

Abstract
Objective
We sought to identify relationship and partner-related moderating variables that influence the effectiveness of both a couples and a solo learning intervention designed to increase skin self-examination behavior in a sample of patients at risk for developing melanoma.
Methods
Patients received a brief intervention designed to teach skin self-examination skills and were randomly assigned into either a solo learning condition where the intervention was administered to the patient alone (n = 65) or a couple learning condition where the intervention was administered to the patient and patient’s spouse or cohabiting partner (n = 65). The main outcome measure was skin self-examination self-efficacy, which is the strongest mediator of skin self-examination. The relationship moderator variables measured were quality of relationship, partner motivation, and ability to assist in implementation of the intervention.
Results
When quality of the marital/partner relationship was high, the beneficial effects provided by the partner being included in the skin self-examination skills training were the highest and patients exhibited higher self-efficacy. Similar effects were observed for those with partners who were motivated to implement the intervention, and for those with partners high in ability to provide support.
Limitations
Study limitations include the need to evaluate whether the effects can be sustained long term and the exclusion of patients with melanoma without partners.
Conclusions
The amount of beneficial effects gained by the patient from the skin self-examination intervention was influenced by marital/partner relationships. Clinicians may need to consider these relationship and partner characteristics when communicating to patients about skin cancer screening.
With an estimated 60,000 new cases of invasive melanoma and 8100 deaths in 2007, the incidence of melanoma, the deadliest form of skin cancer, has increased more rapidly than any other cancer in the past 10 years.1 Early detection techniques, such as skin self-examination (SSE) and the use of the ABCDE rule of melanoma identification,2 have been identified as effective prevention tools to reduce the mortality of melanoma.3 However, few studies exist that report on the efficacy of efforts designed to increase SSE.4-13 Given the importance of early detection in successful treatment of melanoma, this lack of empirical SSE studies suggests that more work is needed to understand these behaviors.
SSE is unlike other self-screening cancer techniques, such as breast or testicular self-examination, because complete SSE often requires assistance from others (eg, significant others, friends, family members) to examine areas of the skin that are not easily seen. Given this reliance on helpers for effective SSE performance, there is a need to study the role of the helper in the adaptation and maintenance of SSE behaviors. In an attempt to elucidate the role of the partner, Robinson et al14 recently examined the efficacy of a SSE skill training intervention for patients with a personal history of melanoma. Patients were randomized to either a solo learning condition where the intervention was administered to the patient with melanoma alone or a couple learning condition in which patients received the intervention with their partner (ie, spouse or cohabiting partner) present. The intervention was found to be efficacious in increasing patient SSE and these increases were significantly higher in the couple learning condition.
Basing our hypothesis on social cognitive theory of Bandura,15,16 in which self-efficacy is a belief that one is capable of performing in a certain manner required to manage prospective situations, the authors hypothesized that patients in the couple learning condition reported higher SSE at follow-up compared with patients in the solo learning condition because the modeling and supportive behaviors by the partners during and after the skills training session provided patients in the couples condition with greater SSE self-efficacy (ie, the patients in the couple condition were more confident in their ability to perform SSE). Support for this hypothesis was found in our subsequent work17 that revealed SSE self-efficacy beliefs were the strongest mediator of the learning condition (eg, couple vs solo) for the SSE behavior (Fig 1). Thus, the differences in SSE outcomes between patients in the couple and solo learning conditions could be explained by changes in patient self-efficacy with the greatest positive changes occurring in the couple learning group.
Fig 1.
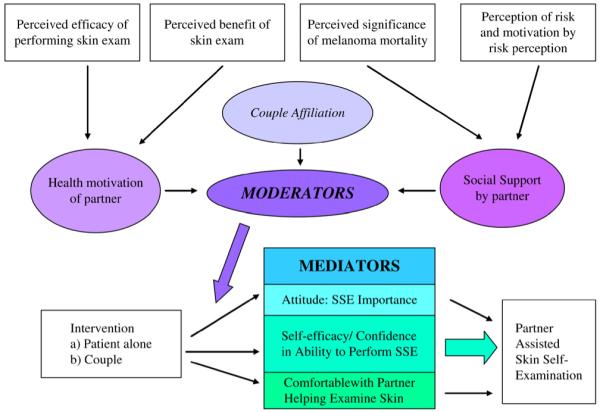
Theoretic model of couple relationship affiliation and partner characteristics as moderators between intervention and mediators of partner-assisted skin self-examination (SSE) performance.
These studies by Robinson et al14,17 suggest that using partners and focusing on increasing SSE self-efficacy can be effective ways for clinicians to increase screening behaviors in patients with melanoma. However, these previous studies do not speak to how patient and partner relationship variables may influence the effectiveness of the SSE intervention. Research in other health domains has shown that relationship and partner variables, such as quality of marital relationship, health motivation of the partner, and social support by the partner, are related to the adoption and maintenance of preventive health behaviors18-21 (Fig 1). The current study examines martial relationship and partner characteristics that might influence how well the SSE skills training increases patients’ SSE self-efficacy. The moderator effect between the intervention condition and the mediator, self-efficacy, is important and interesting, by and large because there have been few interventions that have changed SSE in patients with melanoma. The current program of work is unique in this regard and suggests that patients will conduct more SSEs if they include a partner with the primary reason being that they believe they have greater self-efficacy under those conditions (our primary mediator). Given the importance of self-efficacy in this process, we thought it was critical to understand under what conditions this effect was strengthened or weakened by relationship and partner characteristics.
The first research question is whether quality of marital relationship, couple affiliation, moderates the amount of patient self-efficacy gained after being exposed to the intervention with a partner. A moderating effect occurs when the relationship between two variables (eg, SSE skills training intervention and self-efficacy) strengthens or weakens depending on a third variable (eg, marital relationship).22 We hypothesize that when quality of the marital relationship is high, the beneficial effects provided by including the partner in the SSE skills training will be the highest and patients will exhibit higher self-efficacy. In contrast, when the quality of marital relationship is low, the beneficial effects provided by the partner being included in the SSE skills training will be the lowest and patients will exhibit lower self-efficacy. Although such relationships seem to be consistent with a common sense explanation, it is an empirical question as to whether the quality of the marital relationship does in fact strengthen or weaken the skills training effect on self-efficacy when the partner is included or not included in the training.
The second focus of the research is on whether partner characteristics (eg, motivation to assist their partner and partner’s ability to provide support) moderate the amount of patient self-efficacy gained after being exposed to the intervention with a partner. We hypothesized that for partners who are highly motivated to help implement the intervention, the beneficial effects provided by the partner being included in the SSE skills training will be the highest and patients will exhibit higher self-efficacy. In contrast, when the partners are unmotivated, the beneficial effects provided by the partner being included in the SSE skills training will be the lowest and patients will exhibit lower self-efficacy. Finally, we hypothesize similar patterns to occur regarding partner’s ability to provide social support. When partner’s ability to provide support is high, the beneficial effects provided by the partner being included in the SSE skills training will be the highest and patients will exhibit higher self-efficacy.
METHODS
Sample and procedure
In all, 130 participants were drawn from a hospital registry of patients who were given the diagnosis of cutaneous melanoma and were being seen at least annually by a physician for their skin condition. These patients were randomized into either the couple learning condition (n = 65) or the solo learning condition (n = 65). Patients were excluded from the study if they did not have a cohabiting partner, were overburdened with other comorbid diseases, and/or had insufficient vision to see their own skin. Eligible partners must have had a spousal or cohabiting relationship for at least 1 year with the participant before the intervention. More information about inclusion criteria and the study flow chart are available in previous work.14,17 Table I presents information regarding demographic characteristics of the sample. The study protocol was approved by our institutional review boards.
Table I.
Study participant demographics and tests for baseline differences
| Demographics | Solo | Couple | Test for differences |
|---|---|---|---|
| Patient sex | |||
| Male | 33 | 32 | χ2 (1, N = 130) = 0.07, P > .05 |
| Female | 32 | 33 | |
| Partner sex | |||
| Male | 32 | 32 | χ2 (1, N = 130) = 0.01, P > .05 |
| Female | 33 | 33 | |
| Patient’s age, y | |||
| 18-29 | 11 | 7 | χ2 (5, N = 130) = 6.17, P > .05 |
| 30-39 | 11 | 17 | |
| 40-49 | 9 | 14 | |
| 50-59 | 8 | 8 | |
| 60-69 | 15 | 15 | |
| ≥ 70 | 11 | 4 | |
| Patient’s marital status | |||
| Married | 47 | 45 | χ2 (2, N = 130) = 1.01, P > .05 |
| Never married | 13 | 11 | |
| Divorced/separated | 5 | 9 | |
| Patient’s education level | |||
| ≤ High school education | 18 | 10 | χ2 (3, N = 130) = 6.25, P = .10 |
| Some college education, no degree | 24 | 21 | |
| College graduate | 17 | 30 | |
| Graduate degree | 6 | 4 | |
| Patient’s annual household income, $ | |||
| <20,000 | 8 | 7 | χ2 (3, N = 130) = 2.74, P > .05 |
| 20,000-50,999 | 44 | 38 | |
| 51,000-100,000 | 6 | 12 | |
| >100,000 | 7 | 8 | |
The intervention was administered in an ambulatory care hospital setting by a trained research assistant. The intervention consisted of a card with condensed information about SSE along with color illustrations of the ABCDE rule of melanoma screening. In addition, the research assistant answered questions about card content and gave a SSE skills demonstration. On completion of the intervention, patients were given a SSE enabling kit consisting of the ABCDE card, a lighted hand magnifying glass, a millimeter ruler, and a set of body maps to use as both a guide for SSE and as a place to mark areas of concern found during SSE.
The patient and eligible partner in both the solo and couple learning groups completed a preintervention assessment of relationship and partner variables. Thus, the study procedures were identical between the two groups aside from the partners actually participating in the intervention in the couple learning group. Patients also completed preintervention and postintervention assessments that measured attitudinal, behavioral, and knowledge variables related to SSE and skin cancer. Patients were readministered the assessment at a 4-month follow-up period.
Measures
All measures were drawn from previous SSE literature.23,24 Relationship and partner variables were measured at preintervention baseline and the SSE self-efficacy outcome was measured at the 4-month follow-up.
Quality of the relationship
The Dyadic Adjustment Scale25 was adapted for use to assess quality of the relationship of the couples in the study. The scale consists of 32 items that measure various dimensions of quality of the relationship including satisfaction, cohesion, consensus, and affection expression. Scores are summed on all items to create a single score ranging from 0 to 150. High scores on the Dyadic Adjustment Scale represent high quality of relationship and better marital adjustment.
Partner’s motivation
The Spouse Treatment Mediation Inventory26,27 was adapted for use in the current study and measures various aspects of partner support. The Spouse Treatment Mediation Inventory contains a subscale of 3 items that measure the partners’ motivation to assist in implementation of the intervention (eg, Question: I am highly motivated to make changes through participating in this skin examination program. Response: 1, strongly agree to 5, strongly disagree). The items in the partner motivation scale were averaged to create a single index (coefficient α = .825). Higher scores on this subscale indicate the partner is highly motivated to assist the patient in implementing the SSE intervention.
Partner’s ability
The partner ability subscale of the Spouse Treatment Mediation Inventory assesses the partner’s ability to provide support to the patient. Seven items measured various aspects of partner ability including compliance with medical advice, energy level, ability to handle and cope with stress, recording and observation skills, teachability, and assertiveness.27 The items were averaged to create a single measure (coefficient α = .924) and higher scores on this subscale indicate that the partner is highly capable of helping the patient implement the SSE intervention.
Self-efficacy
The self-efficacy in performing SSE measure consisted of 4 averaged items (α = .917). The items assess the patients’ confidence in their ability to perform SSE (eg, How confident are you that you know how to examine your skin for signs of skin damage or skin cancer?). Responses were in a 5-point Likert-type scale and ranged from 0 (not at all confident) to 4 (extremely confident).
Statistical analysis
Moderator effects were tested using regression analyses based on the work of Jaccard and Turrisi.22 The analyses regressed self-efficacy onto 3 variables: intervention condition, a mean centered moderator variable score, and the product term of the mean centered moderator and the intervention condition. The intervention condition was scored as a 0 for solo learning and 1 for couples learning. Each moderator variable (quality of the relationship, partner motivation, and partner ability) was mean centered before the analyses.22 Finally, product terms were computed by taking the product between the intervention learning condition and the different moderator measures. The regression coefficient for the product term provides an estimate of the moderator effect. If the confidence intervals (CIs) around the regression coefficient contained the value of zero then the effect was considered not significantly different from zero or nonsignificant. Bootstrapped confidence intervals (95%), which make no assumptions regarding the underlying distributions of the variables, were used to test for statistical significance (AMOS 5.0, SPSS Inc, Chicago, Ill). The EM method was used to impute missing data,28 which was less than 2%.
When a significant interaction was observed we examined the effect of learning condition on the self-efficacy at below-average, average, and above-average scores on the moderator variables to evaluate the nature of the interaction.22
RESULTS
Study participants
Patients were compared on background characteristics between intervention groups (Table I). We ran a series of χ2 tests to test for differences in proportions between groups on these variables. Education levels were marginally significantly different between groups (P = .10). To test for confounding effects for education level, all of the interaction effects were tested with education included in the model. Interaction effects were still highly significant, which suggests that education was not a significant confounder. There were not significant baseline differences for SSE self-efficacy between the couple and solo learning conditions.
Research question 1
For the first research question, we hypothesized that when quality of the marital relationship is high, the beneficial effects provided by the partner being included in the SSE skills training will be the highest and patients will exhibit higher self-efficacy. For patients’ perception of the quality of the relationship, the total model tested with all 3 terms (intervention condition, quality of relationship score, and product term of intervention and quality of relationship score) explained a significant proportion of variance in self-efficacy scores (R = .699, R2 = .489, F [3125] = 39.88, P < .001). Both the main effect of intervention condition (b = .96, t [127] = 6.64, P < .001) and patients’ perception of relationship quality (b = .02, t [127] = 7.99, P < .001) significantly predicted SSE self-efficacy. Significant moderator effects were found for the patients’ perception of the quality of the relationship (b for the product term = .013, SE = .005, CI95L = .004, CI95H = .021, P <.01, semipart r2 = .028). For partners’ perception of the quality of the relationship, the total model with all 3 terms explained a significant proportion of variance in self-efficacy scores (R = .706, R2 = .498, F [3125] = 41.36, P < .001). Both the main effect of intervention condition (b = .95, t [127] = 6.60, P < .001) and partners’ perception of relationship quality (b = .02, t [127] = 8.19, P < .001) significantly predicted SSE self-efficacy. Significant moderator effects were found for the partners’ perception of the quality of the relationship (b for the product term = .012, SE = .005, CI95L = .004, CI95H = .021, P < .01, semipart r2 = .028).
Fig 2, A, shows that patients who reported above-average levels of relationship quality had higher mean levels of self-efficacy (2.30 couple and 0.96 solo) when compared with those with average quality (1.52 couple and 0.56 solo). Patients who reported below-average relationship quality had the lowest levels of self-efficacy (0.75 couple and 0.16 solo). Examination of the effect of patients’ reported relationship quality between intervention conditions revealed significant differences at the above-average level (t [127] = 6.72, P < .001), the average level (t [127] = 6.83, P < .001), and the below-average level (t [127] = 2.91, P < .001). This pattern was consistent in the partner’s reported relationship quality (Fig 2, B) with those patients whose partners reporting above-average relationship quality exhibiting the highest levels of self-efficacy (2.30 couple and 0.98 solo) followed by the average relationship quality (1.51 couple and 0.57 solo) and then below average (0.72 couple and 0.15 solo). Examination of the effect of partners’ reported relationship quality between intervention conditions revealed significant differences at the above-average level (t [127] = 6.74, P < .001), the average level (t [127] = 6.88, P < .001), and the below-average level (t [127] = 2.96, P < .01).
Fig 2.
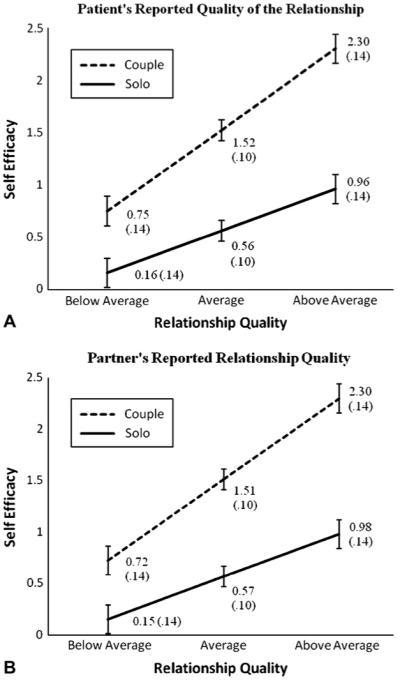
Patients’ (A) and partners’ (B) reported quality of relationship as moderator of patients’ skin self-examination self-efficacy.
Research question 2
For the second research question we hypothesized that for partners who are highly motivated to help implement the intervention, the beneficial effects provided by the partner being included in the SSE skills training would be the highest and patients would exhibit higher self-efficacy. The total model explained a significant proportion of variance in self-efficacy scores (R = .847, R2 = .717, F [3125] = 105.49, P < .001). Both the main effect of intervention condition (b = .62, t [127] = 5.46, P < .001) and partners’ motivation to implement the intervention (b = .61, t [127] = 13.88, P < .001) significantly predicted SSE self-efficacy. Significant moderator effects were observed for the partners’ motivation (b for the product term = .335, SE = .088, CI95L = .194, CI95H = .466, P < .001, semipart r2 = .038). Fig 3 shows that partner’s perception of intervention importance was related to patient self-efficacy. Patients with partners who had above-average motivation had the highest self-efficacy levels (2.01 couple and 1.06). Those patients with partners who had average levels of motivation had less self-efficacy (1.13 couple and 0.61 solo) and those with below-average partners had the lowest self-efficacy (0.25 couple and 0.16 solo). Examination of the effect of partners’ motivation between intervention conditions revealed significant differences at the above-average level (t [127] = 5.86, P < .001), the average level (t [127] = 4.61, P < .001), and a nonsignificant difference at the below-average level (t [127] = .54, P > .05).
Fig 3.
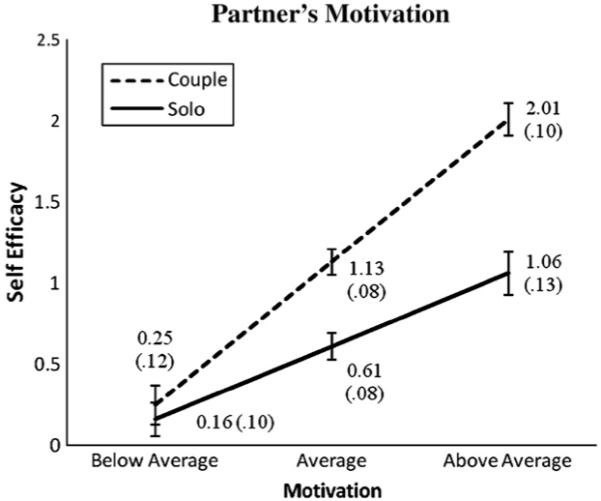
Partners’ reported motivation to assist in implementing intervention as moderator of patients’ self-efficacy.
Finally, the model tested with partners’ ability to assist in the implementation of the intervention as a moderator explained a significant proportion of variance in self-efficacy (R = .523, R2 = .274, F [3125] = 15.72, P < .001). Both the main effect of intervention condition (b = .92, t [127] = 5.36, P < .001) and partners’ ability to assist (b = .29, t [127] = 2.97, P < .01) significantly predicted SSE self-efficacy. Significant moderator effects were observed for the partners’ ability to assist (b for the product term = .462, SE = .177, CI95L = .189, CI95H = .754, P < .01, semipart r2 = .033). Partner’s ability was associated with patient self-efficacy in the couple learning group only (Fig 4). In the couple group, patients whose partners had above-average ability to help had the highest self-efficacy (1.73) followed by those with average helping partners (1.29) and those with below-average partners (0.85). In the solo learning group, partner’s ability did not seem to have an influence on patient self-efficacy. Examination of the effect of partners’ ability between intervention conditions revealed significant differences at the above-average level (t [127] = 5.28, P < .001), the average level (t [127] = 4.86, P < .001), and a nonsignificant difference at the below-average level (t [127] = 1.59, P > .05).
Fig 4.
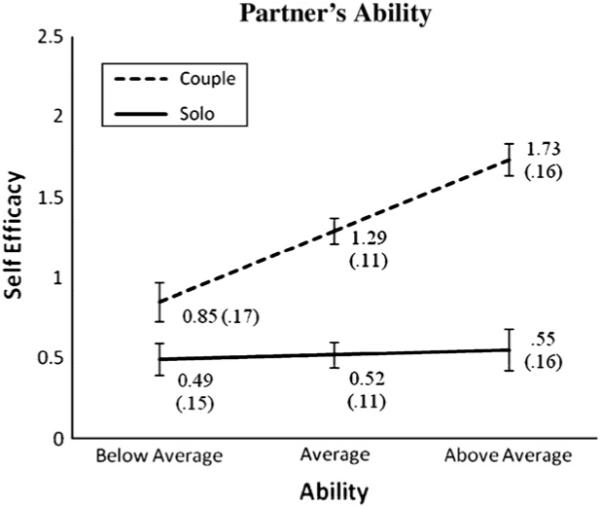
Partners’ reported ability to assist in implementing intervention as moderator of patients’ self-efficacy.
DISCUSSION
Evidence suggests early detection of melanoma through SSE can be effective at reducing skin cancer burden. Recent work14,17 has shown that partner involvement in a SSE skills training intervention can be an important influence in SSE self-efficacy and the adoption of SSE behaviors in patients with melanoma. The current study describes relationship and partner-related dynamics that influenced the amount of patients’ SSE self-efficacy gained from the intervention.
The intervention effects on self-efficacy were the highest when the quality of the relationship was high, the patient’s partner was highly motivated, and the partner had high ability to provide social support. These relationships held for both the couple and the solo learning conditions. This suggests that relationship and partner support variables are important even in situations where the partner is not directly involved in the skills training intervention. However, mean SSE self-efficacy scores were consistently approximately 2 to 3 times higher in patients in the couple learning group. Those in the couple conditioning are benefiting more from the SSE promoting supportive/modeling behaviors provided by the partner. Thus, when quality of relationship is high and partner support is high, gains in SSE self-efficacy increase but the benefit to patients is greater when the partner is actively involved (eg, the couple learning condition).
The observed effects were all greater in the couple learning condition when compared with the solo learning condition. This suggests the relationship and partner support variables are more important in the couple condition because small changes in these variables produce more change in self-efficacy when compared with the solo learning group. Interestingly, those who score average on the relationship and partner variables in the couple condition are reporting higher SSE self-efficacy than those who score the highest on the relationship and partner variables in the solo learning condition. With some variables, such as relationship quality and partner ability, those in the couple learning condition reporting below-average levels are reporting more favorable SSE self-efficacy when compared with those in the solo group who were above average on these variables. The finding that the partner assistance intervention is more effective at increasing SSE self-efficacy than the solo condition even when quality of relationship is low suggests that partner involvement can help compensate for low levels on these variables.
The finding that patients with low quality of relationship or low partner support are reporting low SSE self-efficacy regardless of learning condition lends further credence to the importance of relationship and partner support variables. Because it seems to be detrimental to SSE self-efficacy when these variables are low, it may be important to identify patients who have low quality of relationship or partners who have low ability to provide social support. To increase performance of SSE and partner-assisted SSE, clinicians may offer encouragement to partners with low social support abilities and describe ways that the partner may help reduce patient anxiety over finding a changing mole. When spousal partner social support is low, it might also be beneficial to recruit a different helper, such as a family member or friend, who may be able to provide social support to the patient. If partner support is low and no other helper is available, the dermatologist may need to increase the frequency of physician visits to allay anxiety for the patient at risk. In addition, in these situations, a different intervention approach may be needed that would include information highlighting the importance of these relationship and partner characteristics.
Although the limitations of the current study have been discussed in earlier publications14,15 we are compelled to restate the importance of examining the long-term effects. Future research should evaluate whether the observed short-term changes in SSE self-efficacy can be sustained during a longer time period. Our analysis of relationship and partner variables was limited to quality of marital relationship, health motivation of the partner, and social support by the partner, which was found to be important to the adoption and maintenance of preventive health behaviors in other health domains. Future research should explore other relationship variables such as health dominance between partners. It is also possible that the some of the observed relationships could be explained by a third confounding variable. One possible confounder would be illness status. For example, differences in severity of cancer diagnosis could jointly influence both relationship variables and self-efficacy for screening for future cancers in various ways. In addition, it is important to note patients without partners were excluded from the current study and represent an important portion of the populations at risk to develop another melanoma. The current partner assistance intervention has not been designed to be used by these individuals and future research is needed to determine the best method of promoting screening in this population.
In sum, the current research reinforces findings from health sciences regarding the important role of relationship dynamics on preventive health behaviors and expands the findings to the adoption and maintenance of SSE behavior. The current study also adds to the literature by identifying partner characteristics that are important in SSE skills training. Robinson et al14,17 revealed involving a partner in a SSE skills training program led to more SSE behaviors by increasing SSE self-efficacy. When teaching SSE skills, it is important to realize that the quality of the relationship and partner motivation to help and their ability to provide social support may be influential in whether the behavior is adopted and maintained by the patient.
Acknowledgments
Supported by 5R21 CA-103833-02 (Dr Robinson) from the National Cancer Institute.
Footnotes
Conflicts of interest: None declared.
Reprints not available from the authors.
REFERENCES
- 1.American Cancer Society World Wide Web site [Accessed April 1, 2007];Skin cancer facts. Available from: URL: http://www.cancer.org/docroot/PED/content/ped_7_1_What_You_Need_To_Know_About_Skin_Cancer.asp?sitearea=&level=
- 2.Rigel DS, Friedman RJ, Kopf AW, Polsky D. ABCDE–an evolving concept in the early detection of melanoma. Arch Dermatol. 2005;141:1032–4. doi: 10.1001/archderm.141.8.1032. [DOI] [PubMed] [Google Scholar]
- 3.Berwick M, Begg CM, Fine JA, Roush CG, Barnhill RL. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88:17–23. doi: 10.1093/jnci/88.1.17. [DOI] [PubMed] [Google Scholar]
- 4.Berwick M, Oliveria SA, Luo S, Headley A, Rolognia JL. A pilot study using nurse education as an intervention to increase skin self-examination for melanoma. J Cancer Educ. 2000;15:38–40. doi: 10.1080/08858190009528651. [DOI] [PubMed] [Google Scholar]
- 5.Borland R, Mee V, Meehan JW. Effects of photographs and written descriptors on melanoma detection. Health Educ Res. 1995;12:375–84. doi: 10.1093/her/12.3.375. [DOI] [PubMed] [Google Scholar]
- 6.Friedman LC, Webb JA, Bruce S, Weinberg AD, Cooper HP. Skin cancer prevention and early detection intentions and behavior. Am J Prev Med. 1995;11:59–65. [PubMed] [Google Scholar]
- 7.Hanrahan PF, Hersey P, Watson AB, Callaghan TM. The effect of an educational brochure on knowledge and early detection of melanoma. Aust J Public Health. 1995;19:270–4. doi: 10.1111/j.1753-6405.1995.tb00442.x. [DOI] [PubMed] [Google Scholar]
- 8.Hanrahan PF, Hersey P, Menzies SW, Watson AB, D’Este CA. Examination of the ability of people to identify early changes of melanoma in computer-altered pigmented skin lesions. Arch Dermatol. 1997;133:301–11. [PubMed] [Google Scholar]
- 9.Lowe JB, Balanda KP, Del Mar MB, Hegarty K, Sheldrake M, Clare G. An innovative method of increasing early detection for skin cancer in Australia. Am J Health Behav. 1999;23:243–9. [Google Scholar]
- 10.Mickler TJ, Rodriguez JR, Lescano CM. A comparison of three methods of teaching skin self-examinations. J Clin Psych Med Settings. 1999;6:273–86. [Google Scholar]
- 11.Oliveria SA, Dusza SW, Phelan DL, Ostroff JS, Berwick M, Halpern AC. Patient adherence to skin self-examination: effect of nurse intervention with photographs. Am J Prev Med. 2004;26:152–5. doi: 10.1016/j.amepre.2003.10.006. [DOI] [PubMed] [Google Scholar]
- 12.Phelan DL, Oliveria SA, Christos PJ, Dusza SW, Halpern AC. Skin self-examination in patients at high risk for melanoma: a pilot study. Oncol Nurs Forum. 2003;30:1029–36. doi: 10.1188/03.ONF.1029-1036. [DOI] [PubMed] [Google Scholar]
- 13.Phelan DL, Oliveria SA, Halpern AC. Patient experiences with photo books in monthly skin self-examinations. Dermatol Nurs. 2005;17:109–14. [PubMed] [Google Scholar]
- 14.Robinson JK, Turrisi R, Stapleton J. Efficacy of a partner assistance intervention designed to increase skin self-examination performance. Arch Dermatol. 2007;143:37–41. doi: 10.1001/archderm.143.1.37. [DOI] [PubMed] [Google Scholar]
- 15.Bandura A. Self-efficacy: the exercise of control. WH Freeman and Co; New York: 1997. [Google Scholar]
- 16.Bandura A. Social cognitive theory: an agnatic perspective. Ann Rev Psychol. 2001;52:1–26. doi: 10.1146/annurev.psych.52.1.1. [DOI] [PubMed] [Google Scholar]
- 17.Robinson JK, Turrisi R, Stapleton J. Examination of mediating variables in a partner assistance intervention designed to increase performance of skin self-examination. J Am Acad Dermatol. 2007;56:391–7. doi: 10.1016/j.jaad.2006.10.028. [DOI] [PubMed] [Google Scholar]
- 18.Bovberg VE, McCann BS, Brief DJ, et al. Spouse support and long term adherence to lipid-lowering diets. Am J Epidemiol. 1995;141:451–60. doi: 10.1093/oxfordjournals.aje.a117447. [DOI] [PubMed] [Google Scholar]
- 19.Garay-Sevilla ME, Nava LE, Malacara JM, Huerta R, de Leon JD, Mena A, et al. Adherence to treatment and social support in patients with non-insulin dependent diabetes mellitus. J Diabetes Complications. 1995;9:81–6. doi: 10.1016/1056-8727(94)00021-f. [DOI] [PubMed] [Google Scholar]
- 20.Trief PM, Ploutz-Snyder R, Britton KD, Weinstock RS. The relationship between marital quality and adherence to the diabetes care regimen. Ann Behav Med. 2004;27:148–54. doi: 10.1207/s15324796abm2703_2. [DOI] [PubMed] [Google Scholar]
- 21.Yates BC. The relationship among social support and short- and long-term recovery outcomes in men with coronary heart disease. Res Nurs Health. 1995;18:193–203. doi: 10.1002/nur.4770180303. [DOI] [PubMed] [Google Scholar]
- 22.Jaccard J, Turrisi R. Interaction effects in multiple regression. 2nd ed. Sage Publications; Newbury Park (CA): 2003. [Google Scholar]
- 23.Robinson JK, Rigel DS, Amonette RA. What promotes skin self-examination? J Am Acad Dermatol. 1998;38:752–7. doi: 10.1016/s0190-9622(98)70204-x. [DOI] [PubMed] [Google Scholar]
- 24.Robinson JK, Fisher SG, Turrisi RJ. Predictors of skin self-examination performance. Cancer. 2002;95:135–46. doi: 10.1002/cncr.10637. [DOI] [PubMed] [Google Scholar]
- 25.Spanier GB. Measuring dyadic adjustment: new scales for assessing the quality of marriage and similar dyads. J Marriage Fam. 1976;38:15–27. [Google Scholar]
- 26.Ager RD, Thomas EJ. The spouse treatment mediation inventory (STMI) In: Fischer J, Corcoran K, editors. Measures for clinical practice. 2nd ed. The Free Press; New York: 1994. [Google Scholar]
- 27.Thomas EJ, Ager RD. Treatment mediation and the spouse as treatment mediator. Am J Fam Ther. 1991;19:315–26. [Google Scholar]
- 28.Little R, Rubin D. Statistical analysis with missing data. Wiley; New York: 1987. [Google Scholar]