

Abstract
Background
With more single mothers entering the workforce due to welfare reform efforts, more hospitalized children from single-parent families will have experienced alternate child care arrangements where routine care is provided by adults other than the child’s mother.
Objectives
To investigate with secondary analysis of data whether experience with alternate child care has a moderating effect on the relationship between hospitalization and behavior of preschool children living in female-headed single-parent families.
Method
A sample of 60 preterm and 61 full-term children who were 3,4, or 5 years old was recruited for the larger longitudinal study. Behavior problems were measured with the Child Behavior Checklist. History of hospitalization and alternate child care arrangements were measured with the Life History Calendar.
Results
Preschool children who experienced hospitalization without alternate child care experience had more somatic complaints, but those with both hospital and alternate child care experience had fewer aggressive behaviors than other children. For children with a history of hospitalization, aggressive behaviors decreased as the proportion of the child’s life in alternate child care increased.
Conclusions
Experience with alternate child care may ameliorate some of the negative effects of hospitalization, and potentially other novel and negative experiences, for preschool children. This could be due to child care providing positive experiences with separation from the mother, a peer group with which to talk about the novel experience, or actual instruction about the novel experience.
Keywords: child behavior, child care, hospitalization, single-parent families
Hospitalization of a child is a stressful event for both parent and child. In his review of the research, Thompson (1985) concluded that children have negative reactions to hospitalization, including night terrors, feeding disturbances, loss of newly acquired developmental skills, and intolerance of separation from the mother, that persist for months after the child’s discharge. Despite efforts to make the hospital more child- and family-focused, preschoolers in a recent study also demonstrated distress 1 week after hospital discharge, including irritability, nightmares, appetite changes, and separation anxiety (Rossen & McKeever, 1996). Separation from the parents (primarily the mother), age of the child, and parental anxiety have been implicated as affecting the child’s reaction after hospital discharge. However, most of this research was conducted prior to 1980 when maternal employment and, thus, experience with separation from the mother and alternate child care (routine care provided by adults other than the child’s mother) at an early age was less common.
According to Bowlby (1969/1982), children look to their primary attachment figures, generally their mothers, in times of stress, such as when they are frightened, tired, or ill. The stress of hospitalization for children is likely due to the fear caused by the child’s separation from the mother and care by nonparental adults as well as the child’s illness. Experience with separation from the mother and care by nonparental adults when the child is not ill may reduce the novelty and fear caused by hospitalization. Thus, experience with alternate child care could act as a buffer for the negative effects of hospitalization.
Conversely, although research suggests that daily mother-child separations due to the mother’s employment have no negative effects for children of any age (Hoffman, 1989), it also is possible that separation for employment is a low-level stressor that, when added to the major stressor of hospitalization, pushes the child’s stress to an unmanageable level. In that case, return to alternate child care after hospitalization might prolong or exacerbate any negative effects of hospitalization. With 50% of single mothers with preschoolers in the workforce (U. S. Bureau of the Census, 1992) and the expected increase in this rate due to welfare reform efforts, more hospitalized children from single-parent families will have experience with nonmaternal care. However, the effects of experience with alternate child care on behavioral outcomes for hospitalized children are unknown.
Relevant Literature
Research on children’s reactions after hospitalization clearly indicates that hospitalization is a stressful event for children and that negative effects can continue for months or years after discharge. In the seminal study by Prugh, Staub, Sands, Kirschbaum, and Lenihan (1953), a sizable proportion of preschool and school-age children who experienced “routine” ward conditions had “significant” negative reactions immediately after discharge (92%) and at 3 months (58%). Most subsequent studies have found posthospitalization upset at 1 to 4 weeks after discharge (Brain & Maclay, 1968; Couture, 1976; Goslin, 1979; Mahaffy, 1965; Melnyk, 1994; Rossen & McKeever, 1996; Sides, 1977; Sipowicz & Vernon, 1965; Wolfer & Visintainer, 1975, 1979). However, two other studies have found normal behavior in children after hospitalization (Carson, Council, & Gravley, 1991; Simons, Bradshaw, & Silva, 1980).
Age of the child frequently has been related to posthospitalization upset, with younger children having more severe negative reactions than older children (Brain & Maclay, 1968; Sides, 1977; Simons et al., 1980). Wolfer and Visintainer (1975, 1979) found no age effects in their first experiment, but saw age-by-treatment effects in a later experiment. Tiedeman and Clatworthy (1990) found that older children (8 to 11 years old) experienced a decrease in anxiety through 7 to 14 days after hospital discharge, but 5- to 8-year-old children did not.
Several investigators have found that posthospitalization behavior of preschool or school-age children was not related to the number of previous hospital admissions (Menke, 1981; Simons et al., 1980; Tiedeman & Clatworthy, 1990). However, Elander, Nilsson, and Lindberg (1986) found that 4-year-old children with a history of two or more hospitalizations displayed more somatic symptoms; oral tendencies; and dependent, aggressive, and hyperactive behaviors than children with only one hospitalization. Findings regarding the effect of length of hospital stay also vary. Although Menke and Simons et al. found no relationship between length of stay and child behavior, Tiedeman and Clatworthy found greater anxiety in 5- to 11-year-old children with shorter lengths of stay.
Two studies found significant differences in behavior and coping strategies based on experience with separation. Elander et al. (1986) found an interaction effect of daycare attendance and hospitalization on behavior of 4-year-old Swedish children. Daycare children who had been hospitalized sometime since birth displayed more aggressive, hyperactive/impulsive, dependent, and regressive behaviors than daycare children who had not been hospitalized. Children had these reactions even though 116 (50.2%) of the 231 admissions had lengths of stay of 3 or fewer days; 35 (15.2%) of these were overnight stays.
Children experience separation when they start school, around the age of 5 or 6 years. In a sample of 3- to 7-year-olds (N = 24), Corbo-Richert (1994) found that older children and those with school experience used more information-seeking coping strategies to deal with chest tube removal than younger children and those without school experience; previous experience with hospitalization did not influence choice of coping strategies. However, it is not clear whether these results are due to age of the child or to the effects of separation from having entered elementary school.
In summary, the negative behavioral effects of hospitalization for children are well-known. However, whether experience with alternate child care and, therefore, routine separation of the child from the mother, has a moderating effect on the relationship between hospitalization and child behavior is not known. A sample of preterm and full-term preschoolers living in female-headed single-parent families from a larger, longitudinal study on the effects of maternal employment for preschoolers in single- and two-parent families (Youngblut, Singer, & Rodgers, 1997) was used to examine this question for several reasons. Single mothers are twice as likely to have a preterm birth than married mothers (National Center for Health Statistics, 1995). Research suggests that preterm children are more negatively affected by environmental stressors (Tobey & Schraeder, 1990). Preterm infants and children are more likely to experience hospitalization than full-terms. The research question for this secondary analysis was: Does experience with separation from the mother due to alternate child care moderate the negative effects of hospitalization on preschool children’s behavior?
Thus, the purpose of this study was to examine the interaction effects of alternate child care experience on the relationship between hospitalization and behavior of preschool children living in female-headed single-parent families.
Method
Sample
The sample for this study consisted of 121 female-headed, single-parent families, with 60 preterm and 61 full-term preschoolers (3, 4, or 5 years old). Families with preterm preschoolers were identified from the admission records of three Level III neonatal intensive care units (NICUs); families with full-term preschoolers were identified from birth records of two normal newborn nurseries. A systematic random sample of families with full-terms and all families with preterms from four consecutive birth years were sent a letter that briefly described the study. Interviews were conducted within a month of the child’s third, fourth, or fifth birthday.
Single-parent families were eligible to participate if the mother had not lived with a man in the father role for at least 6 months prior to recruitment. Five index children were being raised by a single woman other than the birth mother (1 by adoptive mother, 2 by grandmothers, and 2 by foster mothers). In each case, the child had lived with the family for most of the child’s life and the woman was performing the role of mother to the child. Thus, these women are referred to here as “mothers.”
Inclusion criteria for the preterm child in the family were: (a) born prior to 36 weeks gestation weighing less than 2,500 grams; (b) appropriate weight for gestational age; and (c) hospitalized for at least 1 week in a Level III NICU. Inclusion criteria for the full-term child in the family were: (a) birth between 38 and 42 weeks gestation; (b) discharged home with the mother after birth; and (c) no preterm siblings that were born within 10 years of the study child’s birth. Children whose mothers were told the child had more than a 2-year developmental delay were excluded. None of the families contacted were excluded on this basis. Of the families contacted and eligible to participate in the larger study, 71% agreed to participate.
Sample demographics are listed in Table 1. The sample had approximately equal numbers of male and female children. Birthweight and gestational age of the preterm and full-term groups reflected study inclusion criteria. In the preterm group, there were 25 (41.7%) low birth weight (LBW; 1,500–2,500 gms), 23 (38.3%) very LBW (1,000–1,499 gms), and 12 (20%) extremely LBW (<1,000 gms) children. Average length of stay in the NICU at birth was 46.1 days (SD = 33.34; range, 4 to 128). Few had experienced complications of prematurity. Thirteen had had an intraventricular hemorrhage (10 with Grade I, and one child each with Grades II, III, and IV). Two children had been diagnosed with cerebral palsy and two with bronchopulmonary dysplasia (BPD). At the time of the study, one child with BPD was using an aerosol machine for asthma, and the other child with BPD did not require any special equipment.
TABLE 1.
Demographics for Preterm and Full-term Groups
| Preterm (n = 60) | Full-term (n = 61) | Statistic | |
|---|---|---|---|
| Child age (months) | 48.7 (9.92) | 48.4 (9.96) | t = .18 |
| Birth weight (g) | 1444.1 (527.21) | 3331.3 (514.18) | t = 19.93* |
| Gestational age (weeks) | 30.5 (3.17) | 39.6 (1.60) | t = 19.98* |
| Child’s gender | |||
| Male | n = 28 | n = 36 | χ2 = 1.85 |
| Female | n = 32 | n = 25 | |
| Mother’s age | 29.9 (6.86) | 29.2 (6.17) | t = .58 |
| Mother’s race | |||
| African American | n = 44 | n = 36 | χ2 = 4.05 |
| Caucasian | n = 16 | n = 23 | |
| Hispanic | n = 0 | n = 2 | |
| Mother’s education | |||
| < High school | n = 12 | n = 16 | χ2 = 1.15 |
| High school graduate | n = 20 | n = 22 | |
| > High school | n = 28 | n = 23 | |
| Family income | |||
| < $20,000 | n = 57 | n = 60 | χ2 = 5.23 |
| $20,000–$40,000 | n = 6 | n = 1 | |
| > $40,000 | n=1 | n = 0 | |
p<.01.
Most of the mothers were African American (66.1%), never married (70.2%), high school graduates (76.9%), and living in poverty (68.6%). Number of children in the family ranged from 1 to 8, including the study child (M = 2.5, SD = 1.44).
Instruments
Child behavior
The Child Behavior Checklist (CBCL) (Achenbach, 1991) was used to measure child behavior. It contains two behavior problems scales (internalizing, externalizing). The internalizing scale contains three subscales: anxious/depressed; somatic complaints; and withdrawn. The externalizing scale contains two subscales: aggressive and delinquent behavior. Mothers rated their child on each of 118 behaviors on a 3-point scale ranging from not true to often true. Scale and subscale scores were obtained by summing the mothers’ ratings. Normed scores, based on child age and gender, then were obtained with the Revised Child Behavior Profile sheet. The CBCL has been widely used with a variety of populations, including LBW children and African American children, with documented evidence for its construct validity (Achenbach). Achenbach reports moderate to strong correlations between the CBCL’s internalizing and externalizing scales and similar scales of the Quay-Peterson (.52–.88). Achenbach reports test-retest reliabilities of .82 to .95 and internal consistency reliability estimates of .90 and .93 for the internalizing and externalizing scales, respectively. For this sample, the alpha coefficients were .83 and .91 for the internalizing and externalizing scales, respectively, and ranged from .58 to .89 for the subscales.
Experience with hospitalization and alternate child care
Mothers indicated when the index child was in the hospital and the lengths of stay for each hospitalization on a Life History Calendar (LHC) (Freedman, Thornton, Camburn, Alwin, & Young-DeMarco, 1988). From that data, number of hospitalizations, total number of days hospitalized, and age at last hospitalization were derived. Additionally, mothers used the LHC to indicate the child’s alternate child care experiences, including timing, duration, and types of alternate child care providers. Alternate child care experiences were defined as situations where routine child care was provided by adults other than the child’s parent(s), primarily for the mother’s employment. Episodic baby-sitting to allow the parent(s) to go out for a few hours were not considered alternate child care experiences. From these data, number of different child care arrangements and proportion of the child’s life in child care were derived. In addition to these interval-level variables, two dichotomous variables also were created: experience with hospitalization (yes/no) and experience with alternate child care (yes/no).
Validity and reliability of the LHC is enhanced through its use of memory cues, relating one event to other events that occurred at about the same time. When Freedman et al. (1988) compared data obtained in 1980 about the respondent’s current situation with data obtained retrospectively with the LHC in 1985 (N = 900), agreement ranged from 72% to 92%. The LHC constructed for the current study contained five segments (years), each with 12 blocks (months). Major life events, such as residential moves, births, and deaths also were recorded to aid the mother’s memory. Recording began with the month and year of the study child’s birth.
Procedure
The study was approved by the appropriate human subjects review committees at the university and each of the three hospitals. Interviewers were trained to administer a set of parent interview and self-complete instruments and developmental tests for the larger study. Within 2 weeks after an introductory letter was mailed, interviewers contacted each family to screen for inclusion criteria, answer questions, and schedule a home visit for data collection. Interviewers offered to read self-complete instruments to parents; parents and children were encouraged to take short breaks as necessary.
Results
More children experienced alternate child care (n = 67) than hospitalization (n = 35). Children with alternate child care experience had spent an average of 28.5 months (SD = 17.2) in up to four different arrangements (M = 1.37, SD = .62). Types of child care arrangements included care in the home by relatives (n = 30, 25.2%) and nonrelatives (n = 8, 6.7%), family daycare (n = 13, 10.8%), and an organized daycare facility (n = 39, 32.8%). Number of hospital admissions ranged from 1 to 18 (M = 1.9, SD = 2.90), days in hospital ranged from 1 to 355 (M = 30.8, SD = 66.78), and time since last admission ranged from 3.4 to 59.7 months (M = 33.7, SD = 18.57) for those who had been hospitalized. Children who had experienced only hospitalization did not differ from children who had both hospital and child care experiences on number of admissions or number of days hospitalized, t(33) = .79 and t(31) = 1.19, respectively, p = NS. However, children with only hospital experience had been hospitalized more recently than children with both hospital and alternate child care experience (months since last admission; M = 26.0, SD = 16.81 vs. M = 39.5, SD = 18.08, respectively), t(33) = 2.25, p =.03.
Gestational status (preterm vs. full-term) was related to child care-by-hospital experience group (hospital only, child care only, neither or both hospital and child care), chi square (3, N = 119) = 15.27, p < .01, primarily because more preterm than full-term preschoolers had been hospitalized (27 vs. 8). The numbers of preterm and full-term preschoolers who had experienced alternate child care were similar (34 vs. 32). Number of different child care arrangements and months spent in alternate child care were similar for preterms and full-terms, t(118) = .88 and .92, respectively, p = NS. However, preterm preschoolers experienced a greater number of hospitalizations and spent more days in the hospital than full-terms, t(60.5) = 2.63 and t(57.3) = 2.27, respectively, p < .05. Separate variance estimates of the t values were used for these two comparisons due to unequal group variances. Time since last hospitalization was similar for preterm and full-term preschoolers, t(34) = 1.50, p = NS.
Two-way ANOVA1 was used to examine the interaction (moderating) effects of experience with hospitalization and child care on the subscales of the CBCL internalizing and externalizing behavior problems scales, controlling for gestational status and race. The interaction effect of experience with alternate child care and hospitalization was significant for somatic complaints, F(1, 105) = 8.40, p = .005, and aggressive behaviors, F(1, 105) = 5.70, p = .02. Children who had experienced hospitalization but not alternate child care had higher somatic complaints than other children (Figure 1). Children who had experienced both hospitalization and alternate child care had lower aggressive behavior scores than other children (Figure 2).
FIGURE 1.
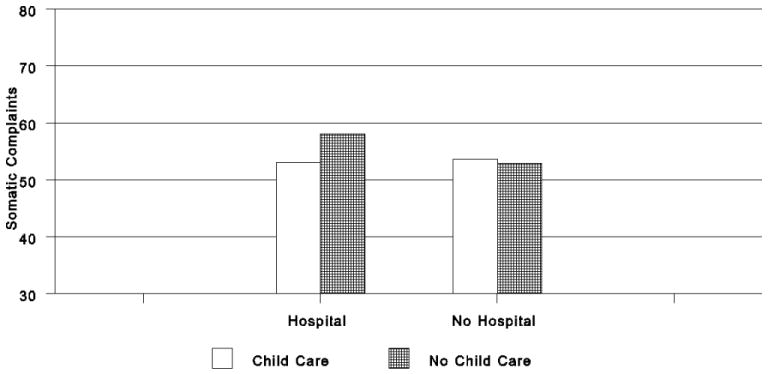
Somatic complaints for children with and without child care experience.
FIGURE 2.
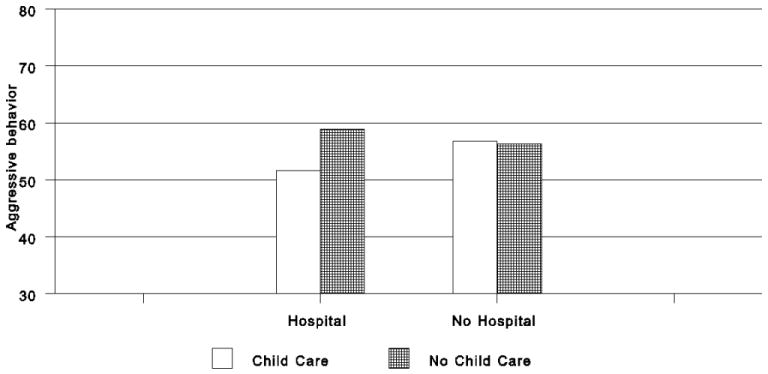
Aggressive behaviors for children with and without child care experience.
To further explore the effects of hospitalization, additional analyses were conducted with data collected from the children who had experienced a hospital stay. Correlations between child behavior subscales and aspects of the child’s experience with hospitalization (number of admissions, total number of days hospitalized, age at last admission, and months since last admission) and child care (proportion of child’s life in alternate care) were examined (Table 2). More recent hospitalization and older age at last hospitalization were related to more aggressive behaviors. However, greater proportion of the child’s life in alternate child care was associated with fewer aggressive behaviors and somatic complaints.
TABLE 2.
Correlations Between Child Development Measures and Hospital and Child Care Experience Indicators (n =35)
| No. of Hospital Admissions | No. of Days Hospitalized | Age at Last Admission | Time Since Last Hospital Admission | Proportion of Child’s Life in Alternate Child Care | |
|---|---|---|---|---|---|
| Anxious/depressed | −.01 | −.04 | .27 | −.26 | −.18 |
| Somatic complaints | .07 | −.07 | .28 | −.22 | −.35* |
| Withdrawn | −.05 | .17 | .07 | −.18 | −.14 |
| Aggressive | .01 | .18 | .45** | −.45** | −.40* |
| Delinquent behavior | −.05 | −.04 | .32 | −.25 | −.21 |
p < .05;
p < .01.
Discussion
In this study, experience with alternate child care and hospitalization had an interaction effect on behavior problems of preschool children regardless of the child’s gestational status at birth. Elander et al. (1986) also found an interaction effect of these two factors. Children in our study who had a history of hospitalization had more somatic complaints. Since these children also had been hospitalized more recently than those with both hospital and child care experiences, this finding could reflect the effects of the child’s more recent illness or an underlying chronic illness. However, because children with both experiences had scores similar to those who had not been hospitalized at all, this finding may reflect a protective effect of experience with alternate child care. That is, experience with child care and, therefore, experience with routine separations from the mother may decrease the negative effects of hospitalization on the child.
Preschool children who had experienced both hospitalization and alternate child care displayed fewer aggressive behaviors than other children in our study. In contrast, Elander et al. (1986) found that 4-year-old daycare children with a history of hospitalization displayed more aggressive behaviors than daycare children without a history of hospitalization. The effects for aggressive behaviors and somatic complaints are in the same direction, although the mean for children with hospital experience only is similar to the mean for children without a history of hospitalization regardless of child care status. Thus, something about having both experiences makes the child less aggressive.
Although effects of hospitalization on preschool children’s behaviors were not related to number of hospitalizations or length of hospital stay, timing of the last hospitalization was important. Children whose last hospitalization was at a younger age and less recent displayed less aggressive behavior. Menke (1981), Simons et al. (1980), and Tiedeman and Clatworthy (1990) also found no effect of number of admissions or length of stay, although Elander et al. (1986) found more behavioral dysfunction in Swedish children with more hospitalizations. In our study, experience with alternate child care again appears to be protective. For children who had been hospitalized, amount of aggressive behavior and somatic complaints decreased as the proportion of the child’s life in alternate child care increased. Thus, greater experience with alternate child care may ameliorate some of the negative psychological effects of hospitalization.
A limitation of this study is that effects of different types of alternate child care situations as well as the quality of these child care arrangements were not considered. The emphasis of the programming in organized daycare has been found to improve cognitive performance, especially for children from low-income families (Caughy, DiPietro, Strobino, 1994). Quality of the child care arrangement has been found to affect cognitive development (Burchinal, Roberts, Nabors, & Bryant, 1996; Pierrehumbert, Ramstein, Karmaniola, & Halfon, 1996). However, research on the effects of quality of child care on the behavior of children from low-income families is lacking.
In summary, preterm preschoolers were more likely to have been hospitalized than full-term preschoolers; however, they were equally likely to have experienced alternate child care. Experience with alternate child care had a protective effect for preschoolers who also had been hospitalized, regardless of gestational status. For those with hospital experience, number of hospitalizations and duration of stay were not related to child behaviors; however, children showed less aggressive behavior as time since last hospitalization increased. Although more research in this area is needed, we speculate that experience with routine separation from the parent for child care diminishes the negative effect of separation from parents during hospitalization and perhaps other types of separation.
Acknowledgments
This study was supported by grant #R01 NR02707 from the National Institute of Nursing Research and an administrative supplement by the Office of Research on Women’s Health through the National Institute of Nursing Research, National Institutes of Health.
Footnotes
An alternate method for testing the interaction effects is to use multiple regression. However, the creation of interaction terms with variables that are not continuous for use in regression analysis is somewhat controversial. Violation of regression assumptions would invalidate the results; therefore, we have chosen to use two-way ANOVA because it assumes that the independent variables are categorical.
Contributor Information
JoAnne M. Youngblut, Associate Dean for Research and an Associate Professor at Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH.
Dorothy Brooten, Dean and John Burry, Jr. Professor at Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- Bowlby J. Attachment and loss, volume 1: Attachment. New York: Basic Books; 1982. (Original work published in 1969) [Google Scholar]
- Brain DJ, Maclay I. Controlled study of mothers and children in hospital. British Medical Journal. 1968;1:278–280. doi: 10.1136/bmj.1.5587.278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burchinal MR, Roberts JE, Nabors LA, Bryant DM. Quality of center child care and infant cognitive and language development. Child Development. 1996;67:606–620. [PubMed] [Google Scholar]
- Carson DK, Council JR, Gravley JE. Temperament and family characteristics as predictors of children’s reactions to hospitalization. Journal of Developmental and Behavioral Pediatrics. 1991;12(3):141–147. [PubMed] [Google Scholar]
- Caughy MO, DiPietro JA, Strobino DM. Daycare participation as a protective factor in the cognitive development of low-income children. Child Development. 1994;65:457–471. [PubMed] [Google Scholar]
- Corbo-Richert BH. Coping behaviors of young children during a chest tube procedure in the pediatric intensive care unit. Maternal-Child Nursing Journal. 1994;22(4):134–146. [PubMed] [Google Scholar]
- Couture CJ. The psychological response of young children to brief hospitalization and surgery: The role of parent-child contact and age. Dissertation Abstracts International. 1976;37:1427–B. [Google Scholar]
- Elander G, Nilsson A, Lindberg T. Behavior in four-year-olds who have experienced hospitalization and day care. American Journal of Orthopsychiatry. 1986;56:612–616. doi: 10.1111/j.1939-0025.1986.tb03494.x. [DOI] [PubMed] [Google Scholar]
- Freedman D, Thornton A, Camburn D, Alwin D, Young-DeMarco L. The Life History Calendar: A technique for collecting retrospective data. Sociological Methodology. 1988;18:37–68. [PubMed] [Google Scholar]
- Goslin ER. The effect of crisis intervention therapy in reducing anxiety in emergency hospitalization of preschool children. Dissertation Abstracts International. 1979;40:3394–B. [Google Scholar]
- Hoffman LW. Effects of maternal employment on the child. American Psychologist. 1989;44:283–292. [Google Scholar]
- Mahaffy PR., Jr The effects of hospitalization on children admitted for tonsillectomy and adenoidectomy. Nursing Research. 1965;14:12–19. doi: 10.1097/00006199-196501410-00006. [DOI] [PubMed] [Google Scholar]
- Melnyk BM. Coping with unplanned childhood hospitalization: Effects of informational interventions on mothers and children. Nursing Research. 1994;43:50–55. [PubMed] [Google Scholar]
- Menke EM. School-aged children’s perception of stress in the hospital. Journal of the Association for the Care of Children in Hospitals. 1981;9:80–86. doi: 10.1080/02739618109450691. [DOI] [PubMed] [Google Scholar]
- National Center for Health Statistics. Health aspects of childbearing by unmarried women. Vital and Health Statistics. 1995;21(53):19–23. [Google Scholar]
- Pierrehumbert B, Ramstein T, Karmaniola A, Halfon O. Child care in the preschool years: Attachment, behaviour problems and cognitive development. European Journal of Psychology of Education. 1996;11:201–214. [Google Scholar]
- Prugh DG, Staub EM, Sands HH, Kirschbaum RM, Lenihan EA. A study of the emotional reactions of children and families to hospitalization and illness. American Journal of Orthopsychiatry. 1953;23:70–106. doi: 10.1111/j.1939-0025.1953.tb00040.x. [DOI] [PubMed] [Google Scholar]
- Rossen BE, McKeever PD. The behavior of preschoolers during and after brief surgical hospitalizations. Issues in Comprehensive Pediatric Nursing. 1996;19:121–133. doi: 10.3109/01460869609038052. [DOI] [PubMed] [Google Scholar]
- Sides JP. Emotional responses of children to physical illness and hospitalization. Dissertation Abstracts International. 1977;38:917–B. [Google Scholar]
- Simons B, Bradshaw J, Silva PA. Hospital admissions during the first five years of life: A report from the Dunedin Multidisciplinary Child Development Study. New Zealand Medical Journal. 1980;91(654):144–147. [PubMed] [Google Scholar]
- Sipowicz RR, Vernon DTA. Psychological responses of children to hospitalization. American Journal of Diseases in Children. 1965;109:228–231. doi: 10.1001/archpedi.1965.02090020230006. [DOI] [PubMed] [Google Scholar]
- Thompson RH. Psychosocial research on pediatric hospitalization and health care. Springfield, IL: Charles C. Thomas; 1985. [Google Scholar]
- Tiedeman ME, Clatworthy S. Anxiety responses of 5- to 11-year-old children during and after hospitalization. Journal of Pediatric Nursing. 1990;5:334–343. [PubMed] [Google Scholar]
- Tobey GY, Schraeder BD. Impact of caretaker stress on behavioral adjustment of very low birth weight preschool children. Nursing Research. 1990;39:84–89. [PubMed] [Google Scholar]
- U. S. Bureau of the Census. Statistical abstract of the United States: 1992. 112. Washington, DC: U. S. Government Printing Office; 1992. [Google Scholar]
- Wolfer JA, Visintainer MA. Pediatric surgical patients’ and parents’ stress responses and adjustment as a function of psychologic preparation and stress-point nursing care. Nursing Research. 1975;24:244–255. [PubMed] [Google Scholar]
- Wolfer JA, Visintainer MA. Prehospital psychological preparation for tonsillectomy patients: Effects on children’s and parents’ adjustment. Pediatrics. 1979;64:646–655. [PubMed] [Google Scholar]
- Youngblut JM, Singer LT, Rodgers WL. Maternal employment and LBW infant outcomes. 1997 Unpublished raw data. [Google Scholar]