

Abstract
Nineteen nicotine-deprived cigarette smokers received monetary rewards for each minute they choose not to initiate smoking in 2-hour laboratory sessions followed by a 30-min period of enforced abstinence from smoking. Reinforcer amounts were delivered according to one of three schedules: increasing, decreasing, and constant. Relapse time (time until first smoke) was shortest in the decreasing condition, longest in the increasing condition, and intermediate in the constant condition. All differences were significant except in the constant-decreasing comparison. The relationships between a battery of baseline assessments and relapse times were examined. Relapse times were predicted by delay-discounting coefficients (k) for $10 and $1000 in money, and for $1000 of cigarettes. Relapse times were also predicted by the number of cigarettes smoked daily and a Wisconsin Card Sorting Test score. Performance on the Stroop Task and the Fagerström Test for Nicotine Dependence differentiated participants dichotomized into those who relapsed “earlier” in sessions versus those who first smoked “later.” Variability on some scores from smoking-urges and affect questionnaires administered after smoking-room sessions was explained by measures related to in-session nicotine intake. Results are discussed as they relate to contingency-management procedures, predictors of relapse, and the competing neuro-behavioral decision systems theory of addiction.
Keywords: laboratory model, smoking relapse, smoking abstinence, contingency management, delay discounting, delay gratification, Stroop task, impulsivity, executive function, human
Introduction
Successful smoking cessation requires a great deal of restraint over an extended period of time. This suggests that it may be fruitful to conceptualize the process of quitting as a test of the smoker's ability to delay the short-term gratification from smoking a cigarette in favor of the long-term health benefits associated with cessation. The study of delay gratification has been undertaken scientifically. In a paradigm developed by Mischel and his colleagues (Mischel et al., 1972; Mischel et al., 1989), children are exposed to a laboratory situation in which they can enjoy a less preferred reward immediately by ringing a bell that will retrieve the experimenter or, alternatively, can receive a more preferred reward if they wait a period of time (e.g., between 10 and 20 minutes) until the voluntary return of the experimenter. The measure of delay gratification is the amount of time until the participant retrieves the experimenter. Extensive research using this measure has shown that the ability to delay gratification during childhood is associated later in life with a lesser tendency toward frustration and aggression, better school and standardized test-score performance, and with greater social responsibility and social competence in adolescence (Mischel et al., 1972, 1989). Thus, the concept of delay gratification has contributed importantly to theories of personality and social psychology (Mischel and Shoda, 1995; Mischel, 2004).
Two previous experiments employed delay-of-gratification procedures to study cigarette smoking. McKee et al. (2006) found that alcohol intake decreased the time until the initiation of smoking and increased the amount smoked in a laboratory model where participants could earn money by delaying the start of smoking and by smoking less after they had started. Dallery and Raiff (2007) also used a model in which participants could earn money by not smoking during laboratory sessions. They found that participants smoked less under these conditions than when no money could be earned, and also that participants' measures from delay discounting assessments predicted whether participants abstained or resumed smoking in the paid-abstinence model, a finding that is consistent with another recent study demonstrating that discounting can predict relapse in clinical settings (Yoon et al., 2007).
The present study uses a new laboratory model to examine how the scheduling of monetary reinforcers for abstinence affects delay to re-initiation of smoking after a determination to avoid smoking for an extended period has been made, and to explore discounting and other measures of executive function as possible predictors of resumption of smoking in these circumstances. The laboratory procedures of the experiment attempt to simulate conditions of the natural environment that frequently terminate in a return to the behavior pattern known as cigarette addiction. While this return of symptomology outside of the laboratory is referred to diagnostically as “relapse,” that term also has the more general meaning of “return to past practice,” and as such it describes the major dependent measure of this experiment. In the model, a participant's visit to the laboratory occurred near the end of an extended period of nicotine deprivation required by experimental procedures. Past research in our laboratory (Bickel et al., 1991; Johnson and Bickel, 2003, 2006; Madden and Bickel, 1999) has shown that six hours of abstinence prior to a laboratory visit produce an effective incentive to smoke while in the laboratory. Other laboratory procedures in the model countervailed the incentive to break from abstinence, as they made the accrual of money contingent upon sustained abstinence. In addition to a control condition in which money was not earnable for abstinence, three methods of scheduling abstinence-contingent amounts of money were tested: an increasing-amount schedule, a constant-amount schedule, and a decreasing-amount schedule. We hypothesized that all schedules that awarded money contingent upon sustained abstinence would more effectively promote abstinence than the control condition. Previous contingency-management studies (Roll et al., 1996b; Roll and Higgins, 2000) suggest the more specific hypothesis that an escalating schedule of abstinence reinforcement would result in longer periods of abstinence than the schedules in which the pay amount for abstinence remains constant or decreases over time. The study also provided the opportunity to examine measures of delay discounting, and several other measures of executive function, to assess their ability to predict relapse in our laboratory model.
Methods
Participants
The University of Arkansas for Medical Sciences Institutional Review Board approved the use of human participants and the procedures implemented in this experiment. Participants were recruited to volunteer by newspaper and radio advertisements from the Little Rock, Arkansas community. Eligible participants (a) were at least 18 years old; (b) smoked at least 20 cigarettes per day; (c) scored five or higher on the Fagerström Test for Nicotine Dependence (Heatherton et al., 1991); (d) met the DSM-IV criterion for nicotine dependence; (e) provided a carbon monoxide (CO) breath level reading (measured with a hand-held monitor; Bedfont Scientific Ltd, Kent England) of at least 15 parts per million; and (f) had no plans to quit smoking within 30 days. Persons were excluded from participation if they were pregnant or if they presented significant medical or psychiatric conditions. Visit 2 entailed a behavioral screening session, the purpose of which was to obtain assurance that the participant would use the laboratory smoke self-administration procedures to smoke freely. Therefore, participants who did not use the apparatus to take 18 or more puffs during this session were discontinued prior to inclusion in the experimental design. Some participants did not smoke in any of the incentive-schedule conditions of block 1 of the experimental design. As this was a demonstration of complete insensitivity to the different levels of the incentive-schedule variable that were being assessed in the experiment, such participants were discontinued from further participation in the study and their data were not included in the analysis. Data from the 19 participants who completed all four conditions in both blocks of the design were included in the analyses.
Apparatus and materials
Participants' opportunity-to-smoke sessions occurred in small well-ventilated smoking rooms containing a chair and a table, on which was located the equipment that mediated their smoking activities. On the table was a response console with three Lindsey plungers (Med Associates Inc., St. Albans, Vermont, USA) mounted on the vertical meridian of its 30 cm × 60 cm interface, at the horizontal center and 20 cm left and right of center. Each plunger registered a response when a pull of approximately 20 N of force was applied. A computer's display monitor was situated on top of the response console. The computer was interfaced to gas pressure sensing equipment (Rayfield Equipment, Waitsfield, Vermont, USA), which was attached via approximately 90 cm of tubing to a cigarette holder. Cigarettes of the participant's preferred brand, a lighter, and an ashtray were located on the tabletop near the response console.
Procedures
Participation entailed up to 10 visits to the laboratory. Upon completion of a visit's task requirements, participants were compensated $25 at the end of visits 1 and 2, and $10 at the end of visits 3-10. Bonus compensation, in the form of a doubling of these payments, was awarded if the participant completed the study. In addition, payment schedules for smoking abstinence that were implemented in six of visits 3-10 afforded participants the opportunity to accrue compensation amounts up to $24. Total possible compensation was $404. Participants were instructed to smoke as normal prior to Visit 1, which entailed the signing of an informed consent document approved by the University of Arkansas for Medical Sciences Institutional Review Board, providing a baseline CO level reading, and undergoing other participant-intake assessments. Participants were required to abstain from smoking six hours prior to visits 2-10. These visits began with verification of abstinence by self-report and a CO breath sample no higher than 50% of the baseline CO measure. If a participant's CO sample did not comply with this requirement, the experimental session was re-scheduled for another day; and repeated failures to comply resulted in discontinuation from the study and denial of bonus compensation. Those with verified abstinence continued on with activities, which consisted predominately of an opportunity-to-smoke session in a smoking room, followed by a 30-minute wait during which the participant was not allowed to smoke and during which s/he completed questionnaires that measured craving for cigarettes (the Questionnaire on Smoking Urges (Tiffany and Drobes, 1991), nicotine withdrawal (the Minnesota Nicotine Withdrawal Scale, Hughes and Hatsukami, 1986), affect (the Positive and Negative Affect Schedule, Watson et al., 1988), and questionnaire assessments of delay and probability discounting for individual cigarette puffs. Data from the discounting-of-cigarette puffs questionnaires are not reported in this paper.
Participant-intake assessments
Baseline assessments collected during the first visit included: Quick Test (a brief assessment of intelligence, Ammons and Ammons, 1962), the Barratt Impulsivity Questionnaire-11 (Barratt, 1985), a cigarette equivalence questionnaire, a utility of cigarettes and money procedure, the Stroop Color-Word Task (Stroop, 1935), the computerized Wisconsin Card Sorting Task (WCST; Heaton et al., 1993), the Time Reproduction Task (McDonald et al., 2003), and delay discounting assessments for money and for cigarettes. Only data from the Stroop Color-Word Task, the WCST, and the discounting assessment are reported in this paper.
The computerized WCST assesses the participant's number of trials to discover, and re-discover, an effective card-sorting strategy based upon feedback regarding correct or incorrect sorting responses. Scores are measures of aspects of executive function such as working memory capacity or attention. The Stroop Color-Word Task assessment is administered as three components, in each of which the participant is asked to complete a task as quickly as s/he can while trying to avoid mistakes. Basic scores are collected as times to complete each of these tasks: (a) Color-naming task (SCN) – identify the colors of items presented in a list; (b) Word-reading task (SWR) – read the words in a list; (c) Interference task (SIT) – identify the display-color of listed words that refer to colors, where the display-color may be incongruent with the color referent. In addition to the basic scores, the derived score, SIT-SCN, is here considered as a possible participant-characteristic measure. Higher scores are indicative of lesser ability to make an appropriate response when given two conflicting signals.
A computerized adjusting-amount discounting assessment procedure determined participants' indifference points in hypothetical choices between large reward amounts to be received in the future and smaller present-time rewards whose magnitudes were adjusted across trials. $10 and $1000 amounts of money were assessed. Amounts of cigarettes that participants reported on the cigarette equivalence questionnaire to equivalent in value to $10 and to $1000 were also assessed. Indifference points were determined for those rewards hypothetically to be received at the following temporal distances, assessed in sequence: 1 day, 1 week, 1 month, 6 months, 1 year, 5 years, and 25 years. The order of presentation of the $10- and $1000-value amounts of each of the commodities was counterbalanced across participants. The indifference points from each assessment were fitted with Mazur's (1987) hyperbolic model:
| (1) |
where E(Y) is the expected indifference point at delay D, conditioned on the discounting coefficient, k. We estimated k with nonlinear regression. Since the distribution of ks are well-described with a lognormal distribution, we took the natural logarithm of k so that it would be approximately normal. All results with regard to discounting assessments are based on ln(k) values.
Experimental design
The study used a within-subjects design. Four conditions (3 implementing schedules of abstinence-contingent reward, and a control condition) were implemented in a random sequence during one block of visits (3-6) and then reassessed using a different random sequence within a second block (visits 7-10).
Smoke self-administration
Participants were instructed to pull the center plunger whenever they wanted two 70-ml-volume puffs from their preferred brand of cigarette. Upon this response, the computer display prompted the participant to light a new cigarette and affix it to the cigarette holder, inhale 70 ml of smoke, hold the smoke in the lungs for five seconds, exhale the smoke, and wait for 25 s (Zacny et al., 1987). This cycle of prompts was repeated twice for each plunger-pull and then the participant was prompted to extinguish the cigarette. Changes detected by the system's gas pressure sensing equipment were reflected in a real-time transformation of an on-screen graphic that prompted the participant to consistently stop inhaling at a puff volume between 65 to 75 ml. Since only two puffs were taken on each cigarette, this procedure avoids extended filtration by the cigarette and thus greater nicotine doses from later versus earlier puffs on the cigarette (Pomerleau et al., 1989).
Pre-smoking-room session instructions
A printed page of instructions given to participants prior to incentive-schedule sessions stated that they “may choose to accumulate money for not smoking or to earn cigarette puffs by pulling brass plungers. You will accumulate money until you make your first response on the brass plunger associated with smoking.” The page went on to describe the sequence of events that would take place during puff self-administration, and to state that “It is completely up to you to determine how many cigarette puffs, if any, you will earn during the opportunity to smoke.” The page also indicated that the center plunger would be the effective plunger; that the session time would be 120 “minutes”; and that there would be a post-session, no-smoking, wait time in the laboratory lasting 30 minutes. The instruction sheet for an incentive-schedule session indicated which kind of incentive schedule (“Decreasing,” “Increasing,” or “Constant”) would be in effect in the session, and the participant was also given another page that graphically illustrated the potential earnings per minute and the potential cumulative earnings over time in the session about to be implemented. Note that because of a slight error in the timing mechanism of the computer programs that mediated events, smoking-room sessions were in fact 2 hours and 5 min in duration and were demarked into 62.5-s segments. In the remainder of this report, all terms and data values referring to time recorded or experienced during opportunity-to-smoke sessions in the smoking rooms refer to an appropriate proportion of these 62.5-s “minutes.”
Incentives to abstain
Participants could smoke at any time during a smoking room session, but they earned money by refraining from pulling the plunger for the first time, to initiate smoking. Each of the three incentive schedules afforded participants the potential of accumulating $24 if they abstained throughout the incentive-schedule session. For a decreasing-amount schedule the amount earned was 32.33 cents in the first 62.5-s time segment and it decreased by 0.20722 cents per each succeeding segment, ending at 7.67 cents. In an increasing-amount schedule the amount earned in the first time segment was 7.67 cents and it increased by 0.20722 cents in each succeeding segment, ending at 32.33 cents. A constant-amount schedule continually allowed earnings of 20.00 cents per 62.5-s segment until the plunger was pulled. The computer's display monitor continuously displayed a whole-number value labeled “Mins Left:” that was updated after each succeeding 62.5 seconds had transpired. Prior to the first plunger-pull, amounts flashed on the screen for 5 seconds at the end of each “minute” indicating how much was earned in the past “minute” and was earnable in the upcoming “minute.”
Control-condition session instructions and contingencies
During control conditions and a behavioral screening session, participants could use the apparatus to smoke freely with no contingency for smoking or not smoking. Written and computer-displayed information in these conditions was identical to that of incentive-schedule conditions except for the absence of descriptions of amounts earnable or amounts earned.
Statistical methods
The primary outcome is the time until relapse, defined as the first plunger-pull, within a smoking-room session that was terminated after the data-collecting computer had recorded the passage of 120 of its “minutes” of session time (or 125 minutes as assessed by a true clock). Any participant not relapsing in a session was assigned a relapse time of 120 minutes, and this was noted as a censored observation in time-to-event analyses. For each of the four experimental conditions, we correlated the block-1 and block-2 relapse times collected from the 19 participants. The analysis revealed a strong positive correlation for the relapse times in each of the three incentive-schedule conditions, as the calculated r values for the decreasing-, constant-, and increasing-amount conditions were 0.64 (p < 0.005), 0.68 (p < 0.001), and 0.78 (p < 0.001), respectively. This suggests that a participant's two relapse times collected for the same incentive-schedule condition are related, and that means of the two relapse times in a condition, which were used in reporting the results, are therefore representative of a participant's data in the condition. Means calculated from censored values are also censored. The censored nature of the data, coupled with the skewed distribution of relapse times, violated usual assumptions when performing analysis of variance; hence nonparametric tests were employed.
To test whether incentive-schedule conditions in general promoted longer abstinence than the control condition, we subtracted each participant's control relapse time from his or her shortest relapse time across incentive-schedule conditions. These differences were then subjected to a signed rank test. When comparing the distributions of relapse times among the incentive-schedules, we used Friedman's test (a nonparametric analogue to a repeated measures one-factor analysis of variance, having a compound symmetric correlation structure on the observations taken within an individual) as the omnibus test, and signed-rank tests, with p-values adjusted by a factor of 3 (Bonferroni's method), for the three pair-wise comparisons. When presenting results from these analyses, we provide medians, along with 95% confidence intervals. Time-to-relapse (i.e., abstinence-survival) curves, estimated with Kaplan-Meier's product-limit method, are provided for each of the schedules to illustrate further the time-to-relapse distributions. Analyses were conducted to explore which among the 40 measures taken during the participant-intake visit may be useful in predicting relapse outcomes. A dichotomous categorization of participants was constructed based upon a median split of participants' overall means of incentive-schedule relapse times derived from the six observations per participant (median average relapse time = 107.11 min). A logistic regression was performed for each of 40 intake-session measures to determine if the measure predicted participants' status within that dichotomy. Data from the logistic regression are presented as odds ratios (ORs) and confidence intervals (CIs). The OR is the change in the odds of late relapse given a one unit increase in the intake measure, where an OR < 1 indicates decreased odds of late relapse as the predictor increases in value; an OR > 1 indicates increased odds of late relapse as the predictor increases in value; and an OR = 1 indicates the odds of late relapse does not change as the “predictor” changes in value. Theory about each participant-intake measure suggested directional hypotheses and the use of one-tailed tests and corresponding upper or lower 95% confidence bounds.
Another analysis linearly regressed the measure of participants' overall mean relapse time on each of the intake-session measures to assess which among the 40 measures predict the summary relapse-time measure as a continuous variable. Again, theory about each of the measures suggested a single direction of effect, so we considered directional (one-sided) alternative hypotheses for the slopes. Due to the small sample size (n=19) and exploratory nature of these analyses, we utilized a priori specified directional hypotheses for each of the intake measures examined, and did not adjust any p-values for multiple comparisons. No unexpected findings went unreported due to the use of one-tailed tests in either this analysis or the dichotomous-category analysis.
In our final analysis, we evaluated whether initial CO level, time to relapse, number of reinforcements obtained by the participant after relapse (i.e., number of plunger pulls), and amount of money earned – all measures collected during incentive-schedule laboratory visits – could explain variability in questionnaire measures collected after the smoking-room sessions – the Questionnaire on Smoking Urges' relief factor (QSU-R) and desire factor (QSU-D), the Minnesota Nicotine Withdrawal Scale (MNWS), and the Positive and Negative Affect Scale's positive subscore (PANAS-P) and negative subscore (PANAS-N). For each post-smoking-room-session measure, a stepwise-selection strategy requiring a significance level of 0.10 to enter and 0.05 to stay was used to select which, if any, incentive-schedule-session measures entered a regression model for that particular post-smoking-room-session questionnaire measure. All analyses were conducted with SAS® version 9.2.
Results
Abstinence-promoting effect of incentive-schedule conditions
Participants' relapse times per condition are illustrated in Figure 1, along with medians and 95% confidence intervals, which are also presented in Table 1. As expected, the median time till relapse for the control condition was extremely short (1.29 min, CI=0.68-3.02), while relapse times under all incentive-schedule conditions were considerably longer. The median difference between participants' control and shortest incentive-schedule relapse time was 91.8 min (CI=76.6-105.1; signed rank test p<0.001). Table 1 shows that among the incentive-schedule conditions, median relapse time was shortest for the decreasing-amount condition (96.24 min, CI=86.48-107.35), intermediate for the constant-amount condition (108.40 min, CI=90.88-116.61), and longest for the increasing-amount condition (113.69 min, CI=111.79-119.50). Figure 1 also makes visually evident the differences in variability of relapse times in different conditions, as the increasing interquartile ranges (IQRs) displayed in Table 1 for the control (2.35 min), increasing- (15.66 min), constant- (26.43 min), and decreasing-amount (28.55 min) conditions correspond to the increasing dispersion of data points observable in Figure 1 for those respective conditions.
Figure 1.
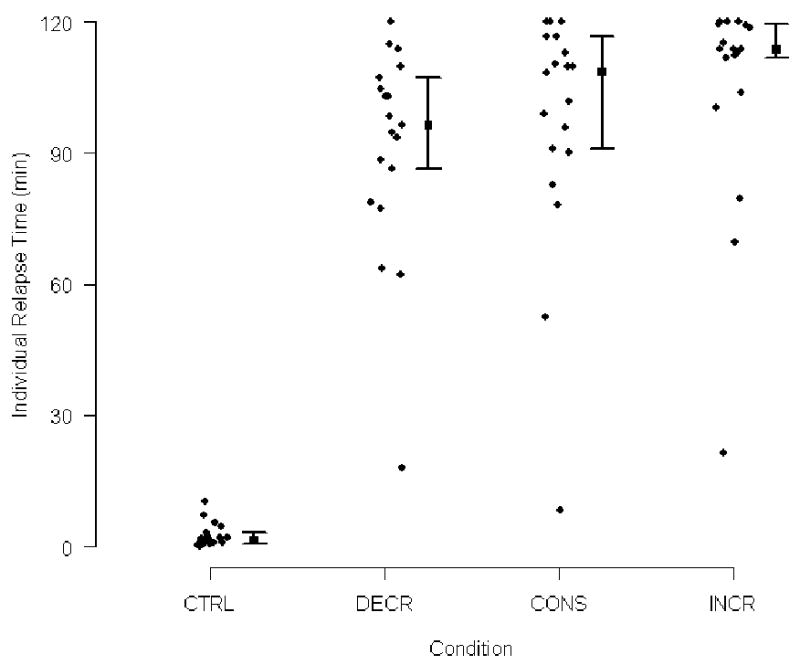
Relapse times (vertical axis) per condition (horizontal axis), with medians (points on vertical lines) and 95% confidence intervals (vertical lines with bars). CTRL = free smoking control; DECR = decreasing-amount condition; CONS = constant-amount condition; INCR = increasing-amount condition.
Table 1.
Medians (with 95% confidence interval) interquartile ranges, and numbers of relapses after minute 110, per condition.
| Condition | Median (95% CI) Relapse Time (min) | Interquartile Range (min) | Number of Post-110-minute Relapses Out of 19 |
|---|---|---|---|
| CTRL | 1.29 (0.68, 3.02) | 2.35 | 0 |
| DECR | 96.24 (86.48, 107.35) | 28.55 | 3 |
| CONS | 108.40 (90.88, 116.61) | 26.43 | 7 |
| INCR | 113.69 (111.79, 119.50) | 15.66 | 14 |
CTRL = free smoking control condition; DECR = decreasing-amount condition; CONS = constant-amount condition; INCR = increasing-amount condition.
There was evidence that the distributions of relapse times were different among the three incentive-schedule conditions (χ2[df=2] = 15.64, p = 0.001). Pair-wise differences for each of the three possible comparisons are shown graphically in Figure 2, while Table 2 presents the medians, Bonferroni-adjusted CIs, and signed rank test Bonferroni-adjusted p-values for each comparison. The increasing-amount condition prolonged abstinence significantly more than both the constant-amount condition (signed rank test p = 0. 0051) and the decreasing-amount condition (signed rank test p = 0. 0012); however the degree to which the constant-amount condition more effectively promoted abstinence than the decreasing-amount conditions was not significant (signed rank test p = 0. 2442).
Figure 2.
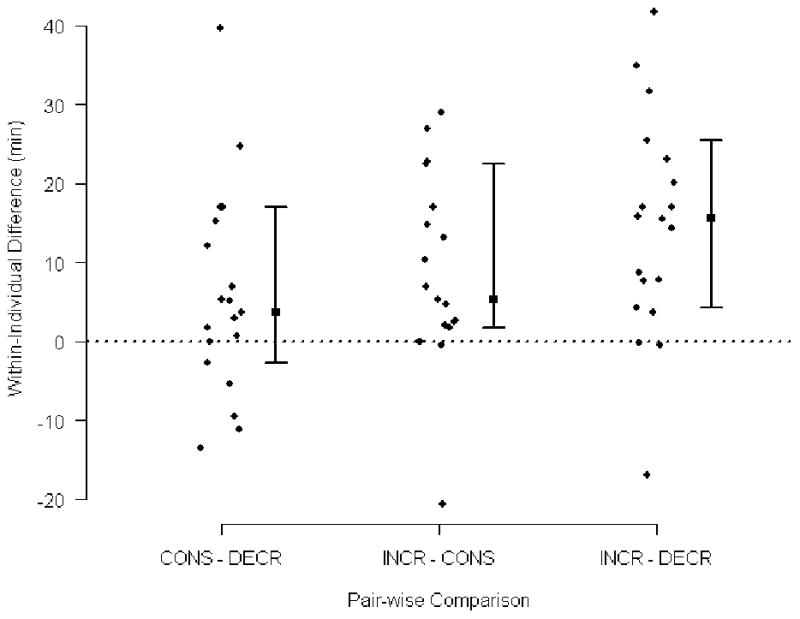
Points (vertical axis) indicate calculated within-participant differences in mean relapse time across specified conditions (horizontal axis). Medians (points on vertical lines) of the difference-score distributions and adjusted 95% CIs (vertical lines with bars) are indicated. In this figure, a significant difference is illustrated when the CI of the comparison does not cross the horizontal line at zero, which represents a null difference between condition relapse times. INCR = increasing-amount schedule; CONST = constant-amount schedule; DECR = decreasing-amount schedule.
Table 2.
Medians, and their corresponding 95% confidence intervals, of differences between relapse times within pairs of incentive-schedule conditions.
| Condition Comparison | Median (95 % CI) Difference | Signed Rank Test p-value |
|---|---|---|
| INCR – CONS | 15.55 (4.38, 25.47) | 0. 0012 |
| INCR – DECR | 5.32 (1.78, 22.40) | 0. 0051 |
| CONS – DECR | 3.69 (-2.69, 16.97) | 0. 2442 |
Note: Confidence levels and p-values adjusted with Bonferroni's method. Condition labels are as in Table 1.
Continuation of abstinence may be construed as a form of “survival”; survival curves are shown in Figure 3l, which clearly depicts the differential relapse rate for control versus all incentive-schedule conditions.
Figure 3.
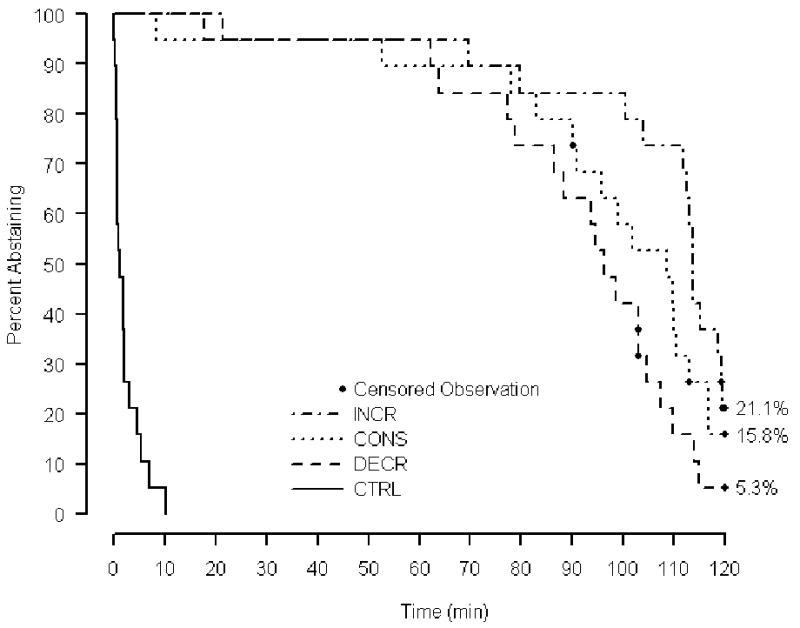
Abstinence-survival curves per condition. Time into the model-of-relapse session is plotted on the horizontal axis and percentage of participants still abstaining is plotted on the vertical axis. Ultimate survival percentages are shown. Censored observations (see text for description) are noted.
Among the incentive conditions, spatial separation of the curves occurs only after 75 minutes. After this time point, abstinence survival was greatest in the increasing-amount condition, with 21.1% (4 of 19) surviving to the end of the session, least in the decreasing-amount condition with only 5.3% (1 of 19) surviving, and intermediate in the constant-amount condition with 15.8% (3 of 19) surviving to the end of the session. Figure 3 also shows that the incentive-schedule curves converge again as minute 120 is approached. Data in Table 1 show that this convergence is due to differences in the concentration of relapses in different incentive-schedules after minute 110. Comparatively few (3/19, 15.8%) of the relapses in the decreasing-schedule condition occurred after minute 110; more than twice that many (7/19, 36.8%) occurred post-110-min for the constant-amount schedule; and that number is doubled again (14/19, 73.7%) for the increasing-schedule condition. These differences in the way relapse times are concentrated in each incentive-schedule condition are also visually evident in Figure 1.
Predictors of relapse latency
Table 3 presents the significant predictors of participants' status in the “late relapser” category (participant's mean overall relapse times ≥ 107.11 min), along with the associated odds ratio (with the 95% upper confidence bound), and the one-sided p-value. The significant predictors are two measures from the Stroop Color Naming task (SIT, SIT-SCN derived score), and the Fagerstöm Test for Nicotine Dependence score.
Table 3.
Significant predictors of participants being in the “late relapser” category.
| Predictor | Odds ratio (95% upper confidence bound) | One-sided p-value |
|---|---|---|
| SIT | 0.958 (1.000) | 0.0488 |
| SIT – SCN | 0.899 (0.988) | 0.0322 |
| Fagerström | 0.422 (0.841) | 0.0198 |
Odds ratios, and 95% upper confidence bounds, and one-sided p-values for measures observed during the participant-intake visit. An odds ratio < 1 indicates the proportional decrease in the probability of being a “late relapser” when the predictor measure increases by 1 unit. A late relapser is defined as a participant whose grand mean of incentive-schedule relapse times was greater than or equal to the cross-participant median of such averages. SIT = Stroop interference task score; SCN = Stroop color-naming task score. Fagerström = score from the Fagerström Test for Nicotine Dependence. See the text for how the predictor scores are determined.
The intake measures having statistically significant associations with the continuous measure of relapse times are illustrated in Figure 4, and their estimated slopes, 95% upper confidence bounds, and one-sided p-values are presented in Table 4. The estimates associated with each of the intake measures in Table 4 indicate the direction and magnitude of effect on relapse time (min) expected with a one-unit increase in the intake-session measure. Several delay-discounting measures were significantly associated with time to relapse measures as a continuous variable. The ln(k) for $10 in money exhibited the strongest association (slope = -4.16, s. e. = 1.72), followed by ln(k) for $1000 worth of cigarettes (slope = -3.03; s.e. = 1.27), and ln(k) for $1000 in money (slope = -2.48; s.e. = 1.34). Reported number of cigarettes smoked per day was also a significant predictor (slope = -0.87; s.e. = 0.40). A rank correlation of 0.552 (two-sided p < 0.02) between mean relapse time and the WCST Failure to Maintain Set Score (W-FTMS) suggested a natural logarithm transformation of the latter when assessing its usefulness in predicting relapse time; the slope associated with the natural logarithm of W-FTMS was 15.93 (s.e. = 8.04).
Figure 4.
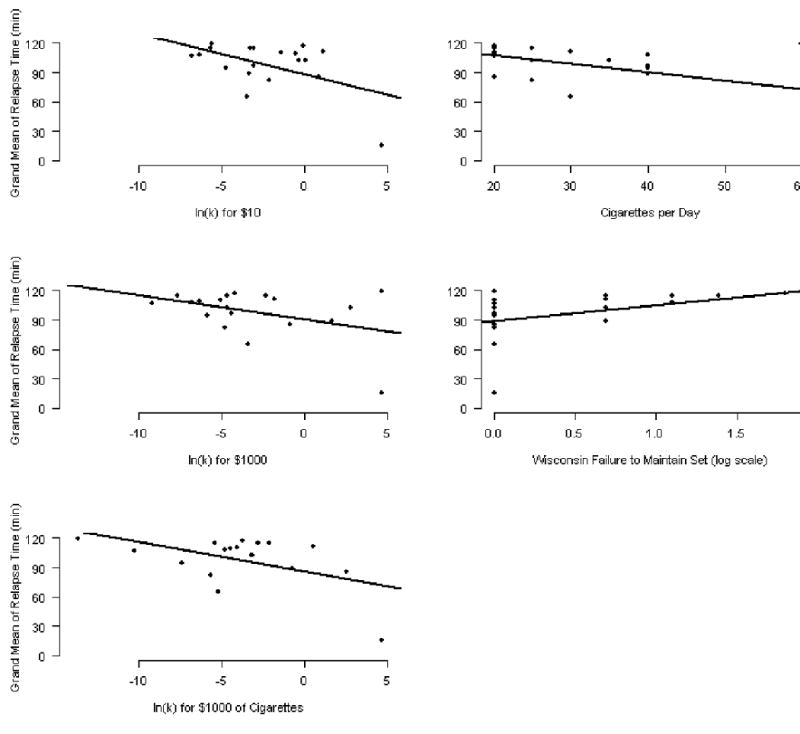
Scatter plots for grand mean relapse times plotted against significant predictors, along with estimated regression lines. Grand mean relapse times are across the six incentive-schedule smoking room sessions. “ln(k)” is the natural log of a participants' discounting coefficient for a commodity, assessed during baseline. The discounting coefficients for $10 in money, $1000 in money, and $1000 worth of cigarettes are the predictors in the top, middle, and bottom panels, respectively, of the left column. Self-reported cigarettes smoked per day, and the natural log of the WCST Failure to Maintain Set Score are the predictors in upper and lower panels, respectively, of the right column.
Table 4.
Slope and significance-level data for regression-models of Figure 4.
| Effect | Slope (95% upper or lower bound) | One-sided p-value |
|---|---|---|
| ln(k) $10 | -4.16 (-1.17) | 0.014 |
| ln(k) $1000 | -2.48 (-0.15) | 0.041 |
| ln(k) $1000 cigs | -3.03 (-0.81) | 0.015 |
| cigarettes per day | -0.87 (-0.17) | 0.022 |
| ln(W-FTMS) | 15.93 (1.94) | 0.032 |
Regression slopes, with 95% upper (alternatively, lower) confidence bounds and one-sided p-values, for predictors of grand mean relapse times. Regression slopes were computed individually for each predictor. “ln(k)” = natural logarithm of a discounting coefficient, where commodities discounted are $10 in money, $1000 in money, $1000 worth of cigarettes. Reported cigarettes smoked per day is also a predictor.
Measures explaining variance in questionnaire measures
For both QSU-D and QSU-R, only the number of reinforcements obtained by the participant was selected in the stepwise regression models, having a slope (s.e., p) of -0.93 (0.20, p< 0.001) and -0.65 (0.16, p< 0.001), respectively. Similarly for the PANAS-P subscore, only one measure remained in the stepwise regression: initial CO, having a slope (s.e., p) of -0.46 (0.18, p < 0.02). None of the in-session measures were found to explain a significant amount of variability in the MNWS score or the PANAS-N subscore.
Discussion
Using a laboratory model that presented to deprived smokers the choice between the short-term gratification of smoking versus more valuable but delayed monetary rewards, it was demonstrated that an increasing-amount schedule for reinforcing sustained abstinence promoted abstinence more effectively than a constant-amount schedule and a decreasing-amount schedule. Incentive schedules, in general, promoted sustained abstinence much more effectively than a control condition that was devoid of reinforcement for abstinence. These relations are illustrated in plots of participants' condition-mean relapse times (Figure 1), and in abstinence-survival curves (Figure 3).
This experiment advanced previous efforts (Dallery and Raiff, 2007; McKee et al., 2006) to develop a behavioral laboratory model of the process of abstaining from smoking. The Dallery and Raiff (2007) experiment was comparable to the present study in that different monetary amounts were used in the different reinforcement schedules under study. Our results join those of Dallery and Raiff from a laboratory context, and numerous others from outpatient treatment contexts, in support of the finding that the scheduling of different-sized amounts of reinforcer contingent upon drug abstinence can cause profound decreases in drug use, as compared to control conditions (Higgins and Petry, 1999; Higgins et al., 2002, 2007). Moreover, we observed significantly different effects between conditions in which our reinforcer-magnitude variable was manipulated differently, whereas Dallery and Raiff (2007) did not. Their two levels of the reinforcer-magnitude variable were proportionately different sizes of maximum amounts earnable via abstinence (“high condition” reinforcers were four times larger than “low condition” reinforcers) that were otherwise scheduled for delivery in the same way. By contrast, the levels of our independent variable involved different scheduling algorithms (decreasing-, constant-, and increasing-amount schedules) for delivering reinforcers that in the aggregate were the same in all conditions ($24). Our results in comparison to those of Dallery and Raiff (2007) highlight the behavior-change effectiveness of scheduling techniques that make reinforcers conditional upon behavior change, as compared to operations that manipulate reinforcer size without regard for changes in behavior that reinforcement may cause (Ferster and Skinner, 1957). Two of the conditions used here, the increasing- and constant-amount conditions, involved amount-scheduling algorithms similar to those that have been used in outpatient treatment programs (Roll et al., 2006a,b). Our results provide further evidence, from a new context, that increasing-amount schedules more effectively promote cigarette abstinence than constant-amount schedules (Roll et al., 1996a; Roll and Higgins, 2000).
The first instance of smoking after the initiation of an attempt to quit cigarettes is one of the best predictors of failure (Brandon et al., 1990; Garvey et al., 1992; Kenford et al., 1994; Marlatt et al., 1988; Nides et al., 1995; Norregaard et al., 1993). Relapses typically occur soon after the resolution to quit (Shiffman et al., 1996) and early relapses are highly correlated with the return to regular smoking (Garvey et al., 1992; Westman et al., 1997). As the first smoking to occur in a cessation attempt appears to be a critical transition point, it is a worthy subject of investigation for laboratory models of cigarette abstinence (McKee et al., 2006). Dallery and Raiff (2007) collected data on latency to the first instance of smoking, but found no significant difference across their two non-control conditions. This is probably because their procedures provided for the resetting of the monetary amounts back down to initial values at various times during procedures, thus de-emphasizing the reinforcement of an extended initial period of abstinence. In sum, their laboratory model was designed to affect general levels of abstinence rather than the time to the initial smoke, in particular. The laboratory model used by McKee et al. (2006) was designed to focus on the time until initiation of smoking, as their payment schedule continued without resetting until smoking was initiated. However, McKee et al.'s independent variable, the metabolic presence or absence of alcohol, was hypothesized and observed to decrease time until relapse. To our knowledge, the present experiment is the first to use a laboratory model designed to focus on the time until the first smoke in a cigarette cessation attempt, and to also explore methods that were expected to increase that time.
Our decreasing-, constant-, and increasing-amount schedules are tools for simulating different kinds of change in resistance to relapse over the course of extended time in abstinence. Their general effectiveness for this purpose is exhibited in the systematic levels of separation of the three incentive-schedule survival-of-abstinence curves (Figure 3) after minute 75. However, some of our observed systematic effects contradict expectations prompted by those schedules. The fact that the scheduled reinforcement magnitudes at the end of the sessions are highest for the increasing-amount schedule, intermediate for the constant-amount schedule, and lowest for the decreasing-amount schedule would lead to the expectation that rates of relapse as the end of the smoking-room session approaches would be lowest for the increasing-amount schedule, intermediate for the constant-amount schedule, and highest for the decreasing amount schedule.
The relapse-time data collected after minute 110 in this experiment contradict this expectation, suggesting that relapse responding in the incentive-schedule conditions is being controlled by variables in addition to the changing magnitudes of the schedules. The detail in the patterns in Figures 1 and 3, and the variability of the relapse time distributions (Table 1) suggest, more precisely, that some relapse responses, rather than being controlled by the continued accumulation of time transpired in the smoking-room session, appear to be controlled instead by delayed events such as termination of the smoking-room session, or the following 30-minute enforced period of abstinence; relapse times of this kind occur predominantly in the constant- and increasing-amount conditions after minute 110, and there are more of them in the increasing-amount condition; these responses may be thought of as delay-influenced consumption. Other relapse times seem to be immediate consumption, as they appear to be controlled by present consummatory cues such as the current state of nicotine deprivation or stimuli that have been associated with smoking; these relapses predominate in the decreasing-amount condition, and in the constant- and increasing-amount conditions they occur predominantly before minute 110. These observations suggest that our laboratory model of relapse may model temporal contingencies of the real world, some retrospective and some prospective (Bickel et al., 2006; Jones et al., 2009; Kowal et al., 2008), such as the periods of enforced abstinence to which cigarette smokers are increasingly exposed as the list of mandated smoke-free areas continues to grow.
In our decreasing-amount schedule condition we simulated declining resistance to relapse, and did so using operations (monetary awards) extrinsic to drug effects. Walsh, et al. (2001) and Donny, et al. (2004) used money amounts that decreased across a series of discrete trials that posed to their participants the choice of cocaine administration versus receiving money rewards. We are not aware of any human-subjects research that used decreasing-amount schedules with a free-operant procedure or cigarette consumption. Thus our results extend the knowledge about procedures for managing the reinforcement of response-omission in human subjects, and with nicotine consumption as the response. It is not surprising that the decreasing-amounts schedule promoted continued abstinence least effectively, as it by definition diminishes with the passage of time the amount of reinforcement that is provided contingent upon response omission. More interesting is the resultant pattern of relapsing produced. Figure 3 reveals that the decreasing-amount schedule results in the most uniform pattern of relapses, which is reflected in the variability of the relapse times in different schedules (see Table 1). Variability in relapse times is importantly related to the reason why monetary reinforcers are used in laboratory models of abstinence (McKee et al., 2006). Abstinence-contingent money provides alternative reinforcers in the experimental context, and this diminishes the reinforcing value of the drug under study (Carroll et al., 1989; Higgins, 1997; Rodefer et al., 1997). This effect, considered alone, increases the likelihood that variables other than reinforcement by the drug will control behavior, and that across a sampling of challenges to abstinence there will greater variability of relapse times and greater sensitivity to variables other than the drug reinforcement effect. However, abstinence-contingent monetary payments are themselves a potentially dominating variable. Such dominance is exhibited for the increasing- and constant-amount schedules of this experiment in the patterns showing their many late relapse times (Figures 1 and 3) and their smaller relapse-time variability (Table 1). The inclusion of a decreasing-amount feature in a schedule that reinforces abstinence with money appears to be an effective means of mitigating this dominance, and thus of exposing sensitivity to variables other than reinforcing value of money or the drug under study. Thus the decreasing-amount feature is tool that should not be overlooked when designing laboratory models for examining variables that impact relapse behavior (Donny et al., 2004; McKee et al., 2006; Walsh et al., 2001).
We conducted analyses pursuant to explaining variability in the questionnaire measures collected after smoking-room sessions. No variability in the MNWS was explained. The implementation of the MNWS in the present study asked the respondent to rate him or herself “in the last 24 hours” with regard to certain characteristics. As this time period is much broader than the period of laboratory exposure to variables tested for explanatory power, the lack of explained variability is not surprising. Variance in the QSU-R and QSU-D measures was explained by number of reinforcements obtained in the smoking rooms session that day. As reinforcers were self-administrations of nicotine to nicotine-deprived participants, it is reasonable that high numbers of obtained reinforcers would be associated with low scores, and vice versa, on an assessment for which high scores indicated greater urges to smoke. Variability in PANAS-P scores was explained by one measure taken on smoking-room-session visit days: initial (pre-smoking-room-session) CO level. As low scores on this measure reflected greater nicotine deprivation, it is again reasonable that there was a negative relationship between such low scores and higher scores on a measure whose high scores reflect emotional changes likely to be associated with decrease in nicotine deprivation. The fact that neither initial CO nor any other measure taken explained variability in PANAS-N subscores suggests that the two PANAS subscores do indeed assess a distinction between participant characteristics – positive affect versus negative affect – engendered by our experimental procedures. Future studies may be designed to manipulate procedures or utilize statistical analyses so as to explore this difference.
The ability to abstain during an initial period of smoking cessation may reflect individual differences in the ability to delay gratification. A growing body of evidence suggests that deficits in this ability, as reflected in higher delay-discounting rates, are characteristic of drug dependency in general (Bickel and Marsch, 2001; Heil et al., 2006; Kirby et al., 1999; Kirby and Petry, 2004; Madden et al., 1997; Petry, 2001) and nicotine dependence in particular (Baker et al., 2003; Bickel et al., 1999., 2008; Dallery and Raiff, 2007; Johnson et al., 2007; Odum et al., 2002; Yoon et al., 2007). In our exploratory analysis among individual differences assessed at study intake, several measures of delay discounting were strong predictors of the continuous measure of average time to relapse during the smoking-room abstinence tests. This is consistent with our postulation that short relapse times in this laboratory model are reflective of the participant's inability outside of the laboratory to delay gratification sufficient to refrain from smoking. Reported number of cigarettes smoked per day was also a predictor. As this may be a measure of nicotine dependence levels and the reinforcing value of cigarettes for the participant, it is not surprising that larger values are correlated with smoking sooner in a period of extended abstinence. The Failure to Maintain Set Score from the WCST was significantly and positively correlated to the continuous measure of average relapse time. This score is nominally a measure of the participant's number of departures from a currently successful criterion for sorting cards in the absence of feedback indicating a change in the effectiveness of that sorting criterion. As the WCST is considered a measure of executive function, the individual Failure to Maintain Set Score reflects particular aspects of executive function, such that high scores indicate comparative deficits in working memory capacity or in attention. Such deficits may be expected among those less successful in the task presented to them in a smoking room in this experiment.
A different pattern of intake-session measures was demonstrated to predict the categorical outcome of “early relapser” versus “late relapser.” These predictors were two Stroop Task measures and the Fagerström Test for Nicotine Dependence Score. As the Fagerström score, like cigarettes consumed per day, is related to nicotine dependence levels, it is again not surprising that higher scores on this measure predict a sooner break from abstinence. Higher scores in the Stroop Task reflect lesser ability to make appropriate responses when given conflicting signals. This experiment created for participants the choice to end nicotine deprivation by smoking, while establishing the conflicting motive to continue abstinence as a means for earning money. When viewed in this context, it is not surprising that measures of diminished ability to respond to conflicting signals were correlated with early relapse. Additional research will be needed to determine why the two outcome measures using continuous versus categorical indicators of relapse yielded a different set of predictors in these exploratory analyses, and what the inter-relationship is among the outcome and predictor measures identified here.
It is of conceptual interest that measures predicting relapse time in our exploratory analyses were scores from the Stroop Task and the WCST – both of which are traditional test of executive function, defined as self-directed action with the purpose of altering behavior to change future outcomes – and performance on delay discounting measures, which have been suggested as indicative of impulsivity (Bickel et al., 1999; Bickel and Marsch, 2001; Perry et al., 2005). Executive function and impulsivity are the two principle concepts that are placed in opposition to each other in an integrative theory of addiction. The competing neuro-behavioral decision systems hypothesis (Bickel et al., 2007; Bickel and Yi, 2009) is a new theory which proposes that substance abuse is due to a hyperactive impulsive system and/or a hypoactive executive system in the brain. As the present laboratory model of relapse engages participants' tendency to be impulse-controlled immediate consumers and also their tendency to be executive-functioning delay-influenced consumers it may be a particularly useful vehicle for studying substance abuse from the perspective of the competing neuro-behavioral decisions systems hypothesis.
The results of the present experiment suggest a potential issue for laboratory models of relapse and how it may be addressed in future research. The laboratory relapse-time measure should be highly sensitive to independent variables that affect relapse behavior, while the distribution of relapse times produced should be related in a useful way to a natural phenomenon worthy of study. Our increasing-amount schedule, for example, produced relapse times that were insensitive to the required pre-visit 6-hour period of abstinence, as the relapse times were clustered late in the smoking-room session for that condition. This pattern of delayed relapses is opposite to the pattern of early post-cessation relapses to smoking that generally prevails under natural environment conditions. Our results show that the manner in which changes in reinforcement amounts are scheduled clearly affects sensitivity to independent variables. As discussed earlier, decreasing-amount schedules may be used to increase variability and modify the skewness of an experiment's relapse-time distributions, and thus to more accurately simulate relapse-time patterns worthy of study. This model allows for additional procedural changes that may be implemented to address that issue, and others that may come to the fore. These procedural modifications include extending smoking-room session length, modifying the pre-visit nicotine deprivation time, restricting participants' access to time-keeping cues while in the smoking room, modifying the amounts earnable during smoking-room sessions, devising and implementing other algorithms for the scheduling of abstinence-contingent awards, implementing variable-length smoking-room sessions, removing information about amounts earned or earnable for abstinence while in smoking rooms, and modifying the post-session smoke-free wait period.
There is also a question as to the most suitable type of smokers to use in laboratory models of relapse. As participants in this experiment reported no current intention to give up smoking, the “motivational structure” underlying their abstinence in the present model may not, on its face, be similar to that of someone who is trying to give up smoking. While a model will, by definition, have differences from the phenomenon it models, the usefulness of the model is supported ultimately by its ability to simulate and predict clinical phenomena. The present experiment found results in its constant- and increasing-amount conditions comparable to those from outpatient studies that used constant- and increasing-amount schedules to promote smoking abstinence. This comparability of effects adds face validity to the present model (McKee et al., 2006). Behavior in a model situation may also be useful for understanding constructs that underlie substance use behavior. In this study, the relationship between delay discounting and smoking relapse times may reflect the operation of delay of gratification or impulsivity (Bickel et al., 1999) as these influence smoking behavior. These points of similarity add support to an analogy implicit in this model of relapse. Results from the present experiment suggest that while in the smoking rooms, participants consume cigarettes in reaction to present states and also consume them proactive to anticipated deprivation (Bickel and Yi, 2009; Kowal et al., 2008). This is a feature of realistic similarity to the world of cigarette smokers, supporting the external validity of the model of relapse.
However, there are also limitations of this study that speak to affirmation of the external validity of the model of relapse presented here. We have inferred from our behavioral data that our model simulates both retrospective and prospective temporal contingencies that smokers may be faced with in the world outside of the laboratory. Self-report measures about participants' reasons for responding as they did are worthy of consideration for inclusion in future research. Data from such measures may support inferences about what features of smoker's lives the model simulates; or they may alter the interpretation of the behavioral data. And they may suggest modifications of the model designed to more effectively simulate and study specific aspects of smokers' experiences. The use of self-report measures in experiments that model and simulate real-world phenomena in the laboratory may also be a basis for analyzing the relationship between self-report data and the personal experience that is the subject of self-report.
In conclusion, the procedures of this experiment constitute a laboratory model which may be used to study the determinants of the first smoke after a resolution to stop smoking has been formed. This experiment supported existing findings about the relationship of delay discounting to cigarette addiction; and it extended the knowledge about contingency management procedures in general, and as they may be applied particularly to promoting sustained cigarette abstinence under controlled laboratory conditions that attempt to model processes involved in real-world smoking relapse. The model has noteworthy potential as a vehicle for studying the effects on cigarette and other drug consumption by alternative reinforcers (e.g. money), by impulse-inducing past (e.g., deprivation) or present (e.g., cue exposure) events, or by future events (e.g. anticipated deprivation) that may be the objects of executive functioning.
Acknowledgments
This research was supported by National Institute on Drug Abuse Grants R37 DA006526 and R01 DA022386.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Ammons RB, Ammons CH. The Quick test (QT): Provisional manual. Psychological Reports. 1962;11:111–61. [Google Scholar]
- Baker F, Johnson MW, Bickel WK. Delay discounting in current and never-before cigarette smokers: similarities and differences across commodity, sign, and magnitude. J Abnorm Psychol. 2003;112:382–92. doi: 10.1037/0021-843x.112.3.382. [DOI] [PubMed] [Google Scholar]
- Barratt ES. Impulsiveness defined within a systems model of personality. In: Spielberger CD, Butcher JN, editors. Advances in Personality Assessment. Hillsdale, NJ: Erlbaum; 1985. pp. 113–32. [Google Scholar]
- Bickel WK, Marsch LA. Toward a behavioral economic understanding of drug dependence: delay discounting processes. Addiction. 2001;96:73–86. doi: 10.1046/j.1360-0443.2001.961736.x. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Yi R. Temporal discounting as a measure of executive function: Insights from the competing neuro-behavioral decision system hypothesis of addiction. In: Houser D, McCabe K, editors. Neuroeconomics: Advances in health economics and health services research. Bingley, UK: Emerald Publishing; 2009. in press. [PubMed] [Google Scholar]
- Bickel WK, DeGrandpre RJ, Hughes JR, Higgins ST. Behavioral economics of drug self-administration. II. A unit-price analysis of cigarette smoking. J Exp Anal Behav. 1991;55:145–54. doi: 10.1901/jeab.1991.55-145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Odum AL, Madden GJ. Impulsivity and cigarette smoking: delay discounting in current, never, and ex-smokers. Psychopharmacology (Berl) 1999;146:447–54. doi: 10.1007/pl00005490. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Kowal BP, Gatchalian KM. Understanding addiction as a pathology of temporal horizon. Behavior Analyst Today. 2006;7:32–47. [Google Scholar]
- Bickel WK, Miller ML, Yi R, Kowal BP, Lindquist DM, Pitcock JA. Behavioral and neuroeconomics of drug addiction: competing neural systems and temporal discounting processes. Drug Alcohol Depend. 2007;90 1:S85–91. doi: 10.1016/j.drugalcdep.2006.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Yi R, Kowal BP, Gatchalian KM. Cigarette smokers discount past and future rewards symmetrically and more than controls: is discounting a measure of impulsivity? Drug Alcohol Depend. 2008;96:256–62. doi: 10.1016/j.drugalcdep.2008.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bouton ME. Learning and behavior: A contemporary synthesis. Sunderland, Massachusetts: Sinauer Associates, Inc. Publishers; 2007. [Google Scholar]
- Brandon TH, Tiffany ST, Obremski KM, Baker TB. Postcessation cigarette use: the process of relapse. Addict Behav. 1990;15:105–14. doi: 10.1016/0306-4603(90)90013-n. [DOI] [PubMed] [Google Scholar]
- Carroll ME, Lac ST, Nygaard SL. A concurrently available nondrug reinforcer prevents the acquisition or decreases the maintenance of cocaine-reinforced behavior. Psychopharmacology (Berl) 1989;97:23–9. doi: 10.1007/BF00443407. [DOI] [PubMed] [Google Scholar]
- Dallery J, Raiff BR. Delay discounting predicts cigarette smoking in a laboratory model of abstinence reinforcement. Psychopharmacology (Berl) 2007;190:485–96. doi: 10.1007/s00213-006-0627-5. [DOI] [PubMed] [Google Scholar]
- Donny EC, Bigelow GE, Walsh SL. Assessing the initiation of cocaine self-administration in humans during abstinence: effects of dose, alternative reinforcement, and priming. Psychopharmacology (Berl) 2004;172:316–23. doi: 10.1007/s00213-003-1655-z. [DOI] [PubMed] [Google Scholar]
- Ferster CB, Skinner BF. Schedules of reinforcement. Englewood Cliffs, NJ: Prentice-Hall; 1957. [Google Scholar]
- Garvey AJ, Bliss RE, Hitchcock JL, Heinold JW, Rosner B. Predictors of smoking relapse among self-quitters: a report from the Normative Aging Study. Addict Behav. 1992;17:367–77. doi: 10.1016/0306-4603(92)90042-t. [DOI] [PubMed] [Google Scholar]
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991;86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G. Wisconsin card sorting test manual: revised and expanded. Odessa, FL: Psychological Assessment Reources; 1993. [Google Scholar]
- Heil SH, Johnson MW, Higgins ST, Bickel WK. Delay discounting in currently using and currently abstinent cocaine-dependent outpatients and non-drug-using matched controls. Addict Behav. 2006;31:1290–4. doi: 10.1016/j.addbeh.2005.09.005. [DOI] [PubMed] [Google Scholar]
- Henningfield JE, Stitzer ML, Griffiths RR. Expired air carbon monoxide accumulation and elimination as a function of number of cigarettes smoked. Addict Behav. 1980;5:265–72. doi: 10.1016/0306-4603(80)90049-0. [DOI] [PubMed] [Google Scholar]
- Higgins ST. The influence of alternative reinforcers on cocaine use and abuse: a brief review. Pharmacol Biochem Behav. 1997;57:419–27. doi: 10.1016/s0091-3057(96)00446-7. [DOI] [PubMed] [Google Scholar]
- Higgins ST, Petry NM. Contingency management. Incentives for sobriety. Alcohol Res Health. 1999;23:122–7. [PMC free article] [PubMed] [Google Scholar]
- Higgins ST, Alessi SM, Dantona RL. Voucher-based incentives. a substance abuse treatment innovation. Addict Behav. 2002;27:887–910. doi: 10.1016/s0306-4603(02)00297-6. [DOI] [PubMed] [Google Scholar]
- Higgins ST, Heil SH, Dantona R, Donham R, Matthews M, Badger GJ. Effects of varying the monetary value of voucher-based incentives on abstinence achieved during and following treatment among cocaine-dependent outpatients. Addiction. 2007;102:271–81. doi: 10.1111/j.1360-0443.2006.01664.x. [DOI] [PubMed] [Google Scholar]
- Hughes JR, Hatsukami D. Signs and symptoms of tobacco withdrawal. Arch Gen Psychiatry. 1986;43:289–94. doi: 10.1001/archpsyc.1986.01800030107013. [DOI] [PubMed] [Google Scholar]
- Johnson MW, Bickel WK. The behavioral economics of cigarette smoking: The concurrent presence of a substitute and an independent reinforcer. Behav Pharmacol. 2003;14:137–44. doi: 10.1097/00008877-200303000-00005. [DOI] [PubMed] [Google Scholar]
- Johnson MW, Bickel WK. Replacing relative reinforcing efficacy with behavioral economic demand curves. J Exp Anal Behav. 2006;85:73–93. doi: 10.1901/jeab.2006.102-04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson MW, Bickel WK, Baker F. Moderate drug use and delay discounting: a comparison of heavy, light, and never smokers. Exp Clin Psychopharmacol. 2007;15:187–94. doi: 10.1037/1064-1297.15.2.187. [DOI] [PubMed] [Google Scholar]
- Jones BA, Landes RD, Yi R, Bickel WK. Temporal horizon: Modulation by smoking status and gender. Drug Alcohol Depend. 2009 doi: 10.1016/j.drugalcdep.2009.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenford SL, Fiore MC, Jorenby DE, Smith SS, Wetter D, Baker TB. Predicting smoking cessation. Who will quit with and without the nicotine patch. JAMA. 1994;271:589–94. doi: 10.1001/jama.271.8.589. [DOI] [PubMed] [Google Scholar]
- Kirby KN, Petry NM. Heroin and cocaine abusers have higher discount rates for delayed rewards than alcoholics or non-drug-using controls. Addiction. 2004;99:461–71. doi: 10.1111/j.1360-0443.2003.00669.x. [DOI] [PubMed] [Google Scholar]
- Kirby KN, Petry NM, Bickel WK. Heroin addicts have higher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol Gen. 1999;128:78–87. doi: 10.1037//0096-3445.128.1.78. [DOI] [PubMed] [Google Scholar]
- Kowal BP, Bickel WK, Landes RD. Temporal horizons of cigarette satiety: determining the window of time over which recent smoking influences motivation to smoke. Behav Pharmacol. 2008;19:339–46. doi: 10.1097/FBP.0b013e3283096833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madden GJ, Bickel WK. Abstinence and price effects on demand for cigarettes: a behavioral-economic analysis. Addiction. 1999;94:577–88. doi: 10.1046/j.1360-0443.1999.94457712.x. [DOI] [PubMed] [Google Scholar]
- Madden GJ, Petry NM, Badger GJ, Bickel WK. Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: drug and monetary rewards. Exp Clin Psychopharmacol. 1997;5:256–62. doi: 10.1037//1064-1297.5.3.256. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Curry S, Gordon JR. A longitudinal analysis of unaided smoking cessation. J Consult Clin Psychol. 1988;56:715–20. doi: 10.1037//0022-006x.56.5.715. [DOI] [PubMed] [Google Scholar]
- Mazur JE. An adjusting procedure for studying delayed reinforcement. In: Commons ML, Mazur JE, Nevin JA, Rachlin H, editors. Quantitative analysis of behavior : Vol 5: The effect of delay and of intervening events on reinforcement value. Hillsdale, NJ: Erlbaum; 1987. pp. 55–73. [Google Scholar]
- McDonald J, Schleifer L, Richards JB, de Wit H. Effects of THC on behavioral measures of impulsivity in humans. Neuropsychopharmacology. 2003;28:1356–65. doi: 10.1038/sj.npp.1300176. [DOI] [PubMed] [Google Scholar]
- McKee SA, Krishnan-Sarin S, Shi J, Mase T, O'Malley SS. Modeling the effect of alcohol on smoking lapse behavior. Psychopharmacology (Berl) 2006;189:201–10. doi: 10.1007/s00213-006-0551-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mischel W. Toward an integrative science of the person. Annu Rev Psychol. 2004;55:1–22. doi: 10.1146/annurev.psych.55.042902.130709. [DOI] [PubMed] [Google Scholar]
- Mischel W, Shoda Y. A cognitive-affective system theory of personality: reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychol Rev. 1995;102:246–68. doi: 10.1037/0033-295x.102.2.246. [DOI] [PubMed] [Google Scholar]
- Mischel W, Ebbesen EB, Zeiss AR. Cognitive and attentional mechanisms in delay of gratification. J Pers Soc Psychol. 1972;21:204–18. doi: 10.1037/h0032198. [DOI] [PubMed] [Google Scholar]
- Mischel W, Shoda Y, Rodriguez MI. Delay of gratification in children. Science. 1989;244:933–8. doi: 10.1126/science.2658056. [DOI] [PubMed] [Google Scholar]
- Nides MA, Rakos RF, Gonzales D, Murray RP, Tashkin DP, Bjornson-Benson WM, et al. Predictors of initial smoking cessation and relapse through the first 2 years of the Lung Health Study. J Consult Clin Psychol. 1995;63:60–9. doi: 10.1037//0022-006x.63.1.60. [DOI] [PubMed] [Google Scholar]
- Norregaard J, Tonnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22:261–71. doi: 10.1006/pmed.1993.1021. [DOI] [PubMed] [Google Scholar]
- Odum AL, Madden GJ, Bickel WK. Discounting of delayed health gains and losses by current, never- and ex-smokers of cigarettes. Nicotine Tob Res. 2002;4:295–303. doi: 10.1080/14622200210141257. [DOI] [PubMed] [Google Scholar]
- Perry JL, Larson EB, German JP, Madden GJ, Carroll ME. Impulsivity (delay discounting) as a predictor of acquisition of IV cocaine self-administration in female rats. Psychopharmacology (Berl) 2005;178:193–201. doi: 10.1007/s00213-004-1994-4. [DOI] [PubMed] [Google Scholar]
- Petry NM. Delay discounting of money and alcohol in actively using alcoholics, currently abstinent alcoholics, and controls. Psychopharmacology (Berl) 2001;154:243–50. doi: 10.1007/s002130000638. [DOI] [PubMed] [Google Scholar]
- Pomerleau CS, Majchrzak MJ, Pomerleau OF. Paced puffing as a method for administering fixed doses of nicotine. Addict Behav. 1989;14:571–5. doi: 10.1016/0306-4603(89)90078-6. [DOI] [PubMed] [Google Scholar]
- Rodefer JS, Mattox AJ, Thompson SS, Carroll ME. Effects of buprenorphine and an alternative nondrug reinforcer, alone and in combination on smoked cocaine self-administration in monkeys. Drug Alcohol Depend. 1997;45:21–9. doi: 10.1016/s0376-8716(97)01341-0. [DOI] [PubMed] [Google Scholar]
- Roll JM, Higgins ST. A within-subject comparison of three different schedules of reinforcement of drug abstinence using cigarette smoking as an exemplar. Drug Alcohol Depend. 2000;58:103–9. doi: 10.1016/s0376-8716(99)00073-3. [DOI] [PubMed] [Google Scholar]
- Roll JM, Higgins ST, Budney AJ, Bickel WK, Badger GJ. A comparison of cocaine-dependent cigarette smokers and non-smokers on demographic, drug use and other characteristics. Drug Alcohol Depend. 1996a;40:195–201. doi: 10.1016/0376-8716(96)01219-7. [DOI] [PubMed] [Google Scholar]
- Roll JM, Higgins ST, Badger GJ. An experimental comparison of three different schedules of reinforcement of drug abstinence using cigarette smoking as an exemplar. J Appl Behav Anal. 1996b;29:495–504. doi: 10.1901/jaba.1996.29-495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roll JM, Huber A, Sodano R, Chudzynski JE, Moynier E, Shoptaw S. A comparison of five reinforcement schedules for use in contingency management-based treatment of methamphetamine abuse. Psychological Record. 2006a;56:67–81. [Google Scholar]
- Roll JM, Petry NM, Stitzer ML, Brecht ML, Peirce JM, McCann MJ, et al. Contingency management for the treatment of methamphetamine use disorders. Am J Psychiatry. 2006b;163:1993–9. doi: 10.1176/ajp.2006.163.11.1993. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA, Gnys M, Kassel JA, Hickcox M. First lapses to smoking: within-subjects analysis of real-time reports. J Consult Clin Psychol. 1996;64:366–79. doi: 10.1037//0022-006x.64.2.366. [DOI] [PubMed] [Google Scholar]
- Stroop RJ. Studies of interference in serial verbal reactions. Journal of Experimental Psychology. 1935;18:643–62. [Google Scholar]
- Tiffany ST, Drobes DJ. The development and initial validation of a questionnaire on smoking urges. Br J Addict. 1991;86:1467–76. doi: 10.1111/j.1360-0443.1991.tb01732.x. [DOI] [PubMed] [Google Scholar]
- Walsh SL, Geter-Douglas B, Strain EC, Bigelow GE. Enadoline and butorphanol: evaluation of kappa-agonists on cocaine pharmacodynamics and cocaine self-administration in humans. J Pharmacol Exp Ther. 2001;299:147–58. [PubMed] [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54:1063–70. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- Westman EC, Behm FM, Simel DL, Rose JE. Smoking behavior on the first day of a quit attempt predicts long-term abstinence. Arch Intern Med. 1997;157:335–40. [PubMed] [Google Scholar]
- Yoon JH, Higgins ST, Heil SH, Sugarbaker RJ, Thomas CS, Badger GJ. Delay discounting predicts postpartum relapse to cigarette smoking among pregnant women. Exp Clin Psychopharmacol. 2007;15:176–86. doi: 10.1037/1064-1297.15.2.186. [DOI] [PubMed] [Google Scholar]
- Zacny JP, Stitzer ML, Brown FJ, Yingling JE, Griffiths RR. Human cigarette smoking: effects of puff and inhalation parameters on smoke exposure. J Pharmacol Exp Ther. 1987;240:554–64. [PubMed] [Google Scholar]