

To the Editor: A 54-year-old morbidly obese male presented with a 3-month history of a red indurated mass on the dependent aspect of his abdomen associated with bullae and peau d’orange appearance (Fig 1). The patient did not report any trauma and had a negative evaluation for underlying endocrine abnormalities, including hypothyroidism. The abdominal lesion was biopsied and showed epidermal thickening, dilated lymphatic channels, dermal edema, and fibrosis (Fig 2). The patient was treated with topical triple paste and binders for abdominal compression with some improvement.
Fig 1.
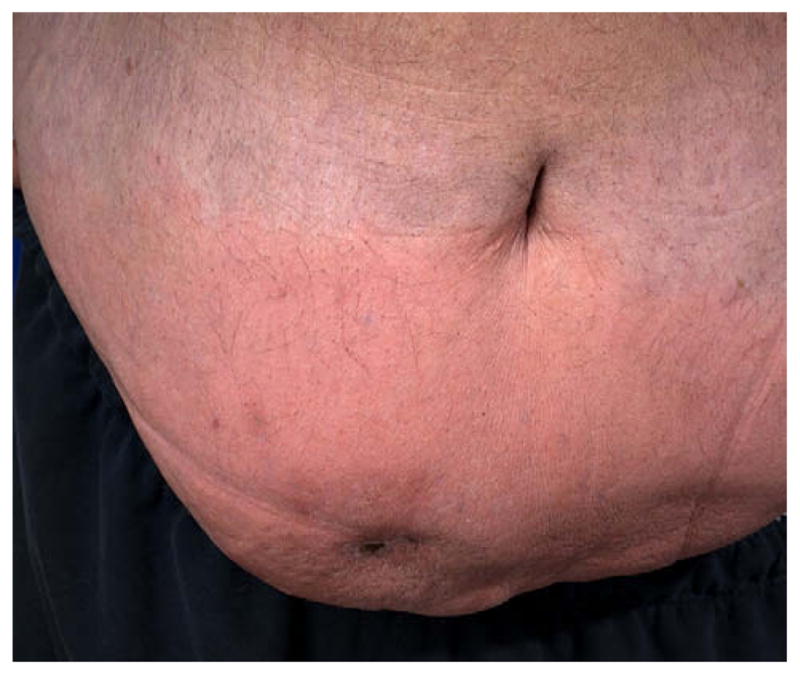
Abdominal pannus demonstrating an ill-defined indurated mass with erythema and peau d’orange appearance.
Fig 2.
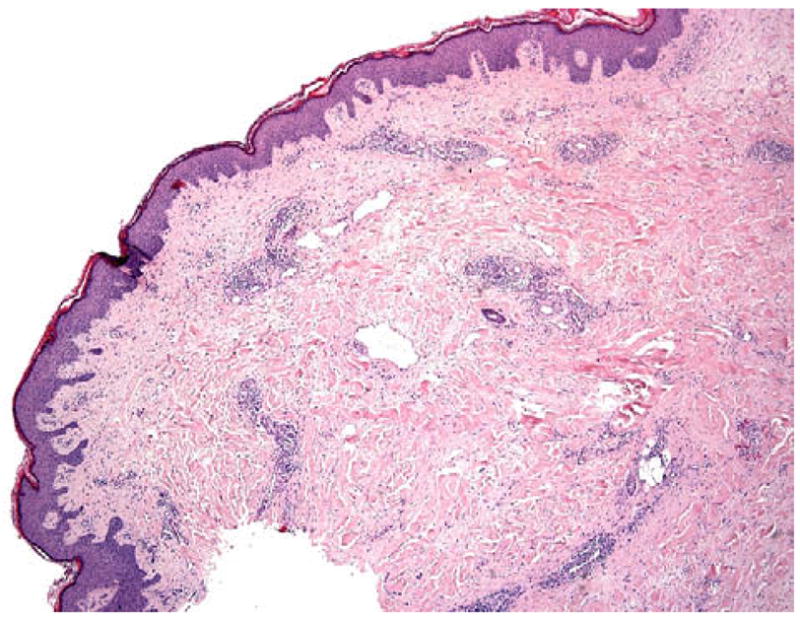
Histology of the abdominal mass shows epidermal thickening, dilated lymphatic channels, dermal edema, and fibrosis. (Hematoxylin-eosin stain; original magnifica-tion: ×40.)
This case is consistent with massive localized lymphedema (MLL) an emerging dermatologic complication of morbid obesity. MLL, which is a benign overgrowth of soft tissue characterized histologically by chronic lymphedematous changes, has primarily been described in the surgical literature.1–5 The initial case series1 described 14 patients with MLL of the proximal medial thigh. Subsequent case series describe MLL occurring in additional locations, including the abdomen, scrotum, upper extremities, and inguinal regions.2 A review of these case reports suggests that the typical patient with MLL is a morbidly obese (mean weight, 450 lbs) female (females outnumber males by a 2:1 ratio) with a mean age of 48 years old. The mass is frequently located on the thigh, is large (mean size, 32 cm), with a mean weight of 7000 g, and is painless. The mass is pendulous but not very well defined and has overlying chronic lymphedema changes including epidermal thickening and a peau d’orange appearance. There is often local inflammation with erythema and serous drainage. The mass typically has been present for 8 months to 10 years.1,2 Patients appear unbothered by the mass until it interferes with daily activities or the patient develops frequent bouts of cellulitis in this location.2,3,5
Radiologically, there is diffuse edema involving the skin and subcutaneous tissue without extension to muscle. Histologically, there is epidermal thickening, and a dermis marked by dilated lymphatic spaces, dense edema, and extensive dermal fibrosis. The deep tissue shows lobules of mature fat intercepted by pale-staining interlobular septa, with a relative absence of atypical septal fibroblasts and lipoblasts.1,2,5 Although it may clinically mimic lipo-sarcoma and has been called pseudosarcoma as a result, histopathology reveals a benign process with lack of nuclear atypia.
Chronic lymphedema may predispose patients to the formation of cutaneous angiosarcomas.3 While the majority of angiosarcomas are seen in the upper extremity of patients who have undergone radical mastectomies, there are two anecdotal cases of angiosarcomas occurring in the lymphedematous tissue of morbidly obese patients.3
Treatment of MLL is difficult. Weight reduction, physical therapy, compression, manual lymphatic drainage, and good skin hygiene are all important to therapy.1,3 Patients are frequently treated with oral and topical antibiotics because of secondary cellulitis. Surgical resection is indicated for the restoration of mobility, to prevent recurrent infections, or if there is any question of malignancy.3,5 In an epidemic of obesity, MLL will likely increase in prevalence; therefore, early identification and treatment may prevent further morbidity for these patients.
Acknowledgments
Funding sources: None.
Footnotes
Conflicts of interest: None declared.
References
- 1.Farshid G, Weiss SW. Massive localized lymphedema in the morbidly obese: a histologically distinct reactive lesion simulating liposarcoma. Am J Surg Pathol. 1998;22:1277–83. doi: 10.1097/00000478-199810000-00013. [DOI] [PubMed] [Google Scholar]
- 2.Wu D, Gibbs J, Corral D, Intengan M, Brooks JJ. Massive localized lymphedema: additional locations and association with hypothyroidism. Hum Pathol. 2000;31:1162–8. doi: 10.1053/hupa.2000.17987. [DOI] [PubMed] [Google Scholar]
- 3.Goshtasby P, Dawson J, Agarwal N. Pseudosarcoma: massive localized lymphedema of the morbidly obese. Obes Surg. 2006;16:88–93. doi: 10.1381/096089206775222014. [DOI] [PubMed] [Google Scholar]
- 4.McCrystal DJ, O’Loughlin BS. Massive localized lymphedema of the thigh. ANZ J Surg. 2007;77:91–2. doi: 10.1111/j.1445-2197.2006.03984.x. [DOI] [PubMed] [Google Scholar]
- 5.Weston S, Clay CD. Unusual case of lymphoedema in a morbidly obese patient. Australas J Dermatol. 2007;48:115–9. doi: 10.1111/j.1440-0960.2007.00349.x. [DOI] [PubMed] [Google Scholar]