

Abstract
We report the case of a 31-year-old male presenting with complaints of mild pain in the right ear for three months and hypoacusis for 10 days. On otoscopic examination, a thin, papery, white material was extracted from his ear and sent for fungal identification. This material revealed presence of Malassezia spp – with characteristic “spaghetti and meat ball appearance”. The patient was treated with 2% acetic acid, hydrocortisone and Clotrimazole powder for one week and he resolved completely.
Keywords: Malassezia, Otitis externa, Otomycosis
INTRODUCTION
Otomycosis is an acute, subacute or chronic fungal infection of the pinna, external auditory meatus and the ear canal. Factors that predispose to otomycosis include absence of cerumen, humid climate, increased temperature, instrumentation of the ear and increased use of topical antibiotic/steroid preparations. Aspergillus niger and Candida albicans are the most common causative agents of otomycosis. Here we present an unusual case of chronic otomycosis caused by Malassezia species.
HISTORY
A 31-year-old non-diabetic male presented with history of chronic otitis externa in the right ear for three months. He gave a history of using antibacterial eardrops on and off for last three months but with no effect. He complained of mild pain in the ear (on and off) for three months and hypoacusis for 10 days. He gave no history of tinnitus. On examination, the ear was dry with no discharge. Otoscopic examination revealed that the external meatus was plugged with abundant wax and was removed. After removal of the ear wax, a thin white papery material was extracted and was sent for fungal identification. Audiology examination showed he had a mild hearing loss of 25-30 db. The patient had no history of any other skin infection. He also gave history of having a pet dog at home.
The extracted white material was sent to the Microbiology department for fungal identification. The sample was examined under 10% KOH (Potassium Hydroxide) mount and inoculated on to SDA (Sabouraud's Dextrose Agar) for culture. 10% KOH mount revealed clusters of round yeast cells 2-7 μ in size with occasional budding. The hyphae were blunt, short, stout and curved- the characteristic “spaghetti and meat ball” appearance was observed, which was diagnostic of Malassezia spp. Malassezia spp. was identified based to their characteristic morphological features. Gram staining and Giemsa staining of the specimen also confirmed the same “spaghetti and meat ball” appearance. [Figure 1]. Several attempts were made to cultivate the organism on SDA overlaid with olive oil but all the attempts were futile.
Figure 1.
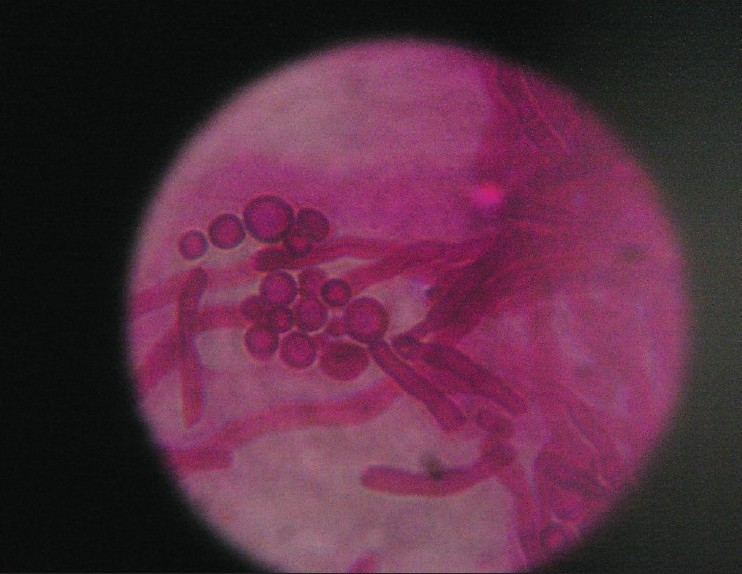
Malassezia species showing short hyphae and clusters of yeast cells occasional budding (Giemsa × 400)
DISCUSSION
Although otomycosis has worldwide occurrence, its frequency is variable and depends on different climatic, occupational and socio-economic conditions.[1] Fungi are identified in about 10% of otomycosis cases.[2] The most common fungal etiological agents are Aspergillus spp. (80-90% of cases) and Candida spp.[3]
The genus Malassezia comprises a group of superficial fungi occurring as normal skin flora on the human body around the areas that are rich in sebaceous glands, but they are also known to cause infections or associated with certain skin diseases. Rarely, they become invasive and cause opportunistic infections under certain conditions. Their association with infection of external auditory canal (EAC) is uncommon however their role in the other human infections is gaining importance with the increase in the number of reports on Malassezia spp. infections in human.[4] Classically, prolonged treatment for bacterial otitis externa with topical antibiotics alters the flora of the ear canal and is also promycotic. Alterations in normal microflora in the ear and skin from prior or concurrent antibiotic therapy play a role as predisposing factors in allowing the overgrowth of Malassezia organisms.[3] Here, in this case report, history of prolonged use of antibacterial ear drops could be a possible explanation for otomycosis (Malassezia). However, reports also elucidate that fungus can occasionally be the primary pathogen, especially in the presence of excessive moisture or heat.[5] Malassezia spp. is commonly isolated from pet dogs and reports of otitis externa in dogs and cats are well known.[6,7] The source of infection for this patient is likely to have come from his pet dog. Dogs are the natural host for Malassezia spp., the potential for human exposure to the organism is therefore quite great and zoonotic transfer has been documented from dogs to immunocompromised patients by healthcare workers.[8] This supports our hypothesis that active Malassezia infection of canine skin or ear canals can become a risk factor for human carriage. Treatment of the patient was done in three steps; cleansing and debriding the ear of debris and lipid substrates, acidifying the canal with topical solution of 2% acetic acid and administration of antifungal agent clotrimazole powder for one week.[9] The patient resolved completely in two weeks.
CONCLUSION
This case report indicates the importance and need for including Malassezia species in differential diagnosis of fungal otitis externa, especially with persons having close association with pet animals. This study also further reveals the indispensible importance of KOH examination in cases where the fungi involved is not easily cultivable. It is concluded that further detailed studies are necessary to confirm the transmission of Malassezia spp. from dogs to humans and role of Malassezia as an emerging pathogen.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Jalali AM. Study the prevalence of superficial fungal diseases, Rasht, Iran. J Faculty Medicine Guilan Univ Med Sci. 1991;10:245–52. [Google Scholar]
- 2.Bojrab DI, Bruderly T, Abdulrazzak Y. Otitis externa. Otolaryngol Clin North Am. 1996;29:761–82. [PubMed] [Google Scholar]
- 3.Lucente FE. Fungal infections of the external ear. Otolaryngol Clin North Am. 1993;26:995–1006. [PubMed] [Google Scholar]
- 4.Jagdish Chander. Text Book of Medical Mycology. 2nd ed. Mehta Publishers; 2002. pp. 69–79. [Google Scholar]
- 5.Sander R. Otitis externa: a practical guide to treatment and prevention. Am Fam Physician. 2001;63:927-36941–2. [PubMed] [Google Scholar]
- 6.Crespo MJ, Abarca ML, Cabañes FJ. Otitis Externa associated with Malassezia sympodialis in two cats. J Clin Microbiol. 2000;38:1263–6. doi: 10.1128/jcm.38.3.1263-1266.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Morris DO, O'Shea K, Shofer FS, Rankin S. Malassezia pachydermatis carriage in dog owners. Emerg Infect Dis. 2005;11:83–8. doi: 10.3201/eid1101.040882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kwok P, Hawke M. Clotrimazole powder in the treatment of otomycosis. J Otolaryngol. 1987;16:398. [PubMed] [Google Scholar]
- 9.Chang HJ, Miller HL, Watkins N, Arduino MJ, Ashford DA, Midgley G, et al. An epidemic of Malassezia pachydermatis in an intensive care nursery associated with colonization of health care workers' pet dogs. N Engl J Med. 1998;338:706–11. doi: 10.1056/NEJM199803123381102. [DOI] [PubMed] [Google Scholar]