

Abstract
A valgus knee is a disabling condition that can affect patients of all ages. Antivalgus osteotomy of the knee is the treatment of choice to correct the valgus, to eliminate pain in the young or middle age patient, and to avoid or delay a total knee replacement. A distal femoral lateral opening wedge procedure appears to be one of the choices for medium or large corrections and is particularly easy and precise if compared to the medial femoral closing wedge osteotomy. However, if the deformity is minimal, a tibial medial closing wedge osteotomy can be done with a faster healing and a short recovery time.
Introduction
The rationale behind the osteotomy is to correct the angular deformity at the knee and, therefore, decrease the excessive weight bearing load across the affected compartment which is the most involved by the degenerative process. Since alternative treatments in the 1970s for severe degenerative and inflammatory diseases of the knee were limited, femoral osteotomy was used early on for osteoarthrosis (OA), rheumatoid arthritis and secondary arthrosis, regardless of the aetiopathogenesis and the magnitude of the angular deformity.
The young patient with knee OA or with an initial condral pathology presents a challenging treatment dilemma to the orthopaedic surgeon. A valgus painful knee is a disabling condition that can affect patients of all ages. Anti-valgus osteotomies are the treatment of choice to correct the valgus deformity and eliminate pain and other functional problems. In particular, patients with an early arthritis of the lateral femoro-tibial compartment or damage of the cartilage of the lateral femoral condyle are candidates for anti-valgus osteotomies. Both the lateral femoral condyle and the lateral tibial plateau have convex surfaces, the congruence of which is maintained thanks to the integrity of the lateral meniscus. The absence of the meniscus can lead to a progressive deterioration of the opposing cartilage surface, due to the increased concentration of stress. Middle-aged patients with previous involvement in sports activities can develop lateral femoro-tibial arthritis early, which may lead to a lateral meniscectomy in early age. Damage to the cartilage of the lateral femoral condyle associated with an anterior cruciate (ACL) and or posterior cruciate (PCL) acute tear or chronic laxity can also lead to lateral meniscectomy. A congenital valgus deformity often associated with excessive weight can also cause early lateral arthritis due to the rapid degeneration of the meniscus and then of the cartilage. A lateral meniscus cyst or a lateral discoid meniscus represent a relatively frequent indication for a “subtotal” meniscectomy even in young athletes. All of the above may be considered candidates for anti-valgus osteotomy.
Indications and contraindications
Nowadays we believe that the patients selected for a distal femoral osteotomy should have mostly unicompartimental OA with axial malalignment. However, fracture and other trauma, congenital and acquired deformities, and idiopatic osteonecrosis may also be in particular cases indications for the osteotomy. There is no definite age below which one should do an osteotomy and above which one should do an arthroplasty. The age of 60 is the most often cited, but activity level, lifestyle and general health must be considered. As long-term studies of arthroplasty would demonstrate, age considerations may change; but it still remains that the age group of osteotomy patients is generally younger than that for knee arthroplasty. Furthermore, the actual trend seems to be oriented towards an early treatment of the unicompartimental OA in relatively young patients since the better results are to be expected when the articular changes are in the initial stage of the degenerative process. Osteotomy is best done for primarily unicompartimental OA in knees with generally well maintained range of motion (ROM). Osteotomy should probably not be done in patients with rheumatoid arthritis, patients with very unstable knees, nor in knees with greater than 20° of varus deformity, because, according to Insall, these knees are complicated by an associated severe ligamentous laxity and subluxation. The latter is a relative contraindication; in fact, even if the correction of the mechanical axis in such a great deformity can result in a relaxed collateral ligamentous complex, often the knee develops a new functional stability and many authors, including ourselves, do not routinely perform retightening of the ligamentous structures.
A patient who has a valgus deformity and anterior cruciate ligament (ACL) insufficiency may be treated with an ACL reconstruction in addition to the distal femoral osteotomy. A technically demanding procedure, the osteotomy associated with the ligament reconstruction addresses the underlying disorder and corrects the problems. Because it is not a routine procedure, it will not be discussed here. However, the symptoms of pain and instability must be separated as clearly as possible because when the pain prevails, especially in sedentary patients, correction of alignment, with consequent relief of lateral compartment pain can be a satisfactory treatment.
The case of the overweight patient is a controversial topic generating a conflict of opinions. Obesity has a negative effect on the outcome of surgery in many orthopaedic operations. Most would agree that excess body weight could make a patient a better candidate for osteotomy than for arthroplasty, but it is also true that obesity will represent a negative factor in view of the possible general postoperative complications. When a patient is overweight, the weight should be brought to near normal before surgery since worse long-term results for osteotomy related to obesity have been demonstrated. Contraindication to the osteotomy is severe bone loss (more than a few millimeters) of the lateral tibia or femur. When lateral compartment bony support is insufficient, congruent weight-bearing on both tibial plateaus following the osteotomy is not possible. In this situation, tibiofemoral contact will teeter on the relatively prominent intercondylar tibial spines.
The presence of severe valgus deformity may be associated with subluxation of the tibia. Subluxation greater than 1 cm is an absolute contraindication to osteotomy and some authors suggest that osteotomy should not be performed if any translation or subluxation is present.
Antivalgus osteotomy is designed to relieve pain caused by an initial arthrosis of the lateral knee compartment. Slight degenerative changes of the patellofemoral joint are not a contraindication to osteotomy, since following a distal femoral opening wedge osteotomy, the Q angle is reduced and the anterior tibial tubercle is medialised, unloading the patello femoral compartment.
Radiographic assessment and preoperative planning
The standard evaluation begins with an assessment of the alignment of the lower limbs with four short films: bilateral weight bearing antero-posterior views in full extension and bilateral weight bearing postero-anterior views at 45°. To complete the evaluation of the knee, we look at the different radiographic views, including the standard lateral and the axial views of the patellofemoral joint. The Rosenberg view [1], a comparative posteroanterior weight-bearing radiograph at 45 degrees of knee flexion, facilitates the diagnosis in case the standard anteroposterior (AP) view is not sensitive enough (Fig. 1). It has a strong predictive value, especially when the deformity is associated with a cruciate insufficiency, and therefore the chondral wear prevails in the posterior part of the tibial plateaus. Most authors do not recommend computed tomography (CT) scans or magnetic resonance imaging (MRI) in studying a candidate for knee osteotomy; but we think that the stress reaction of the subchondral bone, detectable by MRI, could be the only sign of a degenerative process at its earlier stage. If an anti-valgus osteotomy is indicated, one should obtain a bilateral full length standing alignment film with the femoral head and the ankle included in the X-ray. Several measurements taken from these films will assist the preoperative planning. Measurement of the mechanical axis, a straight line drawn from the centre of the femoral head to the centre of the talus is most important, as it indicates where the weight passes through the knee joint. Lateral radiographs are assessed for sagittal plane deformity, including measurement of tibial slope. The osteotomy is planned according to the method described by Dugdale et al. [2]. The weight bearing line is placed at a selected position 48–50% across the width of the tibial plateau from medial to lateral. The correction angle is formed by the angle between the line from the centre of the femoral head to 50% of the width of the tibia and the line from the centre of the talus to the 50% coordinate (Fig. 2). By measuring the width of the femur at the level of the proposed osteotomy, the surgeon can convert the angular correction into the wedge size. Extensive clinical experience has shown that over correction in varus is absolutely contraindicated for an optimal long-term result from osteotomy.
Fig. 1.
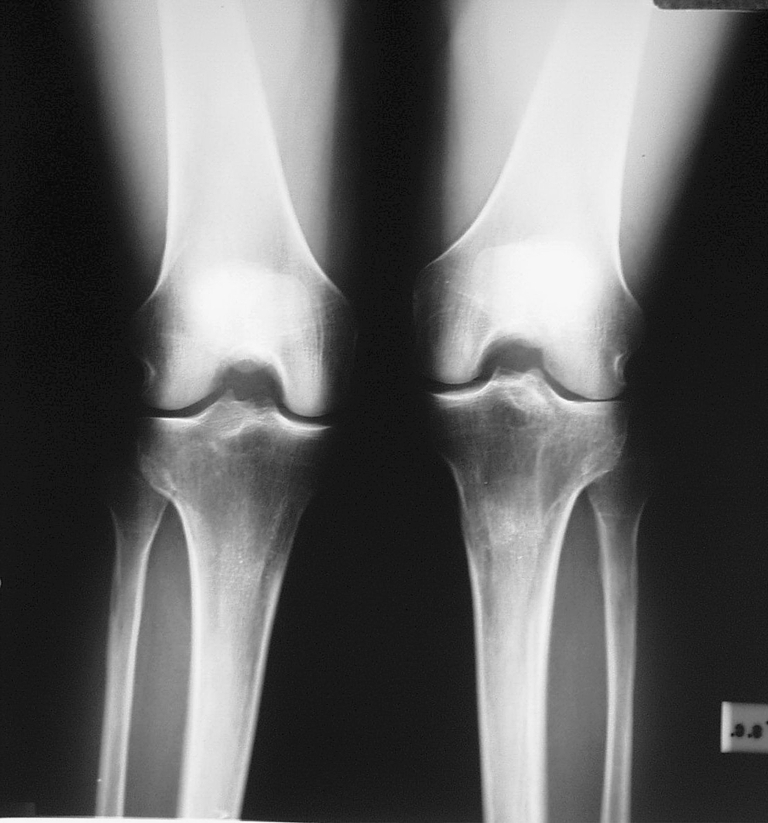
Preoperative Rosenberg’s view of a valgus knee
Fig. 2.

Preoperative planning. a A valgus knee. b The correction angle is formed by the line from the centre of the femoral head to 50% of the tibial plateau and the line from the centre of the talus to the 50% coordinate. c The achieved correction
Surgical options
To perform an anti-valgus osteotomy, the surgeon can choose among three main surgical options: distal femoral medial closing wedge osteotomy, distal femoral lateral opening wedge osteotomy and proximal tibial medial closing wedge osteotomy.
Distal femoral medial closing wedge osteotomy
Distal femoral medial closing wedge osteotomy is performed from the medial side, just proximal to the adductor tubercle and the anterior margin of the femoral articular surface. A stable construction is achieved by taking a 2/3 wedge from the medial supracondylar area, leaving the lateral cortex intact and closing the osteotomy with a 90° blade plate with the tensioning device applied, thus creating intrinsic stability [3]. An ordinary 90° plate with offset, normally used in intertrocanteric osteotomies, provides the necessary extra stability for early mobilisation of the patient. This type of osteotomy requires a medial and therefore a more precarious approach, and the removal of a precise bone wedge can also be difficult and imprecise.
Open wedge distal femoral osteotomy
To accomplish reproducible results with fewer technical difficulties, the senior author (G. Puddu) developed a complete yet simple system of dedicated instruments and plates [4–6]. One unique plate contains a spacer as a tooth, available in different sizes from 5 to 17.5 mm in thickness. The tooth enters into the osteotomy line holding the position and preventing a later collapse of the bone with could result in recurrence of the deformity. The thickness of the spacer must coincide with the desired angle of correction, which is calculated in advance. The plates specially designed for the opening wedge femoral osteotomy (Arthrex, Naples, Florida) are T-shaped with four holes proximal and three holes distal to the tooth (Fig. 3). The current second generation plate is made in titanium alloy and features special screw holes, through which the screws can be freely orientated in any direction then locked into the plate (Fig. 4). Dedicated cortical and cancellous titanium alloy screws are available. A new tool, the “jack opener” (Fig. 5), facilitates the opening of the osteotomy [7, 8]. A “wedge opener” (Fig. 6) is then inserted into the osteotomic site. This device’s two graduated wedge-shaped tines facilitate the positioning of the plate.
Fig. 3.

The distal femoral open wedge osteotomy
Fig. 4.

The titanium plate
Fig. 5.

A double osteotome (jack opener) is used to open the osteotomy
Fig. 6.

The wedge opener
Surgical technique
Step 1: patient position
We prefer a normal operating table with the patient in a supine position and the C-arm of an image intensifier set up opposite to the surgeon. The patient is draped as usual in knee surgery. We also prepare the iliac crest and cover the foot using a very fine stockinette and a transparent adhesive drape to minimise the bulging at the ankle so that it will be possible to better assess the femorotibial alignment after the correction. If iliac crest bone autograft is to be used, the ipsilateral crest is also prepared and draped. The tourniquet may be inflated.
Step 2: arthroscopy
In all the cases arthroscopy was carried out before the osteotomy. Here, arthroscopy serves two purposes. First, it allows assessment of the relative integrity of both the medial compartment and the patellofemoral joint and, second, it facilitates the treatment of any intrarticular pathology, such as the removal of a meniscal flap or anterior tibial osteophyte.
Step 3: incision and exposure
The lateral aspect of the femur is exposed through a standard straight incision through the skin and the fascia, starting two finger-breadths distally to the epicondyle and extending the incision about 12 cm proximally. The dissection is carried down to the vastus lateralis, which was retracted from the posterolateral intermuscular septum using a special dedicated Homan retractor placed ventrally. Perforating vessels are to be expected and should be controlled with ligature or electrocautery. The joint capsule is left intact, and the lateral cortex exposed. The procedure is facilitated by flexion of the knee.
Step 4: osteotomy
An Homan retractor is placed under the posterior aspect of the femoral metaphysis to protect the vessels and to expose the posterolateral aspect of the femur in order to place the plate in the desired position. With the knee in extension and under fluoroscopic control, a guide wire is drilled freehand through the distal femur from lateral to medial (Fig. 7a). A slightly oblique direction (about 20°) should be maintained from a proximal point on the lateral cortex, three finger breadth above the lateral epicondyle, above the trochlear groove, to a distal point a few millimetres proximal to the medial epicondyle (Fig. 7b). The instruments' system also provides a simple osteotomy cutting guide to facilitate the use of the oscillating saw and to keep the osteotomy perpendicular to the long axis of the femur in order to have the T-plate well-oriented with the femoral shaft. The osteotomy is performed keeping the oscillating saw blade proximal and parallel to the cutting guide (Fig. 8a) in order to prevent a possible migration of the osteotomy into the joint. The saw is used to cut only 1 cm in depth of the lateral cortex. A sharp osteotome is used to finish the osteotomy. The surgeon should be certain that the anterior and posterior cortices, as well as all of the cancellous metaphysis, are completely interrupted but should preserve a medial hinge of intact bone (about 1 cm). While performing the osteotomy, it is important to regularly check progress with the fluoroscope to ensure the appropriate depth and direction of the cut. The osteotomy is easily opened to the desired degree of correction with the assistance of the jack opener (Fig. 8b).
Fig. 7.

a and b, a pin is drilled under fluoroscopy
Fig. 8.

a The oscillating saw is proximal to the cutting guide. b The jack opens the osteotomy. c The wedges measure and keep the osteotomy open
Step 5: wedge opening and plate fixation
After the distraction by the jack, the opener wedge is introduced and slowly advanced into the osteotomy (Fig. 8c). The surgeon measures the dimension of the bone gap directly on the graduated tines of the wedges and selects the proper plate in accordance with the preperative measurement. By removing the handle and, if necessary, one of the wedges, with the other still into the osteotomy, the plate can be readily positioned on the lateral femoral cortex with the spacer tooth introduced into the oseotomy line. If the plate does not fit the femur cortex properly, it must be precontoured by modelling with the bending pliers. Before fixing the plate, the mechanical axis is checked by means of the special guide rod, long enough to extend from the centre of the femoral head to the centre of the ankle. Under fluoroscopy, the position of the rod over the knee joint is checked. To obtain a neutral mechanical axis it should be approximately in the centre of the tibial plateaus between the tibial spines. When the correction is excessive a different plate with a thicker or thinner tooth is needed. The plate is then fixed with four cortical screws proximal to the osteotomy and two (rarely three) cancellous screws distally (Fig. 9). We recommend a lateral plate instead of a medial one for an important biomechanical reason. When a normal knee with a valgus femorotibial angle is loaded in single-leg stance, the lateral femur is the tension side secondary to the extrinsic varus component of the body weight. In severe genu valgum, the mechanical axis moves laterally and therefore the convex medial side is subjected to tensile forces. After osteotomy, the mechanical axis is again moved medially, which returns the tension side of the knee to the lateral side. To act as a tension band, the plate must be applied to the lateral femur. Application of the plate to the medial femur after the osteotomy, as in the closing-wedge osteotomy with the AO 90-degree angled blade plate, violates this principle and will probably lead to a high rate of failure.
Fig. 9.

Perioperative fluoroscopic control
Step 6: bone grafting
We always fill the osteotomy defect with three wedge-shaped tricortico-cancellous grafts from the ipsilateral iliac crest (Fig. 9b). According to other authors, bone grafting is recommended in all opening-wedge osteotomies greater than 7.5 mm to prevent delayed union or nonunion and/or fixation failure. In osteotomies 7.5 mm or smaller, the decision to bone-graft should be based on circumstances. The correct position of the plate and grafts is confirmed with AP and lateral radiographs (Fig. 10a and b). One or two drains (one intra-articular) are prepared and the wound is closed in a routine fashion.
Fig. 10.

The iliac crest fills the osteotomy
The lateral positioning of the T-plate is critical. The osteotomy has to be perfectly aligned in the sagittal plane, perpendicular to the longitudinal axis of the femur, to ensure that the long arm of the plate lies in the centre of the diaphysis. In fact, the spacer tooth forms a right angle with the plate that prevents the correct positioning of the long arm on the bone when the osteotomy is oblique in the femur.
Injuries to the vessels are infrequent. Thrombophlebitis and infections are generic complications in common with all the other surgical procedures involving the inferior limb. Delayed union may occur, but most osteotomies will go on to union with time. Nonunion is also a possibility. In our series (55 tibial and 21 femoral osteotomies with a minimum follow-up of four years) we had no nonunions. This probably is the result of the systematic use of bone grafts to fill the osteotomy.
It may be incorrect to include loss of the desired correction as a true complication. In opening wedge, the bone collapse of the grafts might allow a decrease of the angular correction, but the new plates appear to minimise this. Of course continuing degenerative changes and high adduction moment contribute to a gradual loss of correction as time goes by.
Postoperative management
After surgery the knee is immobilised with a range-of-motion brace in full extension or at slight flexion of about 10° that allows a full range of motion when unlocked. Passive flexion and extension in a continuous passive motion device are started the day after surgery. The drains are removed 48 hours later. Patients are allowed to walk with no weight bearing on the limb from the second postoperative day. They are discharged from the hospital in three to four days when postoperative knee pain and effusion are minimal, and range of motion (ROM), flexibility and strengthening exercises commence. The exercise program must also integrate the trunk, hip and ankle muscles to provide dynamic knee stabilisation while addressing isolated quadriceps femoris deficiencies. Physical therapy intervention with the knee osteotomy patient requires continual attention to the balance between protection and function. Although progressive weight bearing and ROM exercises are vital to recovery, excessive early joint loading and terminal knee flexion–extension with external loads can compromise the integrity of the surgical realignment. Patients are usually able to completely flex the knee within the first four weeks following surgery. After six weeks partial weight bearing is allowed. Full weight bearing is normally possible after eight or nine weeks provided there is radiographic evidence that the bone has healed sufficiently. Restoring proprioceptive-kinesthetic normality at the involved lower limb must also be emphasised. The absence of apparent discomfort or movement-avoidance patterns assures the therapist that neuromuscular control for dynamic knee stabilisation is improving. In older patients, particularly those that have not recently participated in a physical exercise regimen, rehab may need to be delayed. In such cases rehabilitation should concentrate on active ROM to facilitate articular cartilage nourishment and preservation.
Tibial medial closing wedge osteotomy
When a small correction is required, tibial medial closing wedge osteotomy may be a suitable surgical choice (Fig. 11a). In our experience, supported by Coventry [9], Chambat et al. [10], and Marti and Verhagen [11], a joint surface tilt of 10° in the coronal plane is well tolerated. If the correction is greater than 10° the tibia gradually subluxates laterally [12], and on an anteroposterior radiograph, the femur appears to fall off the medial tibial plateau. A medial proximal tibial approach is used (the same as in opening wedge osteotomy). No graft is required and healing generally occurs in four weeks from surgery.
Fig. 11.

Postoperative control
After arthroscopy, an antero-medial longitudinal skin incision is performed; the pes anserinus is partially detached. The superficial layer of the medial collateral ligament is divided and the medial tibial metaphysis is exposed. The distal insertion of the patellar tendon is exposed and the osteotomy site confirmed with fluoroscopy using a Steinmann pin. The pin is driven from medial to lateral and from distal to proximal above the tibial tuberosity, pointing towards the fibular head. The osteotomy is begun with the oscillating saw then completed by the appropriate osteotome running underneath the guide wire to prevent entering the epiphisis or the joint space. It is necessary to leave at least 5 mm of intact lateral tibial cortex (“hinge”) to ensure good stability of the osteotomy. Resection must be minimal and can be performed under fluoroscopy and should be commensurate with the preoperative planning. As in the distal femoral open wedge osteotomy, the final correction has to bring the mechanical axis to the mid point of the tibial plateau. It is important that resection be minimal and, by forcing the knee into varus, fracture of the lateral hinge permits medial bone impaction and good bone contact. Final correction can be checked intraoperatively with the guide rod. The osteotomy is fixed with one or two staples (Fig. 11b) or with a four-hole plate. Postoperatively, the lower limb is immobilised in a functional brace with unlimited range of motion and full weight bearing at 30 days. One can expect complete healing of the osteotomy by six to seven weeks from surgery.
Complications
The risk of intrarticular fracture is always present. This is more often due to a mistake in positioning the guide pin too close to the joint, leaving little metaphysical bone stock between the osteotomy and the articular surface. It also may result from failure to completely divide the posterior or more often anterior cortex. This may cause an articular fracture to occur when the correction is attempted. The osteotomy jack reduces this risk, but does not eradicate it completely. Another possible intraoperative complication is subluxation of the osteotomy. It can happen when the surgeon does not leave a sufficient hinge of intact bone. Preventing this technical problem starts with the proper choice of the site of the osteotomy cut. The cut should be sufficiently distal in the femur to avoid the maximum step-off of the bone profile and obtain a more stable fixation. An intact bone hinge is essential for stability and, when correctly performed, protects the osteotomy from possible dislocation. If the undesired subluxation has occurred, a possible method of correction is a staple fixation through a controlateral incision.
Failure of the hardware, especially the plates, is very rare. Vascular injuries are very rare provided the surgeon protects the vessels through correct use of a posterior Homan retractor and the knee remains flexed during surgery. Thrombophlebitis and infections are generic complications common to all other surgical procedures performed on the lower limb.
Results
The results of supracondylar osteotomy reported in the literature are generally good. Healy et al. [13] reported a series of 23 distal femoral osteotomies with a follow-up of four years. The Hospital for Special Surgery (HSS) Knee Score improved from an average of 65 points to 86 points postoperatively. McDermott et al. [14] reported on 24 patients for whom the greatest improvements were found in the “pain” category, with an average increase of 16.5 points. Miniaci et al. [15] reported 86% good or excellent results in a series of 40 supracondylar femoral closing wedge varus osteotomies, with a mean follow-up of 5.5 years. Finkelstein et al. [16], in a study of 21 knees, demonstrated that the probability of survival at ten years was 64%. Marti et al. [3], analysing 15 closed wedge varus femoral osteotomies, obtained 75% good results without any complication.
The author's experience includes a series of 21 patients with an average age of 54 years (seven males and 14 females) operated upon between 1992 and 2002 with a follow-up of four to 14 years (Fig. 12). Every patient improved according to both the International Knee Committe Documentation Committee (IKDC) rating scale and the HSS system.
Fig. 12.
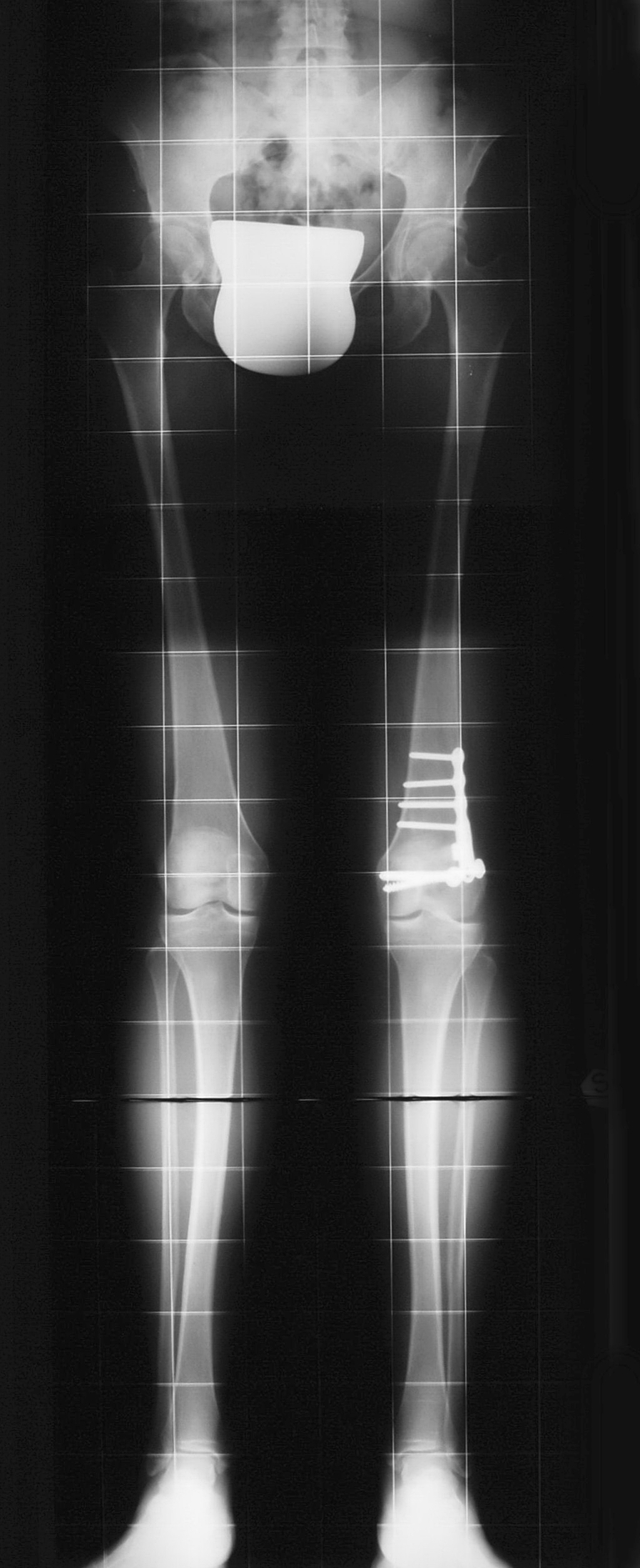
Results at 8-year follow-up exam
In a series of 47 patients treated by a medial tibial closing wedge osteotomy and followed up for a minimum ten years, Chambat et al. [10] found that 72% of patients had “good” and “very good” results, with an improvement in pain in 91%. In our six cases operated on between 1996 and 2002 there was excellent improvement of pain and functional capabilities with the HSS score improving from an average of 60 points to 87 points.
Conclusions
In valgus painful knees with degeneration of the lateral compartment in young or middle-aged patients, antivalgus osteotomies represent an effective surgical treatment. Unicompartimental prosthesis arthroplasty is indicated in older patients and particularly in those cases with osteonecrosis or severe lateral arthrosis. Patients with a depressed lateral compartment and extreme valgus deformity are more suitably treated with total knee replacement (TKR). The literature [16, 17] suggests that supracondylar osteotomy does not preclude TKR. A varus distal femoral osteotomy can make a future TKR technically easier [18]. Opening wedge lateral femoral anti-valgus osteotomy represents a precise and easy technique that allows accurate correction of the alignment, moving the weight-bearing axis from the lateral tibial plateau towards the centre of the knee joint. Moreover, its peculiar method of fixation by special plates with spacers helps prevent secondary loss of correction and shortening of the limb. The medial tibial closing wedge osteotomy is a valid alternative for minor corrections (10° or less). The procedure is easy, safe and does not compromise range of motion.
References
- 1.Rosenberg TD, Paulos LE, Parker RD, et al. The forty-five degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Joint Surg Am. 1988;70:1479–1483. [PubMed] [Google Scholar]
- 2.Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. Clin Orthop. 1992;274:248–264. [PubMed] [Google Scholar]
- 3.Marti RK, Schroder J, Witteveen A. The closed wedge varus supracondilar osteotomy. Oper Tech Sports Med. 2000;8:48–55. doi: 10.1016/S1060-1872(00)80025-8. [DOI] [Google Scholar]
- 4.Puddu G, Cerullo G, Cipolla M. Femoral antivalgus opening wedge osteotomy. In: Osteotomies about the athletic knee. Oper Tech Sports Med. 2000;8:56–60. doi: 10.1016/S1060-1872(00)80026-X. [DOI] [Google Scholar]
- 5.Puddu G, Franco V, Cipolla M, et al (2002) Opening wedge osteotomy. Proximal tibia and distal femur. In: Jackson RW(ed) Reconstructive knee surgery. Master techniques in orthopaedic surgery. Lippincott Williams and Wilkins, Philadelphia, pp 375–390
- 6.Franco V, Cerullo G, Cipolla M, et al. Osteotomy for osteoarthritis of the knee. Curr Orthop. 2005;19:415–427. doi: 10.1016/j.cuor.2005.10.008. [DOI] [Google Scholar]
- 7.Puddu G, Cerullo G, Cipolla M et al (2003) Osteotomies about the knee. In: Fu FH, Browner BD (ed) Management of osteoarthritis of the knee: an international consensus. American Academy of Orthopaedic Surgeons, pp 17–30
- 8.Puddu G, Cipolla M, Cerullo G, et al. Opening wedge osteotomy: femoral. Surgical techniques of the knee. New York: Thieme Med. Publish. Inc; 2005. pp. 241–249. [Google Scholar]
- 9.Coventry MB. Proximal tibial varus osteotomy for osteoarthritis of the lateral compartment of the knee. J Bone Jt Surg Am. 1987;69:32–38. [PubMed] [Google Scholar]
- 10.Chambat P, Ait Si Selmi T, Dejour D. Varus tibial osteotomy. In: Osteotomies about the athletic knee. Oper Tech Sports Med. 2000;8:44–47. doi: 10.1016/S1060-1872(00)80024-6. [DOI] [Google Scholar]
- 11.Marti RK, Verhagen RAW (2001) Upper tibial osteotomy for osteoarthritis of the knee. Surg Techn Orthop Traumatol 55–530-A-10
- 12.Shoji H, Insall J. High tibial osteotomy for osteoarthritis of the knee with valgus deformity. J Bone Jt Surg Am. 1973;55:963–973. [PubMed] [Google Scholar]
- 13.Healy WL, Anglen JO, Wasilewsky SA, et al. Distal femoral varus osteotomy. J Bone Jt Surg Am. 1988;70:102–109. [PubMed] [Google Scholar]
- 14.McDermott PA, Finkelstein JA, Farine I, et al. Distal femoral varus osteotomy for valgus deformity of the knee. J Bone Jt Surg Am. 1988;70:110–116. [PubMed] [Google Scholar]
- 15.Miniaci A, Grossman SP, Jacob RP. Supracondylar femoral varus osteotomy in the treatment of valgus knee deformity. Am J Knee Surg. 1990;3:65–73. [Google Scholar]
- 16.Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur: A survivorship analysis. J Bone Jt Surg Am. 1996;78:1348–1352. doi: 10.2106/00004623-199609000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Cameron HU, Park YS. Total knee replacement after supracondylar femoral osteotomy. Am J Knee Surg. 1997;10:70–71. [PubMed] [Google Scholar]
- 18.Wachtl SW, Gautier E, Jacob RP (2000) Supracondylar femoral osteotomy for osteoarthritis of the knee. Surg Techn Orthop Traumatol 55–520-E-10