

Abstract
Excessive sleepiness occurs frequently in the general population and is a common feature of many psychiatric conditions. The reductions in quality of life associated with excessive sleepiness may be substantial, involving compromised cognitive performance and work productivity as well as possible harm to the individual and the public. Excessive sleepiness may be the result of a number of extrinsic and intrinsic causes. Although it is an established symptom of certain psychiatric illnesses, abnormal excessive sleepiness in psychiatric patients may be the result of a comorbid disorder of sleep or wakefulness. Underdiagnosis and undertreatment of sleep disorders are common in community psychiatric practices because clinicians may not be aware of the different causes and consequences of excessive sleepiness. It is essential to recognize and treat the underlying cause of this disorder. In cases where sleep disorders are suspected, a comprehensive treatment program might include nonpharmacologic approaches, pharmacologic approaches, or both may need to be initiated to encompass the complexity of sleep disorder treatments. Careful monitoring and follow-up of patients with excessive daytime sleepiness, including counseling and long-term support, are essential to ensure treatment compliance and to maintain improvements over time.
Keywords: excessive sleepiness, sleep disorders, psychiatric conditions, depression, psychotropic drugs
Excessive sleepiness may interfere with the levels of alertness and wakefulness needed to perform tasks of daily living.1 It is one of the most frequently reported symptoms associated with sleep deprivation or sleep disorders.2 Excessive sleepiness commonly is seen in patients with psychiatric disorders, particularly affective disorders (e.g., depression, atypical depression, seasonal affective disorder) and psychosis (e.g., schizophrenia), and in patients taking certain psychiatric medications (e.g., benzodiazepines, tricyclic antidepressants).3 Among patients with major depressive disorder (MDD), the prevalence of hypersomnia may be as high as 10 to 20 percent.4–6 Furthermore, cross-sectional studies suggest that approximately five percent of the general adult population in the United States complain of excessive sleepiness.7 This figure may reflect the demands of a 24/7 global economy, in which people work longer hours at the workplace or at home—thanks to technological improvements and the internet.
The condition also affects overall wellbeing. In a 2005 National Sleep Foundation poll, 38 percent of adults reported being so sleepy during the day that it interfered with their daily activities at least a few days a month and 21 percent had this level of daytime sleepiness for at least a few days a week.8 Half of all respondents felt fatigued or not “up to par” during waking hours at least one day a week and 43 percent had missed work or made errors at work at least one day within the previous three months.
The diminished alertness, attention, and concentration associated with excessive sleepiness may cause substantial morbidity and mortality related to occupational injury and motor vehicle accidents.9–16 Men with excessive sleepiness have increased risk of a workplace injury, as compared with non-sleepy subjects.14 Mounting evidence suggests that excessive sleepiness among healthcare professionals compromises both employee and patient safety.10,17,18 In particular, excessive sleepiness reported by resident physicians due to sleep deprivation has been shown to be a leading cause of medical errors. This continues to be a serious problem despite attempts to mandate shorter work hours.19,20
In the 2005 National Sleep Foundation poll, 60 percent of adult drivers said they had driven a vehicle while feeling drowsy within the preceding year, and almost one third admitted to falling asleep at the wheel.8 Driving while drowsy significantly increases by 4 to 6 times the risk of an accident or near accident.16 In a recent internet survey, 1.3 percent of 35,217 respondents reported having at least one driving accident associated with sleepiness within the preceding three years.21 Overall, 18.3 percent of respondents reported at least one near-miss associated with sleepiness, while 1.8 percent reported four or more near-misses. Moreover, sleepiness is related to more than 100,000 police-reported automobile accidents a year, with 71,000 injuries and 1550 deaths.21 Another one million automobile accidents are linked to inattention and fatigue. These accidents cost approximately $12.5 billion annually. Thus, the impact of decreased alertness and excessive sleepiness is substantial, resulting in a diminished quality of life, reduced work productivity, and compromised safety for the individual and society.
There are many causes of excessive sleepiness (Table 1). Pathologic sleepiness can be caused by external factors, primary psychiatric or sleep disorders.22 Extrinsic factors include poor sleep hygiene, chronic alcohol or drug use, and the consumption of caffeinated beverages.1,3,23 Intrinsic causes include psychiatric conditions, such as major depressive disorder, and primary sleep disorders, such as narcolepsy, obstructive sleep apnea (OSA), idiopathic hypersomnia, restless legs syndrome/periodic limb movement disorder (RLS/PLMD), and circadian rhythm disturbances (e.g., shift work disorder [SWD]). 3,24 Excessive sleepiness also may be caused by use of prescription or over-the-counter medications.3 In many patients, a primary sleep disorder causing excessive sleepiness and a psychiatric illness may coexist.23 A National Institute of Mental Health population-based study showed that 46.5 percent of patients diagnosed with hypersomnia also were diagnosed with a psychiatric illness.22
Table 1.
Intrinsic and extrinsic causes of excessive sleepiness and impaired alertness
| INTRINSIC | EXTRINSIC |
|---|---|
| Narcolepsy Sleep-related breathing disorders Circadian rhythm disorders Idiopathic hypersomnia Restless legs syndrome/periodic limb movement disorder Medical conditions Psychiatric disorders
|
Sleep deprivation Poor sleep hygiene Chronic alcohol or drug use Sleep disruption related to consumption of coffee, cola, and other caffeinated beverages |
Many clinicians may be unaware of the connection between sleep disturbances and psychiatric conditions and as a result may fail to determine the cause of abnormal excessive sleepiness.25 Excessive sleepiness is recognized as an important comorbid condition in patients with primary psychiatric disorders. However, the etiologic basis for this comorbidity is not well understood.3 To further complicate matters, psychiatric illnesses often affect sleep and wakefulness and psychotropic medications may alter normal patterns of sleep.26 For instance, psychiatric drugs, such as sedating antidepressants, may exacerbate excessive sleepiness. Sleep disturbances may herald a psychiatric problem, particularly depression, anxiety disorder, and substance abuse.25 Despite these diagnostic challenges, it is essential to determine whether excessive sleepiness is the consequence of an underlying sleep disturbance or a medical or psychiatric condition so that the cause can be found and treated properly. Psychiatrists must diagnose the primary condition before beginning treatment, first with nonpharmacologic approaches and then with wake-promoting medications.
Clinical Assessment
In light of the significant health and economic burdens associated with excessive daytime sleepiness, an accurate diagnosis of its cause is imperative. Unfortunately, excessive sleepiness often is difficult to identify and assess in psychiatry practices, especially because the spectrum of presenting complaints can range from mild sleepiness to involuntary sleep episodes.27 One common problem involves the use of the terms excessive sleepiness and fatigue. Patients and clinicians often use these terms interchangeably, but despite some overlap, excessive sleepiness and fatigue have different features.28 A patient with excessive sleepiness may be unable to remain awake while reading, resting, or watching television, whereas an individual with fatigue may express feelings of apathy or listlessness rather than sleepiness. The International Classification of Sleep Disorders-2, which classifies more than 80 sleep disorders under eight categories based on symptomatic, pathophysiologic, and body system criteria,24,27 describes excessive sleepiness as a state, subjectively reported by the patient, in which he or she experiences difficulty maintaining alertness and wakefulness, followed by rapid entrance into sleep when sedentary. The severity of the abnormal somnolence is based on the frequency and level of daytime impairment and dysfunction.
The evaluation of excessive sleepiness should begin with a detailed history, including assessment of nighttime complaints and daytime problems with maintaining wakefulness and concentration. Direct questioning of the patient and a bed partner (if available) about sleep habits may differentiate nonspecific complaints, such as fatigue, inattentiveness, and stress, which are not related directly to somnolence, from true excessive sleepiness.29 It is important to remember that individuals have a moderate ability to predict performance impairment resulting from sleepiness.20,30 In addition, many people may be reluctant to admit having cognitive or functional difficulties at work or while driving. Any relevant comorbid medical conditions and medication use, as well as the use of legal substances (e.g., alcohol, caffeine, tobacco products), are important factors that should be identified.
Clinical risk factors. A focused physical examination is important because obesity and systemic hypertension are associated with sleep-disordered breathing (SDB).31–33 Obesity increases the risk of developing OSA from 2 to 4 percent in the general adult population to 20 to 40 percent in individuals with a body mass index (BMI) above 30.31 Factors predictive of OSA in the severely obese include observed apneas, male sex, higher BMI, older age, increased fasting insulin, and glycosylated hemoglobin A1c levels.31 OSA has long been associated with hypertension, and there is growing evidence that the relationship may be causal.34 Even patients with mild to moderate OSA have an elevated risk of high blood pressure and associated comorbidities (e.g., cardiovascular disease, stroke, decreased quality of life).
In addition, an upper airway examination (i.e., assessment of the posterior airspace, lower jaw structure, neck circumference) should be part of the physical examination.35 Many upper airway variables shown to be associated with OSA have been incorporated into complex predictive models, but unfortunately these models are not practical in community office practices. However, Nuckton and colleagues have found that the Mallampati score, which is used to identify individuals who may be at risk for a difficult tracheal intubation, is predictive of the presence and the severity of OSA.36 The simplicity of this method of assessing the upper airway makes it a fast and convenient tool in clinical settings. Another commonly used staging system for SDB is the Friedman scale.37
Diagnostic Testing
Validated self-administered questionnaires have been used in research studies and in the clinical setting to determine sleep habits and assess the effects of sleep-inducing and wake-promoting medications. Such questionnaires may be incorporated into clinical practice settings to supplement the clinical interview. Sleep studies, such as the polysomnogram (PSG), the multiple sleep latency test (MSLT), and the maintenance of wakefulness test (MWT), must be performed in a sleep laboratory, and although more labor intensive, may also be helpful in evaluating diminished alertness and excessive sleepiness.
The most commonly used questionnaire to assess excessive sleepiness is the Epworth Sleepiness Scale (ESS) (Figure 1). The ESS is a simple self-administered questionnaire that offers a subjective measurement of a patient's level of excessive sleepiness, defined as the average sleep propensity.38 The patient assesses his or her likelihood of falling asleep in eight situations. Ratings on the ESS range from 0 (would never doze or sleep) to 3 (high chance of dozing or sleeping). As with any subjective instrument, the ESS may be influenced by patient motivation, recall bias, and fatigue. Some researchers have questioned whether the ESS is a valid surrogate for objective tests, such as the MSLT.39
Figure 1.
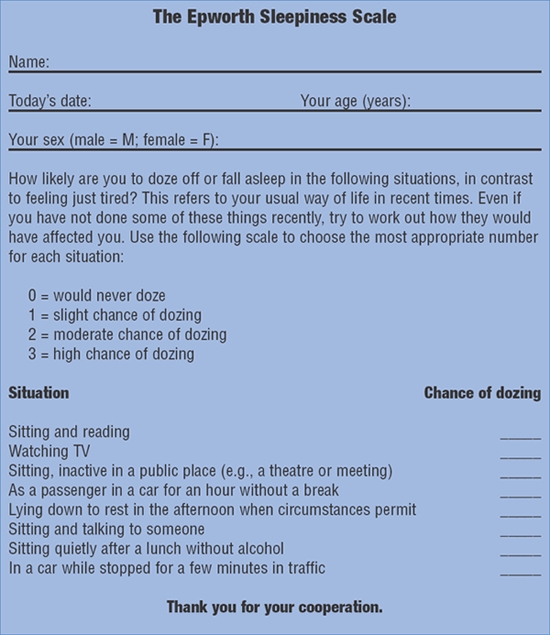
Epworth Sleepiness Scale. [Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991;14(6):540–5.]
Other subjective tests include the Karolinska Sleepiness Scale (KSS), the Stanford Sleepiness Scale (SSS), and the Sleep-Wake Activity Inventory (SWAI). Although useful in tracking symptoms over time, the KSS, SSS, and SWAI are not as effective as the ESS in making an overall assessment of sleepiness.29
Polysomnography. A PSG is the primary objective test to look for sleep disordered breathing or to investigate abnormal movements during sleep.3 Usually performed overnight, a PSG monitors multiple neurophysiologic and cardiorespiratory variables to assess sleep stages, limb movements, airflow, respiratory effort, heart rate and rhythm, oxygenation, and body position. Although it is common for physicians to diagnose a sleep disorder on the basis of a single night study, multiple recordings may provide more reliable information.2 Unfamiliar surroundings may disturb the sleep architecture and result in inaccurate test results. On the other hand, a controlled testing environment may remove environmental factors in the home that can interfere with sleep, potentially biasing results.
The American Academy of Sleep Medicine recommends the use of PSG for the diagnosis of a number of sleep-wake disturbances,24 including sleep-related breathing disorders, narcolepsy (the night before a MSLT), sleep-related behaviors that may result in injury to the patient or others,40 and atypical or unusual parasomnias.
PSG is not routinely needed to diagnose or treat RLS, circadian rhythm disorders, uncomplicated parasomnias, or depression.
Multiple sleep latency test. The MSLT, an objective measure of excessive sleepiness, is considered to be the gold standard measure of somnolence.41 The test was developed to assess excessive sleepiness and to determine the presence of sleep-onset rapid eye movement periods (SOREMP).42 The MSLT is used to diagnose narcolepsy43 and idiopathic hypersomnia,44 as well as to monitor treatment effects.7
The MSLT measures an individual's physiologic sleep tendency when potential alerting cues are controlled. These cues may be environmental (e.g., light, sound, temperature) or internal (e.g., circadian and homeostatic rhythms).7 Sleep latency is assessed over five daytime nap trials of 20 minutes each, at two-hour intervals.3 A two-week sleep log and nocturnal sleep PSG should always precede an MSLT to exclude other possible causes of a short MSL and multiple SOREMPs, such as OSA, sleep deprivation, and delayed-phase sleep syndrome. Patients should be advised not to take stimulant medications or REM-suppressing medications for two weeks before the test.3 Drug discontinuation may be impractical for some patients; however, MSLT results are more difficult to interpret if the medications are not discontinued. In many cases, it may be reasonable to do a urine drug screen before the patient starts the MSLT.
Several physiologic factors influencing MSLT have been reported; they include age, circadian rhythms, prior total sleep times, current medications, and sleep structure disruption due to a comorbid condition. For example, prepubescent children have the longest sleep latencies and young adults have the shortest.7 For shift workers and individuals with delayed sleep phase syndrome, the timing of the test is critical, because variations in circadian phases may alter sleep latency times and SOREMPs.15
Maintenance of wakefulness test. The MWT determines an individual's ability to maintain a state of wakefulness.45 A large study of 258 consecutive patients undergoing evaluation for excessive sleepiness found that although the MSLT and the MWT measure different things (tendency to fall asleep and ability to stay awake, respectively), there is a low but significant correlation between the test results.46
In summary, the MSLT is a reliable objective test to assess excessive daytime sleepiness, and the MWT is a reliable objective test to assess the ability to maintain wakefulness. Nevertheless, the variability in MSL due to protocol differences and potential confounding factors (e.g., prior activity, caffeine use, age), coupled with the nonspecificity of SOREMPs, led a task force of the American Academy of Sleep Medicine to recommend caution in making a diagnosis of excessive sleepiness based solely on MSLT or MWT findings.7 These test results, along with patient history and other medical data, should be incorporated into the diagnosis, since excessive sleepiness due to an intrinsic sleep disorder may have a marked effect on job status, quality of life, and safety.
Treatment of Excessive Sleepiness
The first step in treating excessive sleepiness is to determine its cause. For example, if the excessive sleepiness is due to OSA, nasal continuous positive airway pressure (nCPAP) and weight loss may be the primary treatments. In contrast, treatment of RLS/PLMD may consist of improvements in sleep hygiene, use of iron supplements, and reduction in consumption of alcohol, caffeine, and tobacco products.47 If sleepiness persists despite nonpharmacologic treatments, appropriate pharmacotherapy may be indicated. This includes modafinil for residual sleepiness in the setting of OSA treated with nCPAP, dopaminergic agents, benzodiazepines, and anticonvulsants for RLS/PLMD.
Nonpharmacologic approaches. Treatment of sleep deprivation due to poor sleep behaviors should begin with nonpharmacologic approaches to increase total sleep time. These strategies include measures to improve sleep hygiene (Table 2). In some situations, a trial of short scheduled naps may be helpful, since supplementary sleep periods will increase total sleep time.48 Patients with excessive sleepiness should be instructed to reserve use of the bedroom for sleep and sexual activity. Other activities, such as eating, drinking, watching television, smoking, reading, and working on the computer, should be performed outside of the bedroom. To prevent the development of counterproductive sleep habits, patients who are unable to fall asleep after 20 to 30 minutes should leave the bedroom and engage in a relaxing activity, such as reading or watching television. Patients should return to bed only when they are sleepy.
Table 2.
Techniques to improve sleep hygiene
| Maintain a comfortable bedroom temperature |
| Establish a regular sleep-wake schedule and avoid oversleeping |
| Go to bed only when sleepy |
| Do not eat, drink, watch television, smoke, use a computer, or read in bed |
| Avoid clock-watching |
| Do not exercise within three hours of bedtime |
| Engage in relaxing activities before going to bed |
| Do not go to bed feeling hungry |
| Do not drink caffeinated beverages in the evening |
| Avoid drinking alcohol before going to bed |
Pharmacologic treatments. Pharmacologic options to treat excessive sleepiness include several different chemical classes of wake-promoting medications: 1) direct-acting sympathomimetics (e.g., phenylephrine); 2) indirect-acting sympathomimetics (e.g., methylphenidate, amphetamine); and 3) nonsympathomimetic stimulants (e.g., caffeine, modafinil) (Table 3).49 In addition, there are numerous activating antidepressants, such as bupropion, protryptyline, and several of the selective serotonin reuptake inhibitors (SSRIs), that may be considered for psychiatric patients who have sedation problems. REM-suppressing antidepressants, including venlafaxine and older tricyclic drugs, may be effective in the treatment of cataplexy, hallucinations, and sleep paralysis.
Table 3.
Currently available wake-promoting medications
| Caffeine | Sympathomimetics | Modafinil | |
|---|---|---|---|
| Half-life (hours) | 3–5 | 11–20 | 12–15 |
| Daily dose range | 50mg–200mg | * | 200mg–60mg |
| Side effects | GI disorders, flushing, sweating, elevated heart and respiratory rates, disturbed sleep, withdrawal symptoms (headache, anxiety) | Cognitive, behavioral, and motor problems; GI disturbances; aggravation of existing mood disorders; headache; insomnia; anorexia; abuse liability** | Headache†, nausea, nervousness, rhinitis, diarrhea, back pain, anxiety, insomnia, dizziness, dypepsia |
*Methylphenidate: up to 60mg; dextroamphetamine: up to 60mg; methamphetamine: 5–50mg.
†Regular blood pressure monitoring is recommended.
**Not indicated for patients with pre-existing cardiovascular problems, including hypertension. Regular blood pressure monitoring is essential in all patients.
Sympathomimetic agents. The earliest treatments used for excessive sleepiness, the amphetamines, achieve their alerting effects by directly or indirectly regulating dopaminergic and noradrenergic systems located in the ventral tegmental area and the locus coeruleus, respectively, which project widely throughout the brain. Activation of non–wake-promoting regions, including the striatum and nucleus accumbens, may produce side effects such as tics and abuse liability.49
As noted by Mitler and O'Malley in a previous review of sympathomimetic alerting agents, the dosing guidelines for traditional stimulants, such as dextroamphetamine and methamphetamine, have not changed significantly since their development nearly 70 years ago.49 In a 1956 study, daily doses of methylphenidate ranging from 20mg to 240mg demonstrated effectiveness in treating excessive sleepiness.50 Treatment often begins with trials of low to moderate doses of amphetamines or methylphenidate, with titration up to 60mg of either drug as necessary to promote alertness. Amphetamine prescriptions above 60mg per day are not recommended.51 Amphetamines are available in a range of preparations with different half-lives, allowing flexibility in the development of dosing strategies (Table 3).
Dose-dependent adverse events associated with sympathomimetic therapy include headaches, irritability, nervousness, decreased appetite, insomnia, gastrointestinal problems, dyskinesia, and palpitations.49 Nighttime sleep also may be disturbed.52 Pre-existing psychiatric problems may be aggravated, although psychosis and hallucinations rarely are reported in patients taking amphetamines for excessive sleepiness.49 Cognitive, behavioral, and motor problems (e.g., obsessive thought patterns, paranoia, stereotypical movements, perseveration) may develop after sustained use of sympathomimetic therapies at high doses. The frequency of side effects is similar with use of methylphenidate and amphetamine.49
Although cardiac and vascular complications are infrequent, advanced cardiovascular disease is a contraindication for sympathomimetic drug use. Isolated cases of stroke, cardiomyopathy, and ischemic vascular complications have been reported with chronic use of these medications, especially at high doses.49 However, substantial numbers of patients have taken sympathomimetic drugs for many years without experiencing adverse cardiovascular events. Moreover, normotensive patients typically do not experience clinically significant increases in blood pressure at standard doses.49 Nevertheless, patients receiving sympathomimetic therapy should have regular blood pressure monitoring.
The abuse potential of sympathomimetic drugs is high. Even though most users (more than 90%) do not become addicted, compulsive use may lead to dependence.49 Bingeing may produce a sequence of psychiatric symptoms beginning with euphoria and culminating in psychosis; these may be followed by exhaustion, anxiety, depression, and a strong need for sleep. Amphetamine withdrawal is associated with apathy, anhedonia, and drug cravings, which subside over subsequent weeks.49
Tolerance to the alerting effects of sympathomimetic therapy may develop with varying frequencies and is most evident in patients taking high doses. It is believed that habituation is true tolerance, rather than a consequence of diminished nocturnal sleep. Tolerance does not appear to be less common with methylphenidate than with dextroamphetamine.49
Caffeine. Often used as a remedy for sleepiness, caffeine has central nervous system (CNS) effects by antagonizing adenosine receptors in the hypothalamus. Adenosine contributes to the homeostatic sleep regulatory system, and extracellular levels rise during sustained periods of wakefulness.53 By inhibiting A1 adenosine receptors, caffeine prevents sleep onset; this action may produce the side effects often associated with the drug, including gastric stimulation, diarrhea, flushing, sweating, and elevated heart and respiratory rates.49
The well-known effects of caffeine on alertness and cognitive skills have been demonstrated in numerous clinical studies. Caffeine supplements taken at bedtime can delay sleep onset and disrupt sleep continuity.54 At doses of 2mg/kg, caffeine improved psychomotor performance and vigilance in patients, demonstrating that caffeine is a useful treatment for SWD.55 Slow-release caffeine (300mg) was shown to be effective for a longer period than napping in counteracting drivers' sleepiness induced by partial sleep deprivation.56 Also, high doses of caffeine (600mg) compared favorably with 200mg and 400mg of modafinil in maintaining alertness and cognitive performance in healthy sleep-deprived young adults.57 The body of evidence shows that caffeine may improve alertness and reduce the risk of accidents and injuries in sleep-deprived individuals. For these reasons, caffeine is used most commonly in acute situations (e.g., while driving) to prolong wakefulness. However, the benefits may be lost if the dose is not adequate, if the timing of administration is incorrect, or if there is a background of severe caffeine dependence.49 Habituation may also pose a problem (Table 3).
In the context of excessive sleepiness, the most important side effect associated with caffeine is disturbed nighttime sleep. This side effect typically is seen in patients with high caffeine sensitivity and often is missed as a cause of abnormal nocturnal sleep in those who have become habituated to the drug. In addition, caffeine may be implicated in sleep fragmentation in the elderly, who have slower metabolic rates. Clinicians should discuss caffeine use whenever addressing a patient's complaints about sleeplessness. Education may help patients moderate their caffeine consumption if it is identified as a factor in sleep onset and maintenance. Abrupt cessation of caffeine consumption may cause headaches, increased anxiety and depression, reduced vigor, and increased fatigue.58 In general, moderate doses of caffeine are safe in the absence of these side effects.
Modafinil. Modafinil is a novel somnolytic agent approved for the treatment of excessive sleepiness associated with narcolepsy, SWD, and OSA refractory to mechanical treatments such as nCPAP.59 Although the precise mechanism of action remains unclear, the drug does not appear to be a dopaminergic agonist and its regional effects differ from those of sympathomimetic agents. There is evidence that modafinil is active in selected areas of the hypothalamus and the central nucleus of the amygdala; these regions of the brain are thought to be involved in regulating sleep-wake behavior.60,61 It is likely that the drug uses multiple mechanisms to trigger sleep-wake centers in the hypothalamus.49
The standard dose of modafinil for the treatment of excessive sleepiness is 200mg per day,59 although some individuals with severe sleepiness may require up to 600mg per day in divided doses (400mg at 7 AM, 200mg at noon) for symptomatic relief (Table 3).62
Modafanil may be preferable to sympathomimetic agents as a treatment option because of its favorable side effect profile. It was well tolerated in clinical trials, with headache the most frequent adverse event.63–66 No significant cardiovascular or psychiatric events were reported, although a few patients complained of insomnia or nervousness. These symptoms typically were transient and dose dependent, and habituation to modafinil rarely has been a matter of concern.49 Modafinil at the recommended doses has not been found to increase blood pressure significantly;67 however, regular blood pressure monitoring may be needed during the first few months of therapy.
Initial results from a series of clinical studies suggest that modafinil has the potential to improve symptoms of residual excessive sleepiness in patients with depression.68,69 Modafinil may augment serotonergic drug therapy in partial responders who experience sleepiness and fatigue. Further research may show that modafinil is a useful adjunctive treatment for the short-term management of patients with depression who experience persistent sleepiness and fatigue.
In addition, modafinil may be effective in mitigating the sedating effects of various antipsychotic,70,71 antidepressant,72 and mood-stabilizing drugs.73 Additional studies are necessary to confirm whether modafinil will play a role in the treatment of psychiatric patients with excessive somnolence.
Sodium oxybate. Sodium oxybate (sodium salt of gamma hydroxybutyric acid) is indicated for treating the sleepiness and cataplexy associated with narcolepsy. By activating gamma-aminobutyric acid b (GABAb) and possibly modulating GABAa and GABAc, sodium oxybate improves sleep architecture by increasing slow-wave sleep duration and delta power and decreasing REM sleep duration.74 The drug, which is effective in treating cataplexy, has been shown to limit nocturnal sleep disruptions and consolidate sleep.73 Although sodium oxybate is usually well tolerated at indicated doses, there have been reports of respiratory depression, confusion, and depression and at toxic doses, bradycardia and hypotension.74
Conclusion
Excessive sleepiness is a common symptom that may be related to sleep deprivation or other sleep disorders, such as narcolepsy, OSA, and SWSD. Excessive sleepiness also is a frequent complaint of many patients with psychiatric illness. Sleep disorders and psychiatric conditions often coexist. A poor understanding of the relationship between these comorbidities may result in misdiagnosis, undertreatment and decreased quality of life. This in turn may lead to compromised personal and public safety, particularly when patients are driving or operating machinery.
An accurate diagnosis starts with a detailed interview with the patient about possible factors that may contribute to the abnormal sleepiness. The evaluation process may require a sleep study. Nonpharmacologic approaches to treat should be introduced initially, with an emphasis on proper sleep hygiene and, in some cases, the use of short prophylactic naps. If these techniques do not resolve the problem, a wake-promoting agent or stimulant medications may be indicated. A variety of classes and formulations of drugs are available. These medications have been shown to enhance alertness, increase wakefulness, improve cognition and performance, and decrease the subjective sense of fatigue and should become part of a comprehensive treatment program.
There have been no studies comparing the effectiveness of commonly used wake-promoting agent and CNS stimulants. However, modafinil may be considered a good first choice for patients with narcolepsy, SWD, or OSA who have residual sleepiness despite adequate nonpharmacologic treatment. Modafinil may improve wakefulness without major side effects and only a slight risk of tolerance. Emerging research shows that modafinil may be useful in the treatment of sleepiness associated with MDD and in reducing sedation caused by psychotropic medications. Patients who do not respond to modafinil may benefit from a sympathomimetic drug. In individuals with narcolepsy, sodium oxybate should be a consideration when stimulant medications are inadequate. Regardless of which treatments are used, physicians should monitor their patients regularly and provide counseling and long-term support to help patients adjust to the chronic nature of their condition and ensure treatment adherence over time.
Excessive daytime sleepiness and impaired alertness are often difficult to identify and assess. However, because of the heavy social and economic burden on society, clinicians should evaluate and treat excessive sleepiness as part of a comprehensive treatment regimen.
Acknowledgments
The authors would like to thank BioScience for their editorial assistance.
Contributor Information
Dewey McWhirter, Dr. McWhirter is from the Southeast Medical Group Neurology and Sleep Medicine, Charlotte, North Carolina.
Charles Bae, Dr. Bae is from the Sleep Disorders Center, The Cleveland Clinic, Cleveland, Ohio.
Kumaraswamy Budur, Dr. Budur is from the Sleep Disorders Center, The Cleveland Clinic, Cleveland, Ohio.
References
- 1.Lee-Chiong TL. Manifestations and classifications of sleep disorders. In: Lee-Chiong TL, Sateia MJ, Carskadon MA, editors. Sleep Medicine. Philadelphia, PA: Hanley … Belfus; 2002. pp. 125–41. [Google Scholar]
- 2.Wise MS. Objective measures of sleepiness and wakefulness: Application to the real world? J Clin Neurophysiol. 2006;23:39–49. doi: 10.1097/01.wnp.0000190416.62482.42. [DOI] [PubMed] [Google Scholar]
- 3.Institute of Medicine of the National Academies. Committee on Sleep Medicine and Research. In: Colten HR, Altevogt BM, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington, DC: National Academy of Sciences; 2006. [PubMed] [Google Scholar]
- 4.Posternak MA, Zimmerman M. Partial validation of the atypical features subtype of major depressive disorder. Arch Gen Psychiatry. 2002;59:70–6. doi: 10.1001/archpsyc.59.1.70. [DOI] [PubMed] [Google Scholar]
- 5.Horwath E, Johnson J, Weissman MM, et al. The validity of major depression with atypical features based on a community study. J Affect Disord. 1992;26:117–25. doi: 10.1016/0165-0327(92)90043-6. [DOI] [PubMed] [Google Scholar]
- 6.Reynolds CF, III, Kupfer DJ. Sleep research in affective illness: state of the art circa 1987. Sleep. 1987;10:199–215. doi: 10.1093/sleep/10.3.199. [DOI] [PubMed] [Google Scholar]
- 7.Arand D, Bonnet M, Hurwitz T, et al. The clinical use of the MSLT and MWT. Sleep. 2005;28:123–44. doi: 10.1093/sleep/28.1.123. [DOI] [PubMed] [Google Scholar]
- 8.National Sleep Foundation. [April 30, 2007]. 2005 Sleep in America Poll. Available at: http://www.kintera.org/atf/cf/{F6BF2668-A1B4-4FE8-8D1A-A5D39340D9CB}/2005_summary_of_findings.pdf.
- 9.Caruso C, Hitchcock EM, Dick RB, et al. Overtime and Extended Work Shifts: Recent Findings on Illnesses, Injuries and Health Behaviors. [July 24, 2007]. NIOSH Publication No. 2004-143. Available at http://www.cdc.gov/niosh/docs/2004-143/
- 10.Dembe AE, Erickson JB, Delbos RG, Banks SM. The impact of overtime and long work hours on occupational injuries and illnesses: New evidence from the United States. Occup Environ Med. 2005;62:588–97. doi: 10.1136/oem.2004.016667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.National Center on Sleep Disorders Research Working Group. Recognizing problem sleepiness in your patients. [March 26, 2007];Am Fam Physician. 1999 Feb; Available at: www.aafp.org/afp/990215ap/937.html. [PubMed] [Google Scholar]
- 12.Findley LJ, Unverzagt ME, Suratt PM. Automobile accidents involving patients with obstructive sleep apnea. Am Rev Respir Dis. 1988;138:337–40. doi: 10.1164/ajrccm/138.2.337. [DOI] [PubMed] [Google Scholar]
- 13.Gold DR, Rogacz S, Bock N, et al. Rotating shift work, sleep, and accidents related to sleepiness in hospital nurses. Am J Public Health. 1992;82:1011–4. doi: 10.2105/ajph.82.7.1011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lindberg E, Carter N, Gislason T, Janson C. Role of snoring and daytime sleepiness in occupational accidents. Am J Respir Crit Care Med. 2001;164:2031–5. doi: 10.1164/ajrccm.164.11.2102028. [DOI] [PubMed] [Google Scholar]
- 15.Richardson GS, Miner JD, Czeisler CA. Impaired driving performance in shiftworkers: The role of the circadian system in a multifactorial model. Alcohol Drugs Driving. 1989;90(5/6):265–73. [PubMed] [Google Scholar]
- 16.National Highway Traffic Safety Administration. The Impact of Driver Inattention On Near-Crash/Crash Risk: An Analysis Using the 100-Car Naturalistic Driving Study Data. [August 10, 2007]. Available at: http://wwwnrd.nhtsa.dot.gov/departments/nrd-13/driver-distraction/PDF/DriverInattention.pdf.
- 17.Ilhan MN, Durukan E, Aras E, Türkçüoglu S, Aygün R. Long working hours increase the risk of sharp and needlestick injury in nurses: The need for new policy implication. J Adv Nurs. 2006;56:563–8. doi: 10.1111/j.1365-2648.2006.04041.x. [DOI] [PubMed] [Google Scholar]
- 18.Rogers AE, Hwang WT, Scott LD, et al. The working hours of hospital staff nurses and patient safety. Health Aff (Millwood) 2004;23:202–12. doi: 10.1377/hlthaff.23.4.202. [DOI] [PubMed] [Google Scholar]
- 19.Surani S, Subramanian S, Aguillar R, et al. Sleepiness in medical residents: impact of mandated reduction in work hours. Sleep Med. 2007;8:90–93. doi: 10.1016/j.sleep.2006.08.018. [DOI] [PubMed] [Google Scholar]
- 20.Howard SK, Gaba DM, Rosekind MR, Zarcone VP. The risks and implication of excessive daytime sleepiness in resident physicians. Acad Med. 2002;77:1019–25. doi: 10.1097/00001888-200210000-00015. [DOI] [PubMed] [Google Scholar]
- 21.National Sleep Foundation. Sleepy driver near-misses may predict accident risks. Sleep. 2007;30:331–42. doi: 10.1093/sleep/30.3.331. Drive Alert, Arrive Alive. In: Powell NB, Schechtman KB, Riley RW, et al. [DOI] [PubMed] [Google Scholar]
- 22.Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989;262:1479–84. doi: 10.1001/jama.262.11.1479. [DOI] [PubMed] [Google Scholar]
- 23.Benca RM. Psychiatric sleep-wake disorders. In: Gelder MG, Lopez-Ibor JJ, Andreason NC, editors. New Oxford Textbook of Psychiatry. Oxford, UK: Oxford University Press; 2000. pp. 1021–6. [Google Scholar]
- 24.American Academy of Sleep Medicine. International Classification of Sleep Disorders, Second Edition: Diagnostic and Coding Manual. Westchester, IL: American Academy of Sleep Medicine; 2005. [Google Scholar]
- 25.Stores G. Misdiagnosing sleep disorders as primary psychiatric conditions. Adv Psych Treat. 2003;9:69–77. [Google Scholar]
- 26.Obermeyer WH, Benca RM. Effects of drugs on sleep. Neurol Clin. 1996;14:827–40. doi: 10.1016/s0733-8619(05)70287-5. [DOI] [PubMed] [Google Scholar]
- 27.Thorpy MJ. Which clinical conditions are responsible for impaired alertness? Sleep Med. 2005;6(1):S13–S20. doi: 10.1016/s1389-9457(05)80004-8. [DOI] [PubMed] [Google Scholar]
- 28.Leibowitz SM, Brooks SN, Black JE. Excessive daytime sleepiness: Considerations for the psychiatrist. Psych Clin North Am. 2006;29:921–45. doi: 10.1016/j.psc.2006.09.004. [DOI] [PubMed] [Google Scholar]
- 29.Guilleminault C, Brooks SN. Excessive daytime sleepiness: a challenge for the practising neurologist. Brain. 2001;124:1482–91. doi: 10.1093/brain/124.8.1482. [DOI] [PubMed] [Google Scholar]
- 30.Dorrian J, Lamond N, Holmes AL, et al. The ability to self-monitor performance during a week of simulated night shifts. Sleep. 2003;26:871–7. doi: 10.1093/sleep/26.7.871. [DOI] [PubMed] [Google Scholar]
- 31.Dixon JB, Schachter LM, O'Brien PE. Predicting sleep apnea and excessive day sleepiness in the severely obese: indicators for polysomnography. Chest. 2003;123:1134–41. doi: 10.1378/chest.123.4.1134. [DOI] [PubMed] [Google Scholar]
- 32.Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. JAMA. 2000;283:1829–36. doi: 10.1001/jama.283.14.1829. [DOI] [PubMed] [Google Scholar]
- 33.Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–84. doi: 10.1056/NEJM200005113421901. [DOI] [PubMed] [Google Scholar]
- 34.Goldberg AN, Schwab RJ. Identifying the patient with sleep apnea: upper airway assessment and physical examination. Otolaryngol Clin North Am. 1998;31:919–30. doi: 10.1016/s0030-6665(05)70099-2. [DOI] [PubMed] [Google Scholar]
- 35.Nuckton TJ, Glidden DV, Browner WS, Claman DM. Physical examination: Mallampati score as an independent predictor of obstructive sleep apnea. Sleep. 2006;29:903–8. doi: 10.1093/sleep/29.7.903. [DOI] [PubMed] [Google Scholar]
- 36.Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg. 2002;127:13–21. doi: 10.1067/mhn.2002.126477. [DOI] [PubMed] [Google Scholar]
- 37.Johns MW. Daytime sleepiness, snoring, and obstructive sleep apnea. The Epworth Sleepiness Scale. Chest. 1993;103:30–6. doi: 10.1378/chest.103.1.30. [DOI] [PubMed] [Google Scholar]
- 38.Chervin RD, Aldrich MS. The Epworth Sleepiness Scale may not reflect objective measures of sleepiness or sleep apnea. Neurology. 1999;52:125–31. doi: 10.1212/wnl.52.1.125. [DOI] [PubMed] [Google Scholar]
- 39.Kushida, et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep. 2005;28(4):499–521. doi: 10.1093/sleep/28.4.499. [DOI] [PubMed] [Google Scholar]
- 40.Chervin RD. Sleepiness, fatigue, tiredness, and lack of energy in obstructive sleep apnea. Chest. 2000;118:377–9. doi: 10.1378/chest.118.2.372. [DOI] [PubMed] [Google Scholar]
- 41.Carskadon MA, Dement WC, Mitler MM, et al. Guidelines for the Multiple Sleep Latency Test (MSLT): A standard measure of sleepiness. Sleep. 1986;9:519–24. doi: 10.1093/sleep/9.4.519. [DOI] [PubMed] [Google Scholar]
- 42.Richardson GS, Carskadon MA, Flagg W, et al. Excessive daytime sleepiness in man: Multiple sleep latency measurement in narcoleptic and control subjects. Electroencephalogr Clin Neurophysiol. 1978;45:621–7. doi: 10.1016/0013-4694(78)90162-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.van den Hoed J, Kraemer H, Guilleminault C, et al. Disorders of excessive daytime somnolence: Polygraphic and clinical data for 100 patients. Sleep. 1981;4:23–37. doi: 10.1093/sleep/4.1.23. [DOI] [PubMed] [Google Scholar]
- 44.Mitler MM, Gujavarty KS, Browman CP. Maintenance of wakefulness test: a polysomnographic technique for evaluating treatment efficacy in patients with excessive somnolence. Electroencephalogr Clin Neurophysiol. 1982;53:658–61. doi: 10.1016/0013-4694(82)90142-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sangal RB, Thomas L, Mitler MM. Maintenance of wakefulness test and multiple sleep latency test. Measurement of different abilities in patients with sleep disorders. Chest. 1992;101:898–902. doi: 10.1378/chest.101.4.898. [DOI] [PubMed] [Google Scholar]
- 46.National Institute of Neurological Disorders and Stroke. Restless Legs Syndrome Fact Sheet 2007. [September 5, 2007]. Available at: http://www.ninds.nih.gov/disorders/restless_legs/detail_restless_legs.htm.
- 47.Berger AM, Hobbs BB. Impact of shift work on the health and safety of nurses and patients. Clin J Oncol Nurses. 2006;10:465–71. doi: 10.1188/06.CJON.465-471. [DOI] [PubMed] [Google Scholar]
- 48.Mitler MM, O'Malley MB. Wake-promoting medications: Efficacy and adverse events. In: Kryger MH, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine. Fourth Edition. Philadelphia: WB Saunders; 2005. pp. 484–98. [Google Scholar]
- 49.Daly DD, Yoss RE. The treatment of narcolepsy with methyl phenylpiperidylacetate: A preliminary report. Proc Staff Meet Mayo Clin. 1956;31:620–5. [PubMed] [Google Scholar]
- 50.Guilleminault C. Amphetamines and narcolepsy: Use of the Stanford database. Sleep. 1993;16:199–201. doi: 10.1093/sleep/16.3.199a. [DOI] [PubMed] [Google Scholar]
- 51.Mitler MM, Hajdukovic R, Erman MK. Treatment of narcolepsy with methamphetamine. Sleep. 1993;16:306–17. [PMC free article] [PubMed] [Google Scholar]
- 52.Porkka-Heiskanen T, Strecker RE, Thakkar M, et al. Adenosine: A mediator of the sleep-inducing effects of prolonged wakefulness. Science. 1997;276:1265–8. doi: 10.1126/science.276.5316.1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Roehrs T, Merlotti L, Halpin D, et al. Effects of theophylline on nocturnal sleep and daytime sleepiness/alertness. Chest. 1995;108:382–7. doi: 10.1378/chest.108.2.382. [DOI] [PubMed] [Google Scholar]
- 54.Muehlbach MJ, Walsh JK. The effects of caffeine on simulated night-shift work and subsequent daytime sleep. Sleep. 1995;18:22–9. doi: 10.1093/sleep/18.1.22. [DOI] [PubMed] [Google Scholar]
- 55.De Valck E, De Groot E, Cluydts R. Effects of slow-release caffeine and a nap on driving simulator performance after partial sleep deprivation. Percept Mot Skills. 2003;96:67–78. doi: 10.2466/pms.2003.96.1.67. [DOI] [PubMed] [Google Scholar]
- 56.Silverman K, Evans SM, Strain EC, Griffiths RR. Withdrawal syndrome after the double-blind cessation of caffeine consumption. N Engl J Med. 1992;327:1109–14. doi: 10.1056/NEJM199210153271601. [DOI] [PubMed] [Google Scholar]
- 57.Wesensten NJ, Belenky G, Kautz MA, et al. Maintaining alertness and performance during sleep deprivation: modafinil versus caffeine. Psychopharmacology (Berl) 2002;159:238–47. doi: 10.1007/s002130100916. [DOI] [PubMed] [Google Scholar]
- 58.Provigil (modafinil) Full Prescribing Information. West Chester, PA: Cephalon, Inc.; 2004. [Google Scholar]
- 59.Schwartz JR. Modafinil: New indications for wake promotion. Expert Opin Pharmacother. 2005;6:115–29. doi: 10.1517/14656566.6.1.115. [DOI] [PubMed] [Google Scholar]
- 60.Scammell TE, Matheson J. Modafinil: A novel stimulant for the treatment of narcolepsy. Exp Opin Invest Drugs. 1998;7:99–112. doi: 10.1517/13543784.7.1.99. [DOI] [PubMed] [Google Scholar]
- 61.Schwartz JR, Nelson MT, Schwartz ER, Hughes RJ. Effects of modafinil on wakefulness and executive function in patients with narcolepsy experiencing late-day sleepiness. Clin Neuropharmacol. 2004;27:74–9. doi: 10.1097/00002826-200403000-00005. [DOI] [PubMed] [Google Scholar]
- 62.US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology. 2000;54:1166–75. doi: 10.1212/wnl.54.5.1166. [DOI] [PubMed] [Google Scholar]
- 63.Dinges DF, Weaver TE. Effects of modafinil on sustained attention performance and quality of life in OSA patients with residual sleepiness while being treated with nCPAP. Sleep Med. 2003;4:393–402. doi: 10.1016/s1389-9457(03)00108-4. [DOI] [PubMed] [Google Scholar]
- 64.US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Ann Neurol. 1998;43:88–97. doi: 10.1002/ana.410430115. [DOI] [PubMed] [Google Scholar]
- 65.Czeisler CA, Walsh JK, Roth T, et al. for the US Modafinil in Shift Work Sleep Disorder Study Group. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353:476–86. doi: 10.1056/NEJMoa041292. [DOI] [PubMed] [Google Scholar]
- 66.Black JE, Hirshkowitz M. Modafinil for treatment of residual excessive sleepiness in nasal continuous positive airway pressure-treated obstructive sleep apnea\\hypopnea syndrome. Sleep. 2005;28:464–71. doi: 10.1093/sleep/28.4.464. [DOI] [PubMed] [Google Scholar]
- 67.DeBattista C, Doghramji K, Menza MA, et al. for the Modafinil in Depression Study Group. Adjunct modafinil for the short-term treatment of fatigue and sleepiness in patients with major depressive disorder: A preliminary double-blind, placebo-controlled study. J Clin Psychiatry. 2003;64:1057–64. doi: 10.4088/jcp.v64n0911. [DOI] [PubMed] [Google Scholar]
- 68.Fava M, Thase ME, DeBattista C. A multicenter, placebo-controlled study of modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent fatigue and sleepiness. J Clin Psychiatry. 2005;66:85–93. doi: 10.4088/jcp.v66n0112. [DOI] [PubMed] [Google Scholar]
- 69.Makela EH, Miller K, Cutlip WD., II Three case reports of modafinil use in treating sedation induced by antipsychotic medications [letter] J Clin Psychiatry. 2003;64:485–6. doi: 10.4088/jcp.v64n0420h. [DOI] [PubMed] [Google Scholar]
- 70.Sevy S, Rosenthal MH, Alvir J, et al. Double-blind, placebo-controlled study of modafinil for fatigue and cognition in schizophrenia patients treated with psychotropic medications. J Clin Psychiatry. 2005;66:839–43. doi: 10.4088/jcp.v66n0705. [DOI] [PubMed] [Google Scholar]
- 71.Schwartz TL, Azhar N, Cole K, et al. An open-label study of adjunctive modafinil in patients with sedation related to serotonergic antidepressant therapy. J Clin Psychiatry. 2004;65:1223–7. doi: 10.4088/jcp.v65n0910. [DOI] [PubMed] [Google Scholar]
- 72.Berigan T. Modafinil treatment of excessive sedation associated with divalproex sodium [letter] Can J Psychiatry. 2004;49:72–3. doi: 10.1177/070674370404900118. [DOI] [PubMed] [Google Scholar]
- 73.Black JE, Brooks SN, Nishino S. Conditions of primary excessive daytime sleepiness
- 74.Xyrem (sodium oxybate) Full Prescribing Information. Palo Alto, CA: Jazz Pharmaceuticals, Inc.; 2005. [Google Scholar]