

Abstract
Background
Prospective measures of high knee abduction moment during landing identify female athletes at high risk for non-contact anterior cruciate ligament injury. Biomechanical laboratory measurements predict high knee abduction moment landing mechanics with high sensitivity (85%) and specificity (93%). The purpose of this study was to identify correlates to laboratory-based predictors of high knee abduction moment for use in a clinic-based anterior cruciate ligament injury risk prediction algorithm. The hypothesis was that clinically obtainable correlates derived from the highly predictive laboratory-based models would demonstrate high accuracy to determine high knee abduction moment status.
Methods
Female basketball and soccer players (N=744) were tested for anthropometrics, strength and landing biomechanics. Pearson correlation was used to identify clinically feasible correlates and logistic regression to obtain optimal models for high knee abduction moment prediction.
Findings
Clinical correlates to laboratory-based measures were identified and predicted high knee abduction moment status with 73% sensitivity and 70% specificity. The clinic-based prediction algorithm, including (Odds Ratio: 95% confidence interval) knee valgus motion (1.43:1.30–1.59 cm), knee flexion range of motion (.98:0.96–1.01 deg), body mass (1.04:1.02–1.06 kg), tibia length (1.38:1.25–1.52 cm) and quadriceps to hamstring ratio (1.70:1.06–2.70) predicted high knee abduction moment status with C statistic 0.81.
Interpretation
The combined correlates of increased knee valgus motion, knee flexion range of motion, body mass, tibia length and quadriceps to hamstrings ratio predict high knee abduction moment status in female athletes with high sensitivity and specificity.
Key Terms: Biomechanics correlated to increased ACL injury risk, ACL injury risk factors, Targeted Neuromuscular Training, ACL Injury Prevention, Assessment tools, Clinician Friendly
INTRODUCTION
Female athletes are reported to be four to six times more likely than males to sustain a sports related non-contact anterior cruciate ligament (ACL) injury.(Arendt and Dick, 1995, Malone et al., 1993) Several investigators have demonstrated that female athletes exhibit high knee abduction moment (KAM) related landing mechanics more often than males during landing and pivoting movements.(Ford et al., 2006, Malinzak et al., 2001, Hewett et al., 2004, Ford et al., 2003, Chappell et al., 2002, McLean et al., 2004a, Kernozek et al., 2005, Zeller et al., 2003, Pappas et al., 2007, Hewett et al., 2006b) These altered neuromuscular strategies or decreased neuromuscular control of the lower extremity during the execution of sports movements may underlie the increased risk of ACL injury in female athletes.(Ford et al., 2003, Ford et al., 2005, Hewett et al., 2005, McLean et al., 2004b, Chappell et al., 2002, Myer et al., 2006b) Females often demonstrate knee landing alignments associated with high KAM at the time of injury, in validation of these laboratory findings.(Olsen et al., 2004, Krosshaug et al., 2007, Boden et al., 2000) In addition, prospective measures related to knee abduction moment measured during drop vertical jump also predict ACL injury risk in young female athletes (Hewett et al., 2005) and in military cadets.(Padua et al., 2009)
Calculation of KAM, through inverse dynamics, requires complex laboratory-based three-dimensional kinematic and kinetic measurement techniques. However, a recent report has isolated biomechanical measures that contribute to nearly 80% of the measured variance in KAM during landing.(Myer et al., 2009b) These biomechanical predictors of KAM, which include increased knee abduction angle, increased relative quadriceps recruitment and decreased knee flexion range of motion (ROM), concomitant with increased tibia length and mass nor malized to body height that accompanies growth, are also measurements that have all been related to increased risk of ACL injury in previous prospective and retrospective epidemiological reports.(Boden et al., 2000, Uhorchak et al., 2003, Hewett et al., 2005, Padua et al., 2009) Unfortunately, expensive biomechanical laboratories, with the costly and labor intensive measurement tools to test individual athletes, are required to acquire these measurements. This restricts the potential to perform athlete risk assessments on a large scale, in particular limiting the potential to target high injury risk athletes with the appropriate intervention strategies. If simpler assessment tools are developed that can be administered in a clinic or field testing environment, which are validated by the highly accurate laboratory-based assessment, screening for ACL injury risk can be performed on a more widespread basis. The purpose of the current study was to identify potential correlates to laboratory-based predictors of high KAM for use in clinic-based ACL injury risk prediction algorithm. The hypothesis tested was that clinically obtainable correlates to measures used in the highly predictive laboratory-based models would demonstrate high accuracy in determination of high KAM status.
METHODS
Subjects
Between 2004 and 2008, all sixth through twelfth grade female athlete participants in basketball and soccer were recruited from a county public school district with five middle schools and three high schools to participate in a prospective longitudinal study. The goal of the study was to determine potential underlying mechanisms that increase ACL injury risk. First time visits for 744 subjects’ were designated for inclusion into the current analyses. Subjects were excluded (n=46) from the study if they did not complete biomechanical testing or if errors were found in the calculation of the dependent variable, KAM, leaving 698 subjects available for inclusion in the analyses (mean: 1SD) (age 13.9: 2.4 years; height 159.3: 8.6 cm; body mass 54.0: 12.5 kg; percent in each maturational status 17% pre-pubertal, 30% pubertal and 53% post-pubertal). For the initial model development, 598 of the 698 eligible subjects were randomly assigned to formulate the optimized prediction models. The data from the remaining 100 subjects was retained for verification of the optimized multivariable linear and logistic prediction models from the 598 randomly selected girls.
Procedures
Cincinnati Children’s Hospital Medical Center and Rocky Mountain University of Health Professions Institutional Review Boards approved the data collection procedures and consent forms. Parental consent and athlete assent were received prior to data collection. Subjects were tested prior to the start of their basketball or soccer competitive season. The testing consisted of a knee exam, medical history, maturational estimates, dynamic strength and landing biomechanical analysis.
Anthropometrics
Body mass was measured on a calibrated physician scale. A static standing trial was conducted prior to biomechanical testing in which the subject was instructed to stand still with foot placement standardized to the laboratory coordinate system. The static standing trial was used to calculate segment lengths as the estimated distance between the proximal and distal joint center (e.g. thigh segment distance was equal to the distance between the hip joint center and knee joint center). In addition, the static trial was used to calculate standing anatomical alignment measures.
Dynamic Strength
Isokinetic knee extension/flexion (concentric/concentric muscle action) strength was measured with the subject seated on the dynamometer Biodex System II (Shirley, New York) and the trunk perpendicular to the floor, the hip flexed to 90° and the knee flexed to 90°. Prior to each data collection set, a warm-up set, which consisted of five sub maximal knee flexion/extensions for each leg at 300°/sec, was performed. The test session consisted of ten knee flexion/extension repetitions for each leg at 300°/sec. Peak flexion and extension torques were recorded.(Myer et al., 2008) The ratio of quadriceps to hamstrings (QuadHam) strength peak isokinetic torque was calculated. Inclusion of relative quadriceps to hamstring strength measurements at 300/second has been demonstrated to be related to increased ACL injury risk in female athletes.(Myer et al., 2009a)
Landing Biomechanics
Three-dimensional hip, knee and ankle kinematic and kinetic data were quantified for the contact phase of three drop vertical jump (DVJ) tasks. Each subject was instrumented by a single investigator with 37 retroreflective markers placed on the sacrum, left PSIS, sternum and bilaterally on the shoulder, elbow, wrist, ASIS, greater trochanter, mid thigh, medial and lateral knee, tibial tubercle, mid shank, distal shank, medial and lateral ankle, heel, dorsal surface of the midfoot, lateral foot (5th metatarsal) and toe (between 2nd and 3rd metatarsals). First, a static trial was conducted in which the subject was instructed to stand still with foot placement standardized to the laboratory coordinate system. This static measurement was used as each subject’s neutral (zero) alignment; subsequent kinematic measures were referenced in relation to this position.(Ford et al., 2007) The DVJ involved the subject standing on top of a box (31 cm high) with their feet positioned 35 cm apart.(Ford et al., 2007, Hewett et al., 2005) They were instructed to drop directly down off the box and immediately perform a maximum vertical jump, raising both arms while jumping for a basketball rebound.(Ford et al., 2003)
All trials were collected by a single investigator with EVaRT (Version 4, Motion Analysis Corporation, Santa Rosa, CA) using a motion analysis system consisting of ten digital cameras (Eagle cameras, Motion Analysis Corporation, Santa Rosa, CA) positioned in the laboratory and sampled at 240 Hz. Prior to data collection, the motion analysis system was calibrated based on the manufacturer’s recommendation. Two force platforms (AMTI, Watertown, MA) were sampled at 1200 Hz and time synchronized with the motion analysis system. The force platforms were embedded into the floor and positioned 8 cm apart so that each foot would contact a different platform during the stance phase of the drop vertical jump.(Ford et al., 2007)
Following data collection, the motion and force data were further analyzed in Visual3D (Version 4.0, C-Motion, Inc.). The procedures within Visual3D first consisted of the development of a static model customized for each subject.(Ford et al., 2007) 3D marker trajectories from each trial were filtered at a cutoff frequency of 12 Hz.(Ford et al., 2007) 3D knee joint angles were calculated according to the Cardan/Euler rotation sequence.(Cole et al., 1993) Kinematic and force platform data were utilized to calculate knee joint moments using inverse dynamics.(Andriacchi et al., 1997, Winter, 1990, pp. 91–95) Net external knee moments were reported in the current study and represent the external load on the joint. Peak knee abduction angle and moment were identified during the deceleration phase of the initial stance phase of the DVJ. The deceleration phase was operationally defined from initial contact (vertical ground reaction force first exceeded 10 N) to the lowest vertical position of the body center of mass. Knee valgus motion was calculated as the 2D displacement of the knee in the coronal plane, from just prior to initial contact to the end of the deceleration phase of the drop jump landing task. The left side data were retained for statistical analysis.
Statistical analyses
Data were exported to SPSS (SPSS for Windows version 16.0 Chicago, IL) and SAS®, version 9.1 (SAS Institute, Cary, NC) for statistical analyses. Imputation of missing data observed for the identified correlated variables was performed using Solas (version 3.0). The imputation method employed was based on ordinary least-squares regression, using age and BMI as covariates and was necessary for less than 2% of the observations of any independent variable. Pearson’s correlation coefficients were calculated to assist in the initial screening of surrogate clinic-based predictor variables (Myer et al., 2009b) by selecting significant correlates (P <0.01) of the independent laboratory-based variables (peak knee abduction angle, peak knee extensor moment, knee flexion ROM, BMI Z-score and tibia length) previously shown to predict both KAM and the dichotomized high KAM (KAM >25.25 Nm) status with high R2 (0.78), sensitivity (85%) and specificity (93%).(Myer et al., 2009b) The cut-point used to classify the dependent variable status was >25.25Nm of KAM, which was based on published prediction modeling of ACL injury risk. This cut-point yielded the maximal sensitivity and specificity for prediction of ACL injury risk during a DVJ.(Hewett et al., 2005, Myer et al., 2007) Using this classification, subjects were categorized into a dichotomous (high KAM; “yes” or “no”) as the dependent variable.
For the final step in model development, multivariable logistic regression with a backward elimination strategy was employed. The logistic regression model was estimated using a logit link. An alpha level of 0.05 was used to judge statistical significance in all models. A nomogram was produced from the secondary classification model to allow predictions to be made in individual athletes.(Harrell, 2002) The development of the clinical nomogram was performed using R-project software. R is available as Free Software under the terms of the Free Software Foundation's GNU General Public License in source code form.
RESULTS
Mean and 95% CI for independent variables used in the model development are presented in Table 1, together with the correlation coefficients of the clinic-based surrogate predictor to its laboratory-based principal (Myer et al., 2009b) independent variable. The initial prediction of high KAM, was performed using logistic regression analysis in the training dataset (N=598). The final logistic regression model, which included the independent predictors: knee valgus motion, knee flexion ROM, mass, tibia length and QuadHam ratio, predicted high KAM status with 55% sensitivity and 86% specificity (P<0.001). This model was predictive of high KAM status with a C statistic of 0.83. This logistic regression model was validated by solving the prediction equation for each of the 100 subjects in the validation group and determining into which group (high KAM vs. low KAM) they were classified. The resultant prediction equation yielded a sensitivity of 58% and a specificity of 87% to predict >25.25Nm of KAM during the drop vertical jump.
Table 1.
Means, 95% confidence intervals ( CIs) and correlation coefficients for independent predictor variables used in model development (N=598).
| Mean | 95% Confidence Interval for Mean |
Surrogate Predictor Variable Correlation to Primary Predictor** |
||
|---|---|---|---|---|
| Lower Bound |
Upper Bound |
|||
| Peak Knee Abduction Angle (deg) Knee Valgus Motion (cm)† |
9.62 3.97 |
9.14 3.79 |
10.11 4.14 |
0.42** |
| Knee flexion ROM(deg)* | 59.21 | 58.47 | 59.95 | N/A |
| BMI Z-score (No. of SD) Mass(kg)† |
0.38 54.06 |
0.31 53.05 |
0.46 55.07 |
0.77** |
| Tibia Length (cm)* | 35.89 | 35.68 | 36.09 | N/A |
| Peak Knee Extensor Moment (Nm) QuadHam ratio† |
95.37 1.53 |
93.06 1.50 |
97.69 1.57 |
0.21** |
Predictor variables were included in both laboratory-based and clinic-based regression models.
Correlation is significant at the 0.01 level (2-tailed).
Surrogate clinic-based predictors employed in the logistic regression model.
Based on the relatively low risk of harm due to treatment (neuromuscular training (Myer et al., 2005, Myer et al., 2007, Hewett et al., 1996)) for the high KAM, we redefined the cut-point for classification into high and low KAM groups to predict the outcome with increased sensitivity by examination of the ROC curve. Accordingly, the prediction of secondary classification of high KAM (>21.74Nm of KAM) was repeated using logistic regression analysis techniques in the training dataset (N=598). The resultant logistic regression model, predicted high KAM status with 73% sensitivity and 70% specificity (p<0.001). Table 2 shows the odds ratio (OR) and 95% confidence limits for the predictors of high KAM (> 21.74 Nm of KAM). This model was predictive of high KAM status with a C statistic of 0.81. The ROC curve for this model is presented in Figure 1. This logistic model was also validated by solving the prediction equation for each subject in the validation group, yielded a sensitivity of 72% and a specificity of 72% to predict > 21.74Nm of KAM during the DVJ.
Table 2.
Odds Ratio (OR) Estimates and 95% CI for independent variables used in model development (N=598).
| OR | 95% Confidence Interval for OR |
||
|---|---|---|---|
| Lower | Upper | ||
| Knee valgus motion (cm) | 1.43 | 1.30 | 1.59 |
| Knee Flexion ROM (deg) | .98 | .96 | 1.01 |
| Body Mass (kg) | 1.04 | 1.02 | 1.06 |
| Tibia Length (cm) | 1.38 | 1.25 | 1.52 |
| QuadHam (ratio) | 1.70 | 1.06 | 2.70 |
Figure 1.
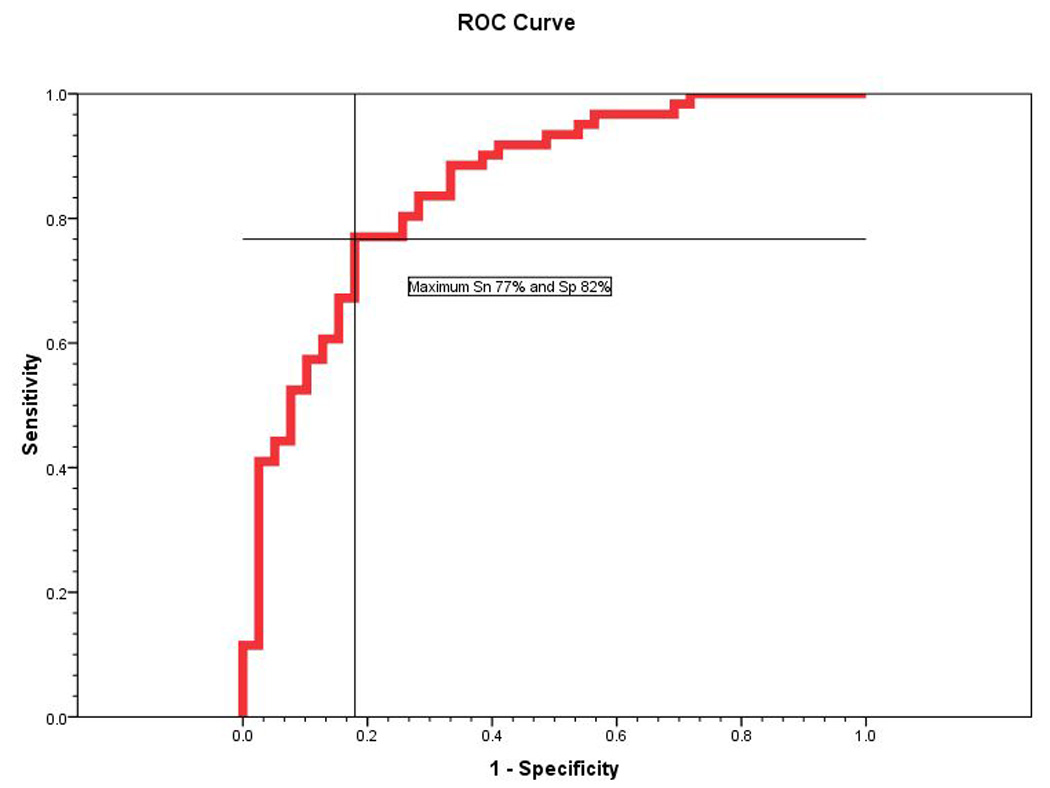
ROC curve for prediction of high KAM (>21.74 Nm of KAM). Cross bar indicates maximum sensitivity and specificity of the prediction model.
Figure 2 presents a predictive, clinician friendly nomogram developed from the analysis described above that can be used to predict high KAM (>21.74Nm KAM) based on tibia length, knee valgus motion, knee flexion ROM, body mass and quadriceps to hamstrings ratio. The nomogram code generates an equally distributed, segmented line representing standardized measurable units for each predictor variable. The range of values for each predictor is determined based on the data used to create the regression model, and therefore creation of the nomogram, requires a sufficiently powered regression model. The magnitude of each intra-segment distance is in direct proportion to that individual variable's strength of association (Beta coefficient) to the predicted outcome as determined in the combined multivariate regression equation.
Figure 2.
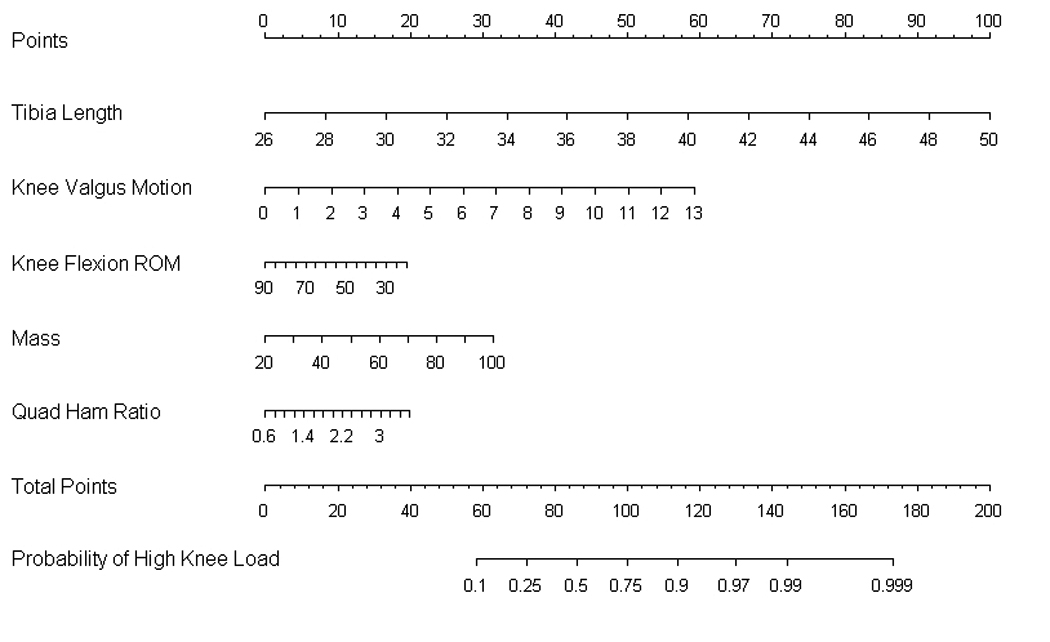
A clinician friendly nomogram that was developed from the regression analysis can be used to predict outcome based on tibia length, knee valgus motion, knee flexion ROM, mass and quadriceps to hamstring ratio. To use the prediction nomogram one should place a straight edge vertically so that it touches the designated variable on the axis for each predictor value, and record the value that each of the five predictors provides on the “points” axis at the top of the diagram. All of the recorded “points” measured using this method are then summed and this value is located on the “total points” line with a straight edge. A vertical line drawn down from the “total points line” to the “probability line” identifies the probability that the athlete will demonstrate high KAM (>21.74 Nm of knee abduction) during the drop vertical jump based on the utilized predictive variables.
DISCUSSION
The purpose of the current study was to develop a “clinician friendly” landing assessment tool derived from the highly predictive laboratory-based measurements that would be easy to use and would facilitate the potential for widespread use in clinical and field settings. A nomogram was developed from the logistic regression analyses that can be used to predict high KAM (>21.74Nm KAM) based on clinically measured tibia length, knee valgus motion, knee flexion ROM, body mass and quadriceps to hamstrings ratio.
The outcome tool (Figure 2) developed from the regression analysis can be used to predict the probability to demonstrate high KAM landing mechanics based on the described clinically obtainable measures tibia length, knee valgus motion, knee flexion range of motion, body mass and quadriceps to hamstrings ratio. Clinic-based tibia length can be measured using a standard measuring tape to quantify the distance between the lateral knee joint line to the lateral malleous. Body mass can be measured on a calibrated physician scale. Two dimensional (clinic-based) frontal and sagittal plane knee kinematic data can be captured with standard video cameras. QuadHam ratio is traditionally captured on isokinetic dynamometers in a clinical setting. If an isokinetic testing device is not readily available, then a surrogate measure of the QuadHam ratio can be developed based on the athlete’s body mass. The surrogate QuadHam ratio measure is obtained when a female athlete’s mass (kg) is multiplied by 0 .01 and the resultant value added to 1.10. If further simplicity is desired the mean value of 1.53 can be input into the nomogram to represent QuadHam ratio for the athlete.
Landing sequence images used for knee valgus motion (Figure 3A–B) and knee flexion ROM (Figure 3C–D) clinic-based measurement can be captured via the “print screen” feature available on most personal computers or they can be captured with freeware software such as VirtualDub software (copyright 1998–2009 Avery Lee). Recommended software for kinematic coordinate data capture and calculation are suggested to be performed with ImageJ (Rasband, W.S., ImageJ, U. S. National Institutes of Health, Bethesda, Maryland, USA, http://rsb.info.nih.gov/ij/, 1997–2009) software that is also available without surcharge (Figure 3).(Myer et al., 2010)
Figure 3.

A. The coordinate position of knee joint center is digitized in the frontal view measured at the frame prior to initial contact is used as the knee valgus position X1.
B. The coordinate position of knee joint center is digitized in the frontal view measured at the frame with maximum medial position and is utilized as the knee valgus position X2. The calibrated displacement measure between the two digitized knee coordinates (X2−X1) is representative of knee valgus motion during the drop vertical jump.
C. Knee flexion angle is digitized a t the frame prior to initial contact and recorded as the first measure of knee flexion ROM (Θ1).
D. Knee flexion angle is digitized at the frame with maximum knee flexion and recorded as the second measure of knee flexion ROM (Θ2).The displacement of knee flexion is calculated as the differences in knee flexion angles at the frame prior to initial contact and maximum knee flexion (Θ1−Θ2) and is representative of knee flexion ROM.
Figure 4A provides a completed algorithm for the presented subject using following the clinically feasible measurements quantified on her left leg: Tibia length: 36 cm; Knee valgus motion: 3.3 cm; Knee flexion ROM: 63.4°; mass: 57.2 kg; QuadHam: 1.78. Based on her demonstrated measurements, the prediction nomogram would indicate that this subject would have a 45% percent chance to demonstrate high KAM during her measured drop vertical jump. Figure 4B presents the completed algorithm for the same subject with the following clinic-based measurement of knee valgus motion on her right leg. The red solid lines indicate the shift in her measured knee valgus motion from 3.3 cm on her left leg to 6.0 cm or her right. Accordingly, this change in knee valgus motion shifts her probability of high knee load on her right leg to be 66% during this trial of the drop vertical jump.
Figure 4.


A. Completed nomogram for a representative subject with the following clinically feasible measurements quantified on her left leg: Tibia length: 36 cm; Knee valgus motion: 3.3 cm; Knee flexion ROM: 63.4°; mass: 57.2 kg; QuadHam: 1.78). Based on her demonstrated measurements, the prediction nomogram would indicate that this subject would have a 45% percent chance to demonstrate high KAM during her measured drop vertical jump.
B. Completed nomogram for the same subject with the following clinic-based measurement of knee valgus motion on her right leg. The red solid lines indicate the shift in her measured knee valgus motion from 3.3 cm on her left leg to 6.0 cm or her right. Accordingly, this change in knee valgus motion shifts her probability of high knee load on her right leg to be 66% during this trial of the drop vertical jump.
Recent studies demonstrate that neuromuscular training reduces the high KAM risk factor for ACL injury, increases performance and decreases knee and ACL injury incidence in female athletes.(Hewett et al., 2004, Myer et al., 2004, Hewett et al., 2006a, Hewett et al., 1996, Myer et al., 2007, Myer et al., 2006a, Myer et al., 2006b, Myer et al., 2005) However, re-evaluation of ACL injury rates in female athletes indicate that this important health issue has yet to be resolved, as increased knowledge and application of injury prevention techniques have not led to measureable reductions in ACL injury incidence in female athletes.(Agel et al., 2005) A recent investigation by Grindstaff and colleagues indicated that standard, non-targeted neuromuscular training programs may require application to 89 female athletes to prevent a single ACL injury.(Grindstaff et al., 2006) It is possible that the identification of female athletes who demonstrate risk factors for ACL injury such as high KAM could improve the efficiency of neuromuscular training by targeting these individuals.
The current investigation provides the critical next step to merge the gap between laboratory identification of injury risk factors (Hewett et al., 2005, Padua et al., 2009) and clinical practice with this simplified algorithm that can be utilized with clinic-based assessment tools. The simplicity and lessened equipment and labor cost (relative to laboratory-based assessments that may exceed $1000 per athlete) associated with utilization of this tool may facilitate the identification of high ACL injury risk athletes on a more widespread basis in clinical and field settings. Prior work has utilized laboratory-based measures to determine the potential differing effects of neuromuscular training in female athletes who demonstrate high KAM landing strategies relative to those who do not.(Myer et al., 2007) This prior study employed an abridged version of a comprehensive training protocol shown to alter biomechanical factors related to increased ACL injury risk in female athletes.(Myer et al., 2005, Paterno et al., 2004, Hewett et al., 2005) The results of this study indicate that females who demonstrate increased high KAM may be able to reduce this risk factor via targeted neuromuscular training, while those athletes without this risk factor may not reap similar benefits from the training program.(Myer et al., 2007) To further evaluate the potential effect of neuromuscular training on the high KAM risk factor, a linear regression analysis was performed to examine the potential association between the pre-test measures of high KAM and the change in this variable with neuromuscular training.(Myer et al., 2007) In the trained group, the pre-test KAM predicted the potential to reduce KAM with training. In contrast, the control group showed no similar causal relationship of pre-test KAM measures to change in the post test measure. If this is the case, a logical extension of these findings would be that it is more important to identify and target athletes identified as high KAM for injury prevention training programs than those with low KAM.
Myer et al. evaluated a comprehensive neuromuscular training protocol that was developed to reduce ACL injury risk and improve sports related performance measures(Myer et al., 2005). This comprehensive protocol successfully reduced knee abduction torques by 21%, but the females in the study who demonstrated low KAM may have masked the potentially larger training effects. This reported mean reduction in KAM may be masked by subjects who already demonstrated a low value of a measured risk factor that has been previously demonstrated (Knaus et al., 1993), but is often ignored in clinical investigations (Harrell, 2001). The current clinic-based tool can aid in the identification of female athletes with high KAM landing mechanics who will most likely obtain the greatest potential to significantly reduce dangerous knee loading profiles with targeted neuromuscular training. In addition, neuromuscular training targeted directly to reduce KAM in those who demonstrate high KAM landing mechanics may help athletes obtain landing mechanics that will take them out of “high-risk” category. These goals have not been previously achievable with non-targeted training protocols.(Myer et al., 2007) In addition, based on the low risk of the treatment for high KAM (neuromuscular training), we chose to influence the algorithm for highly sensitive prediction for this outcome. While an increased number of false positives may be predicted with efforts to maximize sensitivity, female athletes predicted to demonstrate both low and high KAM will likely gain improved performance as a serendipitous effect of neuromuscular training targeted to prevent injury risk.
The risk for osteoarthritis in the female ACL injured population ranges from 50 to 100%,(Myklebust and Bahr, 2005) with or without surgical reconstruction of the ligament. This high risk of long term osteoarthritis may be increased in those athletes who demonstrate excessive and repetitive high KAM during participation in sports and who are at increased risk of a knee valgus injury mechanism.(Meyer et al., 2009, Hewett et al., 2005) Accordingly, the prevention of ACL injury is currently the only effective intervention for these life-altering injuries. The high predictive sensitivity and specificity of this single factor points to the necessity to develop specific injury prevention protocols targeted to athletes who demonstrate high KAM, which increases their risk for ACL injury.
Theoretically, through identification of female athletes at greater risk for ACL injury, prevention strategies to reduce an ACL injury could be substantially improved. As mentioned previously, the current non-targeted neuromuscular training programs require application to 89 female athletes to prevent one ACL injury.(Grindstaff et al., 2006) The current clinic-based assessment tool could increase the efficiency of neuromuscular training if it were to be targeted to high KAM female athletes. The results of the current investigation may aid in the dissemination of assessment techniques required for the application of targeted neuromuscular training intervention to high-risk populations. The authors acknowledge that the proposed algorithmic approach may have limited utility to predict injury risk during cutting, pivoting or maneuvers not associated with landing. Future efforts should aim to validate the proposed algorithm using clinic-based measurement techniques to determine the relationship to ACL injury prediction from both cutting and landing injury mechanisms. In addition, further research is warranted to delineate the most efficient training methods to target females who demonstrate high KAM landing mechanics to further improve the potential prophylactic effects.
CONCLUSION
ACL injury leads to significant short-term disability and currently there is no treatment that effectively prevents the long-term debilitation associated with osteoarthritis that follows this injury. Thus, prevention of ACL injuries is crucial. The current study addresses the increased potential to reduce ACL injury and potentially the long term osteoarthritis risk via identification of simple clinical measures that can be used to asses high KAM landing mechanics. Specifically, we have defined clinically obtainable correlates and developed a prediction algorithm that employs these measures to identify female athletes who demonstrate high KAM landing strategies that likely place them at increased risk for ACL injury. The current investigation provides the critical next step to merge the gap between research findings and clinical practices with the presented clinic-based assessment tool. The simplicity and lessened equipment and labor cost associated with utilization of this tool relative to previous techniques to measure high KAM may facilitate the identification of high ACL injury risk athletes on a more widespread basis in clinical and field settings. Implementation of the prediction tool developed in the current study would likely increase both the efficacy and efficiency of prevention strategies for non-contact ACL injury and its widespread use may impact the endemic rise of this physically and financially devastating injury in female athletes.
Clinical Relevance
Utilization of clinically obtainable correlates with the prediction algorithm facilitates high non-contact anterior cruciate ligament injury risk athletes’ entry into appropriate interventions with the greatest potential to prevent injury.
ACKNOWLEDGEMENTS
The authors would like to acknowledge funding support from National Institutes of Health/NIAMS Grants R01-AR049735, R01-AR05563 and R01-AR056259. The authors would like to thank Boone County Kentucky, School District, especially School Superintendent Randy Poe, for participation in this study. We would also like to thank Mike Blevins, Ed Massey, Dr. Brian Blavatt and the athletes of Boone County public school district for their participation in this study. The authors would also like to acknowledge the Sports Medicine Biodynamics Team who worked together to make large data collection sessions possible. Finally, the authors would like to acknowledge Sam Wordeman for his assistance with the use of R-project software and Dr. Mitch Rauh for his helpful advice throughout this investigation. All authors are independent of any commercial funder, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: a 13-year review. Am J Sports Med. 2005;33:524–530. doi: 10.1177/0363546504269937. [DOI] [PubMed] [Google Scholar]
- Andriacchi TP, Natarajan RN, Hurwitz DE. Musculoskeletal Dynamics, Locomotion, and Clinical Applications. In: Mow VC, Hayes WC, editors. Basic orthopaedic biomechanics. 2nd ed. Philadelphia: Lippincott-Raven; 1997. [Google Scholar]
- Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- Boden BP, Dean GS, Feagin JA, Garrett WE. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573–578. doi: 10.3928/0147-7447-20000601-15. [DOI] [PubMed] [Google Scholar]
- Chappell JD, Yu B, Kirkendall DT, Garrett WE. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. Am J Sports Med. 2002;30:261–267. doi: 10.1177/03635465020300021901. [DOI] [PubMed] [Google Scholar]
- Cole GK, Nigg BM, Ronsky JL, Yeadon MR. Application of the joint coordinate system to three-dimensional joint attitude and movement representation: a standardization proposal. J Biomech Eng. 1993;115:344–349. doi: 10.1115/1.2895496. [DOI] [PubMed] [Google Scholar]
- Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35:1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- Ford KR, Myer GD, Hewett TE. Reliability of landing 3D motion analysis: implications for longitudinal analyses. Med Sci Sports Exerc. 2007;39:2021–2028. doi: 10.1249/mss.0b013e318149332d. [DOI] [PubMed] [Google Scholar]
- Ford KR, Myer GD, Smith RL, Vianello RM, Seiwert SL, Hewett TE. A comparison of dynamic coronal plane excursion between matched male and female athletes when performing single leg landings. Clinical Biomechanics. 2006;21:33–40. doi: 10.1016/j.clinbiomech.2005.08.010. [DOI] [PubMed] [Google Scholar]
- Ford KR, Myer GD, Toms HE, Hewett TE. Gender differences in the kinematics of unanticipated cutting in young athletes. Medicine & Science in Sports. 2005;37:124–129. [PubMed] [Google Scholar]
- Grindstaff TL, Hammill RR, Tuzson AE, Hertel J. Neuromuscular control training programs and noncontact anterior cruciate ligament injury rates in female athletes: a numbers-needed-to-treat analysis. J Athl Train. 2006;41:450–456. [PMC free article] [PubMed] [Google Scholar]
- Harrell FE. Regression Modeling Statistics. New York: Springer-Verlag New York, Inc; 2001. [Google Scholar]
- Harrell FE. Regression modeling strategies with application to linear models, logistic regression, and survival analysis. New York: Springer-Verlag; 2002. [Google Scholar]
- Hewett TE, Ford KR, Myer GD. Anterior Cruciate Ligament Injuries in Female Athletes: Part 2, A Meta-analysis of Neuromuscular Interventions Aimed at Injury Prevention. Am J Sports Med. 2006a;34:490–498. doi: 10.1177/0363546505282619. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Ford KR, Myer GD, Wanstrath K, Scheper M. Gender Differences in Hip Adduction Motion and Torque During a Single Leg Agility Maneuver. J Orthop Res. 2006b;24:416–421. doi: 10.1002/jor.20056. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86-A:1601–1608. doi: 10.2106/00004623-200408000-00001. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Myer GD, Ford KR, Heidt RS, Jr, Colosimo AJ, McLean SG, Van Den Bogert AJ, Paterno MV, Succop P. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am J Sports Med. 2005;33:492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- Kernozek TW, Torry MRHVH, Cowley H, Tanner S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005;37:1003–1012. discussion 1013. [PubMed] [Google Scholar]
- Knaus WA, Harrell FE, Fisher CJ, Jr, Wagner DP, Opal SM, Sadoff JC, Draper EA, Walawander CA, Conboy K, Grasela TH. The clinical evaluation of new drugs for sepsis. A prospective study design based on survival analysis. Jama. 1993;270:1233–1241. [PubMed] [Google Scholar]
- Krosshaug T, Nakamae A, Boden BP, Engebretsen L, Smith G, Slauterbeck JR, Hewett TE, Bahr R. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–367. doi: 10.1177/0363546506293899. [DOI] [PubMed] [Google Scholar]
- Malinzak RA, Colby SM, Kirkendall DT, Yu B, Garrett WE. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech. 2001;16:438–445. doi: 10.1016/s0268-0033(01)00019-5. [DOI] [PubMed] [Google Scholar]
- Malone TR, Hardaker WT, Garrett WE, Feagin JA, Bassett FH. Relationship of gender to anterior cruciate ligament injuries in intercollegiate basketball players. Journal of Southern Orthopaedic Association. 1993;2:36–39. [Google Scholar]
- McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech. 2004a;19:828–838. doi: 10.1016/j.clinbiomech.2004.06.006. [DOI] [PubMed] [Google Scholar]
- McLean SG, Lipfert SW, Van Den Bogert AJ. Effect of gender and defensive opponent on the biomechanics of sidestep cutting. Med Sci Sports Exerc. 2004b;36:1008–1016. doi: 10.1249/01.mss.0000128180.51443.83. [DOI] [PubMed] [Google Scholar]
- Meyer EG, Villwock MR, Haut RC. Osteochondral microdamage from valgus bending of the human knee. Clin Biomech (Bristol, Avon) 2009 doi: 10.1016/j.clinbiomech.2009.05.006. [DOI] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Barber-Foss K, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clinical Journal of Sports Medicine. 2008 doi: 10.1097/JSM.0b013e318190bddb. Under Review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009a;19:3–8. doi: 10.1097/JSM.0b013e318190bddb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Brent JL, Hewett TE. The Effects of Plyometric versus Dynamic Balance Training on Power, Balance and Landing Force in Female Athletes. J Strength Cond Res. 2006a;20:345–353. doi: 10.1519/R-17955.1. [DOI] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in "high-risk" versus "low-risk" athletes. BMC Musculoskelet Disord. 2007;8:1–7. doi: 10.1186/1471-2474-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Divine JG, Hewett TE. Specialized dynamic neuromuscular training can be utilized to induce neuromuscular spurt in female athletes. Med Sci Sports Exerc. 2004;36:343–344. [Google Scholar]
- Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Identification of female athletes with high dynamic knee abduction moments during landing: Development and validation of a laboratory based prediction tool. American Journal of Sports Medicine. 2009b Submitted. [Google Scholar]
- Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Development and validation of a clinic based prediction tool to identify high ACL injury risk female athletes. American Journal of Sports Medicine. 2010 doi: 10.1177/0363546510370933. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer GD, Ford KR, McLean SG, Hewett TE. The Effects of Plyometric Versus Dynamic Stabilization and Balance Training on Lower Extremity Biomechanics. Am J Sports Med. 2006b;34:490–498. doi: 10.1177/0363546505281241. [DOI] [PubMed] [Google Scholar]
- Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J Strength Cond Res. 2005;19:51–60. doi: 10.1519/13643.1. [DOI] [PubMed] [Google Scholar]
- Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005;39:127–131. doi: 10.1136/bjsm.2004.010900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012. doi: 10.1177/0363546503261724. [DOI] [PubMed] [Google Scholar]
- Padua DA, Marshall SW, Beutler AI, Garrett WE. Prospective cohort study of biomechanical risk factors of ACL injury: The JUMP-ACL Study. Keystone, CO: American Orthopaedic Society of Sports Medicine Annual Meeting. 2009
- Pappas E, Hagins M, Sheikhzadeh A, Nordin M, Rose D. Biomechanical differences between unilateral and bilateral landings from a jump: gender differences. Clin J Sport Med. 2007;17:263–268. doi: 10.1097/JSM.0b013e31811f415b. [DOI] [PubMed] [Google Scholar]
- Paterno MV, Myer GD, Ford KR, Hewett TE. Neuromuscular training improves single-limb stability in young female athletes. J Orthop Sports Phys Ther. 2004;34:305–317. doi: 10.2519/jospt.2004.34.6.305. [DOI] [PubMed] [Google Scholar]
- Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P, Taylor DC. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med. 2003;31:831–842. doi: 10.1177/03635465030310061801. [DOI] [PubMed] [Google Scholar]
- Winter DA jn. Biomechanics and Motor Control of Human Movement. New York: John Wiley & Sons, Inc; 1990. pp. 91–95. [Google Scholar]
- Zeller BL, Mccrory JL, Kibler WB, Uhl TL. Differences in Kinematics and Electromyographic Activity Between Men and Women during the Single-Legged Squat. Am J Sport Med. 2003;31:449–456. doi: 10.1177/03635465030310032101. [DOI] [PubMed] [Google Scholar]