

Abstract
Background
Hemorrhagic cystitis is a common cause of morbidity after allogeneic stem cell transplantation, frequently associated with BK virus infection. We hypothesized that patients with positive BK viruria before unrelated or mismatched related donor allogeneic hematopoietic stem cell transplantation have a higher incidence of hemorrhagic cystitis.
Design and Methods
To test this hypothesis, we prospectively studied 209 patients (median age 49 years, range 19–71) with hematologic malignancies who received bone marrow (n=78), peripheral blood (n=108) or umbilical cord blood (n=23) allogeneic hematopoietic stem cell transplantation after myeloablative (n=110) or reduced intensity conditioning (n=99). Donors were unrelated (n=201) or haploidentical related (n=8).
Results
Twenty-five patients developed hemorrhagic cystitis. Pre-transplant BK viruria detected by quantitative PCR was positive in 96 patients. The one-year cumulative incidence of hemorrhagic cystitis was 16% in the PCR-positive group versus 9% in the PCR-negative group (P=0.1). The use of umbilical cord blood or a haploidentical donor was the only significant predictor of the incidence of hemorrhagic cystitis on univariate analysis. There was also a trend for a higher incidence after myeloablative conditioning. Multivariate analysis showed that patients who had a positive PCR pre-transplant and received haploidentical or cord blood grafts with myeloablative conditioning had a significantly higher risk of developing hemorrhagic cystitis (58%) than all other recipients (7%, P<0.001).
Conclusions
Hemorrhagic cystitis is the result of a complex interaction of donor type, preparative regimen intensity, and BK viruria.
Keywords: hemorrhagic cystitis, polyomavirus, allogeneic stem cell transplant
Introduction
Hemorrhagic cystitis (HC) is often a serious complication of renal and hematopoietic stem cell transplants (HSCT), with the potential to cause significant morbidity.1–3 It occurs in up to 70% of hematopoietic stem cell transplant recipients and is associated with prolonged hospitalization.4,5 Early bleeding (occurring 24–72 hours after transplant) is usually ascribed to toxic effects of drugs, while late occurring cystitis is multifactorial.4–8 Reported predisposing factors include allogeneic transplant, advanced age at transplantation, possibly graft-versus-host disease (GVHD), thrombocytopenia, coagulopathy and viral infections (polyoma BK virus, cytomegalovirus and adenovirus). Non-chemotherapy induced hemorrhagic cystitis is usually documented later after hematopoietic stem cell transplants (more than two weeks in the allogeneic setting).9–13
Polyomavirus hominis 1 (genus Polyomaviridae), the BK virus, is a non-encapsulated DNA virus that is highly prevalent in healthy adults with up to 90% seropositivity. Transmission is believed to occur via the respiratory tract, especially during early-childhood years. Infection is usually asymptomatic or may be associated with fever and mild upper respiratory symptoms.10,11,14 After first infection, polyomavirus can be latent in the kidneys, urothelium, and other organs, and may reactivate during immunosuppression. BK virus infection has been connected with development of hemorrhagic cystitis after allogeneic transplant, but most studies detected the virus at the time of bleeding, therefore not allowing the risk imposed by asymptomatic infection to be estimated.7,15
We have shown that hemorrhagic cystitis is more likely to occur in unrelated than in related-donor hematopoietic stem cell transplants,16 and in this analysis we focused on patients receiving unrelated or mismatched haploidentical related hematopoietic stem cell transplants. Here we postulated that a positive BK viruria documented by PCR prior to transplant would increase the risk of hemorrhagic cystitis in recipients of unrelated or haploidentical transplants. Because of poorer immune reconstitution, we also hypothesized that recipients of cord blood and haploidentical transplants would have a higher incidence of hemorrhagic cystitis than recipients of unrelated donor transplants, and prospectively investigated these hypotheses in a cohort of such patients transplanted in our institution.
Design and Methods
Patient and treatment characteristics
The study cohort includes 80% of all adult patients who underwent allogeneic hematopoietic stem cell transplants using an unrelated, haploidentical related, or unrelated cord blood donor at The University of Texas MD Anderson Cancer Center (UTMDACC) from September 2005 to September 2007 (n=209). Patients were excluded due to unavailability of baseline or transplant day 30 samples, early death (within the first 30 days after transplant) or if undergoing a second transplant. Data regarding treatment outcomes were prospectively collected in the department database. Patients were monitored for signs and symptoms of hemorrhagic cystitis on a daily basis during the initial admission for hematopoietic stem cell transplant, then twice weekly after discharge until approximately 100 days after transplant. The retrospective data review was approved by the institutional review board at the UTMDACC.
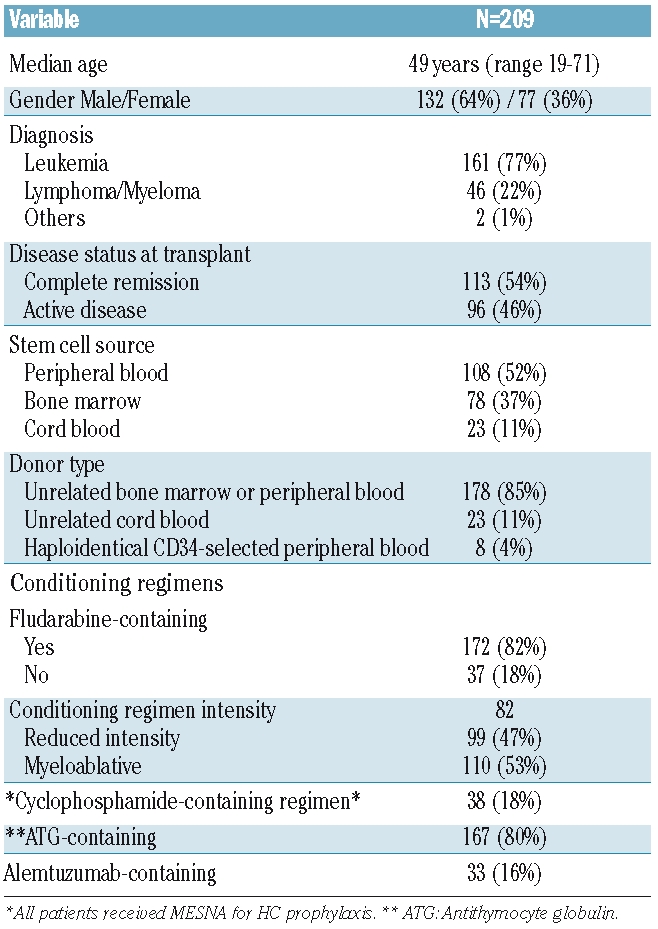
Patient and treatment characteristics are presented in Table 1. Most patients received unrelated bone marrow or peripheral blood stem cell transplants (85%), after a myeloablative or reduced intensity conditioning regimen in 52% and 48% of the cases, respectively. Graft versus host disease prophylaxis consisted of tacrolimus in combination with mini-methotrexate 5 mg/m2 on days +1, +3, +6 and +11 (n=178), or to mycophenolate mofetil (n=23), or CD34 selection/T-cell depletion in haploidentical transplants (n=8). Anti-thymocyte globulin was part of the preparative regimen in all transplants with the exception of combinations containing Campath. Median time to neutrophil and platelet engraftment was 14 days (range 1–51), and 20 days (range 9–64), respectively. Cumulative incidence of grade II–IV and III–IV acute GVHD was 33% and 12%, respectively. Patients developing grade II–IV acute GVHD were initially treated with 2 mg/Kg of methylprednisolone. For the purposes of this analysis, only grade II–IV acute GVHD cases were included.
Table 1.
Patient and treatment characteristics.
Definitions
Considering that hemorrhagic cystitis occurred as frequently in all quartiles of polyoma viruria, BK virus PCR was considered positive if any number of viral copies were detected. Hemorrhagic cystitis occurring more than one week after transplant was defined as “late-onset”. Cystitis was defined by presence of dysuria, pain, increased frequency and/or other urinary tract symptoms, and by the presence of hematuria. Hemorrhagic cystitis was graded as: grade 0 = none; grade I = microscopic hematuria with urinary symptoms; grade II = macroscopic hematuria; grade III = macroscopic hematuria with clots; and grade IV = macroscopic hematuria with intervention for clot evacuation and/or urinary retention.2,6,12 Patients with hemorrhagic cystitis and clots were treated with continuous bladder irrigation, and percutaneous nephrostomy was used if persistent hydronephrosis was documented.
The following preparative regimens were considered myeloablative: BU/MEL (IV busulfan 130mg/m2 for four days and melphalan 70 mg/m2 for two days); intravenous busulfan at 130mg/m2 or 3.2 mg/Kg daily for four days in combination with clofarabine, fludarabine or cyclophosphamide; FM/THIO (fludarabine 30 mg/m2 for four days, melphalan 140 mg/m2 and thiotepa 10 mg/Kg); VP16/TBI (etoposide and 12 Grays total body irradiation: only 5 patients received radiation at this dose); BEAM (carmustine 300mg/m2, etoposide 200 mg/m2 and cytarabine 200 mg/m2 for four days, and melphalan 140 mg/m2).
The following regimens were considered to be of reduced intensity: FCR (fludarabine 30 mg/m2 daily for three days, cyclophosphamide 750 mg/m2 daily for three days, and rituximab 375 mg/m2 for one day plus 1000 mg/m2 for three days with and without alemtuzumab; a small subset received the addition of 2 Gray TBI); FM (fludarabine 30 mg/m2 for four days and melphalan 140 mg/m2); intravenous busulfan at 130mg/m2 for two days with fludarabine 30 mg/m2 for four days; TLI (total lymphoid irradiation).
Polyoma virus studies
We prospectively performed quantitative PCR for BK virus on urine samples collected before admission, and on the 30th and 60th day after hematopoietic stem cell transplant. The quantitative BK virus assay was performed at Focus Diagnostics, Inc. (Cyprus, CA) with a commercially available kit. The PCR target is the large T-antigen gene, but exact primer/probe (TaqMan) sequences are proprietary. The assay is reported to have no cross-reactivity with JC virus.17
Urine cytology
We also performed urine cytology in the same samples, searching for cytological changes compatible with polyoma virus infection.18 Each urine specimen was processed for cytological evaluation by centrifugation for 10 min at 300 rcf. The sample was resuspended after stepwise addition of 2–5 mL of glacial acetic acid with vortex, immediately followed by 2–5 mL of normal saline with vortex. The sample was then centrifuged for 5 min at 300 rcf. After removal of supernatant, the sediment was pulled into a glass Pasteur pipette and examined for clarity. Cytospin slides were prepared by centrifugation for 5 min at 80 rcf and immediately fixed in 95% alcohol and stained by the Papanicolaou method. Polyomavirus cytopathic effect was identified in samples containing cells exhibiting marked nuclear enlargement with ground glass chromatin (viral inclusion; “decoy cell”) occupying most of the nucleus and/or lace-like clumped chromatin (empty post-inclusion).
Statistical methods
The one-year cumulative incidence of hemorrhagic cystitis was estimated considering death without hemorrhage as a competing event. Risk factors for the development of hemorrhagic cystitis were evaluated on univariate and multivariate analysis using Cox’s regression model. The following variables were included: donor type (unrelated, haploidentical and cord blood), conditioning regimen intensity, BK virus PCR status prior to and on day 30 after hematopoietic stem cell transplant, use of cyclophosphamide, stem cell source, age, engraftment, and acute GVHD. Since median time to hemorrhagic cystitis was less than 60 days, day 60 viruria was not used in the model. Landmark analysis was used to assess the correlation between BK virus PCR status on transplant day 30 and subsequent rate of hemorrhagic cystitis development. Statistical significance was defined at 0.05. Statistical analysis was performed using STATA 9.0.
Results
Hemorrhagic cystitis
Hemorrhagic cystitis was diagnosed in 25 of the 209 patients. With a median follow-up of nine months, the median and mean time to bleeding was 49 and 64.4 days, respectively (range 4–230 days; lower quartile = 24 days; upper quartile = 82 days). There were 3 cases of grade I (12% of all hemorrhagic cystitis), 11 (44%) grade II, 8 (32%) grade III and 3 (12%) grade IV; all grade IV cases occurred in recipients of cord blood transplants. The median time to developing hemorrhagic cystitis was 52, 51.5, 49 and 41 days for patients with grade IV, III, II and I cystitis, respectively. Six patients (24% of HC cases) developed hemorrhagic cystitis before platelet engraftment, while 5 had cystitis before neutrophil engraftment (20% of HC cases).
BK viruria and hemorrhagic cystitis
The mean number of viral copies pre-hematopoietic stem cell transplant among those with positive PCR was 1.9×107 copies/mL (range 300 – 2×108 copies/mL). There was no direct correlation between viral load and development of hemorrhagic cystitis. We actually saw hemorrhagic cystitis among patients with very low levels of viruria, and the proportion of patients with hemorrhagic cystitis was similar among patients in the lower and higher quartiles as follows: 25% quartile, 2,100 copies/mL and 17% rate of HC; 50% quartile, 12,000 copies/mL and 12% of HC; 75% quartile, 140,000 copies/mL and HC in 17%; and 95% quartile, 2×108 copies/mL, HC rate of 17%.
Among patients who were BK virus positive prior to transplant (n=96), the median log BK viral load pre-hematopoietic stem cell transplant was not significantly different in patients who subsequently bled (n=15/96; median of 9.5 copies/mL, range 5–19) versus those who did not develop hemorrhagic cystitis (n=81/96; median of 9.4 copies/mL, range 5.3–19, P=0.8).
Mean polyoma viruria was 9.7×107 copies/mL (range 300–2×108 copies/mL, n=105) and 7.7×107 copies/mL (range 200–2×108 viral copies/mL; n=101), respectively 30 and 60 days after hematopoietic stem cell transplant. There was a statistically significant increase in mean viruria from pre-hematopoietic stem cell transplant when compared to both time points after transplant (P=0.0002 and P=0.002, respectively). We repeated the PCR at the time of diagnosis of hemorrhagic cystitis in 11 cases. Viral load increased in 8 cases and remained the same in 3, when compared to pre-transplant levels. In addition, the mean number of viral copies/mL rose significantly (3.3×107 vs. 1.2×108, P=0.01).
Univariate analysis
BK viruria was detected in 96 patients prior to hematopoietic stem cell transplant (46% of the cohort). The one-year cumulative incidence (CI) of hemorrhagic cystitis was 18% (n=15) for PCR positive versus 10% (n=10) among PCR negative patients (Hazard ratio (HR) 1.94, 95% confidence interval (CI), 0.9–4.4; P=0.095). The proportion of patients with BK viruria increased to 58% and 61%, respectively 30 and 60 days after hematopoietic stem cell transplant (missing data on 36 patients on day + 60). Figure 1 describes presence of BK viruria during the first 60 days after hematopoietic stem cell transplant and development of hemorrhagic cystitis.
Figure 1.

Polyoma viruria and hemorrhagic cystitis during the first 60 days after transplant. Median time to cystitis was 49 days (n=168 on day 60).
In addition to BK viruria, donor type and intensity of preparatory conditioning regimen were associated with the development of hemorrhagic cystitis on univariate analysis. Hemorrhagic cystitis occurred in 8 of 31 patients who received a haploidentical or cord blood transplant, versus 17 of 178 recipients of unrelated bone marrow or peripheral blood grafts (cumulative incidence of 31% vs. 11%; respectively, HR 3.1, 95% CI, 1.3–7.2; P=0.009; Figure 2A). Use of myeloablative conditioning regimen was associated with a higher cumulative incidence of hemorrhagic cystitis when compared to the subgroup treated with reduced intensity conditioning regimens, with a borderline statistically significant P value (18 of 110 patients, (17%), vs. 7 of 99 (7%), respectively; HR 2.3, 95% CI, 0.98–5.6; P=0.056; Figure 2B).
Figure 2.
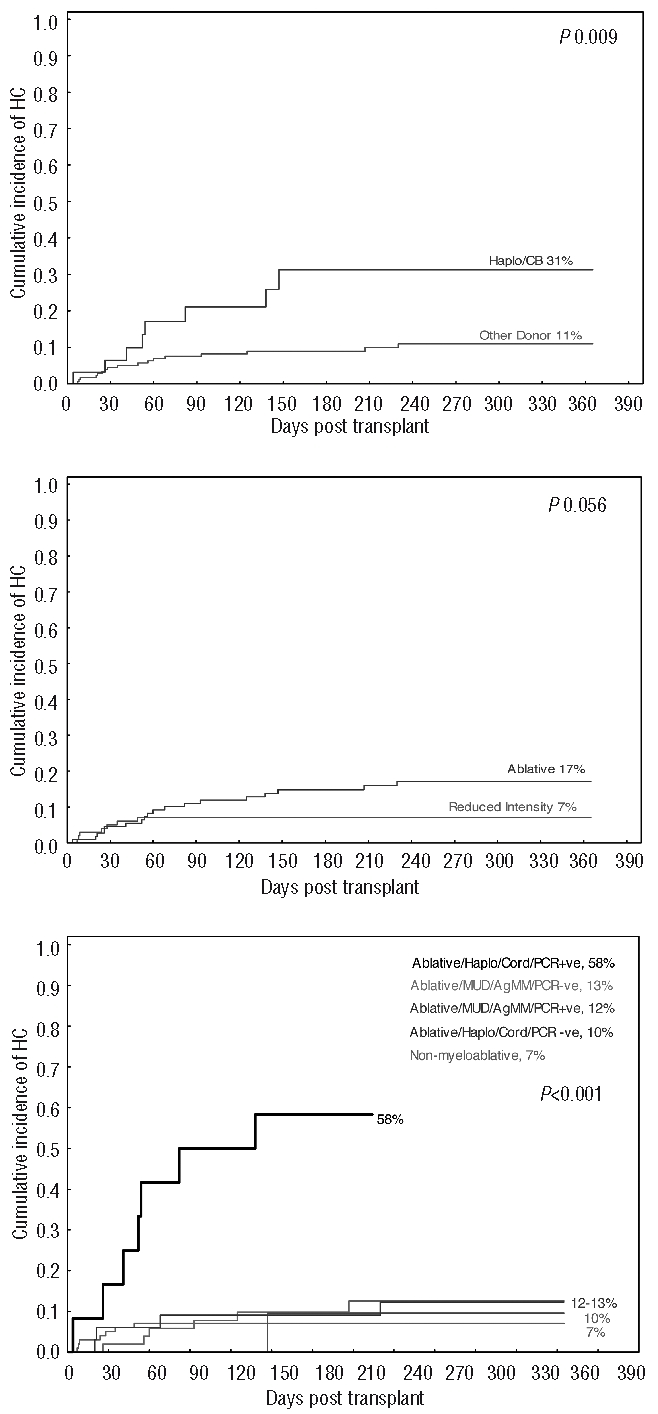
(A) Cumulative incidence of hemorrhagic cystitis as a function of donor type. Recipients of haploidentical (haplo) and cord blood (CB) transplants had a higher incidence of hemorrhagic cystitis than recipients of unrelated bone marrow or peripheral blood transplants. (B) Cumulative incidence of hemorrhagic cystitis as a function of conditioning regimen intensity. (C) High cumulative incidence of hemorrhagic cystitis in recipients of ablative haploidentical (haplo) or cord blood (cord) transplants who had BK viruria (+ve) prior to transplant, when compared to recipients of unrelated donor (UD) transplants (PCR +ve or PCR negative –ve).
None of the remaining evaluated factors was significantly associated with hemorrhagic cystitis development. The cumulative incidence of bleeding occurring after day 30 was comparable in patients with positive (8%) and those with negative (5%) BK viruria 30 days after hematopoietic stem cell transplant (P=0.4).
Use of cyclophosphamide-containing preparative regimen was not associated with an increased cumulative incidence of hemorrhagic cystitis (4%). However, cyclophosphamide was primarily used in reduced intensity conditioning in combination with low-dose total body irradiation, fludarabine and Campath. In addition, use of bone marrow versus peripheral blood had no influence on development of hemorrhagic cystitis (incidence of 12% vs. 8%, respectively, P=0.4). Similarly, no significant impact was found for age, diagnosis, disease status (remission vs. active disease; incidence of 14% vs. 9.4%, respectively), use of fludarabine-based conditioning (incidence of 12.8% with fludarabine vs. 8% without, P=0.6), platelet or neutrophil engraftment, or a diagnosis of grade II–IV acute GVHD (HR 1.3, 95% CI, 0.5–3.5 P=0.6), considered as a time dependent variable (Table 2). Post-hematopoietic stem cell transplant cytomegalovirus reactivation occurred in 48% (n=100) of the patients during the first four months. There was no correlation between cytomegalovirus antigenemia and development of hemorrhagic cystitis (incidence of 13% vs. 11% for antigenemia positive and negative patients, respectively).
Table 2.
Incidence of hemorrhagic cystitis.

Correlation of urinary cytology and BK PCR
Urine cytology data was available in 208 patients prior to hematopoietic stem cell transplant. Nineteen (9%) were deemed to have changes compatible with polyoma virus infection. Hemorrhagic cystitis rates among cytology positive and negative patients were 16% (3 of 19) and 12% (22 of 189), respectively. Double negative samples (PCR and cytology) had a cystitis rate of 9% (9 of 103), while double positive patients had a hemorrhagic cystitis rate of 22% (2 of 9 patients). Cytology negative but PCR positive samples were associated with cystitis in 15% of the cases (13 of 86), while cytology positive but PCR negative cases were linked to hemorrhagic cystitis in 10% (one of 10 cases). Ultimately, 22 of 25 patients (88%) who had hemorrhagic cystitis had no polyoma-induced cytological changes pre-transplant, while 10 of 25 (40%) had no evidence of infection by PCR. At the time of diagnosis of hemorrhagic cystitis, 10 of 13 patients for whom this information was available had cytological changes suggestive of BK infection, usually associated with viruria greater than 1×107 copies/mL.
Hospital stay
During the first 100 days after transplant, median hospital stay for patients who developed hemorrhagic cystitis was 41 days (range 14–81), versus 26 days (range 9–95) for patients who did not (P=0.01). Patients with BK viruria prior to transplant had a stay of 29 (range 9–83) versus 25 days (range 11–95; P=0.2). Although hemorrhagic cystitis was associated with significant morbidity, survival was not affected by presence of BK viruria and/or by cystitis. Fifty-six percent of the patients with hemorrhagic cystitis were readmitted to hospital, versus 44% of patients without cystitis.
Multivariate analysis
We performed stratified and multivariate analysis to adjust for the factors shown to be significant on univariate analysis (Table 3). Stratified analysis showed that the impact of donor type and PCR positivity pre-transplant were significant in patients who received an ablative regimen, but not in those patients who received reduced intensity conditioning. We adjusted for this interaction by considering the impact of donor type and PCR positivity pre-transplant only in patients who received an ablative conditioning, allowing for reduced intensity conditioning as a reference group. This classification showed that the incidence of hemorrhagic cystitis was lowest among recipients of reduced intensity conditioning and highest (58%) among recipients of ablative regimens, haploidentical and cord blood transplants, and those who had a positive PCR pre-transplant (58% vs. 7% for the reference group, HR 13.6, 95% CI, 4.7–39 P<0.001; Figure 2C and Table 3).
Table 3.
Multivariate model for development of hemorrhagic cystitis.

Discussion
Our study showed that polyoma viruria was not per se an independent risk factor for hemorrhagic cystitis, contrary to our central hypothesis. However, viruria interacted with regimen intensity and donor type leading to a very high risk of hemorrhage after transplant. We identified a subgroup of patients who are very likely to develop hemorrhagic cystitis: recipients of haploidentical or unrelated cord blood transplants conditioned with myeloablative regimens who had positive viruria at the time of admission for treatment.
This study recapitulates in a prospective fashion our previous (retrospective) analysis that showed unrelated transplants to be associated with more hemorrhagic cystitis than matched related transplants.16 In that study, however, we did not have BK virus information, and only ablative (radiation-based) conditioning was used. One cannot ignore the impression that there is a continuum of increasing hemorrhagic cystitis rates going from related, unrelated bone marrow or peripheral blood transplants, to unrelated cord blood and haploidentical transplants. It is possible that this reflects poorer immune recovery intrinsic to the latter group. Interestingly, it has been reported by others9 that although BK viruria was detected in autologous and allogeneic transplant patients, only the allogeneic group developed hemorrhagic cystitis. Here, infection per se was not statistically significantly associated with cystitis, illustrating the complexity of the problem. Contrary to what has been previously suggested and would be expected if the immune recovery deficit alone is at play, we did not see a correlation of hemorrhagic cystitis with development of graft versus host disease, studied as a time-dependent variable. Although we did not have detailed data on steroid or other immunosuppressant use, the initial treatment is standardized in our institution.
Another observation is that hemorrhagic cystitis occurred after engraftment of neutrophils in the majority of the patients (and in most cases after platelet engraftment). We speculate that the neutrophil ‘requirement’ illustrates the presence of an inflammatory component, possibly triggered by the preparative regimen and BK virus presence.
Cyclophosphamide use, a common ‘culprit’ in this setting, did not contribute to hemorrhagic cystitis here. This is likely explained by the association of this drug with reduced intensity conditioning in our institution, further suggesting that dose intensity contributes to the problem. Most of our hemorrhagic cystitis cases were of late onset, and were therefore less likely to be chemotherapy-related. Given this limitation, we do not know if our conclusions would extend to fully myeloablative, cyclophosphamide-containing regimens. Use of such preparative regimens has previously been demonstrated to be a risk factor for cystitis (mostly of early onset), although not all investigators confirmed this association while others saw no difference in late onset hemorrhagic cystitis incidence between reduced intensity conditioning and ablative regimens.11,13,15, 19–21
The association of BK viruria and hemorrhagic cystitis has been under investigation for many years, but we failed to document a correlation between viral load and hemorrhagic cystitis (or severity of cystitis) as previously suggested.11,12,22–24 The proportion of patients with hemorrhagic cystitis was very similar in all quartiles of urinary viral load. Given the lack of a clear cut threshold, we opted for labeling any viruria level as ‘positive’. Urine cytology did not correlate with BK viruria as defined here, neither did it predict hemorrhagic cystitis. However, we did not rule out a possible correlation of cytological changes with high urinary viral loads (data not shown). Our observation that combining urinary cytological changes with viral load increased the positive predictive value for hemorrhagic cystitis suggests the possibility that BK infection of the urothelium without detectable viruria might account for hemorrhagic cystitis in some patients. This hypothesis, if true, would strengthen the association between BK virus and hemorrhagic cystitis. It also would strengthen the ‘biological’ explanation for the complex interaction between BK virus, regimen intensity and donor type that we have advanced, as greater immune incompetence might be correlated with urothelial infection with or without viruria.
We somewhat arbitrarily grouped recipients of unrelated cord blood and haploidentical related transplants together. Biologically, however, the two subgroups are likely different in that cord blood donors lack immunity to BK virus, while haploidentical grafts are more often associated with poor immune reconstitution after hematopoietic stem cell transplant.25
A limitation of our study is that we did not measure BK viremia. Others have shown an association between plasma viral load and development of hemorrhagic cystitis21 and it is possible that measuring both viremia and viruria may be more informative than measuring each separately. Another limitation is the lack of information on other viruses, such as adenovirus, which can also lead to hemorrhagic cystitis. However, since our cohort was comprised of adult patients only, the contribution of adenovirus infection is likely to be small, in contrast to a pediatric population.3,26
Other potential risk factors for hemorrhagic cystitis studied here had no significant impact in this prospectively studied cohort. Age, platelet engraftment, bone marrow versus peripheral blood grafts, BK virus PCR 30 days after transplant, and development of acute graft versus host disease were not independently associated with hemorrhagic cystitis.7,16,19 We believe these findings reinforce the interaction between BK virus, preparative regimen and donor type. The identification of this high-risk subgroup may provide a target for interventions designed to improve polyoma virus immune response post-hematopoietic stem cell transplant, and for avoidance of drugs that may increase incidence of hemorrhagic cystitis (such as cyclophosphamide). Since we did not take into account intensity and duration of immunosuppressive treatment used to manage graft versus host disease, nor the results of its treatment, our graft versus host disease findings are somewhat limited and should be interpreted accordingly.
The morbidity of this complication should not be underestimated, as well as the logistical and financial implications of prolonged admissions and hemorrhagic cystitis-mandated urological interventions. Future insights in immune reconstitution after hematopoietic stem cell transplant from donors other than HLA identical siblings are expected to shed light on this complex syndrome, and hopefully allow us to minimize the consequences of this complication of hematopoietic transplants.
Footnotes
Authorship and Disclosures
LdPS and MdL collected and analyzed data, designed the study and wrote the manuscript; NAS, PAP, RR, AC and LG collected and analyzed data, and reviewed the manuscript; RMS analyzed the data and reviewed the manuscript; AG, JN, JAW, DP, ME-Z, PA, ES, RJ, UP, SG, and REC treated patients on study and critically reviewed the manuscript; JT, X-YH and JS reviewed the manuscript, and analyzed PCR and cytology data.
The authors report no potential conflicts of interest.
References
- 1.Sencer SF, Haake RJ, Weisdorf DJ. Hemorrhagic cystitis after bone marrow transplantation. Risk factors and complications. Transplantation. 1993;56(4):875–9. doi: 10.1097/00007890-199310000-00020. [DOI] [PubMed] [Google Scholar]
- 2.Bedi A, Miller CB, Hanson JL, Goodman S, Ambinder RF, Charache P, et al. Association of BK virus with failure of prophylaxis against hemorrhagic cystitis following bone marrow transplantation. J Clin Oncol. 1995;13(5):1103–9. doi: 10.1200/JCO.1995.13.5.1103. [DOI] [PubMed] [Google Scholar]
- 3.Gorczynska E, Turkiewicz D, Rybka K, Toporski J, Kalwak K, Dyla A, et al. Incidence, clinical outcome, and management of virus-induced hemorrhagic cystitis in children and adolescents after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2005;11(10):797–804. doi: 10.1016/j.bbmt.2005.06.007. [DOI] [PubMed] [Google Scholar]
- 4.Shepherd JD, Pringle LE, Barnett MJ, Klingemann HG, Reece DE, Phillips GL. Mesna versus hyperhydration for the prevention of cyclophosphamide-induced hemorrhagic cystitis in bone marrow transplantation. J Clin Oncol. 1991;9(11):2016–20. doi: 10.1200/JCO.1991.9.11.2016. [DOI] [PubMed] [Google Scholar]
- 5.Tomonari A, Takahashi S, Ooi J, Fukuno K, Takasugi K, Tsukada N, Konuma T, et al. Hemorrhagic cystitis in adults after unrelated cord blood transplantation: a single-institution experience in Japan. Int J Hematol. 2006;84(3):268–71. doi: 10.1532/IJH97.05169. [DOI] [PubMed] [Google Scholar]
- 6.Droller MJ, Saral R, Santos G. Prevention of cyclophosphamide-induced hemorrhagic cystitis. Urology. 1982;20(3):256–8. doi: 10.1016/0090-4295(82)90633-1. [DOI] [PubMed] [Google Scholar]
- 7.Leung AY, Suen CK, Lie AK, Liang RH, Yuen KY, Kwong YL. Quantification of polyoma BK viruria in hemorrhagic cystitis complicating bone marrow transplantation. Blood. 2001;98(6):1971–8. doi: 10.1182/blood.v98.6.1971. [DOI] [PubMed] [Google Scholar]
- 8.Freedman A, Ehrlich RM, Ljung BM. Prevention of cyclophosphamide cystitis with 2-mercaptoethane sodium sulfonate: a histologic study. J Urol. 1984;132(3):580–2. doi: 10.1016/s0022-5347(17)49751-5. [DOI] [PubMed] [Google Scholar]
- 9.Apperley JF, Rice SJ, Bishop JA, Chia YC, Krausz T, Gardner SD, et al. Late-onset hemorrhagic cystitis associated with urinary excretion of polyomaviruses after bone marrow transplantation. Transplantation. 1987;43(1):108–12. doi: 10.1097/00007890-198701000-00024. [DOI] [PubMed] [Google Scholar]
- 10.Leung AY, Yuen KY, Kwong YL. Polyoma BK virus and haemorrhagic cystitis in haematopoietic stem cell transplantation: a changing paradigm. Bone Marrow Transplant. 2005;36(11):929–37. doi: 10.1038/sj.bmt.1705139. [DOI] [PubMed] [Google Scholar]
- 11.Giraud G, Bogdanovic G, Priftakis P, Remberger M, Svahn BM, Barkholt L, et al. The incidence of hemorrhagic cystitis and BK-viruria in allogeneic hematopoietic stem cell recipients according to intensity of the conditioning regimen. Haematologica. 2006;91(3):401–4. [PubMed] [Google Scholar]
- 12.Dropulic LK, Jones RJ. Polyomavirus BK infection in blood and marrow transplant recipients. Bone Marrow Transplant. 2008;41(1):11–8. doi: 10.1038/sj.bmt.1705886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bogdanovic G, Priftakis P, Giraud G, Kuzniar M, Ferraldeschi R, Kokhaei P, et al. Association between a high BK virus load in urine samples of patients with graft-versus-host disease and development of hemorrhagic cystitis after hematopoietic stem cell transplantation. J Clin Microbiol. 2004;42(11):5394–6. doi: 10.1128/JCM.42.11.5394-5396.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goudsmit J, Wertheim-van Dillen P, van Strien A, van der Noordaa J. The role of BK virus in acute respiratory tract disease and the presence of BKV DNA in tonsils. J Med Virol. 1982;10(2):91–9. doi: 10.1002/jmv.1890100203. [DOI] [PubMed] [Google Scholar]
- 15.Azzi A, Cesaro S, Laszlo D, Zakrzewska K, Ciappi S, De Santis R, et al. Human polyomavirus BK (BKV) load and haemorrhagic cystitis in bone marrow transplantation patients. J Clin Virol. 1999;14(2):79–86. doi: 10.1016/s1386-6532(99)00055-4. [DOI] [PubMed] [Google Scholar]
- 16.El-Zimaity M, Saliba R, Chan K, Shahjahan M, Carrasco A, Khorshid O, et al. Hemorrhagic cystitis after allogeneic hematopoietic stem cell transplantation: donor type matters. Blood. 2004;103(12):4674–80. doi: 10.1182/blood-2003-08-2815. [DOI] [PubMed] [Google Scholar]
- 17.Focus diagnostic. [Accessed in 5/2009]. http://www.focusdx.com.
- 18.Yuste RS, Frias C, Lopez A, Vallejo C, Martin P, Bellas C. Diagnostic value of JC/BK virus antibody immunohistochemistry staining in urine samples from post-transplant immunosuppressed patients in relation to polyomavirus reactivation. Acta Cytol. 2008;52(2):191–5. doi: 10.1159/000325478. [DOI] [PubMed] [Google Scholar]
- 19.Giraud G, Priftakis P, Bogdanovic G, Remberger M, Dubrulle M, Hau A, et al. BK-viruria and haemorrhagic cystitis are more frequent in allogeneic haematopoietic stem cell transplant patients receiving full conditioning and unrelated-HLA-mismatched grafts. Bone Marrow Transplant. 2008;41(8):737–42. doi: 10.1038/sj.bmt.1705962. [DOI] [PubMed] [Google Scholar]
- 20.Bogdanovic G, Priftakis P, Giraud G, Dalianis T. A related donor and reduced intensity conditioning reduces the risk of development of BK virus-positive haemorrhagic cystitis in allogeneic haematopoetic stem cell-transplanted patients. Anticancer Res. 2006;26(2B):1311–8. [PubMed] [Google Scholar]
- 21.Erard V, Kim HW, Corey L, Limaye A, Huang ML, Myerson D, et al. BK DNA viral load in plasma: evidence for an association with hemorrhagic cystitis in allogeneic hematopoietic cell transplant recipients. Blood. 2005;106(3):1130–2. doi: 10.1182/blood-2004-12-4988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Arthur RR, Shah KV, Baust SJ, Santos GW, Saral R. Association of BK viruria with hemorrhagic cystitis in recipients of bone marrow transplants. N Engl J Med. 1986;315(4):230–4. doi: 10.1056/NEJM198607243150405. [DOI] [PubMed] [Google Scholar]
- 23.Bogdanovic G, Ljungman P, Wang F, Dalianis T. Presence of human polyomavirus DNA in the peripheral circulation of bone marrow transplant patients with and without hemorrhagic cystitis. Bone Marrow Transplant. 1996;17(4):573–6. [PubMed] [Google Scholar]
- 24.Bogdanovic G, Priftakis P, Taemmeraes B, Gustafsson A, Flaegstad A, Winiarski J, et al. Primary BK virus (BKV) infection due to possible BKV transmission during bone marrow transplantation is not the major cause of hemorrhagic cystitis in transplanted children. Pediatr Transplant. 1998;2(4):288–93. [PubMed] [Google Scholar]
- 25.Li J, Melenhorst J, Hensel N, Rezvani K, Sconocchia G, Kilical Y, et al. T-cell responses to peptide fragments of the BK virus T antigen: implications for cross-reactivity of immune response to JC virus. J Gen Virol. 2006;87(Pt 10):2951–60. doi: 10.1099/vir.0.82094-0. [DOI] [PubMed] [Google Scholar]
- 26.Yamamoto R, Kusumi E, Kami M, Yuji K, Hamaki T, Saito A, et al. Late hemorrhagic cystitis after reduced-intensity hematopoietic stem cell transplantation (RIST) Bone Marrow Transplant. 2003;32(11):1089–95. doi: 10.1038/sj.bmt.1704261. [DOI] [PubMed] [Google Scholar]