

Abstract
Previous studies of schizophrenia have suggested a linkage between neuropsychological (NP) deficits and hippocampus abnormality. The relationship between hippocampus volume and NP functioning was investigated in 24 patients with chronic schizophrenia and 24 matched healthy controls. Overall intracranial, white and gray matter, and anterior (AH) and posterior (PH) hippocampus volumes were assessed from magnetic resonance images (MRI). NP domains of IQ, attention, and executive function were also evaluated with respect to volumetric measures. It was hypothesized that AH and PH volumes and episodic memory scores would be positively associated in controls and that the schizophrenia group would depart from this normative pattern. NP functioning was impaired overall and AH volume was smaller in the schizophrenia group. In the controls, the hippocampus–memory relationships involved AH and PH, and correlations were significant for verbal memory measures. In the schizophrenia group, positive correlations were constrained to PH. Negative correlations emerged between AH and verbal and visual memory measures. For both groups, cortical volume negatively correlated with age, but a negative correlation between age and hippocampus volume was found only in the schizophrenia group. In this sample of adults with schizophrenia, atypical relationships between regional hippocampus volumes and episodic memory ability were found, as was an atypical negative association between hippocampus volume and age.
Keywords: Magnetic resonance imaging, Cognition, Neuropsychology, Memory, Temporal lobe, Antipsychotic agents
Introduction
Declarative, episodic, and working memory have long been recognized as being dependent on the function of an intact hippocampus, a medial temporal lobe structure necessary for encoding and consolidating new memories. Schizophrenia is a disorder characterized by both episodic memory deficits and hippocampus abnormality. Because selective memory impairment has been observed in never-medicated patients experiencing first-episode schizophrenia, episodic memory has been posed as a core deficit of the disorder rather than an effect of chronicity or antipsychotic medication (Saykin et al., 1994). Episodic memory deficits appear to be present in schizophrenia before the onset of frank psychosis. In a study of patients at high risk of developing psychosis (predominantly schizophrenia), impairments in the Visual Reproduction and Logical Memory subtests of the Wechsler Memory Scale-Revised (WMS-R) differentiated patients who went on to develop psychosis within the next 12 months from those who did not (Brewer et al., 2005). While it is possible for lower scores on neuropsychological tests of memory to be secondary to any number of environmental or individual attributes, episodic memory impairment in schizophrenia is not commensurate with global impairment, nor is it attributable to lack of motivation, attention, or cooperation (Gold et al., 1992; Saykin et al., 1991; Tamlyn et al., 1992).
Functional neuroimaging has linked hippocampus dysfunction to impaired performance on memory tasks in schizophrenia. In a positron emission tomography (PET) study, Heckers et al. (1998) identified lesser hippocampus activity in patients than controls during attempts to recall studied words. In a functional magnetic resonance imaging (fMRI) study, controls exhibited greater activation than patients in left anterior hippocampus during encoding and in hippocampus bilaterally during recognition (Jessen et al., 2003). Functional impairment related to the hippocampus extends to the ability to comprehend relationships and draw inferences, as demonstrated by a selective deficit in discrimination accuracy when cognitive flexibility is required, which has been observed in schizophrenia using fMRI (Öngur et al., 2006). Using a similar relational-memory task, Hanlon et al. (2005) directly assessed hippocampus activity with magnetoencephalography (MEG), reporting abnormal right hemisphere processing of nonverbal stimuli accompanied by a possibly compensatory, left-lateralized activation in schizophrenia.
Structural abnormalities of the medial temporal lobe, which includes the hippocampus, are among the most robust findings in schizophrenia research. A number of studies have reported smaller volume of the medial temporal lobe in schizophrenia (Bogerts et al., 1993; Gur et al., 2000; McCarley et al., 1999; Wright et al., 2000), particularly in the left hemisphere (DeLisi et al., 1991; Honea et al., 2005; Shenton et al., 1992). However, while hippocampus abnormality is consistently found, the precise nature of the results has varied. Meta-analyses have posited that smaller hippocampus volume is equivalent across hemispheres (Nelson et al., 1998), even when limited to studies of first-episode patients (Steen et al., 2006). However, other first-episode studies have resulted in findings of significant left-less-than-right hippocampus asymmetry (Bogerts et al., 1990; Hirayasu et al., 1998). In a longitudinal study, Velakoulis et al. (2006) demonstrated hippocampus volume deficits bilaterally in chronic schizophrenia, in the left hemisphere only in first-episode schizophrenia, and not at all in schizophreniform psychosis. It is also important to note that there have been scattered reports of null findings with regard to hippo campus volume in schizophrenia. For example, Marsh et al. (1997) reported no group difference in hippocampal volume in an inpatient sample with severe and chronic schizophrenia. Because of the variability in group differences across reports, the etiological role of hippocampal anomaly in schizophrenia and its association with subsequent symptoms and course of the disorder remains a critical area for research (White et al., 2008).
With some degree of hippocampal volume deficits in schizophrenia well established but the nature and mechanisms of its functional consequences unclear, attention is turning to localizing hippocampus volume decrements along the anterior-posterior axis. One study confirmed the presence of overall hippocampus volume deficits in schizophrenia but maintained that the loss was diffuse rather than topographically specific (Weiss et al., 2005). However, Narr et al. (2004) made a strong argument for factoring regional specificity into hippocampus measurements in a study that demonstrated volume deficits localized to midbody and anterior hippocampus in first-episode schizophrenia. Consistent with Narr et al.'s finding, smaller anterior hippocampus volumes have been observed in both first-episode and chronic schizophrenia (Lieberman et al., 2001; Pegues et al., 2003; Szeszko et al., 2003). Other studies have found deficits localized to posterior hippocampus in chronic schizophrenia (Narr et al., 2001) and in first-episode patients (Hirayasu et al., 1998).
The relationship of neuropsychological function to structural abnormality in the hippocampus is under debate. Lack of a relationship between hippocampus volume and episodic memory in people with schizophrenia or controls has been reported by some studies (DeLisi et al., 1991; Torres et al., 1997). Gur et al. (2000), on the other hand, found a positive correlation between gray matter volume of the hippocampus and episodic memory scores across patients and controls of both sexes. This finding is supported by other studies reporting similar correlations between verbal memory and left hippocampus volume (Goldberg et al., 1994; Seidman et al., 2002) or amygdala-anterior hippocampus volume (O'Driscoll et al., 2001) in people with schizophrenia, their relatives, and controls. However, some investigations of structure-function relationships have found differential patterns of correlations between hippocampus volume and verbal IQ or verbal or visual memory in controls and people with schizophrenia (Kuroki et al., 2006; Sachdev et al., 2000; Sanfilipo et al., 2002; Toulopoulou et al., 2004). Findings of differential patterns of correlations for patients and controls are thought to indicate a loss of normal structure-function relationships, possibly arising from aberrant neurodevelopment.
One reason for discrepancies among volumetric studies may be that critical hippocampus subregions are not being discriminated, as few studies have combined neuropsychological assessment with hippocampus subregion measurements as discussed earlier. Anterior hippocampus volume deficits have been correlated with decrements in executive and motor function, but not memory, in first-episode schizophrenia (Bilder et al., 1995), with the effect present for men but not for women in a similar study (Szeszko et al., 2002). Given the substantial evidence for episodic memory dysfunction and hippocampus volume deficits in schizophrenia, further investigation taking subregional measurements into account seems warranted.
The present study was conceived to investigate how measures of cognitive function track structural abnormalities in specific hippocampus subregions. Based on prior research, it was expected that (1) episodic memory would be impaired and (2) hippocampus volume would show deficits in the schizophrenia group. It was also predicted that (3) there would be positive correlations between hippocampus volumes and episodic memory scores in the control group, establishing an assemblage of correlational relationships that represent normal brain-behavioral functioning. It was further predicted that (4) correlations between regional hippocampus volumes and episodic memory scores would differentiate the groups, supporting the presence of abnormal brain-behavioral relationships in schizophrenia. Demographic variables that are known to affect hippocampus volume, such as age and gender, were also investigated.
Method
Participants
Participants in this study were 24 schizophrenia patients and 24 healthy control subjects matched for age, education, and sex (see Table 1). Group membership was determined with the Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV; First et al., 1996). No subject had a history of head injury, neurological disorder, or severe medical illness.
Table 1.
Sample demographics
| Control | Schizophrenia | Statistic | |
|---|---|---|---|
| Age | 41.74 | 40.09 | t =.52 (p =.61) |
| Education (in years) | 13.56 | 12.47 | t = 1.47 (p =.15) |
| Sex | |||
| Male | 16 | 20 | χ2 = 1.78 (p =.32) |
| Female | 8 | 4 |
The schizophrenia group consisted of volunteers and referrals who were relatively stable patients, well known to their providers. They met predetermined criteria for clinical stability, as they had been treated with the same antipsychotic medications for at least 3 months and had had no inpatient stays during the past year. Absence of other current psychiatric disorders was determined using the SCID-CV. Patients with schizophrenia were all taking antipsychotic medications, either haloperidol (n = 6), olanzapine (n = 4), risperidone (n = 5), clozapine (n = 4), aripiprazole (n = 2), or quetiapine (n = 3).
The control group consisted of healthy volunteers recruited via advertisements in local newspapers. Control subjects were screened for the presence of Axis-I psychopathology via SCID-CV with a licensed clinical psychologist (Thoma) or with a psychology graduate student under his direct supervision. Axis II psychopathology was ruled out with a diagnostic clinical interview with a licensed clinical psychologist (Thoma) if necessary. If there was a question of the presence of schizotypal or schizoid symptoms, scores on the Social Anhedonia Scale (Chapman et al., 1994) and the Magical Ideation Scale (Eckblad & Chapman, 1983) were reviewed. During the clinical interview, potential control subjects were asked if they had a first-degree relative with schizophrenia or other psychotic disorder, and if so, they were not included in the study.
Institutional Review Board approval was obtained prior to running subjects, and subjects were informed that they could leave the study at any time. Appropriate informed consent was obtained from all subjects, and data was obtained in compliance with institutional regulations.
Hippocampus volume data from these subjects was previously published elsewhere as part of an analysis of psychophysiological anomalies (Thoma et al., 2008).
Procedures
Magnetic resonance images
Three-dimensional structural magnetic resonance images (MRI), T1 weighted, were collected with a 1.5 Picker Edge Imager at the NMVAHCS Magnetic Source Imaging center. A gradient echo 3-D sagittal sequence with parameters TR = 15 ms; TE = 4.4 ms; FOV = 256 mm; 192 × 256 matrix, flip angle = 25; slice thickness = 1.5 mm, with no gap, was used.
Structural MRI analysis
The method used for this hippocampus volumetric analysis was first described in detail elsewhere (Thoma et al., in press). MRIs were first resliced into coronal images of 1.0 mm thickness (Figure 1a). The skull was then stripped from each MRI image using Brain Extraction Tool software (BET: fMRIB Image Analysis Group, Oxford, UK). Intracranial volume (ICV) was calculated from the mask produced from this program. Images were then segmented using an automated k-means clustering segmentation algorithm, and the volumes of gray matter (GM; not including cerebellum; see Figure 1b), white matter (WM; not including cerebellum), cerebrospinal fluid (CSF), and total ICV (including cerebellum) were determined by the number of pixels in each of their respective clusters (Petropoulos et al., 1999). Pixels that could not be assigned exclusively to GM or CSF were considered partial volume (PV). The number of PV pixels was divided in half and then added to the GM for a final count.
Fig. 1.
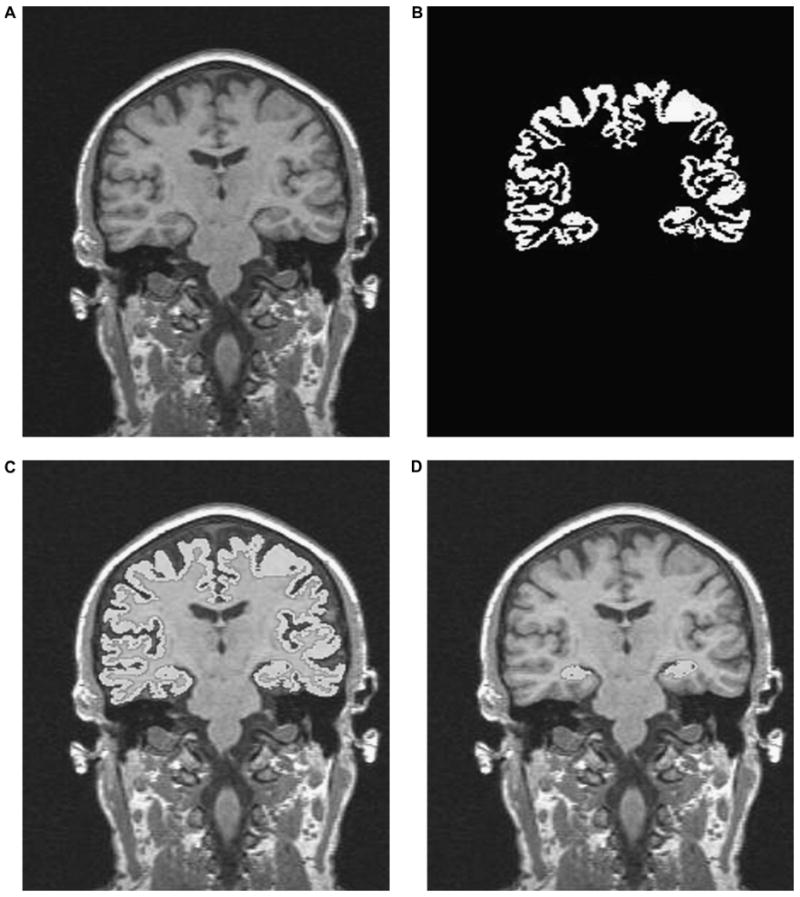
A pictorial representation of the steps involved in the hippocampus quantification routine. (1a) Sagittal MRI series is resliced into 1-mm coronal images. (1b) An example of cortical gray matter segmentation. (1c) Cortical mask “overlay” on T1 image. (1d) Hippocampus tissue extracted by trained rater utilizing manual editing to separate the body of the hippocampus from the cortex.
The k-means algorithm segmented GM from WM to assist raters in selecting the hippocampus, and as a result hippocampus WM was excluded from the overall hippocampus volume measurement (Figure 1c). Two independent raters used interactive software (Driscoll, et al., 2003) to conduct volumetric assessment of the hippocampus using the already k-means segmented coronal T1-weighted images. The software was designed to interact with the segmented imaging data for quantification and allows the user to select a segmented brain section. The user is able to magnify the area of interest to remove sections of segmented data from the volumetric analysis and allow the user to specify brain structures and easily quantify the selection via a pixel-counting algorithm (Figure 1d).
Raters followed the anatomical guidelines outlined by Watson et al. (1992) to measure hippocampus, except in regard to the posterior hippocampus definition. Watson et al. (1992) defined the most posterior slice as where the crux of the fornix separated from the hippocampus. This method, however, eliminates the most posterior slices of the hippocampus. Since active hippocampus MEG source dipoles have been previously found on these most posterior slices of the hippocampus (Hanlon et al., 2005), they were included in the present measurements. Consequently, the most posterior slice was defined in this study as the slice in which the hippocampus connects laterally to the lateral ventricle and medially to the midline. Hippocampus volume was determined for total, right, left, anterior (anterior 9 slices), and posterior (posterior 9 slices) (Maguire et al., 2000). Total hippocampus volume was the sum of the measurements collected for the images available, around 40 (1.0 mm) slices. The mean measurements from the two raters were used. Inter-rater reliability between two raters was established in a subset of 20 hippocampi (alpha =.82).
Neuropsychological battery
While the primary hypotheses focused on the relationship between hippocampus volume and episodic memory, a broad neuropsychological battery was administered to assess a wide array of cognitive functions, including intelligence, attention, working memory, and executive functioning, in addition to episodic memory function. Intelligence was assessed with the Shipley Institute for Living Scale (Shipley, 1940), attention with the Conners' Continuous Performance Test (CPT; Conners, 2000), working memory with the auditory consonant trigrams test, (ACT) as well as Digit Span Forward (DSF) and Back (DSB), and executive functioning with the Trail Making Test (Trails A & B). For the episodic memory assessment, the Wechsler Memory Scale-Revised (WMS-R) Logical Memory I (LM I) and II (LM II) and Visual Reproduction I (VR I) and II (VR II) subtests were used (Wechsler, 1987).
Results
Hypothesis 1
The schizophrenia group was impaired across all neuropsychological tests (p-values ranged from <.001 to .034) with two exceptions. There was a marginal group difference for digit span forward (p =.052), and no difference for digit span back (p=.187; see Figure 2).
Fig. 2.
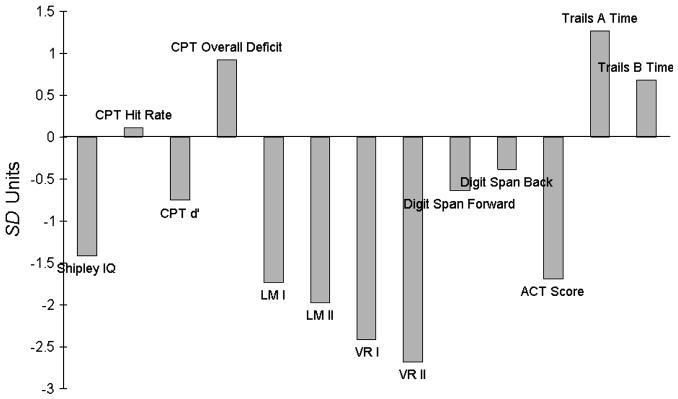
Standardized representation of cognitive deficits in schizophrenia. Each bar represents mean schizophrenia group score as a z -score relative to normal control mean and standard deviation. For most tests, negative scores indicate a schizophrenia group deficit. Trails A, Trails B, and CPT Overall Deficit measures reflect schizophrenia group deficit in terms of increased time on task.
Hypothesis 2
Group differences in hippocampus substructure volumes were assessed using a mixed-model multivariate analyses of variance (MANOVA), with Hemisphere (right and left) × Region (anterior and posterior hippocampus) entered as repeated measures. Overall hippocampus volume was smaller in the schizophrenia group than in controls [Group main effect, F(1, 46) = 6.689, p =.013]. Across groups, anterior hippocampus volume was larger than posterior hippocampus volume [Region main effect, F(1, 46) = 254.554, p < .001], and left hippocampus was larger than right [Hemisphere main effect, F(1, 46) = 4.195, p =.046].
The Group × Region interaction was marginally significant, F (1, 44) = 3.122, p =.084, two-tailed test, and investigation of this predicted interaction using simple-effects tests demonstrated a trend toward smaller anterior hippocampus in the schizophrenia group than in controls, t(46) = 2.701, p =.010, with no group difference for posterior hippocampus (p =.821). No other main effects or interactions approached significance.
Hypotheses 3 and 4
Table 2 shows partial correlations between hippocampus subregional volumes and neuropsychological memory test scores for each group, controlling for ICV. Groups did not differ in ICV, GM, or WM, so using ICV as a covariate is appropriate (Miller & Chapman, 2001). In the control group, LM I and LM II scores correlated positively with right anterior and left posterior hippocampus volumes. No significant brain-behavior correlations associated with VR I or VR II emerged for this group.
Table 2.
Correlations between neuropsychological tests and hippocampus subregions
| Test | Right anterior | Left anterior | Right posterior | Left posterior |
|---|---|---|---|---|
| Control group (n = 24) | ||||
| LM I | .436** | .052 | .268 | .497** |
| LM II | .494** | .048 | .281 | .414** |
| VR I | .020 | .095 | −.097 | .224 |
| VR II | .184 | .352 | .001 | .022 |
| Schizophrenia group (n = 24) | ||||
| LM I | −0.471**a | −0.284 | 0.189 | 0.250 |
| LM II | −0.298 | −0.179 | 0.108 | 0.140b |
| VR I | −0.529**a | −0.246 | 0.365*a | 0.650***a |
| VR II | −0.450**a | −0.271b | 0.427**a | 0.509**a |
Note. Values represent partial correlations controlling for intracranial volume (ICV).
LM I, LM II = Wechsler Memory Scale-Revised (WMS-R) Logical Memory scores;VR I, VR II = WMS-R Visual Reproduction scores.
Group difference in correlations, p < .05.
Group difference in correlations, p < .10.
p < .10.
p < .05.
p < .01.
In the schizophrenia group, the pattern of correlations was markedly different. Only a single correlation was noted with LM: LM I was negatively correlated with right anterior hippocampus volume. VR I and VR II were also negatively correlated with right anterior hippocampus volume. VR I and VR II were positively correlated with bilateral posterior hippocampus volumes. See Figure 3 for scatterplots of relationships between episodic memory scores and hippocampus subregions.
Fig. 3.
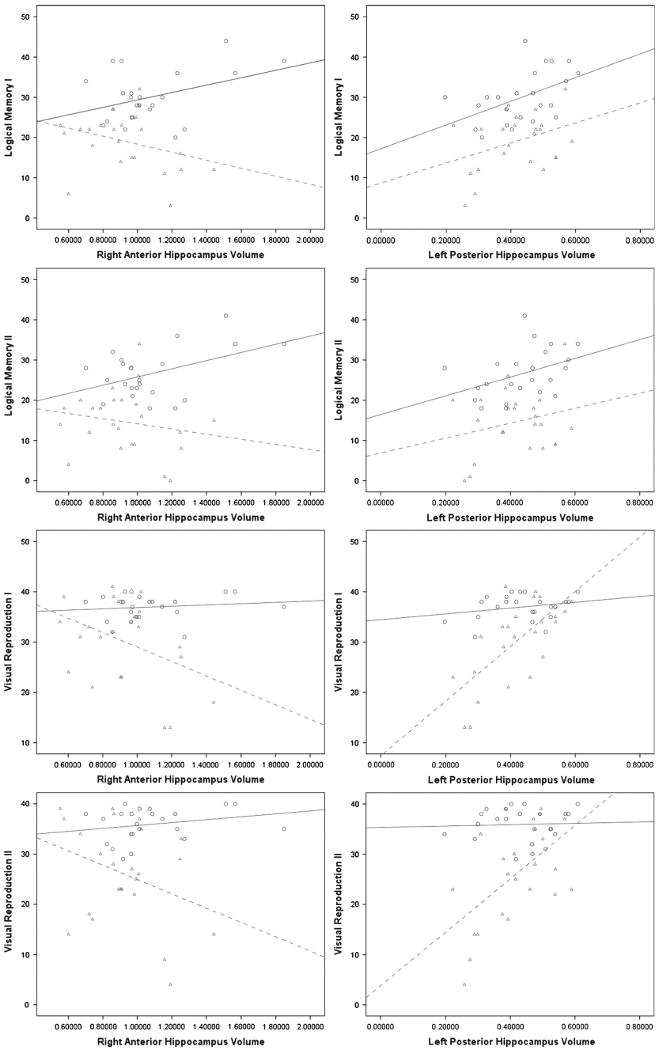
The most dramatic correlational group differences were between memory test scores and right anterior and left posterior hippocampus. The scatterplots depict bivariate correlations between the variables (hippocampus volumes are in cc). Blue = control group, green = schizophrenia group.
Cohen's statistical tables were used to test group differences between brain-behavior correlations (Cohen, 1988). Group correlational differences fell into two basic clusters. First, the schizophrenia group correlations between right anterior hippocampus volume and episodic memory test scores (i.e., LM I, VR I, VR II) were significantly different from those in the control group. In this cluster, the schizophrenia group correlations were strongly negative versus positive or absent in controls. Second, bilateral posterior hippocampus volume correlations with VR I and VR II were significantly different, in this case more positive in the schizophrenia group than those correlations in the control group. In addition, differences between correlations for left anterior volume and VR II and left posterior volume and LM II approached significance (p < .10).
To provide some context for the findings presented in Table 2, Tables 3a and 3b show the zero-order correlations between most test scores derived from the neuropsychological battery and all brain regional volumetric data assessed for this study. Tables 4a and 4b show partial correlation coefficients between test scores and hippocampus regions controlling for gray matter volume.
Table 3.
| Table 3a. Bivariate correlations between neuropsychological tests and hippocampus regional volumes, overall WM and GM, and ICV for the control group (n =24) | |||||||
|---|---|---|---|---|---|---|---|
| Test | Right anterior | Left anterior | Right posterior | Left posterior | White matter | Gray matter | ICV |
| Shipley | .082 | .092 | .050 | .025 | .395* | .278 | .529*** |
| CPT d' | −.188 | −.294 | −.209 | .263 | −.068 | −.005 | −.061 |
| CPT Overall | .112 | −.046 | .191 | .137 | −.274 | −.201 | −.201 |
| LM I | .383* | −.019 | .256 | .481** | −.111 | −.137 | −.113 |
| LM II | .449** | .004 | .272 | .404* | .049 | −.108 | −.080 |
| VR I | .254 | .318 | −.048 | .220 | .429** | .220 | .424 |
| VR II | .276 | .420** | −.013 | .091 | .101 | .251 | .234 |
| DSF | .214 | .133 | .133 | .028 | .085 | .137 | .175 |
| DSB | −.041 | .192 | −.098 | .013 | .168 | .086 | .218 |
| ACT | .262 | .144 | .441** | .262 | .334 | .292 | .376* |
| Trails A | −.264 | −.120 | −.383* | −.132 | −.238 | −.332 | −.163 |
| Trails B | −.151 | .148 | −.311 | .038 | −.390* | −.169 | −.231 |
| Table 3b. Bivariate correlations between neuropsychological tests and hippocampus regional volumes, overall WM and GM, and ICV for the schizophrenia group (n =24) | |||||||
| Test | Right anterior | Left anterior | Right posterior | Left posterior | White matter | Gray matter | ICV |
| Shipley | −.463** | −.248 | .318 | .312 | .173 | .153 | .208 |
| CPT d′ | −.387 | −.322 | −.177 | .096 | .037 | −.238 | −.117 |
| CPT Overall | .270 | −.001 | −.132 | −.424** | −.336 | −.231 | −.276 |
| LM I | −.203 | −.019 | .334 | .266 | .321 | .238 | .343 |
| LM II | −.172 | .092 | .100 | .117 | .328 | .167 | .284 |
| VR I | −.398* | −.065 | .393* | .685** | .278 | .233 | .285 |
| VR II | −.330 | −.092 | .452* | .560** | .301 | .244 | .274 |
| DSF | −.278 | .071 | −.008 | .208 | .239 | .202 | .323 |
| DSB | −.350* | −.061 | .035 | .190 | .329 | .213 | .323 |
| ACT | −.477** | .153 | .296 | .197 | −.003 | −.017 | −.066 |
| Trails A | .404** | .180 | −.256 | −.602** | −.134 | −.466** | −.329 |
| Trails B | .350* | .136 | −.153 | −.436** | −.104 | −.369* | −.229 |
Note. ICV = intracranial volume, GM = gray matter, WM = white matter, CPT Overall = Continuous Performance Test Overall Deficit, CPT d′ = CPT detectability, DSF = Digit Span Forward, DSB = Digit Span Back, ACT = Auditory Consonant Trigrams, Trails A, B = Trail-Making Tests A & B.
p < .10.
p < .05.
p < .01.
Table 4.
| Table 4a. Partial correlations between neuropsychological tests and hippocampus regional volumes for the control group, controlling for GM (n =24) | |||||||
|---|---|---|---|---|---|---|---|
| Test | Right anterior | Left anterior | Right posterior | Left posterior | |||
| Shipley | .127 | .215 | .043 | .041 | |||
| CPT d′ | −.215 | −.195 | −.179 | .212 | |||
| CPT Overall | .236 | .008 | .138 | .172 | |||
| LM I | .408** | .142 | .262 | .411** | |||
| LM II | .393* | .075 | .243 | .309 | |||
| VR I | .112 | .104 | −.077 | .366 | |||
| VR II | .180 | .303 | .000 | .149 | |||
| DSF | .159 | .196 | .135 | .008 | |||
| DSB | −.120 | .089 | −.119 | .025 | |||
| ACT | .129 | .076 | .425** | .272 | |||
| Trails A | −.246 | −.106 | −.278 | −.056 | |||
| Trails B | −.247 | .179 | −.080 | −.126 | |||
| Table 4b. Partial correlations between neuropsychological tests and hippocampus regional volumes for the schizophrenia group, controlling for GM (n = 24) | |||||||
| Test | Right anterior | Left anterior | Right posterior | Left posterior | |||
| Shipley | −.529** | −.380* | −.230 | .174 | |||
| CPT d′ | −.373* | −.240 | −.137 | .210 | |||
| CPT Overall | .330 | .126 | −.050 | −.304 | |||
| LM I | −.391* | −.184 | .099 | .149 | |||
| LM II | −.243 | −.092 | .057 | .097 | |||
| VR I | −.466** | −.183 | .253 | .486** | |||
| VR II | −.404** | −.213 | .293 | .330 | |||
| DSF | −.323 | .029 | −.075 | .101 | |||
| DSB | −.406** | −.186 | −.047 | .045 | |||
| ACT | −.495** | −.178 | .250 | .146 | |||
| Trails A | .531*** | .430** | −.031 | −.235 | |||
| Trails B | .432** | .285 | .071 | −.050 | |||
p < .10.
p < .05.
p < .01.
Demographic Variables
As a result of the nature of the population from which these samples were drawn (i.e., a VA population consisting largely of middle-aged veterans), only 13 women were included in the study. When sex was considered as a covariate in the mixed model MANOVA described earlier, there was no main effect (p =.381) or significant interactions between sex and hippocampus volume variables.
There was a group difference in how age related to hippocampus volume [Group × Age interaction, F(2, 45) = 4.513, p =.016]. Further correlational analysis indicated that there was no effect of age on hippocampus volumes for control subjects but that age was negatively correlated with left anterior hippocampus (r(24) = -.406, p =.049) and marginally correlated with right posterior (r(24) = -.382, p =.065) and left posterior (r (24) = -.383, p =.065) hippocampus volumes in the schizophrenia group (see Figure 4).
Fig. 4.
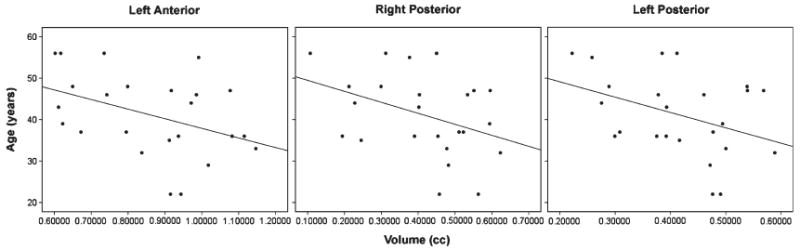
Scatterplots represent the significant correlations between age and hippocampus subregional volumes in the schizophrenia group.
Consistent with the prevailing literature, GM volume correlated negatively with age for both groups. In a regression, no effect was found for Group, or for the Group × Age interaction term, indicating that GM volume decreased equally with age for control and schizophrenia groups. A series of hierarchical regressions was used to investigate whether this generalized GM diminution might account for the age–hippocampus volume correlations in the schizophrenia group. With age used as a dependent variable, and GM as a lone predictor variable, the overall regression was significant for the schizophrenia group (R2 =.386, p =.001). However, there was no additional variance accounted for when hippocampus volumes were added as predictors. Taken together, these analyses suggest that age–hippocampus volume correlations in schizophrenia are proportionate to age–GM correlations, whereas in controls, age predicts only smaller GM and there was no evidence of a correlation with hippocampus volume.
The mean number of years since schizophrenia symptom onset was 16.18 (SD = 8.34) and was considered as a demographic covariate for the schizophrenia group. To investigate an effect for time since first diagnosis, a mixed-model MANOVA was used with Region and Hemisphere as repeated measures and Years since symptom onset entered as a covariate. There was a three-way Hemisphere × Region × Years interaction, F(1, 19) = 7.233, p =.015. Post-hoc investigation with correlations suggested that Years was most significantly correlated with right hemisphere posterior hippo campus volume (r = −.505, p =.017).
To investigate possible medication effects, Medication type (typical, atypical) was entered as a covariate for the schizophrenia group. Although there was no main effect of Medication type, there was a signification Medication type × Region interaction, F(1, 22) = 5.267, p =.032; schizophrenia subjects taking atypical antipsychotic medications had larger anterior hippocampus and smaller posterior hippocampus than those taking typical antipsychotic medications (see Figure 5). When Medication type was entered as a covariate in the correlation matrix relating neuropsychological tests and hippocampal subregions, there were no significant changes from Table 2 evident in the pattern or size of the correlations.
Fig. 5.
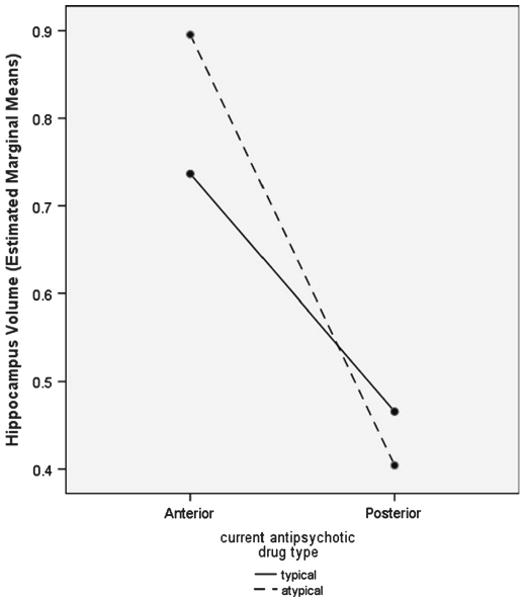
Schizophrenia patients taking atypical antipsychotic medications had larger anterior hippocampi and smaller posterior hippocampi than those taking typical antipsychotic medications.
Discussion
Associations between hippocampus and memory are one of the core findings in neuropsychology (Milner, 2005). Both hippocampus abnormality and normal variability in volume have been linked to episodic memory measures. Because hippocampus volume deficits are among the most consistent findings in schizophrenia, a key focus of this study was to better characterize the relationship between hippocampus subregion volume and episodic memory function in healthy control subjects and patients with schizophrenia.
The first hypothesis was that the schizophrenia group would be impaired on neuropsychological measures relative to controls. Across measures and presumed cognitive domains, with a single exception, neuropsychological function was impaired in the schizophrenia group, a finding consistent with the majority of studies investigating the extent of cognitive changes associated with schizophrenia (e.g., Goldberg et al., 1993; Gruzelier et al., 1988; Saykin et al., 1991; 1994). The exception was for the digit span backward portion of the digit span test. Further analysis indicated that a single, high-scoring subject in the schizophrenia group accounted for the lack of group difference, as he achieved the highest score of either group. With his data removed from the analysis, patients scored significantly worse than controls on the digit span backward test.
The second hypothesis was that hippocampus volume would be smaller in the schizophrenia group. This hypothesis was supported, but of particular interest was the finding that the group difference was specific to bilateral anterior (not posterior) hippocampus. Overall intracranial, GM, and WM volumes were statistically equivalent across groups, although these three measures were smaller in mean size. With increased power, that is, larger sample size, group differences may have been found. Certainly, such a finding would not be unusual and would be well supported by the prevailing literature (Andreone et al., 2007; Sanfilipo et al., 2000; 2002; Steen et al., 2006; Zipursky et al., 1998). In any case, however, none of these measures accounted for the group difference in anterior hippocampus when considered as statistical covariates, indicating that smaller hippocampus volume is not part of a more general effect for GM or WM volume, but is specific to anterior hippocampus.
Because of the importance of an intact hippocampus for episodic memory, the third hypothesis predicted that hippocampus volumes would positively correlate with episodic memory scores. Again, there was support for this hypothesis, but the answer was more complicated than initially supposed. Correlations between hippocampus and episodic memory scores were first evaluated in healthy control subjects to establish a frame of reference. In the control group, strong positive correlations between the size of hippocampus and episodic memory test performance were observed only for LM I and LM II, tests of immediate and delayed verbal memory. Verbal memory is often thought to be later-alized to the left hemisphere, yet positive correlations with both left posterior and right anterior hippocampus volumes indicate that current models of episodic memory may be oversimplified. Certainly, frontotemporal interaction and intrahippocampus circuitry are critical to the encoding, storage, and retrieval of relevant information. VR I and VR II, tests of memory for nonverbal information, evinced no correlations with any measure of hippocampus volume in controls.
A fourth prediction was that the pattern of correlations established in controls would not hold for the schizophrenia group, and this hypothesis was supported. Patterns of correlations between episodic memory scores and hippocampus volumes differed markedly according to diagnosis. Bilateral posterior hippocampus volumes correlated positively with performance on VR I and VR II in the schizophrenia group. Since mean posterior hippocampus volumes did not differ by group, this finding suggests that hippocampus organization in service to episodic memory is quite different in schizophrenia. Perhaps most damaging to a simple “bigger-is-better” model was the finding that right anterior hippocampus volume was negatively correlated with both verbal and nonverbal memory functions (i.e., LM I, VR I, and VR II) in schizophrenia. That these partial correlations were weaker and generally nonsignificant (but still negative) in bivariate correlations suggests that the effect is partially, but not entirely, accounted for by overall brain size in schizophrenia. It may be that smaller size reflects more efficient design or some developmental anomaly associated with schizophrenia. For example, anomalous schizophrenia neurodevelopment is thought to involve neurodevelopmental delays interacting with a fixed “developmental window” (see Yeo et al., 2007). To the extent that a “smaller-is-better” model applies to hippocampus function in normal childhood (Van Petten, 2004), it is possible that the present negative correlations simply reflect a straightforward schizophrenia neuro-developmental delay. Of course, the current negative association between hippocampal volume and episodic memory score runs contrary to the typical findings in this literature and requires replication.
Beyond the main hypotheses, the effects of demographic variables were considered. The age of subjects in this study ranged from 20 to 62 years. There was a strong negative association between overall GM volume and age that was equivalent for both groups. In controls, however, there was no effect for age on hippocampus volume, which appeared to remain relatively constant across the lifespan (at least ages 20–62). In contrast, hippocampus volume in the schizophrenia group correlated with age to the same extent as overall cortical volume. The cross-sectional design and limited sample size in the present study allow only for speculation as to the cause of this finding. Other researchers have demonstrated similar effects among controls (Sullivan et al., 1995) and subjects with schizophrenia (Chakos et al., 2005). These findings invite further investigation into possibly differential aging of neocortical versus limbic cortical tissue. Another demographic variable effect investigated was gender. This sample was drawn from the population of a veteran's hospital, and the small number of women included reflects the representation of women in that population. Because of the small sample size, this study was not an ideal test of population-typical gender differences. When sex was considered as a covariate in the analysis, there was no evidence of an effect.
In brain-behavioral studies of schizophrenia, the effect of medication must be considered. When included as a covariate, medication type had no effect on the hippocampus– memory correlations, suggesting that medication does not mediate this relationship. Rather, schizophrenia subjects taking atypical antipsychotic medications were found to have larger anterior hippocampi and smaller posterior hippocampi than those taking typical antipsychotic medications. This group was a chronic population and had been on medication for years or decades. Medication decisions for these patients were based on clinical criteria of maximizing good effects and limiting side effects, using the standard VA formulary. It may be that this pattern of hippocampal structure is an indicator of who will derive the best outcome from each medication type; however, this result was unexpected and will require replication.
Hippocampus volume is consistently and positively associated with episodic memory performance across both the normal lifespan and a host of disorders, including temporal lobe epilepsy, neurodegenerative disease, depression, post-traumatic stress disorder, dementia, and Alzheimer's disease (Griffith et al., 2004; Hickie et al., 2005; Kramer et al., 2004; 2005; Mungas et al., 2005; Nemeroff et al., 2006; Petersen et al., 2000; Reminger et al., 2004; Walhovd et al., 2004). In none of these disorders has the relationship between hippocampus volume and episodic memory function differed notably from that for normal samples. Hence, growing evidence for a divergent pattern of correlations between hippocampus volumes and episodic memory scores in schizophrenia suggests the presence of multiple processes in this disorder. These processes may be more complex than the hippocampus atrophic changes found in dementia or epilepsy that result in a relatively linear correspondence between reduced hippocampus volume and impaired episodic memory. Although the present study did identify an inverse correlation of hippocampus volume and age in the schizophrenia group, this effect was not associated with decrements in episodic memory performance. It may be that the abnormal structure-function relationship between hippocampus and episodic memory in schizophrenia precedes the onset of the disorder and catalyzes an abnormal aging process throughout the lifespan.
Several weaknesses in this research remain to be addressed. The generalizability of the present conclusions regarding hippocampus volume and episodic memory relationships is limited by the relatively small sample size. The use of a longitudinal design in the future would allow for stronger conclusions regarding aging and hippocampus–memory relationships in schizophrenia. Further, the investigation of sex differences was weakened by the gender bias in this VA sample. Moreover, very recent research by Squire and colleagues (i.e., Bayley et al., 2008) suggests that certain aspects of semantic memory processing traditionally assumed to be based in the hippocampus actually involve neocortical structures while minimally engaging the hippocampus. To the extent that this is true, some of the variance unaccounted for in episodic memory scores might be explained by abnormalities in distal neocortical regions. It may be that schizophrenia hippocampus–memory relationships are best considered in the context of a distributed brain network (Eyler et al., 2008; Nestor et al., 2007), and future research will be necessary to investigate this possibility. Our current results require replication prior to drawing any strong conclusions, but the data serve as an incremental step in our understanding of brain– behavioral relationships in schizophrenia.
Acknowledgments
This research was supported by the National Institutes on Alcohol Abuse and Alcoholism grants 1K23AA016544-01 and 1R21AA017313-01 to Dr. Thoma and by the National Institute of Mental Health grant 1R01MH65304-01 and VA MERIT grant 0104 to Dr. Cañive. None of the authors have commercial interests constituting potential conflict of interest. Information in this article was previously published only where noted.
References
- Andreone N, Tansella M, Cerini R, Rambaldelli G, Versace A, Marrella G, Perlini C, Dusi N, Pelizza L, Balestrieri M, Barbui C, Nosé M, Gasparini A, Brambilla P. Cerebral atrophy and white matter disruption in chronic schizophrenia. European Archives of Psychiatry and Clinical Neuroscience. 2007;257:3–11. doi: 10.1007/s00406-006-0675-1. [DOI] [PubMed] [Google Scholar]
- Bayley PJ, O'Reilly RC, Curran T, Squire LR. New semantic learning in patients with large medial temporal lobe lesions. Hippocampus. 2008;18:575–583. doi: 10.1002/hipo.20417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bilder RM, Bogerts B, Ashtari M, Wu H, Alvir JM, Jody D, Reiter G, Bell L, Lieberman JA. Anterior hippocampal volume reductions predict frontal lobe dysfunction in first episode schizophrenia. Schizophrenia Research. 1995;17:47–58. doi: 10.1016/0920-9964(95)00028-k. [DOI] [PubMed] [Google Scholar]
- Bogerts B, Ashtari M, Degreef G, Alvir JMJ, Bilder RM, Lieberman JA. Reduced temporal limbic structure volumes on magnetic resonance images in first episode schizophrenia. Psychiatry Research: Neuroimaging. 1990;35:1–13. doi: 10.1016/0925-4927(90)90004-p. [DOI] [PubMed] [Google Scholar]
- Bogerts B, Lieberman JA, Ashtari M, Bilder RM, Degreef G, Lerner G, Johns C, Masiar S. Hippocampus-amygdala volumes and psychopathology in chronic schizophrenia. Biological Psychiatry. 1993;33:236–246. doi: 10.1016/0006-3223(93)90289-p. [DOI] [PubMed] [Google Scholar]
- Brewer WJ, Francey SM, Wood SJ, Pantelis C, Phillips LJ, Yung AR, Anderson VA, McGorry PD. Memory impairments identified in people at ultra-high risk for psychosis who later develop first-episode psychosis. American Journal of Psychiatry. 2005;192:71–78. doi: 10.1176/appi.ajp.162.1.71. [DOI] [PubMed] [Google Scholar]
- Chakos MH, Schobel SA, Gu H, Gerig G, Bradford D, Charles C, Lieberman JA. Duration of illness and treatment effects on hippocampal volume in male patients with schizophrenia. British Journal of Psychiatry. 2005;186:26–31. doi: 10.1192/bjp.186.1.26. [DOI] [PubMed] [Google Scholar]
- Chapman LJ, Chapman JP, Kwapil TR, Eckblad M. Putatively psychosis-prone subjects 10 years later. Journal of Abnormal Psychology. 1994;103:171–183. doi: 10.1037//0021-843x.103.2.171. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Conners CK. Conners' CPT II: Continuous Performance Test II Computer program for Windows. North Tonawanda, NY: Multi-Health Systems; 2000. [Google Scholar]
- DeLisi LE, Hoff AL, Schwartz JE, Shields GW, Halthore SN, Gupta SM, Henn FA, Anand AK. Brain morphology in first-episode schizophrenic-like psychosis: A quantitative magnetic resonance imaging study. Biological Psychiatry. 1991;29:159–175. doi: 10.1016/0006-3223(91)90044-m. [DOI] [PubMed] [Google Scholar]
- Driscoll I, Hamilton DA, Petropoulos H, Yeo RA, Brooks WA, Baumgartner RN, Sutherland RJ. The aging hippocampus: Cognitive, biochemical and structural findings. Cerebral Cortex. 2003;13:1344–1351. doi: 10.1093/cercor/bhg081. [DOI] [PubMed] [Google Scholar]
- Eckblad M, Chapman L. Magical ideation as an indicator of schizotypy. Journal of Consulting and Clinical Psychology. 1983;51:215–225. doi: 10.1037//0022-006x.51.2.215. [DOI] [PubMed] [Google Scholar]
- Ellison-Wright I, Glahn DC, Laird AR, Thelen SM, Bullmore E. The anatomy of first-episode and chronic schizophrenia: An anatomical likelihood estimation analysis. American Journal of Psychiatry: AJP in Advance. 2008:1–9. doi: 10.1176/appi.ajp.2008.07101562. AiA. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eyler LT, Jeste DV, Brown GG. Brain response abnormalities during verbal learning among patients with schizophrenia. Psychiatry Research: Neuroimaging. 2008;162:11–25. doi: 10.1016/j.pscychresns.2007.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV) Washington, DC: American Psychiatric Press; 1996. [Google Scholar]
- Gold JM, Randolph C, Carpenter CJ, Goldberg TE, Weinberger DR. Forms of memory failure in schizophrenia. Journal of Abnormal Psychology. 1992;101:487–494. doi: 10.1037//0021-843x.101.3.487. [DOI] [PubMed] [Google Scholar]
- Goldberg TE, Torrey EF, Berman KF, Weinberger DR. Relations between neuropsychological performance and brain morphological and physiological measures in monozygotic twins discordant for schizophrenia. Psychiatry Research: Neuroimaging. 1994;55:51–61. doi: 10.1016/0925-4927(94)90011-6. [DOI] [PubMed] [Google Scholar]
- Goldberg TE, Torrey EF, Gold JM, Ragland JD, Bigelow LB, Weinberger DR. Learning and memory in monozygotic twins discordant for schizophrenia. Psychological Medicine. 1993;23:71–85. doi: 10.1017/s0033291700038861. [DOI] [PubMed] [Google Scholar]
- Gothelf D, Soreni N, Nachman RP, Tyano S, Hiss Y, Reiner O, Weizman A. Evidence for the involvement of the hippocampus in the pathophysiology of schizophrenia. European Neuropsychopharmacology. 2000;10:389–395. doi: 10.1016/s0924-977x(00)00097-3. [DOI] [PubMed] [Google Scholar]
- Griffith HR, Pyzalski RW, Seidenberg M, Hermann BP. Memory relationships between MRI volumes and resting PET metabolism of temporal lobe structures. Epilepsy and Behavior. 2004;5:669–676. doi: 10.1016/j.yebeh.2004.06.020. [DOI] [PubMed] [Google Scholar]
- Gruzelier J, Seymour K, Wilson L, Jolley A, Hirsch S. Impairments on neuropsychological tests of temporo-hippocampal and frontohippocampal functions and word fluency in remitting schizophrenia and affective disorders. Archives of General Psychiatry. 1988;45:623–629. doi: 10.1001/archpsyc.1988.01800310027003. [DOI] [PubMed] [Google Scholar]
- Gur RE, Turetsky BI, Cowell PE, Finkelman C, Maany V, Grossman RI, Arnold SE, Bilker WB, Gur RC. Temporolimbic volume reductions in schizophrenia. Archives of General Psychiatry. 2000;57:769–775. doi: 10.1001/archpsyc.57.8.769. [DOI] [PubMed] [Google Scholar]
- Hanlon FM, Weisend MP, Yeo RA, Huang M, Lee RR, Thoma RJ, Moses SN, Paulson KM, Miller GA, Cañive JM. A specific test of hippocampal deficit in schizophrenia. Behavioral Neuroscience. 2005;119:863–875. doi: 10.1037/0735-7044.119.4.863. [DOI] [PubMed] [Google Scholar]
- Heckers S, Rauch SL, Goff CR, Schacter DL, Fischman AJ, Alpert NM. Impaired recruitment of hippocampus during conscious recollection in schizophrenia. Nature Neuroscience. 1998;1:318–323. doi: 10.1038/1137. [DOI] [PubMed] [Google Scholar]
- Hickie I, Naismith S, Ward PB, Turner K, Scott E, Mitchell P, Wilhelm K, Parker G. Reduced hippocampal volumes and memory loss in patients with early- and late-onset depression. British Journal of Psychiatry. 2005;186:197–202. doi: 10.1192/bjp.186.3.197. [DOI] [PubMed] [Google Scholar]
- Hirayasu Y, Shenton ME, Salisbury DF, Dickey CC, Fischer IA, Mazzoni PM, Kisler T, Arakaki H, Kwon JS, Anderson JE, Yurgelun-Todd D, Tohen M, McCarley RW. Lower left temporal lobe MRI volumes in patients with first-episode schizophrenia compared with psychotic patients with first-episode affective disorder and normal subjects. American Journal of Psychiatry. 1998;155:1384–1391. doi: 10.1176/ajp.155.10.1384. [DOI] [PubMed] [Google Scholar]
- Honea R, Crow TJ, Passingham D, Mackay CE. Regional deficits in brain volume in schizophrenia: A meta-analysis of voxel-based morphometry studies. American Journal of Psychiatry. 2005;162:2233–2245. doi: 10.1176/appi.ajp.162.12.2233. [DOI] [PubMed] [Google Scholar]
- Jessen F, Scheef L, Germeshausen L, Tawo Y, Kockler M, Kuhn K, Maier W, Schild HH, Heun R. Reduced hippocampal activation during encoding and recognition of words in schizophrenia patients. American Journal of Psychiatry. 2003;160:1305–1312. doi: 10.1176/appi.ajp.160.7.1305. [DOI] [PubMed] [Google Scholar]
- Kramer JH, Rosen HJ, Du AT, Schuff N, Hollnagel C, Weiner MW, Miller BL, Delis DC. Dissociations in hippocampal and frontal contributions to episodic memory performance. Neuropsychology. 2005;19:799–805. doi: 10.1037/0894-4105.19.6.799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kramer JH, Schuff N, Reed BR, Mungas D, Du AT, Rosen HJ, Jagust WJ, Miller BL, Weiner MW, Chui HC. Hippocampal volume and retention in Alzheimer's disease. Journal of the International Neuropsychological Society. 2004;10:639–643. doi: 10.1017/S1355617704104050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuroki N, Kubicki M, Nestor PG, Salisbury DF, Park HJ, Levitt JJ, Woolston S, Frumin M, Niznikiewicz M, Westin CF, Maier SE, Shenton ME. Fornix integrity and hippocampal volume in male schizophrenic patients. Biological Psychiatry. 2006;60:22–31. doi: 10.1016/j.biopsych.2005.09.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lieberman J, Chakos M, Wu H, Alvir J, Hoffman E, Robinson D, Bilder R. Longitudinal study of brain morphology in first episode schizophrenia. Biological Psychiatry. 2001;49:487–499. doi: 10.1016/s0006-3223(01)01067-8. [DOI] [PubMed] [Google Scholar]
- Maguire EA, Gadian DG, Johnsrude IS, Good CD, Ashburner J, Frackowiak RSJ, Frith CD. Navigation-related structural change in the hippocampi of taxi drivers. Proceedings of the National Academy of Sciences, USA. 2000;97:4398–4403. doi: 10.1073/pnas.070039597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsh L, Harris D, Lim KO, Beal M, Hoff AL, Minn K, Csernansky JG, DeMent S, Faustman WO, Sullivan EV, Pfefferbaum A. Structural magnetic resonance imaging abnormalities in men with severe chronic schizophrenia and an early age at clinical onset. Archives of General Psychiatry. 1997;54:1104–1112. doi: 10.1001/archpsyc.1997.01830240060009. [DOI] [PubMed] [Google Scholar]
- McCarley RW, Wible CG, Frumin M, Hirayasu Y, Levitt JJ, Fischer IA, Shenton ME. MRI anatomy of schizophrenia. Biological Psychiatry. 1999;45:1099–1119. doi: 10.1016/s0006-3223(99)00018-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller GM, Chapman JP. Misunderstanding analysis of covariance. Journal of Abnormal Psychology. 2001;110:40–48. doi: 10.1037//0021-843x.110.1.40. [DOI] [PubMed] [Google Scholar]
- Milner B. The medial temporal-lobe amnesic syndrome. Psychiatric Clinics of North America. 2005;28:599–611. doi: 10.1016/j.psc.2005.06.002. [DOI] [PubMed] [Google Scholar]
- Mungas D, Harvey D, Reed BR, Jagust WJ, DeCarli C, Beckett L, Mack WJ, Kramer JH, Weiner MW, Schuff N, Chui HC. Longitudinal volumetric MRI change and rate of cognitive decline. Neurology. 2005;65:565–571. doi: 10.1212/01.wnl.0000172913.88973.0d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Narr KL, Thompson PM, Sharma T, Moussai J, Blanton R, Anvar B, Edris A, Krupp R, Rayman J, Khaledy M, Toga AW. Three-dimensional mapping of temporo-limbic regions and the lateral ventricles in schizophrenia: Gender effects. Biological Psychiatry. 2001;50:84–97. doi: 10.1016/s0006-3223(00)01120-3. [DOI] [PubMed] [Google Scholar]
- Narr KL, Thompson PM, Szezsko P, Robinson D, Jang S, Woods RP, Kim S, Hayashi KM, Asunction D, Toga AW, Bilder RM. Regional specificity of hippocampal volume reductions in first-episode schizophrenia. NeuroImage. 2004;21:1563–1575. doi: 10.1016/j.neuroimage.2003.11.011. [DOI] [PubMed] [Google Scholar]
- Nelson MD, Saykin AJ, Flashman LA, Riordan HJ. Hippocampal volume reduction in schizophrenia as assessed by magnetic resonance imaging. Archives of General Psychiatry. 1998;55:433–440. doi: 10.1001/archpsyc.55.5.433. [DOI] [PubMed] [Google Scholar]
- Nemeroff CB, Bremner JD, Foa EB, Mayberg HS, North CS, Stein MB. Post-traumatic stress disorder: A state-of-the-science review. Journal of Psychiatric Research. 2006;40:1–21. doi: 10.1016/j.jpsychires.2005.07.005. [DOI] [PubMed] [Google Scholar]
- Nestor PG, Kubicki M, Kuroki N, Gurrera RJ, Niznikiewicz M, Shenton ME, McCarley RW. Episodic memory and neuroimaging of hippocampus and fornix in chronic schizophrenia. Psychiatry Research: Neuroimaging. 2007;155:21–28. doi: 10.1016/j.pscychresns.2006.12.020. [DOI] [PubMed] [Google Scholar]
- O'Driscoll GA, Florencio PS, Gagnon D, Wolff AV, Benkelfat C, Mikula L, Lal S, Evans AC. Amygdala-hippocampal volume and verbal memory in first-degree relatives of schizophrenic patients. Psychiatry Research: Neuroimaging. 2001;107:75–85. doi: 10.1016/s0925-4927(01)00095-6. [DOI] [PubMed] [Google Scholar]
- Öngür D, Cullen TJ, Wolf DH, Rohan M, Barreira P, Zalesak M, Heckers S. The neural basis of relational memory deficits in schizophrenia. Archives of General Psychiatry. 2006;63:356–365. doi: 10.1001/archpsyc.63.4.356. [DOI] [PubMed] [Google Scholar]
- Pegues MP, Rogers LJ, Amend D, Vinogradov S, Deicken RF. Anterior hippocampal volume reduction in male patients with schizophrenia. Schizophrenia Research. 2003;60:105–115. doi: 10.1016/s0920-9964(02)00288-8. [DOI] [PubMed] [Google Scholar]
- Petersen RC, Jack CR, Jr, Xu YC, Waring SC, O'Brien PC, Smith GE, Ivnik RJ, Tangalos EG, Boeve BF, Kokmen E. Memory and MRI-based hippocampal volumes in aging and AD. Neurology. 2000;54:581–587. doi: 10.1212/wnl.54.3.581. [DOI] [PubMed] [Google Scholar]
- Petropoulos H, Sibbitt WL, Brooks WM. Automated T2 quantitation in neuropsychiatric lupus erythematosus: A marker of active disease. Journal of Magnetic Resonance Imaging. 1999;9:39–43. doi: 10.1002/(sici)1522-2586(199901)9:1<39::aid-jmri5>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- Reminger SL, Kaszniak AW, Labiner DM, Littrell LD, David BT, Ryan L, Herring AM, Kaemingk KL. Bilateral hippocampal volume predicts verbal memory function in temporal lobe epilepsy. Epilepsy & Behavior. 2004;5:687–695. doi: 10.1016/j.yebeh.2004.06.006. [DOI] [PubMed] [Google Scholar]
- Sachdev P, Brodaty H, Cheang D, Cathcart S. Hippocampus and amygdala volumes in elderly schizophrenic patients as assessed by magnetic resonance imaging. Psychiatry and Clinical Neurosciences. 2000;54:105–112. doi: 10.1046/j.1440-1819.2000.00644.x. [DOI] [PubMed] [Google Scholar]
- Sanfilipo M, Lafargue T, Rusinek H, Arena L, Loneragan C, Lautin A, Feiner D, Rotrosen J, Wolkin A. Volumetric measure of the frontal and temporal lobe regions in schizophrenia: Relationship to negative symptoms. Archives of General Psychiatry. 2000;57:471–480. doi: 10.1001/archpsyc.57.5.471. [DOI] [PubMed] [Google Scholar]
- Sanfilipo M, Lafargue T, Rusinek H, Arena L, Loneragan C, Lautin A, Rotrosen J, Wolkin A. Cognitive performance in schizophrenia: Relationship to regional brain volumes and psychiatric symptoms. Psychiatry Research. 2002;116:1–23. doi: 10.1016/s0925-4927(02)00046-x. [DOI] [PubMed] [Google Scholar]
- Saykin AJ, Gur RC, Gur RE, Mozley PD, Mosley LH, Resnick SM, Kester B, Stafaniak P. Neuropsychological function in schizophrenia. Archives of General Psychiatry. 1991;48:618–624. doi: 10.1001/archpsyc.1991.01810310036007. [DOI] [PubMed] [Google Scholar]
- Saykin AJ, Shtasel DL, Gur RE, Kester DB, Mozley LH, Stafiniak P, Gur RC. Neuropsychological defi cits in neuroleptic naïve patients with first-episode schizophrenia. Archives of General Psychiatry. 1994;51:124–131. doi: 10.1001/archpsyc.1994.03950020048005. [DOI] [PubMed] [Google Scholar]
- Seidman LJ, Faraone SV, Goldstein JM, Kremen WS, Horton NJ, Makris N, Toomey R, Kennedy D, Caviness VS, Tsuang MT. Left hippocampal volume as a vulnerability indicator for schizophrenia. Archives of General Psychiatry. 2002;59:839–849. doi: 10.1001/archpsyc.59.9.839. [DOI] [PubMed] [Google Scholar]
- Shenton ME, Kikinis R, Jolesz FA, Pollak SD, LeMay M, Wible CG, Hokama H, Martin J, Metcalf D, Coleman M, McCarley RW. Abnormalities of the left temporal lobe and thought disorder in schizophrenia: A quantitative magnetic resonance imaging study. New England Journal of Medicine. 1992;327:604–612. doi: 10.1056/NEJM199208273270905. [DOI] [PubMed] [Google Scholar]
- Shipley WC. A self-administered scale for measuring intellectual impairment and deterioration. Journal of Psychology. 1940;9:371–377. [Google Scholar]
- Silver H, Feldman P, Bilker W, Gur RC. Working memory as a core neuropsychological dysfunction in schizophrenia. American Journal of Psychiatry. 2003;160:1809–1816. doi: 10.1176/appi.ajp.160.10.1809. [DOI] [PubMed] [Google Scholar]
- Steen RG, Mull C, McClure R, Hamer RM, Lieberman JA. Brain volume in first-episode schizophrenia. British Journal of Psychiatry. 2006;188:510–518. doi: 10.1192/bjp.188.6.510. [DOI] [PubMed] [Google Scholar]
- Sullivan EV, Marsh L, Mathalon DH, Lim KO, Pfefferbaum A. Age-related decline in MRI volumes of temporal lobe gray matter but not hippocampus. Neurobiology of Aging. 1995;16:591–606. doi: 10.1016/0197-4580(95)00074-o. [DOI] [PubMed] [Google Scholar]
- Sweatt JD. Hippocampal function in cognition. Psychopharmacology. 2004;174:99–110. doi: 10.1007/s00213-004-1795-9. [DOI] [PubMed] [Google Scholar]
- Szeszko PR, Goldberg E, Gunduz-Bruce H, Ashtari M, Robinson D, Malhotra AK, Lencz T, Bates J, Crandall DT, Kane JM, Bilder RM. Smaller anterior hippocampal formation in antipsychotic-naïve patients with first-episode schizophrenia. American Journal of Psychiatry. 2003;160:2190–2197. doi: 10.1176/appi.ajp.160.12.2190. [DOI] [PubMed] [Google Scholar]
- Szezsko PR, Strous RD, Goldman RS, Ashtari M, Knuth KH, Lieberman JA, Bilder RM. Neuropsychological correlates of hippocampal volumes in patients experiencing a first episode of schizophrenia. American Journal of Psychiatry. 2002;159:217–226. doi: 10.1176/appi.ajp.159.2.217. [DOI] [PubMed] [Google Scholar]
- Tamlyn D, McKenna PJ, Mortimer AM, Lund CE, Hammond S, Baddeley AD. Memory impairment in schizophrenia: Its extent, affiliations and neuropsychological character. Psychological Medicine. 1992;22:101–115. doi: 10.1017/s0033291700032773. [DOI] [PubMed] [Google Scholar]
- Thoma RJ, Hanlon FM, Moses SN, Ricker D, Huang M, Edgar C, Irwin J, Torres F, Weisend MP, Adler LE, Miller GA, Cañive JM. M50 sensory gating predicts negative symptoms in schizophrenia. Schizophrenia Research. 2005;73:311–318. doi: 10.1016/j.schres.2004.07.001. [DOI] [PubMed] [Google Scholar]
- Thoma RJ, Hanlon FM, Petropoulos H, Miller GA, Moses SN, Smith A, Parks L, Lundy SL, Sanchez NM, Jones A, Huang M, Weisend MP, Cañive JM. Schizophrenia diagnosis and anterior hippocampal volume make separate contributions to sensory gating. Psychophysiology. 2008 doi: 10.1111/j.1469-8986.2008.00692.x. Early View Date: September 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torres IJ, Flashman LA, O'Leary DS, Swayze V, II, Andreasen NC. Lack of an association between delayed memory and hippocampal and temporal lobe size in patients with schizophrenia and healthy controls. Biological Psychiatry. 1997;42:1087–1096. doi: 10.1016/s0006-3223(97)00024-3. [DOI] [PubMed] [Google Scholar]
- Toulopoulou T, Grech A, Morris RG, Schulze K, McDonald C, Chapple B, Rabe-Hesketh S, Murray RM. The relationship between volumetric brain changes and cognitive function: A family study on schizophrenia. Biological Psychiatry. 2004;56:447–453. doi: 10.1016/j.biopsych.2004.06.026. [DOI] [PubMed] [Google Scholar]
- Van Petten C. Relationship between hippocampal volume and memory ability in healthy individuals across the lifespan: Review and meta-analysis. Neuropsychologia. 2004;42:1394–1413. doi: 10.1016/j.neuropsychologia.2004.04.006. [DOI] [PubMed] [Google Scholar]
- Velakoulis D, Wood SJ, Wong MTH, McGorry PD, Yung A, Phillips L, Smith D, Brewer W, Proffitt T, Desmond P, Pantelis C. Hippocampal and amygdala volumes according to psychosis stage and diagnosis. Archives of General Psychiatry. 2006;63:139–149. doi: 10.1001/archpsyc.63.2.139. [DOI] [PubMed] [Google Scholar]
- Walhovd KB, Fjell AM, Reinvang I, Lundervold A, Fishl B, Quinn BT, Dale AM. Size does matter in the long run: Hippocampal and cortical volume predict recall across weeks. Neurology. 2004;63:1193–1197. doi: 10.1212/01.wnl.0000140489.33249.95. [DOI] [PubMed] [Google Scholar]
- Watson C, Andermann F, Gloor P, Jones-Gotman M, Peters T, Evans A, Olivier A, Melanson D, Leroux G. Anatomic basis of amygdaloid and hippocampal volume measurement by magnetic resonance imaging. Neurology. 1992;42:1743–1750. doi: 10.1212/wnl.42.9.1743. [DOI] [PubMed] [Google Scholar]
- Wechsler D. Wechsler Memory Scale-Revised manual. New York: Psychological Corporation; 1987. [Google Scholar]
- Weiss AP, DeWitt I, Goff D, Ditman T, Heckers S. Anterior and posterior hippocampal volumes in schizophrenia. Schizophrenia Research. 2005;73:103–112. doi: 10.1016/j.schres.2004.05.018. [DOI] [PubMed] [Google Scholar]
- White T, Cullen K, Rohrer LM, Karatekin C, Luciana M, Schmidt M, Hongwanishkul D, Kumra S, Schulz SC, Lim KO. Limbic structures and networks in children and adolescents with schizophrenia. Schizophrenia Bulletin. 2008;34:18–29. doi: 10.1093/schbul/sbm110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright IC, Rabe-Hesketh S, Woodruff PWR, David AS, Murray RM, Bullmore ET. Meta-analysis of regional brain volumes in schizophrenia. American Journal of Psychiatry. 2000;157:16–25. doi: 10.1176/ajp.157.1.16. [DOI] [PubMed] [Google Scholar]
- Yeo RA, Gangestad SG, Thoma RJ. Developmental instability and individual variation in brain development: Implications for the etiology of neurodevelopmental disorders. Current Directions in Psychological Science. 2007;15:245–249. [Google Scholar]
- Zipursky RB, Lambe EK, Kapur S, Mikulis DJ. Cerebral gray matter volume deficits in first episode psychosis. Archives of General Psychiatry. 1998;55:540–546. doi: 10.1001/archpsyc.55.6.540. [DOI] [PubMed] [Google Scholar]