they had been treated for active TB; they were able to mention the year and place of treatment. Twenty-one subjects reported having had pulmonary TB; one had a history of pleural and one of renal TB. None of these subjects had had more than one TB episode.
DISCUSSION
We found an association between HTLV-1 infection and a lifetime history of active TB among relatives of HTLV-1-infected patients. After adjustment for demographic and HTLV-1 risk factor characteristics, relatives with a history of TB were more than twice as likely to be HTLV-1 infected than those who never had TB. In this population, TB history was also associated with older age and with being sibling of an HTLV-1-infected index case.
Because of the cross-sectional design of the study in which there is no direct information on temporal relationship between events, these results could be compatible with three different hypotheses: that HTLV-1 increases the susceptibility to active TB, that TB increases the susceptibility to HTLV-1 infection, or that a third factor increases the probability to have both TB and HTLV-1. We can assume, however, that in at least 16 out of the 45 subjects in whom both events occurred, HTLV-1 infection preceded the TB episode. Because these subjects were children or siblings of infected subjects, they were most probably infected with HTLV-1 at an early age through mother-to-child transmission.
Protective immunity to M. tuberculosis depends on the correct function of T cells and their interaction with macrophages. HTLV-1 preferentially infects T cells and causes chronic T-cell dysfunction, which appears to result in an impaired immune response to specific pathogens [21]. Even though the mechanism and the impact of such immune suppression remain unknown, it makes an association between HTLV-1 and TB biologically plausible. Moreover, it is well documented that HTLV-1-infected individuals have a reduced delayed-type hypersensitivity response to PPD [9, 10, 22]. This hypo-responsiveness appears to be specific for PPD, since the response to phytohaemagglutinin, and mumps and C. albicans antigens is normal [9, 11].
In the case of strongyloidiasis, a parasitical infection clearly linked to HTLV-1, the immunological processes underlying the association are better understood [23]. Patients with strongyloidiasis and HTLV-1 have a stronger Th1 and a weaker Th2 response than patients with strongyloidiasis alone. This weak Th2 response interferes with mast cell degranulation, impairs the recruitment of eosinophils, and reduces the killing activity against the parasite [23, 24]. However, this suppression of protective Th2 responses by HTLV-1 is not a satisfactory explanation for its association with TB, where Th1 responses are protective. Another, tentative explanation is that HTLV-1 would cause a generalized immune suppression; but it then remains to be clarified why HTLV-1 is associated with some and not all infections known to be frequent among immune-suppressed subjects.
In several epidemiological studies, a high prevalence of HTLV-1 was found among TB patients [12, 13]. In a case-control study in Brazil, HTLV-1 was three times more frequent in TB patients than in hospital controls [14]. Moreover, HTLV-1 infection might also increase the severity of TB disease, as in two reports of hospitalized TB patients, co-infection with HTLV-1 was associated with mortality [25, 26]. On the other hand, a case-control study in Senegal did not find an association between both infections and in Papua New Guinea, none of 102 TB patients were infected with HTLV-1 [15, 16]. Our study differs from the latter two in several aspects: the geographical region (and possibly HTLV-1 subtype), the larger population size, the high prevalence of HTLV-1, and the fact that the control subjects without TB came from the same families as the cases.
In this family-based study population there is a risk of selection bias because both TB and HTLV-1 are known to cluster within families. However, because the inclusion of the family code in the multivariate model did not affect the results, we believe that the association between HTLV-1 and TB is real. In addition, there are also important advantages to family-based recruitment, particularly in the context of TB. The risk of TB is associated with poverty, crowding, room ventilation, and duration and intensity of exposure to an infectious TB case among many other factors [27]. In a community-based study, such factors could be important confounders for which it would be difficult to adjust. In this family-based study population, we can assume that the exposure to such risk factors is similar among HTLV-1-infected and -uninfected subjects, because they all come from families with at least one case of HTLV-1. Despite the similar socio-economic status and housing conditions, the HTLV-1-infected subjects report more frequently a history of TB (11%) than the uninfected (4%), and this association between HTLV-1 and TB history is independent of demographic and HTLV-1 risk factor variables, and cannot be explained entirely by clustering of HTLV-1 and/or TB within families.
A limitation of this study is that confirmatory tests could not be done on all EIA-positive samples. It is possible that some of the relatives considered to be HTLV-1 infected in our analysis were in fact HTLV-1 seronegative (false-positive EIA results). However, we believe that the number of false-positive EIA results must have been small, because both the specificity of the EIA tests (98–100%) and the prevalence of HTLV-1 in this population (32%) were high. Moreover, it seems unlikely that the frequency of false-positive results would differ systematically between the subjects with a history of TB and those without. Finally, if we excluded all relatives with unconfirmed EIA-positive tests from the analysis, the results were similar.
Theoretically, it is also possible that some of these unconfirmed seropositives were infected with HTLV-2. However, HTLV-2 rarely occurs outside the jungle areas of Peru and very few of the families included originated from the jungle. No cases of HTLV-2 infection were found in several surveillance studies in Lima and in the Peruvian Andes [5, 6, 28]. HTLV-2 infection is also uncommon at our institute: only 4/475 samples in which confirmation tests were done over the past 15 years, were typified as HTLV-2 (E. Gotuzzo et al., unpublished data).
The fact that we relied on patient interview to determine a history of active TB, based on history of TB treatment, is another possible source of misclassification. However, because TB treatment takes several months, we believe that it is an event that most people remember when specifically asked about, particularly since the introduction of DOTS in 1990 [29]. The fact that the 23 relatives who were interviewed afterwards easily remembered the place and time of treatment supports this view. The Peruvian TB Control Programme accepts few smear-negative patients for treatment, making it unlikely that many people received treatment without proof of TB [29].
The proportion of subjects with a history of TB was slightly higher among the HTLV-1-infected index cases (15%) than among their HTLV-1-infected relatives (11%); this difference was not significant. At the time of the interview, most index cases suffered from HTLV-1-associated conditions and in many cases, the interviewer knew or suspected the patient's positive HTLV-1 status. Both factors could have led to an increased recall of a history of TB. By contrast, in the case of the relatives, both the interviewer and the participants were unaware of HTLV-1 status at the time of data recording. Recall bias is, therefore, unlikely among the relatives, although an underestimation of the number of relatives with a history of TB is possible. In order to avoid recall bias, we focused this study on relatives rather than on index cases.
The information on the HIV status of the included relatives is limited. Nonetheless, out of the 26 subjects with a history of TB and known HIV status, only one was HIV infected. In addition, since we included HIV screening in the routine evaluation at our institute in September 2004, 109 HTLV-1-infected relatives have been tested and no one was HIV positive (E. Gotuzzo et al., unpublished data). The latter population is very similar to the relatives evaluated in this study. Furthermore, the HIV prevalence has remained relatively low in Peru, both in the general population (0·6% in 2005) and among TB patients (1·9% in 2004) [30, 31]. Therefore, although we cannot rule out the possibility of a confounding effect of HIV infection, we believe that this did not interfere substantially in our study.
In conclusion, our findings suggest that HTLV-1 infection may increase an individual's susceptibility to active TB. If this observation is confirmed through prospective studies, its potential impact on TB control strategies should be evaluated in areas with a high HTLV-1 prevalence. It would also be important to investigate which immune dysfunction contributes to this association, e.g. by studying CD4 T cell-macrophage interaction in HTLV-1-infected subjects. Even though the immune suppression caused by HTLV-1 is less profound than that caused by HIV, the consequences of an association between HTLV-1 and TB could be important in populations in which both infections are endemic.
ACKNOWLEDGEMENTS
We thank Carlos Seas for reviewing the manuscript, and Mónica Arbizú, Juana Dionicio, Viviana Quintana and Yessica Ramos for their efforts in visiting the patients. This study received financial support from the Directorate-General for Development Cooperation of the Belgian Government through a Framework Agreement with the Institute of Tropical Medicine of Antwerp and through the Flemish Inter-University Council (VLIR grant 1179).
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Manns A, Hisada M, La Grenade L. Human T-lymphotropic virus type I infection. Lancet. 1999;353:1951–1958. doi: 10.1016/s0140-6736(98)09460-4. [DOI] [PubMed] [Google Scholar]
- 2.de The G, Bomford R. An HTLV-I vaccine: why, how, for whom? AIDS Research and Human Retroviruses. 1993;9:381–386. doi: 10.1089/aid.1993.9.381. [DOI] [PubMed] [Google Scholar]
- 3.Marsh BJ. Infectious complications of human T cell leukemia/lymphoma virus type I infection. Clinical Infectious Diseases. 1996;23:138–145. doi: 10.1093/clinids/23.1.138. [DOI] [PubMed] [Google Scholar]
- 4.Murphy El et al. Respiratory and urinary tract infections, arthritis and asthma associated with HTLV-I and HTLV-II infection. Emerging Infectious Diseases. 2004;10:109–116. doi: 10.3201/eid1001.020714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sanchez-Palacios C et al. Seroprevalence and risk factors for human T-cell lymphotropic virus (HTLV-I) infection among ethnically and geographically diverse Peruvian women. International Journal of Infectious Diseases. 2003;7:132–137. doi: 10.1016/s1201-9712(03)90009-9. [DOI] [PubMed] [Google Scholar]
- 6.Alarcón JO et al. High endemicity of human T-cell lymphotropic virus type 1 among pregnant women in Peru. Journal of Acquired Immune Deficiency Syndromes. 2006;42:604–609. doi: 10.1097/01.qai.0000221680.52563.d5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.WHO Report. Geneva: World Health Organization; 2007. . Global tuberculosis control: surveillance, planning, financing (WHO/HTM/TB/2007.376). [Google Scholar]
- 8.Havlir DV, Barnes PF. Tuberculosis in patients with human immunodeficiency virus infection. New England Journal of Medicine. 1999;340:367–373. doi: 10.1056/NEJM199902043400507. [DOI] [PubMed] [Google Scholar]
- 9.Murai K et al. Suppression of delayed-type hypersensitivity to PPD and PHA in elderly HTLV-I carriers. Journal of Acquired Immune Deficiency Syndromes. 1990;3:1006–1009. [PubMed] [Google Scholar]
- 10.Welles SL et al. Decreased reactivity to PPD among HTLV-I carriers in relation to virus and hematologic status. International Journal of Cancer. 1994;56:337–340. doi: 10.1002/ijc.2910560307. [DOI] [PubMed] [Google Scholar]
- 11.Murphy EL et al. Delayed hypersensitivity skin testing to mumps and Candida albicans antigens is normal in middle-aged HTLV-I- and HTLV-II-infected U.S cohorts. AIDS Research and Human Retroviruses. 2001;17:1273–1277. doi: 10.1089/088922201750461339. [DOI] [PubMed] [Google Scholar]
- 12.Hanada S et al. The prevalence of human T-cell leukemia virus type I infection in patients with hematologic and nonhematologic diseases in an adult T-cell leukemia-endemic area of Japan. Cancer. 1989;64:1290–1295. doi: 10.1002/1097-0142(19890915)64:6<1290::aid-cncr2820640620>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 13.Olaleye DO et al. Type-specific immune response to human T cell lymphotropic virus (HTLV) type I and type II infections in Nigeria. American Journal of Tropical Medicine and Hygiene. 1994;50:479–486. doi: 10.4269/ajtmh.1994.50.479. [DOI] [PubMed] [Google Scholar]
- 14.Marinho J et al. Increased risk of tuberculosis with human T-lymphotropic virus-1 infection: a case-control study. Journal of Acquired Immune Deficiency Syndromes. 2005;40:625–628. doi: 10.1097/01.qai.0000174252.73516.7a. [DOI] [PubMed] [Google Scholar]
- 15.Kaplan JE et al. Low prevalence of human T-lymphotropic virus type I among patients with tuberculosis in Senegal. Journal of Acquired Immune Deficiency Syndromes. 1994;7:418–420. [PubMed] [Google Scholar]
- 16.Seaton RA. Tuberculosis and human T-cell lymphotropic virus type 1 infection. Clinical Infectious Diseases. 1997;24:1026. doi: 10.1093/clinids/24.5.1026. [DOI] [PubMed] [Google Scholar]
- 17.Matsuzaki T et al. Diseases among men living in human T-lymphotropic virus type I endemic areas in Japan. Internal Medicine. 1993;32:623–628. doi: 10.2169/internalmedicine.32.623. [DOI] [PubMed] [Google Scholar]
- 18.Kohno S et al. Epidemiology of HTLV-I carriers in Hirado Island and virological and immunological investigation of HTLV-I associated pulmonary disease. Nihon Kyobu Shikkan Gakkai Zasshi. 1992;30:763–769. [PubMed] [Google Scholar]
- 19.Hanley JA et al. Statistical analysis of correlated data using generalized estimating equations: an orientation. American Journal of Epidemiology. 2003;157:364–375. doi: 10.1093/aje/kwf215. [DOI] [PubMed] [Google Scholar]
- 20.R Develompent Core Team R Foundation for Statistical Computing; Vienna, Austria: 2007. . R: a language and environment for statistical computing. ). Accessed 20 August 2007. [Google Scholar]
- 21.Suzuki M et al. Modulation of T-cell responses to a recall antigen in human T-cell leukemia virus type 1-infected individuals. Clinical and Diagnostic Laboratory Immunology. 1999;6:713–717. doi: 10.1128/cdli.6.5.713-717.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hisada M et al. Gender difference in skin reactivity to purified protein derivative among carriers of HTLV-I in Japan. Journal of Acquired Immune Deficiency Syndromes. 1999;22:302–307. doi: 10.1097/00126334-199911010-00013. [DOI] [PubMed] [Google Scholar]
- 23.Hirata T et al. Impairment of host immune response against Strongyloides stercoralis by human T cell lymphotropic virus type 1 infection. American Journal of Tropical Medicine and Hygiene. 2006;74:246–249. [PubMed] [Google Scholar]
- 24.Carvalho EM, Da Fonseca PA. Epidemiological and clinical interaction between HTLV-1 and Strongyloides stercoralis. Parasite Immunology. 2004;26:487–497. doi: 10.1111/j.0141-9838.2004.00726.x. [DOI] [PubMed] [Google Scholar]
- 25.Pedral-Sampaio DB et al. Co-infection of tuberculosis and HIV/HTLV retroviruses: frequency and prognosis among patients admitted in a Brazilian hospital. Brazilian Journal of Infectious Diseases. 1997;1:31–35. [PubMed] [Google Scholar]
- 26.Verdonck K et al. Association between infection with human T cell lymphotropic virus type I (HTLV-I) and mortality in hospitalized patients with tuberculosis. Revista Medica Herediana. 2004;15:197–202. [Google Scholar]
- 27.Gustafson et al. Tuberculosis in Bissau: incidence and risk factors in an urban community in sub-Saharan Africa. International Journal of Epidemiology. 2004;33:163–172. doi: 10.1093/ije/dyh026. [DOI] [PubMed] [Google Scholar]
- 28.Zurita S et al. Prevalence of human retroviral infection in Quillabamba and Cuzco, Peru: a new endemic area for human T cell lymphotropic virus type 1. American Journal of Tropical Medicine and Hygiene. 1997;56:561–565. doi: 10.4269/ajtmh.1997.56.561. [DOI] [PubMed] [Google Scholar]
- 29.Suarez PG et al. The dynamics of tuberculosis in response to 10 years of intensive control effort in Peru. Journal of Infectious Diseases. 2001;184:473–478. doi: 10.1086/322777. [DOI] [PubMed] [Google Scholar]
- 30.UNAIDS Report. Geneva: Switzerland: 2006. p. 429. . Report on the global AIDS epidemic. Joint United Nations Programme on HIV/AIDS (UNAIDS/06.20E), p. [Google Scholar]
- 31.Ministerio de Salud 2005 Lima, Peru: Ministerio de Salud; 2005. p. 30. . Evaluación de la Estrategia Sanitaria Nacional de Prevención y Control de la Tuberculosis; año 2004; informe del seminario taller. , p. ). Accessed 9 September 2007. [Google Scholar]