

Deep brain stimulation (DBS) of the medial thalamic nuclei and globus pallidus internus (GPi)1,2 has been tried in the treatment of medically refractory Tourette syndrome (TS). Subthalamic nucleus (STN) is the target most commonly used for DBS in Parkinson disease (PD). A double-blind randomized study has shown the efficacy of STN-DBS in obsessive compulsive disorder (OCD),3 which is considered within the spectrum of TS.
We report a patient with PD who also had a history of TS in whom bilateral STN-DBS improved both PD and tics.
Case report.
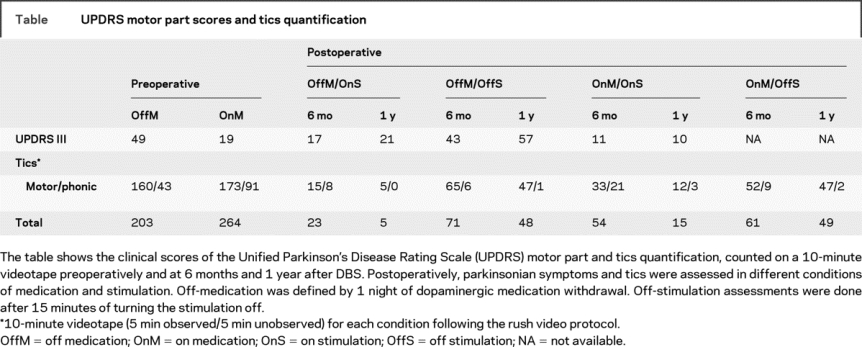
A 38-year-old man with an 8-year history of PD was referred for DBS consideration. He had a history of tics that began at the age of 7 and improved by the age of 12. Tics increased in adulthood prior to the diagnosis of PD. No changes of tics were noticed following the onset of PD or dopaminergic medication. No treatment for tics was ever prescribed. Prior to surgery he had motor and phonic tics and compulsion of checking that doors were locked. A single exon 5 deletion in the parkin gene was detected. Quadripolar 3389 DBS electrodes (Medtronic, Minneapolis, MN) were implanted bilaterally in the STN under local anesthesia and connected a few days later to a pulse generator (Kinetra®, Medtronic). The position of each electrode’s contact was calculated using preoperative and postoperative stereotactic MRI and the software Framelink (Medtronic). The active contacts were located in the dorsal tip of the STN on the left side and adjacent to the medial border of the center of the STN on the right. Stimulation was monopolar with pulse width 60 μsec and frequency 130 Hz. Amplitude was progressively increased over time to 3.0 volts for the left STN and 3.2 for the right, in parallel with a reduction in dopaminergic medication. The patient reported a subjective amelioration of tics before stimulation was started. An improvement of both tics and parkinsonian symptoms was observed once the stimulation was initiated. At 1 year, STN DBS produced a 57% improvement in the motor part of the Unified Parkinson’s Disease Rating Scale and allowed a 56% reduction in dopaminergic medication dosage. Tics frequency diminished by 89% at 6 months and 97% at 1 year, counted on a 10-minute videotape by a blinded investigator. Switching off the stimulation produced an immediate increase in tic frequency (table). The compulsion improved but did not resolve completely.
Table UPDRS motor part scores and tics quantification
Discussion.
Coexistence of TS and PD has previously been described, with the evolution of PD or dopaminergic medication having variable effects on TS manifestations.4 Although the more than 50% reduction in dopaminergic medication could in part explain the improvement of tics, the immediate deterioration in tics frequency after switching off the stimulation suggests a direct impact of STN stimulation. The remaining improvement observed in the off-stimulation assessment compared to preoperative could be explained by a long-term tic-suppressant effect of STN DBS, as stimulation was left off only for 15 minutes. A microlesion effect could account for the amelioration reported by the patient prior to stimulation onset.
From a physiologic perspective, STN occupies a privileged position influencing both output nuclei of the basal ganglia, GPi and substantia nigra (SN) reticulata. Several findings link the STN with behavioral changes that may improve with STN-DBS.3 François et al.5 found that stereotyped behaviors in nonhuman primates, resembling tics and compulsive disorders, were related to dysfunction of the limbic parts of the globus pallidus externus, the STN, and the SN reticulata, rather than to dysfunction of the GPi. Involvement of the SN in TS was also found in a functional MRI study.6 Furthermore, stimulation of the anterior STN was effective in reducing stereotypes in a primate model of behavioral disorder7 and STN DBS in PD can also result in behavioral changes. Indeed, the small size of this nucleus may allow modulation of abnormal neuronal activity of both limbic and sensorimotor territories, more easily than GPi or thalamic DBS.
This report suggests that the STN may be a potential target for DBS in TS. STN-DBS would allow modulation of both limbic and sensorimotor territories and may provide a quicker relief of symptoms than medial thalamic nuclei or GPi stimulation.
The University College London Hospitals and University College London (UCLH/UCL) receive a proportion of funding from the Department of Health’s National Institute for Health Research (NIHR) Biomedical Research Centres funding scheme. The Unit of Functional Neurosurgery is supported by the Parkinson’s Appeal. I.M.T. is supported by a Postgraduated Grant of the Fundacion Caja Madrid.
Disclosure: The authors report no disclosures.
Medical Devices: Pulse generator (Kinetra®) and quadripolar 3389 DBS electrodes (Medtronic, Minneapolis, MN).
Received October 2, 2008. Accepted in final form January 30, 2009.
Address correspondence and reprint requests to Dr. Irene Martinez-Torres, 33 Queen Square, Box 146, WC1N 3BG, London, UK; i.torres@ion.ucl.ac.uk
&NA;
- 1.Ackermans L, Temel Y, Visser-Vandewale V. Deep brain stimulation in Tourette’s syndrome. Neurotherapeutics 2008;5:339–344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Welter ML, Mallet L, Houeto JL, et al. Internal pallidal and thalamic stimulation in patients with Tourette syndrome. Arch Neurol 2008;65:952–957. [DOI] [PubMed] [Google Scholar]
- 3.Mallet L, Polosan M, Nermatollah J, et al. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. N Engl J Med 2008;359:2121–2134. [DOI] [PubMed] [Google Scholar]
- 4.Kumar R, Lang AE. Coexistence of tics and parkinsonism: evidence for non-dopaminergic mechanism in tic pathogenesis. Neurology 1997;49:1699–1701. [DOI] [PubMed] [Google Scholar]
- 5.François C, Grabli D, McCairn K, et al. Behavioural disorders induced by external globus pallidus dysfunction in primates II: anatomical study. Brain 2004;127:2055–2070. [DOI] [PubMed] [Google Scholar]
- 6.Bohlhalter S, Goldfine A, Matteson S, et al. Neuronal correlates of tic generation in Tourette syndrome: an event-related functional MRI study. Brain 2006;129:2029–2037. [DOI] [PubMed] [Google Scholar]
- 7.Baup N, Grabli D, Karachi C, et al. High-frequency stimulation of the anterior subthalamic nucleus reduces stereotypes behaviours in primates. J Neurosci 2008;27:8785–8788. [DOI] [PMC free article] [PubMed] [Google Scholar]