

Abstract
Aims
To evaluate the effectiveness of acupuncture in treating symptoms associated with myofascial pain of the jaw muscles.
Methods
Twenty-eight subjects over the age of 18 and diagnosed with chronic myofascial pain of the jaw muscles were randomized to receive real (n = 16) or sham (n = 12) acupuncture. Prior to treatment, each subject clenched his or her teeth for 2 minutes. Acupuncture or sham acupuncture was then administered at the Hegu large intestine 4 (LI4) acupoint for 15 minutes. Real acupuncture was given by penetrating the needle through a sticky foam pad at the acupoint. Sham acupuncture was conducted by pricking the skin, without penetration, with a shortened, blunted acupuncture needle through a foam pad placed away from the acupoint. General head and neck pain ratings were obtained before and after treatment on a numerical rating scale. A mechanical pain stimulus on the masseter muscle was given before and after treatment and rated on a visual analog scale to measure pain tolerance level. Paired t tests were performed to detect significant changes in pain levels.
Results
Subjects receiving real acupuncture experienced a significant reduction in jaw pain (P = .04), jaw/face tightness (P = .04), and neck pain (P = .04), and a significant increase in pain tolerance of the masseter muscle (P = .001). Subjects were not able to determine whether they received real or sham acupuncture (P = .69). No significant pain reductions were observed in the sham acupuncture group.
Conclusion
A single acupuncture session using one acupoint at Hegu large intestine 4 significantly reduced most myofascial pain endpoints when compared to sham acupuncture.
Keywords: acupuncture, analgesia, Hegu large intestine 4, myofascial pain, placebo, sham
Myofascial pain is characterized by localized, hypersensitive spots in palpable taut bands of muscle fibers (myofascial trigger points). These trigger points may be due to muscle overload from trauma or repetitive activities that cause abnormal stress on specific muscle groups. Clinically, patients complain of tenderness, headaches, restricted movement, and muscle stiffness and weakness.1,2
Acupuncture is an increasingly utilized treatment option for myofascial pain in the United States. According to the 2007 National Health Interview Survey (NHIS), which included a comprehensive survey of complementary and alternative medicine use by Americans, an estimated 3.1 million adults and 150,000 children had used acupuncture in the previous year. Between the 2002 and 2007 NHIS, acupuncture use among adults increased by 0.3% (approximately 1 million people). In 1996, the United States Federal Drug Agency also promoted acupuncture needles from the investigational and experimental medical device category to the regular medical-device category, and the following year the National Institutes of Health (NIH) consensus statement on acupuncture supported the treatment efficacy of acupuncture for conditions such as pain and nausea.3 Despite this increased recognition of acupuncture as a treatment for pain, much evidence for its effectiveness comes from poorly designed studies with inadequate controls and blinding procedures.
A variety of mechanisms have been proposed to explain the analgesic effects of acupuncture. These mechanisms are based on concepts that range from traditional views that center on imbalances of energy flow (chi) through the body, to modern Western views that stress the role of activated neural14–17 and endogenous opioid systems.18 The involvement of classic analgesic systems has been supported by neuroimaging and other studies performed on human and animal subjects.19–22 It is also likely, however, that acupuncture involves a strong placebo component.23,24 For example, while manual needle manipulation and electroacupuncture at the Hegu large intestine 4 (LI4) acupoint produced prominent decreases of blood oxygen level dependent signals (BOLD) in the posterior cingulate, superior temporal gyrus, and putamen/insula, so did sham acupuncture.25 As more is learnt about the physiological basis of placebo analgesia,26 it becomes increasingly important that its effects be separated from true, treatment-specific effects.
The purpose of this study was to evaluate the effectiveness of acupuncture in treating symptoms associated with myofascial pain of the jaw muscles. In contrast to many earlier studies, this investigation utilized a strong sham acupuncture procedure that allowed general placebo effects to be separated from acupuncture-specific effects. The authors’ previous study was underpowered,27 so the power for this study was enhanced by increasing the sample size. It was hypothesized that acupuncture-specific effects would produce a significant amount of analgesia, even when controlling for expectancy with a sham procedure.
Materials and Methods
Participants
Thirty-one patients seeking treatment at the University of California San Francisco (UCSF) Orofacial Pain Center were recruited to participate in this study. Twenty-eight of the subjects, diagnosed with bilateral chronic myofascial pain of the jaw muscles and who met the inclusion criteria, consented and were consecutively invited to participate in the study. The inclusion criteria were: (1) at least 18 years of age, (2) confirmed diagnosis of chronic myofascial pain of the jaw muscles,28 (3) pain at least 4 times a week in the jaw muscles for at least 12 weeks, (4) average pain severity of at least 4 on a 10-point scale for at least 1 hour per day, (5) acupuncture naïve, and (6) pain in the jaw, temples, face, pre-auricular area, or in the ear during rest or function. The exclusion criteria were: (1) pregnancy, (2) current opioid use, and (3) diagnosis of metabolic disease, coagulopathy, neurological disorder, vascular disease, or neoplasia. Participants taking non-steroidal anti-inflammatory drugs and acetaminophen were asked to stop those medications at least 1 day prior to their study appointment.
Materials
Acupuncture needles (Seirin 30-gauge) were used for all subjects. To apply sham acupuncture, the needles were shortened by 10 mm and blunted to avoid actual piercing of the skin. To ensure blinding of both subject and experimenter, needles were inserted through a 10 × 10 × 10-mm poly foam pad (Ace weather strip). The acupuncturist was aware of the study condition, but was instructed not to speak to the patient or experimenter during the session.
Procedures
All study procedures were carried out at the UCSF China Basin Landing Radiology Department. Approval for clinical research was obtained by the UCSF Committee on Human Research (CHR#H 9237-23642-01A). All subjects were asked to discontinue any analgesic medication 24 hours prior to the study. After subject consent was obtained, baseline psychophysical measures were recorded. Participants rated the severity of their jaw and facial pain, jaw and face tightness, headache, neck pain, and tooth pain on an 11-point numerical rating scale (NRS). Using an analog algometer (FPK, Wagner Instruments), the blinded experimenter applied pressure to the right masseter muscle at the angle of the right mandible at a rate of 2 lbs/minute. A sticker dot was placed onto each subject’s right masseter to mark the placement of the algometer. The stimulus pressure was increased at a rate of 1lb/second until the subject raised his or her hand at their maximum tolerance of pain. The pressure algometer reading was recorded and the subject was asked to rate his or her pain to the mechanical stimulus on a visual analog scale (VAS).
A single acupoint was used for all participants. The Hegu LI4 acupoint is located at the highest point of the adductor pollicis muscle between the thumb and index finger. The radial nerve innervates this site. This acupoint is commonly used for head and neck pain,29 A single needle acupuncture treatment modality was used for this study because past studies have shown it to be sufficient for clinically significant results, to minimized potential confounders, and for easy access.30–32 All acupuncture placements were performed by a state-certified dental acupuncturist.
Prior to the acupuncture treatment, the skin at the Hegu LI4 acupoint on the left hand was wiped with alcohol pads, air dried, and then covered with the foam pad. The participants was positioned supinely in a 3.0 Tesla GE Signa magnetic resonance imaging (MRI) scanner system [MRI data not analyzed in this report] (GE Medical Systems), and instructed to close their eyes and relax throughout the session. After a baseline period of 2.5 minutes, the acupuncturist tapped the foot of the participant. This signal indicated that the participant should start clenching their posterior teeth at maximal force for 2 minutes. Participants were instructed to clench at maximal force, as a pain inducer. This 2-minute stimulus period was followed by 30 seconds of rest. Then, the acupuncturist performed the acupuncture or sham protocol by inserting a needle through the foam pad. Subjects were not asked by the acupuncturist about whether they felt the sensation of de-qi because all subjects were acupuncture naïve and would not understand the de-qi sensation.
A list of 50 random numbers was generated by computer and subjects were assigned a number subsequently by enrollment. Subjects with an odd number received sham acupuncture, while those with an even number received real acupuncture. Sixteen subjects received real acupuncture and 12 received sham acupuncture. Real acupuncture consisted of a needle insertion through the sterile foam pad into the left hand Hegu LI4 acupoint to a depth of 10 to 20 mm. The depth of the needle into tissue was estimated by subtracting the 10-mm thickness of the foam pad from the 30-mm length of the needle. Sham acupuncture consisted of a blunted needle insertion through the sterile foam pad, positioned 1 cm distal to Hegu LI4 acupoint, until the needle touched and did not penetrate the skin (Fig 1). After sham acupuncture, the foam pad was removed by the acupuncturist, who visually inspected the skin surface to ensure no skin penetration occurred. This procedure has been found to be an effective sham control for acupuncture.33,34
Fig 1.
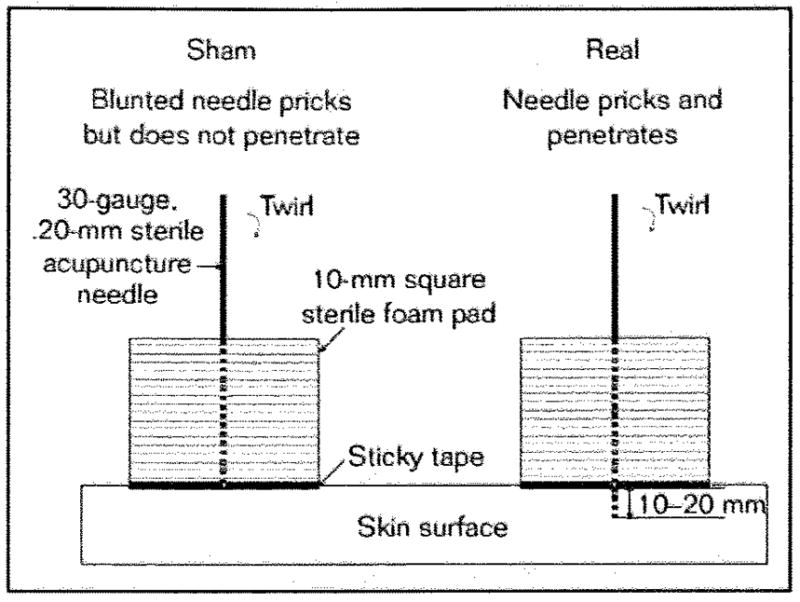
Acupuncture method.
The acupuncture needle was left in place for a total of 15 minutes. After the initial 5 minutes of acupuncture, restimulation was performed by quick quarter turns of the needle for 15 seconds. The needle stayed in place for the remaining 10 minutes. After a total time course of 20 minutes (Fig 2), the subject was removed from the MRI Scanner, and the acupuncturist removed the needle and foam pad. The hands of individuals that received sham acupuncture were double checked to ensure no skin penetration had occurred.
Fig 2.
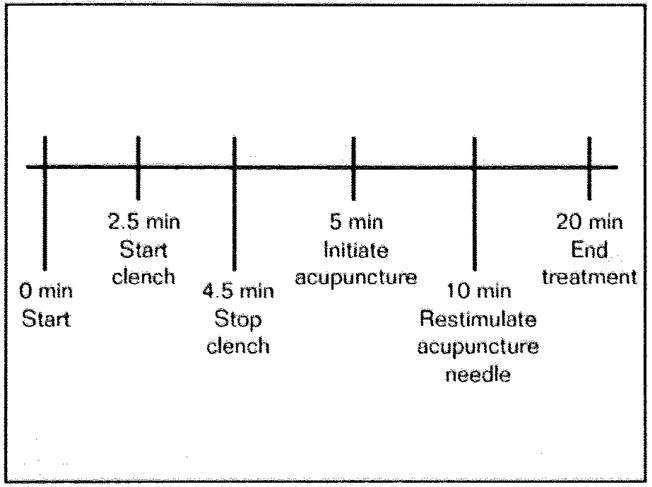
Time course of treatment.
After the acupuncture procedure, participants were reevaluated for general jaw and face pain, jaw and face tightness, headache, and neck pain on the NRS. Mechanical stimulation with the algometer was repeated by the blinded experimenter, using the same location and maximum tolerance levels determined at the beginning of the experiment. Participants were informed that the intensity of the two mechanical stimulations were the same and they were asked to provide a new VAS rating of their pain. Finally, participants were asked whether they believed that they had received real or sham acupuncture. Upon completion of the entire study, subjects were compensated for their time.
Power Analysis
Power analyses were conducted separately for the real and sham acupuncture groups. Given paired t tests and the large variance in response (taken from the observed data), and α = 0.05, there was 0.86 power to detect a minor (30%) response in the real acupuncture group, and 0.73 power in the sham acupuncture group. For a major (50%) response, there was 0.99 power to detect effects in both real and sham groups.
Statistical Analysis Approach
To determine whether age and baseline pain measurements were significant variables between real and sham acupuncture groups, t tests were performed. The effectiveness of the sham control was determined using a 2 × 2 χ2 test between group assignment (acupuncture and sham) and the participants’ guess (guess acupuncture and guess sham). A non-significant result from the χ2 test would indicate a successful sham procedure. To determine the main effect of acupuncture on myofascial pain, paired t tests were performed on the pre- and postacupuncture psychophysical measures on the NRS and VAS. As an alternative to underpowered interaction analyses, these tests were performed separately on the real and sham acupuncture groups.
Results
A total of 31 female subjects were asked to participate in the study, but only 28 of them consented, which resulted in an unequal number of participants in each group. Three subjects withdrew prior to the start of the study because of needle phobia, claustrophobia, and lack of posterior teeth for clenching. The average age of the real acupuncture group was 36.94 years old (SD = 13.82). The average age of the sham acupuncture group was 44.83 years old (SD = 11.61). The age difference between both treatment groups was not significant (P = .12).
Before main analyses were carried out, the effectiveness of the sham procedure in blinding participants was tested. The results of the χ2 test (χ2 = 0.159, P = .69) indicated that participants were unable to accurately guess their experimental condition assignment (Table 1).
Table 1.
Actual Treatment Versus Perceived Treatment
| True treatment | Perceived treatment |
||
|---|---|---|---|
| Real | Sham | Total | |
| Real | 13 | 3 | 16 |
| Sham | 9 | 3 | 12 |
| Total | 22 | 6 | 28 |
Summary of the number of subjects who correctly guessed their true treatment.
χ2 = .159, P= .69
For data analysis, subjects were grouped by the treatment administered. Baseline pain endpoint measurements were similar in both treatment groups (Table 2). Paired t tests were first conducted on the acupuncture group (Table 3). Individuals receiving real acupuncture experienced significant reduction in jaw pain (t (15) = 2.06, P = .04), jaw tightness (t(15) = 2.25, P = .04), neck pain (t(15) = 2.28, P = .04), and masseter muscle pain tolerance (t(15) = 3.09, P = .01) (Fig 3). The reduced pain level for headache in the acupuncture group was only suggestive of statistical significance (t(15) = 1.88, P = .08); there were two outliers in the data and if these outliers were removed from the data, the average change in headache would not reach statistical significance (P = .41). In the sham group, there were no significant changes found in any of the endpoint variables (all P values > .1).
Table 2.
Paired t tests on Average Baseline Clinical Endpoints in Mean (SD) values for Acupuncture (n = 16) and Sham (n = 12) Groups
| Acupuncture | Sham acupuncture | P value | |
|---|---|---|---|
| Jaw/face pain (NRS) | 5.1 (2.0) | 5.2 (3.0) | .843 |
| Jaw/face tightness (NRS) | 5.7 (1.9) | 5.3 (2.9) | .637 |
| Headache (NRS) | 4.9 (2.9) | 3.8 (3.3) | .092 |
| Neck pain (NRS) | 5.3 (2.7) | 5.3 (2.8) | .419 |
| Masseter muscle pain tolerance (VAS) | 7.4 (1.3) | 7.3 (0.8) | .360 |
Baseline clinical endpoints of both treatment groups on an 11-point NRS (0–10) or on a VAS.
Table 3.
Paired t tests on Average Primary Clinical Endpoints in Mean (SD) Values for Acupuncture (n = 16) and Sham (n = 12) Groups
| Acupuncture |
Sham acupuncture |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Change | t | P | Pre | Post | Change | t | P | |
| Jaw/face pain (NRS) | 5.1 (2.0) | 4.0 (2.6) | −1.1 (2.3) | 2.06 | .04 | 5.2 (3.0) | 4.3 (2.6) | −0.9 (2.8) | 1.48 | .17 |
| Jaw/face tightness (NRS) | 5.7 (1.9) | 4.3 (2.8) | − 1.4 (2.4) | 2.25 | .04 | 5.3 (2.9) | 4.8 (3.3) | −0.5(3.1) | 0.90 | .39 |
| Headache (NRS) | 4.9 (2.9) | 3.3 (2.9) | − 1.6 (2.9) | 1.88 | .08 | 3.8 (3.3) | 3.2 (3.3) | −0.6 (3.3) | 0.63 | .55 |
| Neck pain (NRS) | 5.3 (2.7) | 3.6 (3.0) | − 1.7 (2.9) | 2.28 | .04 | 5.3 (2.8) | 4.3 (3.3) | −1.0 (3.0) | 1.32 | .21 |
| Masseter muscle pain tolerance (VAS) | 7.4 (1.3) | 5.8 (2.1) | − 1.6 (1.8) | 3.09 | .001 | 7.3 (0.8) | 6.5 (2.8) | −0.8(1.6) | 0.83 | .43 |
Clinical endpoints of both treatment groups on an 11–point NRS (0–10) or on a VAS.
Fig 3.
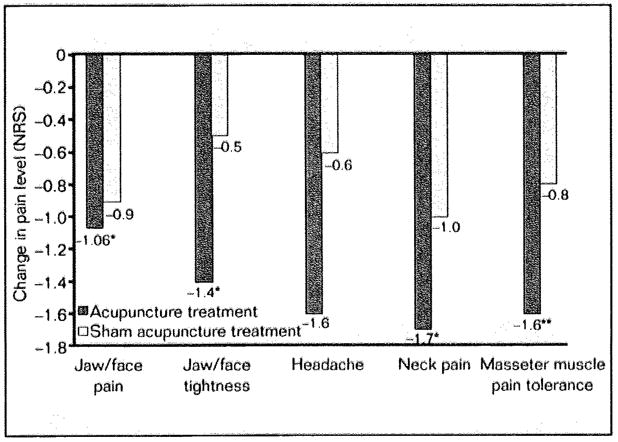
Average change after real acupuncture and sham acupuncture treatment. Change in pain levels after treatment in both groups. Significant changes indicated with: *P = .04; **P = .01. Headache was not significantly changed (P = .80).
As a post-hoc analysis, the number of clinically significant responders in both the real and sham groups was determined. Minimal clinical response was set at 30% symptom reduction, and major clinical response was set at 50% symptom reduction.35 In the sham group, one out of the 12 participants was a minimal responder, and three were major responders. In the real acupuncture group, four individuals were minimal responders, and eight were major responders. Any participant in the real acupuncture group was significantly more likely to be a positive responder than any participant of the sham group (75% versus 33%, χ2 = 4.86, P = .02).
Discussion
Increasing evidence supports the use of acupuncture in treating chronic conditions such as myofascial pain disorder. A retrospective review of 116 patients treated for musculoskeletal pain with acupuncture found that 69% of them benefited with a 30% or greater reduction in pain after an average of three treatment sessions with three acupoints.36 There were limitations, however, due to the relatively small numbers in each diagnosis group of myofascial pain (head, neck, leg, and back), the variability in acupoints used, and the lack of a control group. Smith et al took a more specific approach and tested 27 temporomandibular disorder myofascial pain subjects with six treatment sessions at two acupoints with real acupuncture or sham acupuncture with the Park Sham Device37 and found a significant improvement in signs and symptoms of myofascial pain with real acupuncture but not with sham acupuncture.38 A significant drawback of this study was the low baseline pain level of the sham acupuncture group (average VAS score of 1.3 cm), which limited the range for change in posttreatment pain levels.
The present study addressed these limitations with a focus on individuals with moderate pain levels of chronic myofascial pain of the jaw muscles. Participants were more likely to experience clinically significant reductions of jaw/face pain, jaw/face tightness, and neck pain with one treatment session at one acupoint of real versus sham acupuncture (75% versus 33% positive response rate of at least 30% pain reduction). Participants were also likely to have an increase in pressure-pain tolerance of the masseter muscle with real acupuncture than sham acupuncture. This suggests that acupuncture can increase the functional tolerance of the masseter muscle in myofascial pain patients, who have significantly lower pressure-pain tolerance than healthy individuals.39 The only clinical endpoint acupuncture did not significantly reduce was headache, which concurred with a placebo-controlled study of treating tension-type headache patients with multiple acupoint sites in 10 acupuncture sessions.40 Overall, these findings suggest that acupuncture has short-term beneficial clinical effects above general placebo analgesia induced from sham acupuncture for alleviating most myofascial pain symptoms.
The present study also has shown the successful use of a sham acupuncture procedure as a control method to compare real acupuncture and general placebo effects. While the sham procedure was associated with non-significant symptom relief, it may nonetheless constitute part of the clinical effect of acupuncture. When measuring jaw pain, for example, relief of symptoms in the sham group approached that of the real acupuncture group. It is still possible, therefore, that acupuncture involves nonspecific, placebo-related factors for its analgesic efficacy.41 These findings highlight the need for effective sham procedures in studies of acupuncture.
This study has limitations. First, all participants underwent a 2-minute clench period that was intended to acutely increase their jaw pain and other symptoms. Because of that activity, it is likely that the postacupuncture pain levels were higher than they would have been without clenching. Therefore, the percent relief of symptoms may not accurately reflect the true analgesic effect of acupuncture or the effect of placebo. Second, acupuncture treatment can involve the use of multiple acupoints over several treatment sessions; however, because of the strictly controlled experimental environment, only one acupoint in one treatment session was performed in the present study, which limited the maximum therapeutic effect of acupuncture. Third, the sample size was relatively small, with unequal participants in each treatment group due to withdrawals from the study. The reduced sample size limits generalizability of the results. With a reduced sample size, the 8-year age difference between the mean ages of both treatment groups was not statistically significant, but could have been a significant confounder. Fourth, there was no assessment of longer-term relief of myofascial pain disorder symptoms. The small sample size and lack of long-term outcome assessment of acupuncture remain common limitations amongst randomized controlled clinical trials.42 Thus large scale, randomized controlled trials in acupuncture are needed.
Acknowledgments
The authors acknowledge the UCSF Osher Center for Alternative and Integrative Medicine for funding this study and also like to thank Charles McNeill, DDS, and Patricia Rudd, PT, DPT, for the recruitment of subjects.
Contributor Information
Yoshi F. Shen, Department of Oral and Maxillofacial Surgery, Center for Orofacial Pain, University of California, San Francisco.
Jarred Younger, Anesthesia and Pain Management, Stanford University School of Medicine.
Greg Goddard, Department of Oral and Maxillofacial Surgery, Center for Orofacial Pain, University of California, San Francisco.
Sean Mackey, Department of Anesthesia, Stanford University School of Medicine.
References
- 1.Simons DG, Travell JG, Simons PT. Upper Half of Body. 2. Vol. 1. Baltimore: Williams and Wilkins; 1999. Travell and Simons’ Myofascial Pain and Dysfunction. The Trigger Point Manual. [Google Scholar]
- 2.Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 1. Baltimore: Williams and Wilkins; 1983. [Google Scholar]
- 3.National Institutes of Health Consensus Panel. Acupuncture: National Institutes of Health Consensus Development Conference Statement. [Accessed June 22, 2007]; http://consensus.nih.gov/t99y/1997acupuncture107html.htm.
- 4.Lytle CD. History of the Food and Drug Administration’s regulation of acupuncture devices. J Altern Complement Med. 1996;2:253–256. doi: 10.1089/acm.1996.2.253. [DOI] [PubMed] [Google Scholar]
- 5.NIH Consensus Statement. Acupuncture. JAMA. 1998;280:1518–1524. [Google Scholar]
- 6.Audette J, Blinder RA. Acupuncture in the management of myofascial pain and headache. Curr Pain Headache Rep. 2003;7:395–401. doi: 10.1007/s11916-003-0040-2. [DOI] [PubMed] [Google Scholar]
- 7.Harris RE, Clauw DJ. The use of complementary medical therapies in the management of myofascial pain disorders. Curr Pain Headache Rep. 2002;6:370–374. doi: 10.1007/s11916-002-0078-6. [DOI] [PubMed] [Google Scholar]
- 8.Edelist G, Gross AE, Langer F. Treatment of low back pain with acupuncture. Can J Anaesth Soc. 1976;23:303–306. doi: 10.1007/BF03005706. [DOI] [PubMed] [Google Scholar]
- 9.Brandwein A, Corcos J. Extraction of incisors under acupuncture anesthesia: A standardized method. Am J Acup. 1975;3:352–354. [Google Scholar]
- 10.Goddard G, Karibe H, McNeil C, Villafuerte E. Acupuncture and sham acupuncture reduce muscle pain in myofascial pain patients. J Orofac Pain. 2002;16:71–76. [PubMed] [Google Scholar]
- 11.Kerr NW. Acupuncture for therapy and analgesia. A possible application in dental surgery. Br Dent J. 1973;134:201–204. doi: 10.1038/sj.bdj.4802979. [DOI] [PubMed] [Google Scholar]
- 12.Lao L, Bergman S, Hamilton GR, Langenberg P, Herman B. Evaluation of acupuncture for pain control after oral surgery: A placebo-controlled trial. Arch Otolaryngol Head Neck Surg. 1999;125:567–572. doi: 10.1001/archotol.125.5.567. [DOI] [PubMed] [Google Scholar]
- 13.Lee MHM, Teng P, Zaretzky HH, Rubin M. Acupuncture anesthesia in dentistry. A clinical investigation. N Y State D J. 1973;39:299–301. [PubMed] [Google Scholar]
- 14.Mann F. Acupuncture analgesia in dentistry. Lancet. 1972;1:898–899. doi: 10.1016/s0140-6736(72)90760-x. [DOI] [PubMed] [Google Scholar]
- 15.Rosted P. The use of acupuncture in dentistry: A review. Compl Med Int. 1996;3:18–21. [Google Scholar]
- 16.Silva SA. Acupuncture for the relief of pain of facial and dental origin. Anesth Prog. 1989;36:244–245. [PMC free article] [PubMed] [Google Scholar]
- 17.Tany M, Matsudaira K, Sawatsugawa S, Manaka Y. Acupuncture analgesia and its application in dental practice. Am J Acup. 1974;2:287–295. [Google Scholar]
- 18.Shen J. Research on the neurophysiologies mechanisms of acupuncture: Review of selected studies and methodological issues. J Altern Complement Med. 2001;7(suppl 1):S121–S127. doi: 10.1089/107555301753393896. [DOI] [PubMed] [Google Scholar]
- 19.Biella G, Sotgiu ML, Pellegata G, Paulesu E, Castiglioni I, Fazio F. Acupuncture produces central activations in pain regions. Neuroimage. 2001;14:60–66. doi: 10.1006/nimg.2001.0798. [DOI] [PubMed] [Google Scholar]
- 20.Bowsher D. Mechanisms of acupuncture. In: Filshie J, White A, editors. Medical Acupuncture: A Western Scientific Approach. London: Churchill Livingston; 1998. pp. 69–82. [Google Scholar]
- 21.Han JS. Neurochemical basis of acupuncture. Annu Rev Pharmacol Toxicol. 1982;22:193–220. doi: 10.1146/annurev.pa.22.040182.001205. [DOI] [PubMed] [Google Scholar]
- 22.Hess J, Magelvang B, Simonsen H. Acupuncture versus metoprolol in migraine prophylaxis: A randomized trial of trigger point inacrivation. J Intern Med. 1994;235:451–456. doi: 10.1111/j.1365-2796.1994.tb01102.x. [DOI] [PubMed] [Google Scholar]
- 23.Ekblom A, Hansson P, Thomsson M, Thomas M. Increased post operative pain and consumption of analgesics following acupuncture. Pain. 1991;44:241–247. doi: 10.1016/0304-3959(91)90092-C. [DOI] [PubMed] [Google Scholar]
- 24.Grabow L. Controlled study of the analgesic effectivity of acupuncture. Arzneimirtelforschung. 1994;44:554–558. [PubMed] [Google Scholar]
- 25.Kong J, Ma L, Gollub RL, et al. A pilot study of functional magnetic resonance imaging of the brain during manual and electroacupuncture stimulation of acupuncture point (LI-4 Hegu) in normal subjects reveals differential brain activation between methods. J Altern Complement Med. 2002;8:411–419. doi: 10.1089/107555302760253603. [DOI] [PubMed] [Google Scholar]
- 26.Kaptchuk TJ. Acupuncture: Theory, efficacy, and practice. Ann Intern Med. 2002;137:702–703. doi: 10.7326/0003-4819-136-5-200203050-00010. [DOI] [PubMed] [Google Scholar]
- 27.Shen Y, Goddard G. Short term effects of acupuncture on myofascial pain patients after clenching. Pain Pract. 2007;7:256–264. doi: 10.1111/j.1533-2500.2007.00140.x. [DOI] [PubMed] [Google Scholar]
- 28.Okeson JP. Management of Temporomandibular Disorders and Occlusion. 5. St. Louis: Mosby; 2003. pp. 339–342. [Google Scholar]
- 29.Stacher G, Wancura I, Bauer P, Lahoda R, Schulze D. Effect of acupuncture on pain threshold and pain tolerance determined by electrical stimulation of the skin: A controlled study. Am J Chin Med. 1975;3:143–149. doi: 10.1142/s0192415x75000177. [DOI] [PubMed] [Google Scholar]
- 30.Hui KK, Liu J, Makris N, et al. Acupuncture modulates the limbic system and subcortical gray structures of the human brain: Evidence from fMRI studies in normal subjects. Hum Brain Mapp. 2000;9:13–25. doi: 10.1002/(SICI)1097-0193(2000)9:1<13::AID-HBM2>3.0.CO;2-F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tillu A, Roberts C, Tillu S. Unilateral versus bilateral acupuncture on knee function in advanced osteoarthritis of the knee: A prospective randomised trial. Acupunct Med. 2001;19:15–18. doi: 10.1136/aim.19.1.15. [DOI] [PubMed] [Google Scholar]
- 32.Audette JF, Wang F, Smith H. Bilateral activation of motor unit potentials with unilateral needle stimulation of active moyfascial trigger points. Am J Phys Med Rehabil. 2004;83:368–374. doi: 10.1097/01.phm.0000118037.61143.7c. [DOI] [PubMed] [Google Scholar]
- 33.Goddard G, Shen Y, Steele B. A controlled trial of placebo vs real acupuncture. Pain. 2005;4:237–242. doi: 10.1016/j.jpain.2004.12.009. [DOI] [PubMed] [Google Scholar]
- 34.Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998;352:364–365. doi: 10.1016/S0140-6736(97)10471-8. [DOI] [PubMed] [Google Scholar]
- 35.Farrar JT, Young JP, Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149–158. doi: 10.1016/S0304-3959(01)00349-9. [DOI] [PubMed] [Google Scholar]
- 36.Kam E, Eslick G, Campbell I. An audit of the effectiveness of acupuncture on musculoskeletal pain in primary health care. Acupunct Med. 2002;20:35–38. doi: 10.1136/aim.20.1.35. [DOI] [PubMed] [Google Scholar]
- 37.Park J, White A, Stevinson C, Ernst E, James M. Validating a new non-penetrating sham acupuncture device: Two randomised controlled trials. Acupunct Med. 2002;20:168–174. doi: 10.1136/aim.20.4.168. [DOI] [PubMed] [Google Scholar]
- 38.Smith P, Mosscrop D, Davies S, Sloan P, Al-Ani Z. The efficacy of acupuncture in the treatment of temporomandibular joint myofascial pain: A randomised controlled trial. J Dent. 2007;35:259–267. doi: 10.1016/j.jdent.2006.09.004. [DOI] [PubMed] [Google Scholar]
- 39.Michelotti A, Farella M, Stellato A, Martina R, De Laat A. Tactile and pain threholds in patients with myofascial pain of the jaw muscles: A case-control study. J Orofac Pain. 2008;22:139–145. [PubMed] [Google Scholar]
- 40.Karst M, Rollmk JD, Fink M, Reinhard M, Piepenbrock S. Pressure pain threshold and needle acupuncture in chronic tension-type headache: A double-blind placebo-controlled study. Pain. 2000;88:199–203. doi: 10.1016/S0304-3959(00)00315-8. [DOI] [PubMed] [Google Scholar]
- 41.McMillan AS, Nolan A, Kelly PJ. The efficacy of dry needling and procaine in the treatment of myofascial pain in the jaw muscles. J Orofac Pain. 1997;11:307–314. [PubMed] [Google Scholar]
- 42.Tough EA, White AR, Cummings M, Richards SH, Campbell JL. Acupuncture and dry needling in the management of myofascial trigger point pain: A systematic review and meta-analysis of randomized controlled trials. Eur J Pain. 2009;13:3–10. doi: 10.1016/j.ejpain.2008.02.006. [DOI] [PubMed] [Google Scholar]