

Abstract
Women are more prone to anterior cruciate ligament (ACL) injury during cutting sports than men. The purpose of this study was to examine knee kinematic and ground reaction forces (GRF) differences between genders during cutting. Male and female athletes performed cutting trials while force platform and video data were recorded (180 Hz). Differences (p ≤ .05) were observed between groups for knee flexion at contact and GRF at maximum knee flexion. Women averaged 5.8° less flexion at contact and 1.0 N· (kg·m·s−1)−1 greater GRF at maximum flexion. Knee range of motion and peak GRF variables were not significantly different, but women had greater values. Women exhibited technique characteristics believed to increase ACL injury risk, but men exhibiting similar characteristics were also observed and could also be at risk.
Keywords: anterior cruciate ligament, cutting, female athletes, knee injury
Female athletes are at greater risk of noncontact anterior cruciate ligament (ACL) injuries than male athletes in sports involving sudden deceleration, landing, and cutting (Arendt & Dick, 1995; Dehaven & Lintner, 1986; Gray et al., 1985; Moeller & Lamb, 1997; Zelisko, Noble, & Porter, 1982). Numerous studies have investigated the nature of ACL injuries and possible explanations for the differences in injury rates between genders. Several causes have been suggested, including anatomical, physiological, and biomechanical characteristics, such as differences in intercondylar notch configuration (Anderson, Lipscomb, Liudahl, & Addlestone, 1987; LaPrade & Burnett, 1994; Souryal & Freeman, 1993), inherent joint looseness and ligament laxity (Weesner, Albohin, & Ritter, 1986), lower limb alignment (e.g., Qangle, tibial valgus, femoral anteversion, tibial rotation, pelvis width; Loudon, Jenkins, & Loudon, 1996; Moeller & Lamb, 1997), muscular strength and conditioning levels (Hutchinson & Ireland, 1995; Moeller & Lamb, 1997). neuromuscular performance characteristics (Huston & Wojtys, 1996; Nyland Shapiro, Caborn. Nitz, & Malone, 1997; Wojtys, Ashton-Miller, & Huston, 2002), hormonal influences (Liu, Al-Shaikh, Panossian, Finerman, & Lane, 1997; Slauterbeck, Clevenger, Lundberg, & Burchfield, 1999), and movement technique (Arnold, Coker, Heaton, Park, & Harris, 1979; Hewett, Stroupe, Nance, & Noyes, 1996). Movement technique is a complex factor, as it not only reflects many of the other preceding anatomical, physiological, and internal biomechanical characteristics, but it is also a function of volitional control and perceptual influences. It is probable that the injury differences among individuals are a result of a multifactorial interaction among several characteristics that might or might not be gender related, and differences in many of these characteristics manifest themselves as differences in movement technique.
Movement technique influences the characteristics (e.g., location, magnitude, direction, etc.) of loading of the knee joint and the ACL, specifically. The ACL is loaded in a complex manner, and the magnitude and location of stress on the anteromedial and posterolateral fiber bundles depends on knee position (Cabaud, 1983; Markolf, et al., 1995). Markolf et al. (1995) observed that the force imposed on the ACL is greater with the knee positioned near terminal extension, particularly when an internal torque or varus moment is added. Arnold et al. (1979) evaluated 361 patients with ACL injuries and noted that most tears occurred when the participants attempted to twist or turn with their involved knee positioned in extension and the involved foot fixed or twisted on impact with the ground. This injury mechanism commonly occurs during a basketball rebound or cutting maneuver. When the knee is positioned near full extension, the posterior fibers of the ACL are most taut (Cabaud, 1983). These fibers provide the principle resistance to hyperextension and can be most susceptible to injury while the knee is extended (Markolf, et al., 1995), especially under conditions of increased loading due to anterior shear or torsion. Moreover, Nigg (1985) demonstrated that peak impact forces produced while running are greater when the knee is positioned further in extension, presumably increasing the force or stress on internal knee structures such as the ACL. Together, these elements suggest that the ACL may be under greater load when the knee is extended, high ground reaction forces are exerted on the foot, and tibial torsion or anterior shear is present (Markolf et al., 1995).
Several investigators have examined technique characteristics related to gender and knee function throughout a cutting sequence or similar activity (e.g., Malinzak, Colby, Kirkendall, & Garrett, 1999; McLean, Neal, Myers, & Walters, 1999; Nyland et al., 1997). These investigators have suggested that specific injury mechanisms are equivocal, and results are often inconsistent among studies. For example, Malinzak and colleagues (1999) reported that female athletes performed cutting maneuvers with less knee flexion, more knee valgus, and less hip flexion than male athletes. McLean and colleagues (1999) reported that female participants performed cutting with more knee abduction but found no differences in flexion-extension or rotation variables. Relative to knee kinetics. McLean et al., (1999) reported that female participants exhibited greater knee abductor moments during cutting than male participants. Chappell, Yu, Kirkendall, and Garrett (2002) observed that female participants exhibited greater anterior tibial shear force during a rapid stop jump task than male participants, which is consistent with an earlier report of greater anterior knee shear force for female participants during vertical landing (James, 1997). Hewett and colleagues (1996) found ground reaction forces (GRF) to be significantly related to abduction-adduction moments at the knee during landing. Additionally, Dufek and Bates (1991) and Hewett et al. (1996) suggested that GRFs are directly related to joint forces and are believed to have an important influence on lower extremity injury. Few studies have reported GRF loading characteristics in conjunction with sagittal plane knee kinematics during cutting.
While male and female athletes both participate in sports involving sudden deceleration, landing, and cutting, female athletes are injured more frequently, suggesting they may respond to the demands of these activities differently. Because movement technique may-influence the force or stress on the ACL, any observed differences in technique could indicate differences in injury risk. Therefore, the purpose of this study was to test the hypothesis that female athletes perform cutting maneuvers using a technique more likely to place the ACL at risk of injury. Additionally, while injury incidence may generally differentiate male and female athletes, any individual (male or female) who exhibits movement techniques associated with greater ACL loading may be at greater risk for injury. Therefore, a second purpose was to examine the movement techniques of individual participants to determine whether women or men may be at greater risk of injury. It was hypothesized that (a) some male athletes would also exhibit movement techniques associated with greater ACL loading and injury risk, and (b) many female athletes would not exhibit these characteristics.
Method
Participants
Thirty-eight (19 men and 19 women) high school and collegiate basketball players with no prior history of ACL injury participated in the study. Participant characteristics for male athletes were: M age = 17.0 years, SD = 2.63, M mass = 73.2 kg, SD = 13.85, and M height = 1.82 m, SD =0.12. Female athlete characteristics were: M age = 17.7 years, SD = 2.31, M mass = 63.2 kg, SD= 10.12, and M height = 1.69 m, SD= 0.08. Of the 19 male athletes, 12 and 7 were high school and collegiate players, respectively. Of the 19 female athletes, 11 and 8 were high school and collegiate players, respectively. All individuals were healthy at the time of testing and performed without braces on the lower extremities. Participants were permitted to perform the procedures in their own court shoes. Written informed consent was obtained from each individual or legal guardian as stipulated by the institutional review board for the protection of human subjects at the affiliated university.
Procedures
Following a brief warm up (5 min on a cycle ergometer at a heart rate of 40% of estimated maximum), participants were prepared for data collection and then performed three–five practice sprint and cut attempts to establish starting position and foot placement. For the experimental cutting trials, each participant completed two maximum effort sprint and cut performances while dribbling a basketball with the right hand. Each consisted of a four–five step maximum effort sprint toward a force platform (Bertec, Model 4060A, Columbus, OH; 180 Hz), with the participant planting the right foot on the force platform and cutting at a 60° angle left of the initial progression line (i.e., side step cut). Participants received verbal encouragement to participate at maximum effort. A basketball court playing surface was simulated by mounting a parquet wood floor cutout on top of the force platform such that it was flush and level with the surrounding floor. The cutout was visible to participants and investigators, and participants performed all cutting trials on the force platform. Although potential alterations in GRF due to the floor surface were not investigated, it was assumed that any effects present were consistent for all individuals and did not influence the relative gender comparisons. During the cut, each participant was instructed to switch dribbling from the right to the left hand. Following the cut, each participant was required to continue dribbling the ball while sprinting four–five additional steps to complete a lay up shot with the left hand on a portable regulation height basketball goal.
Right side, three dimensional lower extremity kinematic data were obtained using a three-camera video tracking system (Motion Analysis, Inc., Expert Vision Software, Santa Rosa, CA; 180 Hz). The three cameras were positioned on the participant’s right side to obtain rear oblique, near sagittal, and front oblique views. To facilitate data capture and reduction, two centimeter diameter retroreflective spheres were fixed at the following anatomic sites to define the link system of the right lower extremity: fifth metatarsal head, lateral malleolus, lateral femoral condyle at the knee, and tip of the greater trochanter at the hip. An additional reference marker was fixed posterior to the lateral femoral condyle in the same horizontal plane but was not used in the current analysis. Two-dimensional raw coordinate data from three cameras were used to reconstruct the coordinates in three dimensions of the laboratory reference frame using a direct linear transformation algorithm provided by the software. The raw data were smoothed at a cutoff frequency of 6 Hz using a fourth-order zero lag low-pass digital filter.
The angle in space between the thigh and leg (i.e., knee) was determined by computing the scalar (dot) product of the vectors defining each segment in three dimensions (Anton, 1991). The vectors representing the leg and thigh segments were translated to the origin and used to compute the scalar product. Then, knee angle (θ) was calculated using the following formula:
where, V1 and V2 were the vectors for the leg and thigh segments containing the x, y, and z coordinates of the translated vector endpoints relative to the origin; |V1| and |V2| were the magnitudes of the vectors. The resulting angle was interpreted to represent combined flexion and abduction (positive values) of the leg relative to the thigh. It was assumed that frontal plane motion at the knee was small compared to the motion in the sagittal plane (e.g., approximately 140° maximum range of motion in the sagittal plane compared to just a few degrees in the frontal plane; Nordin & Frankel, 1989). Examining the combined movement was believed more representative of actual joint function than evaluating isolated flexion or abduction in their respective planes. Tibiofemoral rotation was not investigated.
Ground reaction force data were temporally synchronized to the kinematic data by visually identifying the frame number of the instant of foot contact (near sagittal view) with the force platform then temporally aligning this frame identifier to the first data sample of the initial rise in vertical GRF. Using the 180-Hz sampling frequency, the possible temporal error introduced by this manual synchronization method was estimated to be ± 0.006 s, which, if present, was deemed to have a negligible effect on the ground reaction force and kinematic variables chosen for analysis. Additionally, the potential positive or negative temporal error was assumed to be random among participants, thus minimizing any systematic bias for the group.
Data Analysis
The center of mass velocity at the instant of foot contact was estimated for all participants by computing the resultant linear velocity of the right hip marker for the frame immediately preceding foot contact with the force platform. This method was used to determine the average approach velocity for male (3.28 ± 0.42 m·s−1) and female athletes (3.09 ± 0.44 m·s−1), with a group range of 2.44–4.25 m·s−1.
Knee angle and GRF time histories were plotted, analyzed, and reduced to four dependent variables representing knee kinematic and GRF characteristics. Two kinematic variables selected for analysis were knee flexion at the instant of ground contact and knee range of motion during the support phase of die cutting sequence. Range of motion was defined as the angular displacement of the joint from the instant the foot contacted the ground to the maximum flexion angle of the knee during support. These two variables were chosen, because of the reported relationship between knee joint position and ACL loading (Cabaud, 1983; Markolf et al., 1995) as described previously. The two GRF variables were the peak resultant GRF magnitude during the support phase and the resultant GRF magnitude at maximum knee flexion. The resultant GRF was obtained by computing the vector sum of the three orthogonal GRF components. The GRF variables represented general loading of the lower extremity dining the cutting sequence. While GRF does not completely determine loading within the knee joint, greater GRF magnitudes are typically associated with greater moments and reaction forces at the knee (e.g., Hewett et al., 1996), presumably creating an environment within which the ACL could be exposed to greater loading. Actual ACL loading depends on a number of factors, such as muscular forces involved, other joint and capsular forces, line of action of the net external force, direction and amount of surface motion at the joint, and anthropometric characteristics. The peak resultant GRF variable was selected to quantify the maximum external loading occurring during the cutting sequence. The GRF at maximum knee flexion variable was chosen to represent loading at a common and transitional kinematic event during the support phase. Both GRF variables were normalized to the estimated running momentum, N· (kg·m·s−1)−1, at the instant of foot contact to facilitate grouping participant data from individuals of different masses and running velocities. This step was necessary, because participants were instructed to perform using maximal effort, and thus, running velocities were not explicitly controlled. Kinematic data were not normalized, because absolute position of knee flexion-extension was believed to be more closely related to ACL loading by the mechanism described by Cabaud (1983) and Markolf, et al. (1995).
A participant’s average performance was represented by the two trial mean for that individual and variable. Note that for 6 participants, 3 men and 3 women, one of the two trials was unusable, thus, information from the single good trial was used in place of the mean for those participants. While more than two trials would have been preferred to represent each participant’s performance over time, Bates, Dufek, and Davis (1992) demonstrated, using a Monte Carlo approach, that statistical power in a group design exceeded 90% for a model data set using as few as one trial per participant for sample sizes greater than 20. Hence, the use of only two trials was deemed acceptable, albeit not ideal, in the current investigation.
The four kinematic and GRF dependent variables were examined for multicollinearity and sphericity by generating a correlation matrix among the participant variables. Correlation coefficient values exceeding the range of −.707 < r < .707 with r ≠ 0 were interpreted to contain redundant information and excluded from subsequent analyses (Tabachnick and Fidell, 1989). On satisfying this condition, the dependent variables were used to evaluate the first hypothesis by comparing male and female athletes using a one-way multivariate analysis of variance (MANOVA), λ(4,33), α = .05. SPSS 2000, v. 10.0.1, and follow-up one-way analyses of variance (α = .05). In addition to determining the probability of statistical significance (p value), 95% confidence intervals, effect size, and statistical power were also computed for each variable. Evaluation of the second hypothesis was contingent on the results of the preceding analyses. A scatter plot was used to further examine variables found to significantly differentiate the male and female groups by participant. Individual participant scores, along with the group mean of all 38 participants and standard deviation values were computed and plotted for the identified variables. The region within the scatter plot that contained the most extreme scores relative to the group mean (origin) on the included variables was identified as a region of greatest potential risk. The group mean was defined as the plot origin to indicate the estimated population mean values of the included variables.
Results
Correlation results suggest that no dependent variables were excessively correlated with each other. All correlation values (see Table 1) fell within the acceptable range of −.707 < r < .707 with r ≠ 0; thus, all variables were retained for subsequent analyses. Example knee angle and nonnormalized resultant GRF data from one female participant are shown (see Figure 1).
Table 1.
Correlation matrix for dependent variables
| Knee flexion at contact | Knee ROM | Peak GRF | GRF at max knee flexion | |
|---|---|---|---|---|
| Knee flexion at contact | 1.000 | |||
| Knee ROM | −.324 | 1.000 | ||
| Peak GRF | −.218 | .099 | 1.000 | |
| GRF at max knee flexion | −.359 | .078 | .642 | 1.000 |
Note. Values are Pearson product-moment correlation coefficient (r) values; ROM = range of motion; GRF = ground reaction force.
Figure 1.
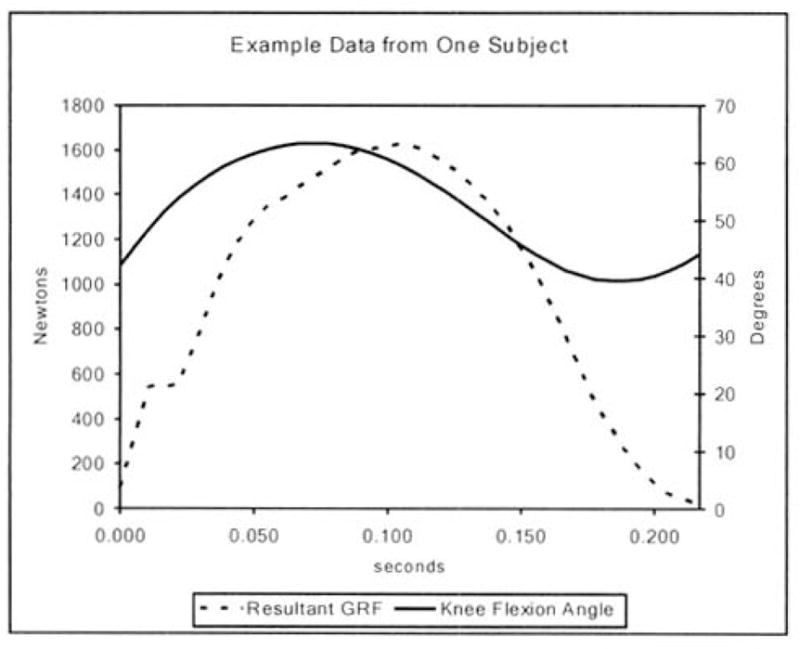
Example knee angle and nonnormalized resultant GRF data from one female participant (mass = 65 kg; hip marker resultant linear velocity at contact = 3.2 m/s).
Results of the group comparisons suggest that male and female athletes performed the cutting maneuver using different movement techniques (see Tables 2 and 3). MANOVA results revealed a significant (λ = 2.78, p = .043) difference between male and female athletes for the combined dependent variables. Follow-up comparisons revealed that female athletes exhibited 5.8° less knee flexion at contact (p ≤ .05) and 1.0 N·(kg·m·s−1) −1 greater GRF at maximum knee flexion (p ≤ .05) than male athletes (see Tables 2 and 3). Effect size and statistical power results associated with each comparison indicated that three of the four variables exhibited a moderate to high (≥ .50) effect size, and one variable demonstrated statistical power greater than 80%.
Table 2.
Summary of descriptive results.
| Variable | 95% CI lower limit | M | SD | 95% CI upper limit |
|---|---|---|---|---|
| Male athletes | ||||
| Knee flexion at contacta | 42.2 | 46.0 | 8.05 | 49.8 |
| Knee ROMa | 16.2 | 18.4 | 4.79 | 20.6 |
| Peak GRFb | 6.4 | 6.9 | 0.80 | 7.4 |
| GRF at max knee flexionb | 4.9 | 5.3 | 0.80 | 5.7 |
| Female athletes | ||||
| Knee flexion at contacta | 36.4 | 40.2 | 8.04 | 44.0 |
| Knee ROMa | 17.0 | 21.2 | 8.94 | 25.4 |
| Peak GRFb | 6.9 | 7.5 | 1.38 | 8.1 |
| GRF at max knee flexionb | 5.7 | 6.3 | 1.25 | 6.9 |
Note. CI = confidence interval; ROM = range of motion; GRF = ground reaction force.
Units for knee kinematic variables are degrees of flexion.
Units for GRF variables are N·(kg·m·s−1)−1; the GRF variables were normalized to resultant running momentum at foot contact.
Table 3.
Summary of follow up analysis of variance results comparing male and female athletes
| Variable | P(1,36) | p | Observed power (%) | Effect sizea |
|---|---|---|---|---|
| Knee flexion at contact | 4.90 | .033 | 58 | .72 |
| Knee ROM | 1.74 | .196 | 25 | .39 |
| Peak GRF | 299 | .092 | 39 | .50 |
| GRF at max knee flexion | 8.82 | .005 | 82 | .95 |
Note. ROM = range of motion; GRF = ground reaction force.
Effect size = (M1 − M2)/SDp; where M1 and M2 are the mean values for male and female athletes, respectively, and SDp is the pooled standard deviation.
Participant groupings within the scatter plot suggest that 10 participants in the current sample may have been at greater risk of injury than the others (see Figure 2; Region IV) based on the observed variables. A simple count of participants by region indicates that 16, 42, 16, and 26% of participants clustered in regions I, II, III, and IV, respectively. Region I consisted of 3 male and 3 female athletes. Region II contained 10 male and 6 female athletes. Region III comprised 5 and 1 male and female athletes, respectively. Region IV contained 1 male athlete and 9 female athletes. Region IV represents performances in which less knee flexion at contact was accompanied by greater GRF at maximum knee flexion. This region was thought to be the most dangerous combination of GRF and knee angle responses.
Figure 2.
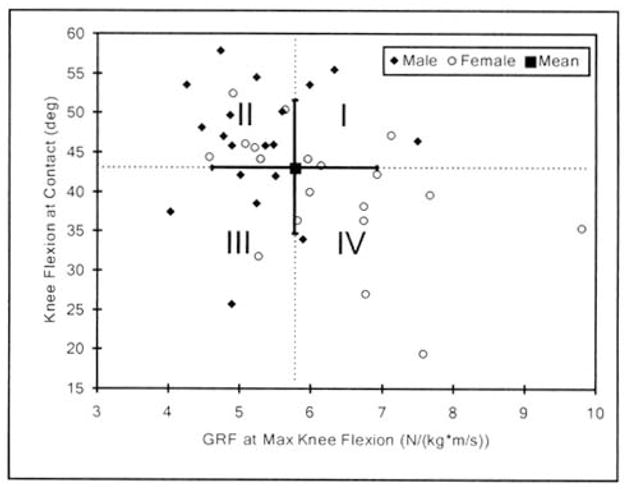
Scatter plot demonstrating the relationship between the knee flexion at contact and GRF at maximum knee flexion variables. Four regions were defined based on the location of the group mean and standard deviation bars. Regions I and IV represent performances with greater magnitudes of ground reaction force (GRF) at maximum knee flexion for greater and lesser values of knee flexion at contact, respectively. Regions II and III represent performances involving less GRF at maximum knee flexion for greater and lesser values of knee flexion at contact, respectively. Individuals falling within Region IV are believed to be at a greater risk of injury compared to individuals in other regions.
Discussion
Female athletes experience ACL injuries more frequently than male athletes in similar sports (Arendt & Dick, 1995; Dehaven & Lintner, 1986; Huston & Wojtys, 1996;Zelisko et al., 1982). Many anatomical, physiological, and biomechanical characteristics have been suggested to play a role in the injury differences, but a growing body of evidence supports the importance of movement technique, such as lower extremity alignment during critical phases of loading (Arnold et al., 1979; Feagin et al., 1987; Kirkendall & Garrett, 2000; Markolf et al., 1995).
The first hypothesis that female athletes would perform the cutting maneuver using a technique more likely to place the ACL at greater risk of injury was supported. Kinematic results indicated that the female athletes initiated the cutting sequence in a position of less knee flexion (5.8° less) but exhibited 3.5° greater range of motion (ROM) during the support phase. The knee flexion at contact result was in agreement with a previous study (Malinzak et al., 1999) that reported female athletes initiated a similar cutting activity with 5.2° greater knee extension at contact. Landing in a position of greater knee extension at contact, if concurrent with tibial torsion or anterior shear, could stress the ACL by the mechanism described by Markolf et al., (1995). Although tibial torsion and anterior shear were not examined, for similar values of torsion or shear in the current study female athletes would be at greater risk of ACL injury due to the additional loading created by the mechanism of greater knee extension.
Although no statistical difference was found between male and female athletes for the ROM variable, the observed 3.5° difference may have been meaningful due to the direction tendency of the effect and the low-to-moderate effect size (.39; see Table 2). The difference suggests that female athletes performed the cutting maneuver using a slightly greater ROM. The greater ROM could reflect a difference in joint control (e.g., stiffness, coordination) during the loading phase or differences in extensor muscle strength (hip or knee). These speculations are supported by the observation that the relative ROM difference is maintained even after normalizing to body mass and running velocity—0.079 ± 0.027 and 0.1134 ± 0.054 deg·(kg·m·s−1)−1 for male and female athletes, respectively—thus minimizing any mass or speed effects. However, although female athletes exhibited slightly greater ROM values during the cutting maneuver, they initiated and ended the ROM sequence in a position of greater knee extension. Male and female athletes differed in knee flexion at contact, as described previously, but they also differed in their values of maximum knee flexion. The values for maximum knee flexion were 64.1 ± 9.1 and 61.4 ± 9.3° for male and female athletes, respectively, suggesting a tendency for the female athletes to maintain a more extended knee position throughout the loading phase of the cut. Together, the kinematic variables suggest that female athletes may land in and maintain a more extended knee position during the loading phase of the cutting sequence and might control sagittal plane knee joint motion differently from male athletes.
GRF results further supported the first hypothesis. Both peak GRF and GRF at maximum knee flexion, when normalized to running momentum, were greater for female athletes, with the latter variable statistically different between the two groups and the former variable exhibiting a moderate effect size (.50; see Table 2). Because the greater GRF at maximum knee flexion value for female athletes could not be attributed to either body mass or running velocity, the difference must be attributed to cutting technique (e.g., knee kinematics) or other unmeasured factors. The GRF results suggest that female athletes experienced greater lower extremity loading during the cutting maneuver and that this occurred with a more extended knee, potentially increasing force or stress on the ACL.
The second hypothesis—that some male athletes would also exhibit movement techniques associated with greater ACL loading and injury risk and many female athletes would not exhibit these characteristics—was supported. While the data presented by group (see Table 2) suggest that male and female athletes were statistically different for two of the examined variables, not all individuals performed as suggested by their group association. Because less knee flexion at foot contact and greater GRF at maximum knee flexion may be independently related to greater force or stress on the ACL by the mechanisms described previously (e.g., Cabaud, 1983; Hewett et al., 1996; Markolf et al., 1995; Nigg, 1985), individuals who exhibit both characteristics simultaneously could be considered at greatest risk of injury. Individuals whose performances placed them in Region IV of Figure 2 exhibited these characteristics, thus suggesting that these individuals could be at greatest risk. Of the 10 participants whose performances fell within Region IV, there were 9 women and 1 man. With this information, these individuals could receive specific training to avoid continued high risk behaviors. This observation suggests that main gender-based studies of injury mechanisms may oversimplify the problem and the focus should shift to the physiological, structural, or functional characteristics thought to result in injury (Sizer, James, & Schot, 2000).
Methods for altering similar technique characteristics have been studied relative to the ability to prevent ACL injury (Caraffa et al., 1996; Hewett et al., 1996; Hewett et al., 1999). In a prospective controlled study of semiprofessional male soccer players. Caraffa et al. (1996) observed more than a sevenfold decrease in expected ACL injury with proprioceptive training. Hewett et al. (1996) used a jump training program to affect lower extremity strength and landing mechanics in female soccer, volleyball, and basketball players. They noted a 22% decrease in ground reaction force and an increase in maximum knee flexion at landing after 6 weeks of training. A subsequent report (Hewett, et al., 1999) noted a significant decrease in the expected rates of serious knee injuries in the female athletes who underwent this training. The advent and systematic implementation of such programs could ultimately decrease the health costs and debilitating effects of ACL injuries in female and male athletes at all levels of athletic participation.
In conclusion, results of this study suggest that, on average, female athletes may land in a position of less knee flexion and experience greater GRF magnitudes at maximum knee flexion than male athletes during the cutting sequence. Additionally, individual female or male athletes who exhibit similar characteristics might be at greater risk of ACL injury.
Acknowledgments
The authors would like to thank Gina Fick, Felix Guerra, Tracy Paxton, and Jason Sims for their contributions to the literature review, participant recruitment, and data collection.
Contributor Information
C. Roger James, Department of Health, Exercise, and Sport Sciences at Texas Tech University.
Phillip S. Sizer, Department of Rehabilitation Sciences at Texas Tech University Health Sciences
David W. Starch, Department of Orthopedics at Texas Tech University Medical Center
Thurmon E. Lockhart, Grado Department of Industrial and Systems Engineering at Virginia Polytechnic Institute and State University
James Slauterbeck, Department of Orthopedics at Texas Tech University Medical Center.
References
- Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB. Analysis of the intercondylar notch by computed tomography. American Journal of Sports Medicine. 1987;15:547–552. doi: 10.1177/036354658701500605. [DOI] [PubMed] [Google Scholar]
- Anton H. Elementary linear algebra. New York: John Wiley & Sons. Inc; 1991. [Google Scholar]
- Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. American Journal of Sports Medicine. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- Arnold J, Coker T, Heaton L, Park JP, Harris WD. Natural history of anterior cruciate tears. American Journal of Sports Medicine. 1979;7:305–313. doi: 10.1177/036354657900700601. [DOI] [PubMed] [Google Scholar]
- Bates BT, Dufek JS, Davis HP. The effect of trial size on statistical power. Medicine and Science in Sports and Exercise. 1992;24:1059–1068. [PubMed] [Google Scholar]
- Cabaud HE. Biomechanics of the anterior cruciate ligament. Clinical Orthopaedics and Related Research. 1983;172:26–31. [PubMed] [Google Scholar]
- Caraffa A, Cerulli G, Projetti M, Aisa G, Rizzo A. Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 1996;4:19–21. doi: 10.1007/BF01565992. [DOI] [PubMed] [Google Scholar]
- Chappell JD, Yu B, Kirkendall DT, Garrett WE. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. American Journal of Sports Medicine. 2002;30:261–267. doi: 10.1177/03635465020300021901. [DOI] [PubMed] [Google Scholar]
- Dehaven K, Lintner D. Athletic injuries: Comparison by age, spoil and gender. American Journal of Sports Medicine. 1986;14:218–224. doi: 10.1177/036354658601400307. [DOI] [PubMed] [Google Scholar]
- Dufek JS, Bates BT. Biomechanical factors associated with injury during landing in jump sports. Sports Medicine. 1991;12:326–337. doi: 10.2165/00007256-199112050-00005. [DOI] [PubMed] [Google Scholar]
- Feagin JA, Lambert KL, Cunningham RR, Anderson LM, Reigel J, King PH, VanGenderen L. Consideration of anterior cruciate ligament injury in skiing. Clinical Orthopaedics and Related Research. 1987;216:3–18. [PubMed] [Google Scholar]
- Gray J, Taunton JE, McKenzie DC, Clement DB, McConkey JP, Davidson RG. A survey of injuries to the anterior cruciate ligament of the knee in female basketball players. International Journal of Sports Medicine. 1985;6:314–316. doi: 10.1055/s-2008-1025861. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Linderfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: A prospective study. American Journal of Sports Medicine. 1999;27:699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. American Journal of Sports Medicine. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- Huston LJ, Wojtys EM. Neuromuscular performance characteristics in elite female athletes. American Journal of Sports Medicine. 1996;24:427–436. doi: 10.1177/036354659602400405. [DOI] [PubMed] [Google Scholar]
- Hutchinson MR, Ireland ML. Knee injuries in female athletes. Sports Medicine. 1995;19:288–302. doi: 10.2165/00007256-199519040-00006. [DOI] [PubMed] [Google Scholar]
- James CR. Effects of gender and landing height on lower extremity forces during landing. Medicine & Science in Sports & Exercise. 1997;29(Suppl):1334. [Google Scholar]
- Kirkendall D, Garrett WK. The anterior cruciate ligament enigma: Injury mechanisms and prevention. Clinical Orthopaedics and Related Research. 2000;372:64–68. doi: 10.1097/00003086-200003000-00008. [DOI] [PubMed] [Google Scholar]
- LaPrade RF, Burnett QM. Femoral intercondylar notch stenosis and correlation to anterior cruciate ligament injuries. A prospective study. American Journal of Sports Medicine. 1994;22:198–202. doi: 10.1177/036354659402200208. [DOI] [PubMed] [Google Scholar]
- Liu SH, Al-Shaikh RA, Panossian V, Finerman GA, Lane JM. Estrogen affects the cellular metabolism of the anterior cruciate ligament. A potential explanation for female athletic injury. American Journal of Sports Medicine. 1997;25:704–709. doi: 10.1177/036354659702500521. [DOI] [PubMed] [Google Scholar]
- Loudon JK, Jenkins W, Loundon KL. The relationship between static posture and ACL injury in female athletes. Journal of Orthopedic and Sports Physical Therapy. 1996;24:91–97. doi: 10.2519/jospt.1996.24.2.91. [DOI] [PubMed] [Google Scholar]
- Malinzak R, Colby S, Kirkendall D, Garrett WE. Electromyograph and 3-dimensional kinematic analysis of cutting maneuvers in men and women: Implications for anterior cruciate ligament injury [Abstract #36] Proceedings of the American Academy of Orthopaedic Surgeons, USA. 1999;66:12. [Google Scholar]
- Markolf K, Burchfield D, Shapiro M, Shepard MF, Finerman GA, Slauterbeck JL. Combined knee loading states that generate high anterior cruciate ligament forces. Journal of Orthopaedic Research. 1995;13:930–935. doi: 10.1002/jor.1100130618. [DOI] [PubMed] [Google Scholar]
- McLean SG, Neal RJ, Myers PT, Walters MR. Knee joint kinematics during sidestep cutting maneuver: potential for injury in women. Medicine & Science in Sports & Exercise. 1999;31:959–968. doi: 10.1097/00005768-199907000-00007. [DOI] [PubMed] [Google Scholar]
- Moeller JL, Lamb MM. Anterior cruciate ligament injuries in female athletes. Why are women more susceptible? Physician and Sportsmedicine. 1997;25:31–54. doi: 10.3810/psm.1997.04.1272. [DOI] [PubMed] [Google Scholar]
- Nigg BM. Biomechanics, load analysis and sports injuries in the lower extremities. Sports Medicine. 1985;2:367–379. doi: 10.2165/00007256-198502050-00005. [DOI] [PubMed] [Google Scholar]
- Nordin M, Frankel VH. Biomechanics of the knee. In: Nordin M, Frankel VH, editors. Basic biomechanics of the musculoskeletal system. Philadelphia: Lea & Febiger; 1989. pp. 115–134. [Google Scholar]
- Nyland JA, Shapiro R, Caborn DN, Nitz AJ, Malone TR. The effect of quadriceps femoris, hamstring, and placebo eccentric fatigue on knee and ankle dynamics during crossover cutting. Journal of Orthopedic and Sports Physical Therapy. 1997;25:171–184. doi: 10.2519/jospt.1997.25.3.171. [DOI] [PubMed] [Google Scholar]
- Sizer PS, James CR, Schot PK. ACL injury risk goes beyond gender. Biomechanics. 2000;7(10):45–46. [Google Scholar]
- Slauterbeck JR, Clevenger C, Lundberg W, Burchfield DM. Estrogen level alters the failure load of the rabbit anterior cruciate ligament. Journal of Orthopedic Research. 1999;17:405–408. doi: 10.1002/jor.1100170316. [DOI] [PubMed] [Google Scholar]
- Souryal TO, Freeman TR. Intercondylar notch size and anterior cruciate ligament injuries in athletes. A prospective study. American Journal of Sports Medicine. 1993;21:535–539. doi: 10.1177/036354659302100410. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. New York: Harper Collins Publishers; 1989. [Google Scholar]
- Weesner CL, Albohm MJ, Ritter MA. A comparison of anterior and posterior cruciate ligament laxity between female and male basketball players. Physician and Sportsmedicine. 1986;14:149–154. doi: 10.1080/00913847.1986.11709076. [DOI] [PubMed] [Google Scholar]
- Wojtys EM, Ashton-Miller JA, Huston LJ. A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. Journal of Bone and Joint Surgery. 2002;84-A(1):10–16. doi: 10.2106/00004623-200201000-00002. [DOI] [PubMed] [Google Scholar]
- Zelisko JA, Noble HB, Porter M. A comparison of men’s and women’s professional basketball injuries. American Journal of Sports Medicine. 1982;10:297–299. doi: 10.1177/036354658201000507. [DOI] [PubMed] [Google Scholar]