

Abstract
Background:
Meconium aspiration syndrome (MAS) is still a condition associated with a high mortality, and many patients require extracorporeal membrane oxygenation (ECMO) as rescue therapy. Beneficial effects of surfactant and perflubron lavage have been reported. However, pure surfactant supplementation has not been proven to be beneficial in the most severe forms of MAS. This study was performed to demonstrate an improvement in oxygenation in neonates transferred for ECMO and fulfilling ECMO criteria with a saline lavage and surfactant resupplementation.
Methods:
Twelve newborns with MAS [gestational age 36–40 weeks, mean birth weight 3200 g, age 4–16 h, oxygenation index (OI) > 40] transferred for ECMO therapy were treated with saline lavage (5–10 cm3/kg body weight, as long as green colored retrieval was observed) and resupplementation with bovine surfactant (Alveofact, Boehringer, Ingelheim, Germany). The OI at admission and 3 h after this procedure was compared using the t-test for paired samples. ECMO was available as rescue therapy at all times.
Results:
The OI decreased from 49.4 (SD ± 13.3) to 27.4 (SD ± 7.3), P < 0.01. The decrease was sustained in nine patients, three patients required ECMO and all patients survived.
Conclusions:
As MAS is a condition with parenchymal damage, pulmonary hypertension and obstructive airway disease, no simple causative therapy is possible. Surfactant application after removal of meconium by extensive lavage is feasible as long as 16 h after birth even in infants considered for ECMO therapy; it might reduce the necessity of ECMO.
Keywords: bronchoalveolar lavage, meconium aspiration, neonates, respiratory failure, surfactant
Introduction
Meconium aspiration syndrome (MAS) is a leading cause of severe respiratory failure in term neonates and is associated with high mortality. Extracorporeal membrane oxygenation (ECMO) has improved the outcome of infants with MAS significantly [1]. In addition, the enforcement of standardized management algorithms, with detailed advice for pharyngeal and in some cases tracheal suctioning, have reduced the incidence of MAS, especially in Europe [2,3,4,5,6,7].
In our state, only four cases in 29 000 deliveries were registered in 1997 [8]. In cases of MAS with moderate severity, exogenous surfactant therapy improves oxygenation and increases the rate of survival [9].
Infants are still transferred, however, to ECMO centers after prolonged periods of hypoxemia; in extreme conditions, with oxygenation indices > 40, the transport-associated mortality is high [10]. Treatment options that improve the conditions in severe MAS and can be used in all NICU are therefore warranted.
As MAS is a condition combining pulmonary hypertension and obstructive airway disease with a considerable inflammatory reaction, a simple causative therapy is not possible [2]. Exogenous surfactant has been proven to improve oxygenation in animal models of MAS [11,12].
Clinical observations in severe cases of MAS, however, are contradictory; in general, a marginal improvement in oxygenation has been observed [13,14,15,16,17]. Lavage procedures with either surfactant alone or fluorocarbons have been published as case reports [18,19]. Two cases of successful saline lavage followed by surfactant administration have been reported [20]. We studied this method in a pilot series of 12 patients consecutively admitted with an oxygenation index (OI) > 40. As the calculated mortality in these infants is still 61% without ECMO [1], our institutional review board (IRB) did not allow a clinically controlled study comparing saline lavage followed by surfactant with saline lavage alone or saline lavage plus placebo (placebo material with a high viscosity as surfactant). In addition, the IRB demanded that ECMO had to be available at all times after admission of these patients.
Patients and methods
All neonates admitted to our unit in their first 24h of life with a diagnosis of MAS for evaluation of ECMO therapy were considered suitable for this pilot study if their OI (mean airway pressure × FiO2 × 100/paO2) was > 40 admission. Exclusion criteria were the same as the usual ECMO exclusion criteria, in other words a major congenital malformation such as obvious chromosomal disorders, congenital heart disease (excluded by echocardiography), intracerebral hemorrhage (excluded by cerebral ultrasound) or no informed consent obtainable. All patients were ventilated with the Babylog 8000 (Dräger, Lübeck, Germany), the mean airway pressure was calculated by the ventilator integrated software and arterial blood gases were obtained at admission. Patients were recruited over an 18-month period. The diagnosis of MAS was based on patient's history, typical chest X-rays, and the green colored appearance of tracheal secretions. ECMO was available at all times as a rescue therapy. Informed consent of the custodians was obtained, and the IRB did not have any objections against this study.
Under hand bagged ventilation a bronchoalveolar lavage was performed with 5–10cm3 saline/kg in portions of 3 cm3/kg as long as green colored retrieval was observed (mean 7.7, SD ± 1.6). This procedure had to be performed in a maximum of 3 min; 100 mg/kg bovine surfactant (Alveofact, Thomae, Biberach, Germany) was applied via a 5G feeding tube fed through a bronchoscopy adapter to the bifurcation under continuous hand bagging over a period of 2–3 min. During the procedure, the patients were monitored by electrocardiogram, impedance respirography, blood pressure registration via arterial lines (Sirecust 404 N, Siemens, Erlangen, Germany) and pulse oximetry (Dräger Oxisat 2, Dräger, Lübeck, Germany). Arterial blood gases were again obtained 3 h after the procedure. The oxygenation indices before and after the lavage/surfactant resupplementation procedure were compared using the t-test for paired samples. The primary endpoint of this study was to observe a significant decrease in the OI 3 h after the lavage/surfactant resupplementation procedure. P < 0.05 was accepted as the level of significance. We calculated a sample size of 10 to achieve this level of significance with a β error of 5%, if the decrease in OI was > 20%.
The number of patients requiring ECMO in the further course of their disease was documented. Venoarterial ECMO was started if the OI was > 40 for 8 h or the paO2< 35 for 2 h.
In all patients, a ventilatory strategy based on the concept of low tidal volume ventilation was followed after the procedure. A lowest arterial pH of 7.2, paO2 of 45 and SaO2 of 85% were acceptable. For hemodynamic stabilization dopamine, dobutamine, epinephrine, and norepinephrine were used to keep the mean arterial blood pressure > 45mmHg, the heart rate between 140 and 200 beats/min, and maintain urinary output at 1 cm3/kg per h.
All patients were followed in our neurodevelopmental clinics over a 12-month period. Secondary endpoints were taken as the survival rate compared with the UK-ECMO trial [1], the rate of infants requiring ECMO, and the rate of intact survival (no oxygen and no major neurological handicaps at 1 year of age).
Results
We included 12 neonates with MAS transferred from outside centers for evaluation of ECMO therapy in our study (Table 1). The mean oxygenation index decreased significantly from 49.4 (SD ± 13.3) before the lavage/surfactant supplementation procedure to 27.4 ± 7.3 after the procedure (P < 0.01, t-test for paired samples; Fig 1). The oxygenation index 1h after the procedure was 38.6 ± 8.9 and was not significantly different.
Table 1.
Characteristics of the 12 infants studied
| Mean birth weight (± SD) | 3200 g (± 444) |
| Mean gestational age (range) | 38.8 weeks (36–42) |
| Mean 5-min APGAR (range) | 6.4 (4–9) |
| Girls/boys | 7/5 |
| c-sections/vaginal deliveries | 2/10 |
APGAR, American Pediatric Gross Assessment Record.
Figure 1.
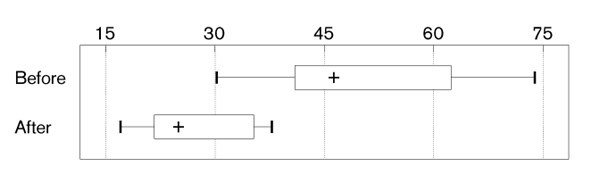
Oxygenation index (mean airway pressure×FiO2 ×100/paO2) beforeand after saline lavage and surfactant resupplementation in 12 neonates (mean 75th and 97th percentile).
The improvement in oxygenation was sustained in nine patients; in other words, no secondary increase of OI was observed (OI in these patients 48 h after the procedure 19.2 ± 3.1). All of these could be weaned off ventilation (time on ventilator: 6-17 days) and were discharged home without oxygen supplementation. The improvement in oxygenation was reflected in the clearing of infiltrates on chest X-rays at day 2 after the procedure (Figs 2 and 3). In three patients the initial improvement of OI was not sustained; these were treated with venoarterial ECMO, weaned successfully and discharged home without oxygen supplementation. ECMO was started in these three patients 7, 7.5, and 11 h after the lavage/surfactant procedure.
Figure 2.
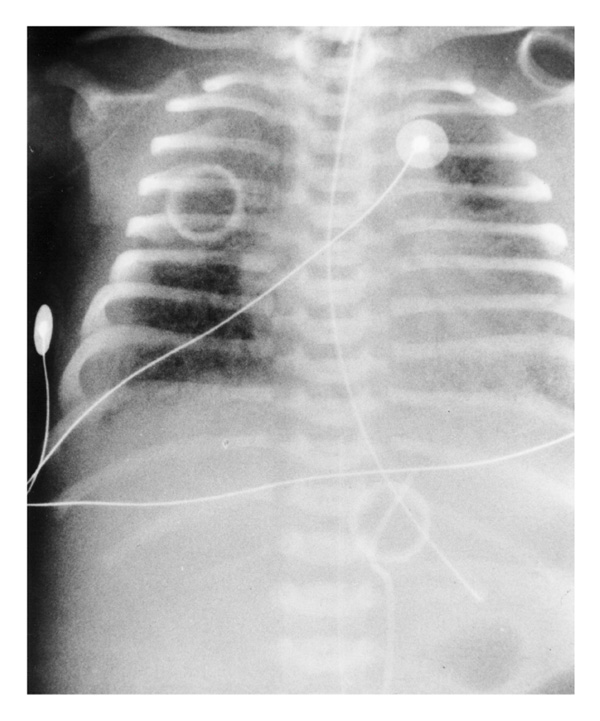
Chest X-ray in one patient at admission, demonstrating features of meconium aspiration.
Figure 3.
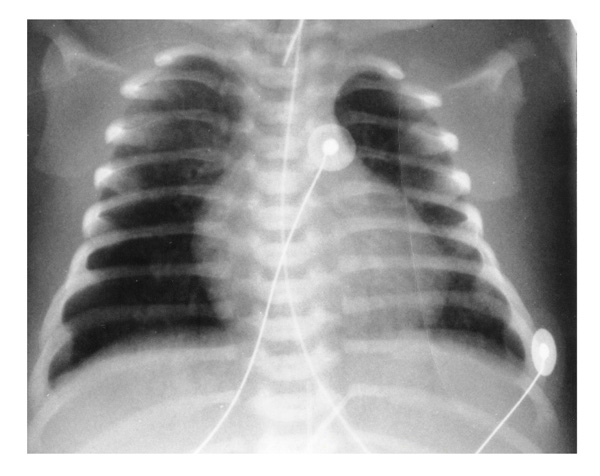
Chest X-ray 2 h after lavage/surfactant procedure in the same patient as in Fig 1, showing clearing of infiltrate.
No late deaths were registered (observation time 12 months). The lavage/hand bagging/surfactant administration procedure did not cause pneumothoraces or cardiac arrests. Bradycardia (< 80 beats/min) lasting less than 30 s was observed in all patients.
In neurodevelopmental follow-up clinics, none of the 12 patients exhibited signs of severe neurological complications; the neurodevelopmental delay was 4 months at the age of 12 months in one patient, the others had a normal neurodevelopmental examination.
Discussion
MAS is the leading cause of respiratory failure in term neonates and the major indication for ECMO therapy [1]. Prophylaxis by enforcement of standard suctioning procedure (vigorous pharyngeal followed by tracheal suctioning in infants with continued respiratory distress) in all obstetric units has not been very successful [2]. ECMO is a very successful therapy for MAS that was previously associated with a high mortality [1]; however, many infants still succumb before, during, and shortly after transport to ECMO centers [10]. Surfactant to treat MAS should be available in all level I and II neonatal facilities as it has been shown to be successful in resuscitation after meconium aspiration in two cases [20].
In animal models of MAS a beneficial effect of surfactant therapy has been demonstrated [11,12,18,21,22]. This was attributed to the anti-inflammatory, alveolar recruiting, and pulmonary vasodilatative effect of surfactant [16, 21,22,23,24,25]. Clinical studies, however, lead to very contradictory, predominantly discouraging results [13,14,16,21,24, 25]. This might be because of the fact that, until recently, surfactant preparations had a high viscosity that made it unsuitable for lavage and caused airway obstruction in these patients with an already underlying obstructive airway disease. Our group has observed these difficulties in surfactant treatment studies in acute respiratory distress syndrome (ARDS) in infants and children, where the initial trials caused a sudden deterioration of the oxygenation after surfactant bolus application [26]. A recent clinical controlled study of surfactant therapy in term infants including a considerable number of patients after meconium aspiration could demonstrate a significant improvement in oxygenation after surfactant use; however, these infants with a mean OI of 25 were suffering only from moderate MAS [9]. This group of patients in our region has a mortality of < 15% and is therefore not comparable with the patient group we studied [8,26]. Initial reports using fluorocarbons for lavage and alveolar recruitment in MAS patients have been published [19].
In our study, we followed a protocol based on quick saline lavage followed by surfactant resupplementation to overcome these difficulties. As a controlled study comparing surfactant with a placebo of the same high viscosity causing airway obstruction in this patient population with a mortality > 60% [1] was not acceptable for our IRB, we tried to overcome a selection bias by including at least all consecutively admitted neonates with MAS and an OI > 40 to our institution over a 2-year period. This pilot study showed a marked improvement in oxygenation in MAS patients. The need for ECMO was low; in the UK-ECMO study all patients would have been suitable for ECMO therapy. However, as the overall number of patients evaluated was small, the power of this study to prove a decrease in ECMO necessity was low (β error 10%). In addition, it has to be borne in mind that the conclusion of Wiswell et al [2] in 1990 that we had made no difference in MAS might no longer be true. Standard treatment protocols, nitric oxide, and occasional surfactant application have lowered the number of patients requiring ECMO recently [8,17].
We would conclude from our pilot study that saline lavage followed by surfactant application in MAS patients is feasible and improves oxygenation; it might lower the need for ECMO or reduce the transport-related mortality in neonates with MAS, which exceeds 25% in a study based in Germany [28].
Its value in comparison with fluorocarbons and new reconstituted surfactant preparations with a lower viscosity has to be studied in the future. The latter might be used as lavage fluid alone and be beneficial as a simple therapeutic agent comparable with the indication in term infants with respiratory failure with a lower OI [9].
References
- UK Collaborative ECMO Trial Group UK collaborative randomised trial of neonatal extracorporeal membrane oxygenation. Lancet. 1996;348:75–82. [PubMed] [Google Scholar]
- Wiswell TE, Tuggle JM, Turner BS. Meconium aspiration syndrome: have we made a difference? Pediatrics. 1990;85:715–721. [PubMed] [Google Scholar]
- Greenough A, Emery E. ECMO and outcome of mechanical ventilation in infants of birthweight over 2 kg. Lancet. 1990;ii:360. doi: 10.1016/0140-6736(90)92264-i. [DOI] [PubMed] [Google Scholar]
- Wiswell TE, Henley MA. Intratracheal suctioning, systemic infection, and the meconium aspiration syndrome. Pediatrics. 1992;89:203–206. [PubMed] [Google Scholar]
- Bull DH, Sola A, Wakeley A. Meconium and tracheal aspiration. Pediatrics. 1992;90:474. [PubMed] [Google Scholar]
- Cunningham AS, Lawson EE, Martin RJ, Pildes RS. Tracheal suction and meconium: a proposed standard of care. J Pediatr. 1990;117:153–154. doi: 10.1016/s0022-3476(05)81670-1. [DOI] [PubMed] [Google Scholar]
- Goetzman BW. Meconium aspiration. Am J Dis Child. 1992;146:1282–1283. doi: 10.1001/archpedi.1992.02160230040012. [DOI] [PubMed] [Google Scholar]
- Neonatalerhebung Schleswig-Holstein Bad Segeberg, Germany: Arztekammer Schleswig -Hoistein; 1996.
- Lotze A, Mitchell BR, Bulas DI, Zola EM, Shalwitz RA, Gunkel H. Multicenter study of surfactant use in the treatment of term infants with severe respiratory failure. J Pediatr. 1998;132:40–47. doi: 10.1016/s0022-3476(98)70482-2. [DOI] [PubMed] [Google Scholar]
- Möller JC, Schaible TF, Reiss I, Gortner L. High mortality in children with respiratory failure transferred for novel therapies (NO, Surfactant, ECMO) related to transport: necessity to enforce 'in time referrals'. 5th European Congress of Extracorporeal Life Support. Stockholm.1997. pp. 37–38.
- Sun B, Curstedt B, Robertson B. Surfactant inhibition in experimental meconium aspiration. Acta Paediatr. 1993;82:182–189. doi: 10.1111/j.1651-2227.1993.tb12635.x. [DOI] [PubMed] [Google Scholar]
- Sun B, Herting E, Curstedt B, Robertson B. Exogenous surfactant improves lung compliance and oxygenation in rats with meconium aspiration. . J Appl Physiol. 1994;77:1961–1971. doi: 10.1152/jappl.1994.77.4.1961. [DOI] [PubMed] [Google Scholar]
- Blanke JG, Jorch G. Surfactanttherapie bei 10 Neugeborenen mit Mekonium- aspirationssyndrom. Klin Pädiatr. 1993;205:75–78. doi: 10.1055/s-2008-1034531. [DOI] [PubMed] [Google Scholar]
- Brehmer U, Jorch G. Surfactanttherapie bei 41 Frühgeborenen < 34.SSW. mit Verdacht auf konnatale Infektionen. Klin Pädiatr. 1993;205:78–82. doi: 10.1055/s-2008-1034532. [DOI] [PubMed] [Google Scholar]
- Findlay RD, Taeusch HW, Walther FJ. Surfactant replacement therapy for meconium aspiration syndrome. Pediatrics. 1996;97:48–52. [PubMed] [Google Scholar]
- Halliday HL, Speer CP, Robertson B. Treatment of severe meconium aspiration syndrome with porcine surfactant. Eur J Pediatr. 1996;155:1047–1051. doi: 10.1007/BF02532529. [DOI] [PubMed] [Google Scholar]
- Lachmann B, Gommers D. Surfactant treatment for neonatal lung disease other than the idiopathic respiratory distress syndrome. Lung Respir. 1994;11:35–39. [Google Scholar]
- Paranka MS, Walsh F, Stancombe BB. Surfactant lavage in a piglet model of meconium aspiration syndrome. Pediat Res. 1992;31:625–628. doi: 10.1203/00006450-199206000-00017. [DOI] [PubMed] [Google Scholar]
- Mararo G, Bonati M, Ferrari A, Pagani C, Galibati A. A comparison of perflourocarbone with saline solution for bronchoalveolar lavage in experimental meconium aspiration. Cardiology of the Young . 1995;5 (suppl 2):9. [Google Scholar]
- Mosca F, Colnaghi M, Castoldi F. Lung lavage with a saline volume similar to functional residual capacity followed by surfactant administration in newborns with severe meconium aspiration syndrom. . Intensive Care Med. 1996;22:1412–1413. doi: 10.1007/BF01709561. [DOI] [PubMed] [Google Scholar]
- Herting E, Sun B, Harms K, et al. Surfactant Behandlung bei Mekoniumaspiration: Widerspruch tierexperimenteller und klinischer Ergebnisse? Z Geburtsh Neonatol. 1995;199:210. [Google Scholar]
- Cleary GM, Antunes MJ, Ciesielka DA, Higgins ST, Spitzer AR, Chander A. Exudative lung injury is associated with decreased levels of surfactant proteins in a rat model of meconium aspiration. . Pediatrics. 1997;100:998–1003. doi: 10.1542/peds.100.6.998. [DOI] [PubMed] [Google Scholar]
- Duncan JE, Hatch G, Belik J. Is surfactant a pulmonary vasodilator? Pediatr Res. 1994;35:223A. [Google Scholar]
- Möller JC. Surfactanttherapie beim akuten Atemnotsyndrom. In Wauer RR (editor) Surfactanttherapie Thieme: Stuttgart; 1997. pp. 133–146.
- Herting E. Surfactanttherapie bei neonataler Pneumonie und beim Mekonium-aspirationssyndrom. In Wauer RR (editor) Surfactant-therapieThieme:Stuggart; 1997. pp. 124–132.
- Möller JC, Schaible TF, Reiss I, Artlich A, Gortner L. Treatment of severe non-neonatal ARDS in children with surfactant and nitric oxide in a 'pre ECMO' situation. Int J Artif Organs. 1995;18:598–602. [PubMed] [Google Scholar]
- Ito Y, Kawano T, et al. Alternative treatment may lower the need for use of extracorporeal membrane oxygenation. Acta Paediat Jpn. 1996;36:673–677. doi: 10.1111/j.1442-200x.1994.tb03268.x. [DOI] [PubMed] [Google Scholar]
- Möller JC, Reiss I, Kohl M, Ahrens P, Gortner L. Treatment of severe meconium aspiration syndrome with saline lavage and surfactant resupplementation. Intensive Care Med. 1997;23 (suppl 1):S15. [Google Scholar]