

Abstract
Background:
The purpose of this study was to evaluate the effect of altering the use of the protocol for brain death determination in traumatically injured patients, on time to brain death determination, medical complication rates, organ procurement rates and charges for care rendered during brain death determination. A retrospective chart review of trauma patients with lethal brain injuries at an urban tertiary care trauma center was performed. Two groups of trauma patients with lethal head injuries were compared. Group I consisted of patients pronounced brain dead using a protocol requiring two brain examinations, and group II contained patients evaluated using a protocol requiring one brain examination in conjunction with a nuclear medicine brain flow scan.
Results:
Group II had a significantly (P < 0.01) shorter mean brain death stay (3.5 ± 1.8 h) than group I (12.0 ± 1.0 h). Patients in groups I and II developed a similar number of medical complications, 3.2 ± 0.2 and 4.0 ± 1.3, respectively. The number of organs procured per patient did not differ significantly (4.1 ± 0.2 for group I and 4.4 ± 1.4 for group II). There was a significant (P < 0.01) decrease in the brain death stay charges for group II ($6125 ± 1100) compared to group I ($16,645 ± 1223).
Conclusions:
Medical complications are universal in the traumatized patient awaiting the determination of brain death. These complications necessitate aggressive and costly care in the intensive care unit in order to optimize organ function in preparation for possible transplantation. In our institution, the determination of brain death using a single clinical examination and a nuclear medicine flow study significantly shortened the brain death stay and reduced associated charges accrued during this period. The complication and organ procurement rates were not affected in this small, preliminary report sample.
Keywords: brain death, cerebral blood flow, organ donor, traumatic brain injury
Introduction
Between 1990 and 1995, the organ transplant waiting list in the US more than doubled to over 43,000 patients [1]. The donor pool necessary to meet current US transplantation needs has been projected to between 10,000 and 15,000 per year [2,3]. The major obstacle to organ transplantation is the limited organ supply [2,4]. Consequently, in the early 1990s, nearly 2000 patients died in the US each year while on organ transplantation waiting lists [5]; currently, this number may be as high as 3500 [1]. It has been estimated that between 12,500 and 27,000 potential organ donors die each year in the US [2,6]. Despite what seems to be an adequate donor pool, only 15 to 20% of potential donors become actual donors, approximately 98% of whom originate from intensive care units (ICUs) [7,8]. Because many factors contribute to the shortage of organs, early donor recognition, rapid and accurate declaration of brain death, physiological maintenance of potential organ donors, and coordination with the local organ procurement organization (OPO) are all important aspects of organ donor management [9].
Once a potential donor has been identified, brain death must be legally determined [10,11]. The multiple physiological derangements which the potential organ donor manifests require aggressive, labor intensive management in order to maintain organ function until legal brain death is declared and procurement can be undertaken [12]. One recent review suggests that the medical failures occurring prior to organ procurement in brain dead patients may be largely preventable by the use of invasive hemodynamic monitoring, aggressive rewarming and liberal transfusion therapy [13]. The level of care necessary to sustain potential organ donors until legal brain death is declared is expensive [14]. These charges, accrued before the OPO assumes financial responsibility, may be unknowingly referred to donor families, essentially penalizing them for the altruistic act of organ donation.
This review was performed in order to measure the impact of altering the use of the brain death determination protocol at the University of Pennsylvania Medical Center, in an attempt to decrease the time between the first examination consistent with brain death and actual legal determination of brain death (brain death stay). The impact on the organ procurement process, including hospital charges, length of brain death stay, and number of organs procured per patient was studied.
Materials and methods
With cooperation from the Delaware Valley Transplant Program, the local OPO, traumatically injured organ and tissue donors cared for between 1 July 1991 and 31 December 1996 at the University of Pennsylvania Medical Center (an urban Level 1 trauma center) were identified. Two groups of trauma patients were studied: group I consisted of 31 patients evaluated between 1 July 1991 and 30 June 1995, and group II consisted of seven patients evaluated between 1 January and 31 December 1996. The OPO and hospital medical records for these patients were reviewed. Demographic information, including age, sex and mechanism of injury was abstracted. In addition, the timing of specific diagnostic studies and therapies such as laboratory tests, radiographs, medications, and transfusions were recorded for concurrent financial analysis with charges obtained from itemized hospital billing sheets.
The presence or absence of specific major medical complications during the hospital stay was determined by medical record review. Clinical complications, based on a chart review of specific interventions by clinicians caring for these patients rather than on strict predefined criteria, were defined as:
1. cardiovascular instability — blood pressure support with a vasopressor;
2. cardiovascular instability — invasive hemodynamic monitoring with a Swan Ganz catheter;
3. anemia — transfusion of packed red blood cells (PRBC);
4. coagulopathy — transfusion of fresh frozen plasma (FFP) or platelets (PLTS), and
5. diabetes insipidus (DI) — treatment with vasopressin infusion.
Because of their depressed neurological status, all patients were maintained on mechanical ventilation. Therefore, pulmonary complications were not thought to add differently to charges between groups, and the incidence of respiratory insufficiency was not calculated.
At the University of Pennsylvania, brain death is basically defined by:
1. two neurological examinations demonstrating lack of cortical and brainstem function, performed 12 h apart;
2. two neurological examinations performed 6 h apart along with a confirmatory electroencephalogram documenting lack of cortical function, or
3. a single brain death examination demonstrating a lack of cortical and brainstem function in conjunction with a confirmatory nuclear medicine brain flow scan demonstrating absence of cerebral blood flow.
Until January 1996, brain death was typically determined using one of the first two methods described above. The third option was reserved for patients with equivocal examinations due to confounding factors (pentobarbital, etc). In order to speed the determination of brain death and potentially reduce costly ICU stays, beginning in January 1996 the brain flow scan became the primary method of confirming brain death in our trauma patient population.
The nuclear medicine brain flow scan is performed by intravenous injection of 20–25 mCi of either 99mTc labeled HMPAO or ECD followed 25–30 min later by conventional lateral planar imaging of the patient's head using a scintillation camera interfaced to a digital computer. These scans are performed in the radiology department without moving the patient from the bed to a scanning table, thus facilitating timely acquisition of the necessary images. The images are then interpreted by on-screen visual inspection, allowing optimal evaluation of the degree of blood flow to the brain. Under normal circumstances, a substantial uptake of the aforementioned radio tracers is noted in the brain and cerebellum (Fig 1). In patients with brain death, no detectable uptake is noted. In fact, uptake in the scalp and skull, which is not typically seen in images from normal patients, appears quite prominent in those with brain death, allowing definition of the contours of the head in such subjects (Fig 2).
Figure 1.
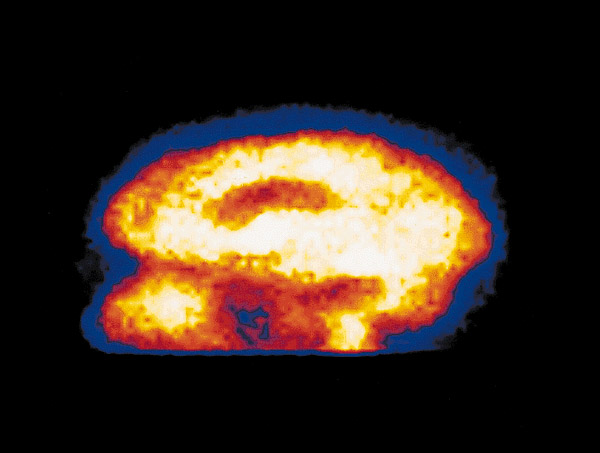
A nuclear medicine cerebral blood flow scan of a normal human brain from a lateral view, showing flow (light shades) to the cerebrum and cerebellum.
Figure 2.
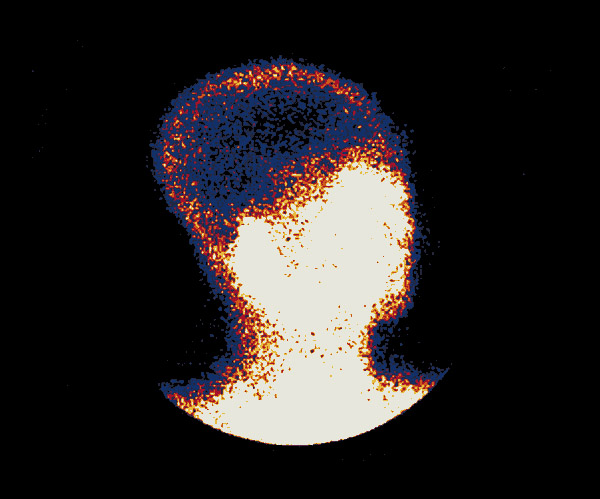
Oblique whole-head view of a nuclear medicine study showing no cerebral blood flow, consistent with brain death. Note the presence of soft tissue blood flow (light shades) and lack of cerebral blood flow (black area).
For each patient in group I, the specific timing of the first and second brain death examinations was recorded. Likewise, for each patient in group II, the specific timing of the brain death examination and nuclear medicine scan result, coinciding with official declaration of death, was recorded.
The brain death stay was determined for each patient. Because OPOs assume patient management responsibility upon declaration of death, individual clinicians have no influence over events after this time. Therefore, no attempt was made to quantify the period between declaration of death and organ procurement, or to identify complications developed during this time. Itemized financial records of all patients were reviewed concurrently with their medical records. The timing of diagnostic and therapeutic maneuvers, including the nuclear medicine scan, was cross-referenced with the patient's itemized hospital bill. Individual item charges were then credited to the specific brain death stay period as described above. Of note, charges associated with diagnostic studies which were part of the donor evaluation process (eg echocardiography, hepatitis serology) and were specifically ordered by, and therefore billed to, the OPO during and after the brain death stay were not credited against the patient as brain death stay charges. All data are displayed as mean ± standard error of the mean. Statistical analysis was performed using the Mann–Whitney U test.
Results
Thirty-one organ and/or tissue donors were identified in group I and seven in group II. Demographic data are displayed in Table 1. Reflecting the urban trauma population, donors were most commonly young, African-American males who had sustained a gunshot wound to the head. In group I, 28 patients were declared brain dead and went on to donate 4.1 ± 0.2 organs/ donor. Three patients died in the ICU prior to brain death determination and became tissue donors. These three patients did not reach their second brain death examination and were therefore excluded from further consideration in the brain death stay group. In group II, all seven patients were declared brain dead using the modified protocol and went on to donate 4.4 ± 1.4 organs/donor.
Table 1.
Donor demographics
| Group I | Group II | |
| Number of patients | 28 | 7 |
| Age (years) | 28 ± 3 | 33 ± 5 |
| Sex | ||
| Male | 22 (71%) | 6 (86%) |
| Female | 9 (29%) | 1 (14%) |
| Race | ||
| African-American | 19 (61%) | 5 (71%) |
| White | 11 (35%) | 2 (29%) |
| Other | 1 (4%) | 0 (0%) |
| Mechanism of injury | ||
| Penetrating | 20 (65%) | 4 (57%) |
| Blunt | 11 (35%) | 3 (43%) |
Major medical complications during the hospital course were reviewed. Every study patient developed one or more major complication. Hypotension requiring intervention with one or more vasopressor agents was the most common of these complications. The hematologic complications of anemia and coagulopathy requiring blood component therapy with PRBCs, FFP or PLTS were also frequently noted (Table 2). The mean number of complications per patient was 3.2 ± 0.2 in group I, and 4.0 ± 1.3 in group II. The difference was not statistically significant (Table 3).
Table 2.
Major medical complications
| Medical complication | Intervention | No of group I | No of group II |
| patients affected (%) | patients affected (%) | ||
| Cardiovascular instability | Vasopressor | 27 (87) | 5 (71) |
| Cardiovascular instability | Swan Ganz | 9 (29) | 5 (71) |
| Anemia | PRBC | 25 (81) | 6 (86) |
| Coagulopathy | FFP/PLTS | 22 (71) | 7 (100) |
| Diabetes insipidus | Vasopressin | 14 (45) | 5 (71) |
Table 3.
Effect of rapid brain death protocol implementation
| Medical complications | Solid organs procured | Brain death | Brain death | |
| per patient* | per patient | stay (h) | charges ($) | |
| Group I | 3.2 ± 0.2 | 4.1 ± 0.2 | 12.0 ± 1.0 | 16,645 ± 1223 |
| Group II | 4.0 ± 1.3 | 4.4 ± 1.4 | 3.5 ± 1.8 | 6125 ± 1100 |
*Diabetes insipidus, anemia, coagulopathy, hemodynamic instability.
The mean brain death stay for each group was calculated, and was 12.0 ± 1.0 h for group I, and 3.5 ± 1.8 h for group II. The mean brain death stay for group II was significantly shorter (P < 0.01) (Table 3).
Itemized financial records of all 35 study patients were reviewed. Charges for ICU stay as well as specific diagnostic studies and therapeutic maneuvers were identified. These charges were cross-referenced with the patients medical records and individual charges were credited to specific periods before, during and after the brain death stay period. Mean charges accrued during the brain death stay were $16,645 ± 1223 for group I and $6125 ± 1100 for group II, which was significantly less (P < 0.01) (Table 3).
Discussion
Throughout the world, the shortage of donor organs has reached critical proportions. Despite efforts to increase the national supply, the number of patients dying in the US while awaiting solid organ transplantation has risen from six per day at the start of the study period, to 10 per day currently [1,5]. Attempts to increase referrals to OPOs by enacting mandatory request laws have had minimal impact on organ donation rates [15]. Once a potential organ donor is referred to an OPO, the failure to obtain consent from the next of kin remains the single largest cause of eligible organ procurement failure, with more than 40% of families refusing donation [13,16,17].
Since 1990, firearms have surpassed motor vehicle crashes as the single largest cause of lethal traumatic brain injury in the US [18]. This trend is consistent with our findings (Table 1). Unfortunately, the individuals most likely to be involved in inter-personal firearm violence seem to come from families less likely to agree to organ donation when compared to the general population [19,20]. Multiple efforts to educate the population at large on the societal benefits of organ donation are underway but the impetus to donate remains one based largely on altruism.
From initial hospitalization until organ procurement or cessation of life support, the potential organ donor manifests daunting medical challenges due to the dramatic physiological changes that accompany the development of brain death. The principle goals of medical management of the organ donor include early recognition and treatment of hemodynamic instability, maintenance of systemic perfusion pressure to maximize post-transplantation allograft function, and the prevention and treatment of other complications related to brain death and supportive care. Ideally, medical management of the potential multi-organ donor begins once it seems that brain death is inevitable and that the likelihood of donation by the family is high [9].
Major medical complications were universal in this study population. Every patient developed at least one complication. Hypotension requiring treatment with vasopressors and/or invasive hemodynamic monitoring was the most frequent complication. Hematologic abnormalities requiring blood component transfusion were also seen in over 80% of the patients. Additional complications, such as DI were also common (Table 2). These results are consistent with other studies which have reported similar complication rates during the brain death stay period [21,22,23]. Of note; the incidence of coagulopathy reported in our series is higher than that reported in the general organ donor population [21,23]. This is most likely explained by the nature of the lethal brain insult in our trauma population.
Unfortunately, 17–25% of potential organ donors are lost due to medical failure [13,16]. Complications related to prolonged supportive care, as a consequence of delays in the diagnosis of brain death, reduce the availability and suitability of potentially transplantable organs [24,25]. One recent review suggests that the medical failures occurring during the time leading up to actual organ procurement in brain dead patients may be preventable with early invasive hemodynamic monitoring, aggressive rewarming and liberal transfusion therapy, all readily available in a modern critical care setting [13]. This aggressive management, which is necessary to maintain organ function until brain death is declared and procurement can be undertaken, is extremely labor and resource intensive [13,16,21,22,23,26]. As a result, significant costs are accrued and charges generated while awaiting the declaration of brain death. A rapid, accurate diagnosis of brain death would seem to facilitate the organ procurement process and may well decrease its associated charges [27].
In this study, the mean charge for total hospital stay included charges accrued during initial evaluation in the trauma resuscitation area, during the ICU stay and during actual organ procurement. All charges accrued after the patient was declared legally brain dead, and charges for diagnostic studies specifically ordered by the OPO during the brain death stay as a part of the donor evaluation process, were the responsibility of the local OPO as per national standards (Hawthorne RV, pers comm). Charges accrued before the legal determination of brain death were not billed to the local OPO. In this study these included $16,645 ± 1223 in patient charges during the brain death stay in group I and $6125 ± 1100 in group II (Table 3). Group II charges include the additional fees for the nuclear medicine brain scan (charges for nuclear tracer, the scan itself and professional fees for interpretation of the scan), totaling nearly $1500. Therefore, the true difference in ICU-related charges is even more significant.
The legal definition of brain death may vary between different institutions and states [11,28]. At the Hospital of the University of Pennsylvania, brain death confirmation is basically defined by the three protocols mentioned previously. The third method, that of using a cerebral blood flow scan (a technique which was previously ordered rather infrequently at our institution) in conjunction with only one brain death examination, dramatically shortens brain death stay. Therefore, we are currently using this method in order to minimize brain death stay and maximize organ procurement possibilities; nuclear medicine scans can be performed quite expeditiously at our institution. In most cases, the criteria for brain death determination by nuclear scan are clear cut, allowing a decision to be made without equivocation. The brain scan technique, as previously described, is noninvasive, usually requiring only a venous access line to adminster the radio tracer [34]. There are no known side-effects of such preparations and therefore organs of interest for transplantation, such as the kidney, liver, heart, lungs and pancreas, are not affected by performing this type of examination. The results of the scan are available within 30 min of radio tracer injection and the technique can be performed at the bedside with portable nuclear medicine cameras, although these are currently unavailable at our institution [27]. While cerebral arteriography can be used for the same purposes, it is generally more costly and time consuming than the nuclear scan [30,32]. Overall, the nuclear scan leads to a decrease in associated charges and is safe, fast and accurate [31]. It has become the method of choice to determine brain death in our trauma population.
An additional potential benefit of rapid brain death determination is the reduction in time for the development of significant end organ dysfunction, thereby increasing the number of organs procured per donor. This may be offset by the possibility that procurement rates may fall if families do not have enough time to grieve, and may therefore be more prone to refuse organ donation. Both of these factors merit further investigation.
We specifically examined institutional charges and not costs associated with the care of the potential organ donor. Charges are billed by health care providers and, therefore, have the advantage of being specific to an individual procedure and relatively easy to obtain [35]. Examining charges appears to be somewhat misleading because for any one given resource they seem to bear little relationship to the cost, and are also widely variable between institutions [36]. However, charges are typically related to costs in a proportional sense and are therefore useful in measuring relative resource consumption [35]. In addition, because this study addresses issues pertinent to health care utilizers (the families of potential organ donors), as well as to health care providers, we felt that the examination of charges rather than costs was relevant.
This study has several obvious shortcomings — its small sample size, its retrospective and descriptive nature, and the fact that only institutional charges (as opposed to cost data) are examined. Also, we did not attempt to identify the ultimate bearer of financial responsibility for these charges. However, this study does point out that a large cost of care accumulates and is passed on to someone (tax-payer, insurance company or family) in the process of supporting organs for transplantation. At the institutional level, brain death protocols should be designed to shorten brain death stays as much as possible. At our institution, the nuclear medicine cerebral blood flow scan appears to fulfill this goal successfully. As a result, we have significantly by minimized charges associated with the determination of brain death, regardless of who ultimately subsidizes the process.
References
- UNOS 1996 Annual Report: http:www.unos.orgunos_ar_97tab_cont.htm
- Stuart FP. Need, supply and legal issues related to organ transplantation in the United States. Transplant Proc. 1984;16:87–94. [Google Scholar]
- Evans RW, Manninen DL, Garrison LP, et al. Donor availability as the primary determinant of the future of heart transplantation. JAMA. 1986;255:1892–1898. [PubMed] [Google Scholar]
- Merz B. The organ procurement problem: many causes, no easy solutions. JAMA. 1985;254:3285–3288. [PubMed] [Google Scholar]
- Peters TG. Life or death: the issue of payment in cadaveric organ donation. JAMA. 1991;265:1302–1305. doi: 10.1001/jama.265.10.1302. [DOI] [PubMed] [Google Scholar]
- Broznick BA. Organ procurement: fulfilling a need. . Transplant Proc. 1988;20(suppl 1):1010. [Google Scholar]
- Bart KJ, Macon EJ, Humphries AL, et al. Increasing the supply of cadaveric kidneys for transplantation. Transplantation . 1981;31:383–387. doi: 10.1097/00007890-198105010-00016. [DOI] [PubMed] [Google Scholar]
- Tolle SW, Bennett WM, Hickam DH, Benson JA. Responsibilities of primary physicians in organ donation. Ann Intern Med. 1987;106:740–744. doi: 10.7326/0003-4819-106-5-740. [DOI] [PubMed] [Google Scholar]
- Darby JM, Stein K, Grenvik A, Stuart S. Approach to management of the heartbeating brain dead organ donor. JAMA. 1989;261:2222–2228. [PubMed] [Google Scholar]
- Dobb GJ, Weekes JW. Clinical confirmation of brain death. . Anaesth Intensive Care. 1995;23:37–43. doi: 10.1177/0310057X9502300125. [DOI] [PubMed] [Google Scholar]
- Hanley DF. Brain death: an update on the North American view point. Anaesth Intensive Care. 1995;23:24–25. doi: 10.1177/0310057X9502300106. [DOI] [PubMed] [Google Scholar]
- Power BM, VanHeerden PV. The physiologic changes associated with brain death — current concepts and implications for the treatment of the brain dead organ donor. Anaesth Intensive Care. 1995;23:26–36. doi: 10.1177/0310057X9502300107. [DOI] [PubMed] [Google Scholar]
- Grossman MD, Reilly PM, McMahon DJ, et al. Loss of potential solid organ donors due to medical failure. Crit Care Med . 1996;24:A76. [Google Scholar]
- Reilly PM, Sing RF, Grossman MD, et al. The cost of altruism: patient charges for organ donation. J Trauma. 1995;39:1213. [Google Scholar]
- Ross SE, Nathan H, O'Malley KF. Impact of a required request law on vital organ donation. J Trauma. 1990;38:820–824. doi: 10.1097/00005373-199007000-00009. [DOI] [PubMed] [Google Scholar]
- Mackersie RC, Bronsther OL, Shackford SR. Organ procurement in patients with fatal head injuries. . Ann Surg. 1991;213:143–150. doi: 10.1097/00000658-199102000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris JA, Slaton J, Gibbs D. Vascular organ procurement in the trauma population. J Trauma. 1989;29:782–787. doi: 10.1097/00005373-198906000-00014. [DOI] [PubMed] [Google Scholar]
- Sosin DM, Snlezek JE, Waxweiler RJ. Trends in death associated with traumatic brain injury, 1979 through 1992. JAMA. 1995;273:1778–1780. [PubMed] [Google Scholar]
- Schwab CW. Violence: America's uncivil war - Presidential address, sixth scientific assembly of the Eastern Association for the Surgery of Trauma. J Trauma. 1993;35:657–665. [PubMed] [Google Scholar]
- Yang SL, Abrams J, Smolinski S, et al. Organ donation and referrals among African-Americans. Transplant Proc. 1993;25:2487–2488. [PubMed] [Google Scholar]
- Ali MJ. Essentials of organ donor problems and their management. . Anesth Clinics NA. 1994;12:655–671. [Google Scholar]
- Ali MJ, Wood G, Gelb AW. Essentials of organ donor problems and their management: a four year review of a Canadian transplant center. Can J Anesth. 1992;39:A125. [Google Scholar]
- Teja JL, Quesada JM, Rabanal JM, et al. Organ donor management: review of 68 consecutive cases. Transplant Proc. 1991;23:2490. [PubMed] [Google Scholar]
- Lucas BA, Baughn WK, Spees EK Sanfillipo F. Identification of donor factors predisposing to high discard rates of cadaver kidneys and increased graft loss within one year post-transplantation: SEOPF 1977-1982. . Transplantation. 1987;43:253–258. doi: 10.1097/00007890-198702000-00018. [DOI] [PubMed] [Google Scholar]
- Chatterjee SN, Payne JE, Berke TV. Difficulties in obtaining kidneys from potential postmortem donors. JAMA. 1975;232:822–824. [PubMed] [Google Scholar]
- Scheinkestel CD, Tuxen DV, Cooper DJ, et al. Medical management of the potential organ donor. Anaesth Intensive Care . 1995;23:51–59. doi: 10.1177/0310057X9502300110. [DOI] [PubMed] [Google Scholar]
- Spieth M, Abella E, Sutter C, et al. Importance of the lateral view in the evaluation of suspected brain death. Clin Nuc Med. 1995;20:965–968. doi: 10.1097/00003072-199511000-00003. [DOI] [PubMed] [Google Scholar]
- Pennsylvania Brain Death Law: Act 1982-323 (SB 1092): signed by Richard Thornburg. 1982.
- Hospital of the University of Pennsylavania: Policy regarding determination of death by neurologic criteria Philadelphia, PA: Hospital of the University of Pennsylvania. 1994.
- de la Riva A, Gonzalez FM, Llamas-Elvira JM, et al. Diagnosis of brain death: superiority of perfusion studies with 99m Tc-HMPAO over conventional radionuclide cerebral angiography. Br J Radiol. 1992;65:289–294. doi: 10.1259/0007-1285-65-772-289. [DOI] [PubMed] [Google Scholar]
- Wieler H, Marohl K, Kaiser KP, et al. Tc-99m HMPAO cerebral scintigraphy: a reliable, noninvasive method for determination of brain death. Clin Nuc Med. 1993;18:104–109. doi: 10.1097/00003072-199302000-00002. [DOI] [PubMed] [Google Scholar]
- Wilson K, Gordon L, Selby JB. The diagnosis of brain death with Tc-99m HMPAO. Clin Nuc Med. 1993;18:428–434. doi: 10.1097/00003072-199305000-00013. [DOI] [PubMed] [Google Scholar]
- Monsein LH. The imaging of brain death. Anaesth Intensive Care. 1995;23:44–50. doi: 10.1177/0310057X9502300109. [DOI] [PubMed] [Google Scholar]
- Laurin NR, Driedger AA, Hurwitz GA, et al. Cerebral perfusion imaging with the technetium-99m HMPAO. J Nuc Med. 1989;30:1627–1635. [PubMed] [Google Scholar]
- Eggers PW, Kucken LE. Cost issues in transplantation. Surg Clin North Am. 1994;74:1259–1267. [PubMed] [Google Scholar]
- Gorman KJ, Fein AJ, Shield CF. Relationship between clinical outcome, inpatient length of stay, and cost of renal transplantation at four US transplant centers. Transplant Proc. 1993;25:1690–1691. [PubMed] [Google Scholar]