

ABSTRACT
Eyebrow and eyelash reconstruction surgery has expanded the options for hair restoration surgeons to assist patients seeking to recover self-esteem by enhancing their appearance. This type of surgery can be performed efficiently and effectively in a properly equipped clinic. This article, in addition to detailing eyebrow and eyelash reconstruction using hair follicular unit transplantation, addresses the etiology of eyebrow and eyelash loss, offers suggestions on evaluating prospective patients, and explains preoperative and postoperative procedures. The author demonstrates how undesirable eyebrow and eyelash conditions can be altered to recuperate their natural design using a technique that has a more natural appearance than scalp hair strips, is easier to perform than temporal artery island flaps, and the results of which are more discreet than punch hair transplantation.
Keywords: Eyebrows, pathology, surgery, plastic surgery, abnormalities, injuries, eyelashes, hair, transplantation
The eyes are the windows of the soul, as the adage goes. Society looks to the eyes for important information about the person behind the eyes. Assumptions are made, often unconsciously, as to whether someone is confident, lying, nervous, flirting, angry, or so on, based on the appearance and expression of the eyes. The eyelashes and eyebrows are an integral part of these expressions (Fig. 1). Few know this as well as those afflicted with hair loss in these areas. These sufferers frequently report feeling unnatural or alien, which contributes to a compromised self-image and lack of confidence (Fig. 2).
Figure 1.

Expressions of the eyebrows.
Figure 2.

Alopecia areata.
In addition to these esthetic and social roles, eyebrows and eyelashes serve in other capacities as well: they provide protection for the eyes themselves. Eyelashes shield the eyeball from irritants, defend it from trauma, and stimulate the closing reflex. Eyebrows form a barrier sheltering the eyes and eyelashes from forehead perspiration.
These humble features of the human face perform valuable functions, and eyebrow and eyelash reconstruction can contribute to a more normal and healthy life for the patient.
HISTORY
Eyebrow transplantation procedures as we know them began in 1914, when Krusius1 used small punches to harvest scalp grafts, subsequently transplanting them to the ciliary border of the eyelid. In 1917, Knapp2 transplanted free graft strips from the eyebrow to the eyelid border. Then, in 1929, Sasagawa3 used a specially designed needle to implant human hair into eyebrow subcutaneous tissue. In 1953, Fujita4 was able to make punctiform insertions, using an injection needle. In 1980, Marritt5 used a solid needle to insert hair follicles harvested from the periphery of 4-mm punch grafts into the eyelid border (Fig. 3).
Figure 3.

Barrera’s slit and insert technique using a Chalazion clamp.
Currently, numerous techniques are available to the hair transplantation surgeon. For eyebrow reconstruction, he or she may use the following: free or pedicled strip hair grafts from the scalp; strip hair grafts from the contralateral eyebrow; punch hair transplantation; advancement flaps; temporal artery island flaps; rotation flaps; simple vertical closure; follicular units inserted with automated needles6; slit and insert technique.7
For eyelash reconstruction, the surgeon may use the following: strip grafts from eyebrows; pedicled flaps from eyebrows; or follicular units inserted with automated needles6
ETIOLOGY OF EYEBROW AND EYELASH LOSS
Madarosis, or loss of eyebrows and eyelashes, occurs for several reasons:
• disease: dermatological diseases; endocrinopathy, such as thyroid disease; psychological disease, such as trichotillomania;
• heredity: congenital aplasia;
• trauma: avulsion; burns; complications from tattooing; complications from implantation with piercing method; tumor excision; irradiation; direct brow lift with incision in supraorbital area.
SURGICAL PROCEDURE AND TECHNIQUES
Patient Evaluation
A complete medical history of the prospective patient should include the following:
• Has the patient undergone eyebrow/eyelid surgery?
• What will be the impact of dermatological diseases or conditions?
• Lupus and alopecia areata should be fully controlled before proceeding.
• Psoriasis does not interfere with treatment.
• Does the patient have a history of keloids, hypertrophic scars, or exuberant cicatricial formation? Such cases, if accepted, should be handled with extreme caution.
• Is the patient suffering from any relevant psychiatric illness? (See Fig. 4.) If so, what are the recommendations of the attending psychiatrist?
Figure 4.

Trichotilomania.
• Does the patient present hypertension or diabetes? If so, these conditions should be fully controlled before proceeding.
• Does the patient adhere to a specific diet that may affect treatment or healing? (Protein-free diets, for example, may compromise cicatrisation or growth of graft.)
Tattooed Eyebrows or Eyelashes
Tattooed eyebrows or eyelashes often enhance the results of surgical intervention: the tattoo forms a background for the implanted hair that further defines the reconstructed design, without affecting graft integration (Figs. 5, 6, and 7).
Figure 5.

Tattooed eyebrows.
Figure 6.

Eyebrows growing over tattoo.
Figure 7.

Eyebrows growing over tattoo.
Nylon Implants
Reconstruction using nylon implants is practiced throughout the world. It is illegal in the United States, however, because it often leads to scar sequelae and chronic infection. Before intervention begins, all nylon threads must be removed and any infection treated.
Laboratory Tests
Results from the following tests should be analyzed before proceeding: blood count; hepatitis; partial thromboplastin time; platelet count; prothrombin time. An AIDS test may be indicated.
Designing Eyebrows
First, analyze Fig. 8 (most common eyebrow pattern) with the patient. Then analyze Figs. 9 and 10: Women’s eyebrows sit higher over the orbital rim and arch into a C shape (Fig. 9), while men’s eyebrows sit lower, are straighter, and have a T shape (Fig. 10).
Figure 8.

Most common eyebrow pattern.
Figure 9.

Feminine eyebrow model (peak of the arch above the lateral limbus).
Figure 10.

Man’s eyebrow model (flatter than the woman’s model).
Second, compare photographs of the patient with those of the figures. Demonstrate the proposed design, adapting as necessary with respect to patient-specific topographical considerations and preferences.
Third, outline the area to be grafted for the patient’s approval.
Preoperative Procedures
The following precautions normally preclude the need for antibiotics. During the week prior to surgery, the patient is advised to:
• avoid aspirin, vitamin E, and alcohol (excessive bleeding during surgery can cause graft to pop, leading to hematoma and/or infection);
• take 1000 mg of vitamin C daily;
• wash face and hair with an antiseptic soap;
• avoid cutting or trimming hair in the donor area.
On the day of surgery, a light meal is recommended. Thirty minutes prior to surgery, administer benzodiazepine to reduce patient anxiety.
Surgery
Both eyebrow and eyelash reconstruction procedures require microscopes and magnifying glasses, as well as a 30-gauge dental syringe for applying dental anesthetic to the donor and receptor areas.
Caution: Contact with antiseptics such as Chlorohexidine may cause cornea damage. Should contact occur, irrigate immediately and thoroughly with water or saline solution.
DONOR AREA
Originally, it was thought that harvesting the finer hair from the nape of the neck or temporal area would avoid disproportionately thick eyelashes or eyebrows. Experience has not confirmed this theory, however, with results of harvesting from the midoccipital area comparable to those from the above-mentioned areas.
Recipient dominance is suggested by authors who report that the diameter of scalp hair follicles transplanted to eyebrows, arms, or legs tends to resemble that of the donor area as the transplanted hair growth. This author has observed a metaplasia-like transformation of transplanted hair, which contributes to a more natural result.
According to the research of William Parsley, M.D., (personal communication, live surgery workshop Orlando, Florida, 2001), the diameter of scalp hair is normally thicker than eyebrow hair in Asian patients, while the reverse is true in Caucasians.
HARVESTING FOR EYEBROWS
The Limmer8 technique is used to harvest grafts for eyebrow reconstruction: From the midoccipital area, a 1 × 4 cm ellipse is removed and follicular units separated using a microscope. Follicular units with more than three roots should be discarded.
INSERTING EYEBROW GRAFT
Parallel to the skin surface, incisions are made as close together as possible using an Arnold microsurgical blade (Figs. 11 and 12) or 20- to 22-gauge needles (Fig. 13). Each eyebrow is reconstructed using an average of 150 hairs. No dressing is necessary, but the patient should use protective glasses for 2 days.
Figure 11.

Incisions made with an Arnold blade parallel to skin surface.
Figure 12.

Inserting the follicular units in previous incisions.
Figure 13.

Stick and place follicular units using 22-gauge needles.
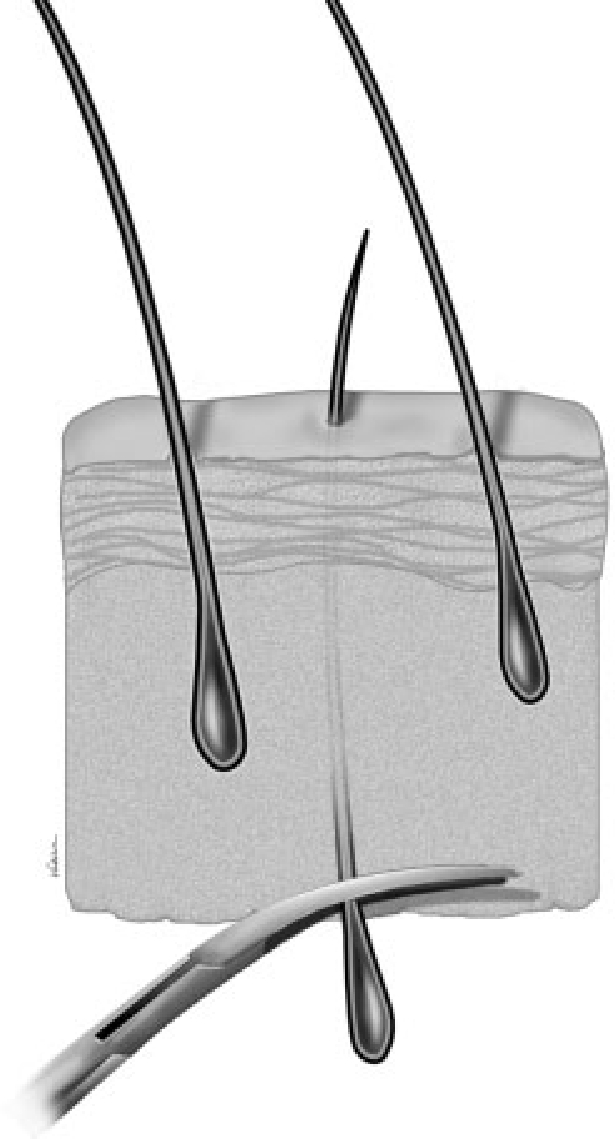
HARVESTING FOR EYELASHES
Surgery begins with the removal of a scalp ellipse or by pulling a moistened bundle of hair through the lumen of a 4-mm biopsy punch9 (Fig. 14).
Figure 14.

Dissecting a donor plug with long hair bundle passing through the lumen of a 4-mm biopsy punch.
A cylindrical graft with hair is removed with a punch. Aided by a microscope, a microsurgical blade is used to dissect the follicles, moving from the underpart of the graft toward the underside of the epidermis10 (Fig. 15). Jeweler’s forceps are used to pull the follicle, with the strand of hair still attached, through the epidermis. The result is a suture thread with a hair follicle at one end (Fig. 16).
Figure 15.
Dissecting follicle from lower graft toward underside of epidermis.
Figure 16.

Inserting the needle in the eyelid skin at the tarsus border. Suture thread with hair follicle at one end.
Caution: All tissues must be kept moist throughout the process, as any drying could lead to cell apoptosis and loss of the follicle.
INSERTING EYELASH GRAFT
The cornea is treated with topical anesthetic, and an eye shield appropriate for laser blepharoplasty is positioned over the eyes. Like a common suture, the hair is passed through a French eye needle. This needle is then inserted and pulled through the eyelid skin, exiting at the tarsus border from which the eyelashes emerge (Fig. 16), leaving the follicle in the hole left by the needle. The hair is then cut to eyelash length. No dressing is necessary, but patient should use protective glasses for 2 days.11
Caution: Intervention in the inferior eyelid is not recommended due to a high incidence of postoperative trichiasis.
Postoperative Course
During the first 48 hours, analgesics are used to alleviate pain, ice is applied to reduce edema, and protective glasses are recommended for the first night to prevent dislodging of grafts, especially during sleep.12
Crusts will form, and until they fall off (usually around 4 days after surgery), a thin layer of ophthalmic ointment or gel is recommended.13,14,15
Many surgeons report 90 to 100% growth of eyebrow grafts. Growth of eyelash grafts, however, often reaches only 50%, possibly due to being handled more frequently. This can be offset by transplanting around 50% more than desired in the final result.
The new eyebrows and eyelashes grow at the same rate and to the same length as scalp hair, meaning faster and longer than normal eyelashes and eyebrows. At first, we were afraid this would be an inconvenience, but many patients report great satisfaction in trimming eyebrows and trimming and/or curling eyelashes, which should be done every 2 weeks, or as needed (Figs. 17 and 18).
Figure 17.

Uncurled reconstructed eyelashes.
Figure 18.

Growing eyebrows (4 months).
ACKNOWLEDGMENT
I would like to express my gratitude to Lisa Dean Hawkins for help in editing this article.
REFERENCES
- Krusius F. Ueber die einplflanzung lebender haare zur wimpernbildung. Deutsche Medizinische Wochenschrift. 1914;19:958. [Google Scholar]
- Knapp P. Klin Monatsbl Augenheilkd. 1917;59:447. [Google Scholar]
- Sasagawa M. Hair transplantation. Japanese Journal of Dermatology and Urology. 1930;30:493. [Google Scholar]
- Fujita K. Reconstruction of eyebrow. La Lepro. 1953;22:364. [Google Scholar]
- Marritt E. Transplantation of single hairs from the scalp as eyelashes. Review of the literature and a case report. J Dermatol Surg Oncol. 1980;6:271–273. doi: 10.1111/j.1524-4725.1980.tb00858.x. [DOI] [PubMed] [Google Scholar]
- Choi Y-C, Kim J-C. In: Unger WP, Shapiro R, editor. Hair Transplantation. New York: Marcel Dekker, Inc; 2004. Eyebrow, eyelash, mustache and pubic area hair transplantation. pp. 579–584.
- Barrera A. In: Barrera A, editor. Hair Transplantation. St. Louis, MO: Quality Medical Publishing; 2002. Slit and insert technique. pp. 181–183.
- Limmer B L. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. J Dermatol Surg Oncol. 1994;20:789–793. doi: 10.1111/j.1524-4725.1994.tb03706.x. [DOI] [PubMed] [Google Scholar]
- Gandelman M. Eyelash reconstruction. Hair Transplant Forum International. 1996;6:18. [Google Scholar]
- Caputy G G, Flowers R S. The “pluck and sew” technique of individual hair follicle placement. Plast Reconstr Surg. 1994;93:615–620. [PubMed] [Google Scholar]
- Gandelman M. In: Barrera A, editor. Hair Transplantation. St. Louis, MO: Quality Medical Publishing; 2002. French needle technique. pp. 178–180.
- Gandelman M. In: Unger WP, Shapiro R, editor. Hair Transplantation. New York: Marcel Dekker, Inc; 1995. Eyebrow and eyelash transplantation. pp. 294–308.
- Gandelman M, Epstein J S. In: Epstein JS, editor. Facial Plastic Surgery Clinics of North America. Philadelphia: Elsevier Saunders; 2004. Hair transplantation to the eyebrow, eyelashes, and other parts of the body. pp. 253–261. [DOI] [PubMed]
- Gandelman M. In: Bosniak SL, Zilkha MC, editor. Eyebrow and eyelash reconstruction. Operative Techniques in Oculoplastic, Orbital and Reconstructive Surgery. 2001. pp. 94–99.
- Gandelman M. In: Norwood O, editor. Hair Transplant Video Forum. Vol 7. Oklahama City, OK: O'Tar Norwood; 1993. Eyebrow transplantation.