

Abstract
Background:
A helium-oxygen gas mixture (heliox) has low gas density and low turbulence and resistance through narrowed airways. The effects of heliox on pulmonary mechanics following severe methacholine-induced bronchospasm were investigated and compared to those of a nitrogen-oxygen gas mixture (nitrox) in an innovative pediatric porcine, independent lung, mechanical ventilation model.
Results:
All of the lungs showed evidence of severe bronchospasm after methacholine challenge. Prospective definition of 'heliox response' was a 15% or greater improvement in lung function in the lung receiving heliox compared with the matched lung receiving nitrox. Seven out of 10 pigs responded to heliox therapy with respect to resistance and eight out of 10 pigs responded to heliox therapy with respect to compliance and tidal volume (P < 0.03). After crossover from nitrox to heliox, eight out of eight lungs significantly improved with respect to tidal volume, resistance and compliance (P < 0.001). After crossover from heliox to nitrox all eight lungs showed a significant increase in resistance and a significant decrease in tidal volume (P < 0.001).
Conclusions:
In a pediatric porcine model of acute, severe methacholine-induced bronchospasm and independent lung mechanical ventilation, administration of heliox improves pulmonary mechanics, gas flow, and ventilation. Administration of heliox should be considered for support of pediatric patients with acute, severe bronchospasm requiring mechanical ventilation through small artificial airways.
Keywords: asthma, bronchospasm, heliox, helium, independent lung ventilation, mechanical ventilation
Introduction
In 1935, Barach first advocated helium-oxygen gas mixtures (heliox) as a therapy for obstructive lesions of the airway [1]. Since then, heliox has been shown to be efficacious in the treatment of various disease entities involving narrowed airways [2,3,4,5,6,7,8]. Its safety has been demonstrated in both mechanically ventilated and spontaneously breathing patients [7]. Combining 70% helium and 30% oxygen results in a gas which is much less dense than a nitrogen-oxygen gas mixture (nitrox) and has approximately the same viscosity [1]. The therapeutic effects of heliox gas mixtures are believed to relate to its ability to deliver oxygen and gas flow with less turbulence and resistance through narrowed airways. Since airway resistance is directly proportional to the density of the gas, the administration of heliox is expected to improve ventilation by decreasing resistance, reducing turbulence and promoting laminar gas flow.
Although there have been advancements in the treatment of asthma since Barach first studied heliox in 1935, mortality continues to increase [9]. The use of bronchodilators and anti-inflammatory agents have become the standard of care for reactive airway disease and asthma. However, some patients fail to respond to aggressive therapy and require mechanical ventilation. Mechanical ventilation may result in turbulent gas flow secondary to high gas velocity which may cause additional difficulty achieving adequate ventilation. Heliox may, therefore, be most effective in intubated patients with severe bronchospasm and small diameter airways by decreasing turbulent flow, improving ventilation and limiting barotrauma while therapies targeted to the underlying etiology of the bronchospasm are given time to achieve their effect.
Several animal and human studies have investigated the effects of heliox on pulmonary function [10,11,12,13,14]. Although results from these studies have been promising, the wide variation between each patient's biological response to bronchospasm make many of these results difficult to interpret. We have developed a pediatric porcine, independent lung ventilation model of severe bronchospasm which allows one of the animal's lungs to act as a simultaneous control for the contralateral lung. This unique model allows each subject to act as its own control during the same bronchospastic event, thereby minimizing influence from various systemic variable biological responses to acute stress and eliminating the need to compare matched control subjects or different bronchospastic events in the same animal. Our hypothesis is that, during mechanical ventilation, the low density heliox gas mixture will increase flow through constricted airways and improve pulmonary mechanics in the lung receiving heliox compared to the lung receiving nitrox.
Methods and materials
This study was approved by the Institutional Review Board at the Alfred I. duPont Institute of the Nemours foundation. Thirteen pre-adolescent Yucatan swine (9.0 ± 1.7 kg) were pre-anesthetized with 500 mg pentobarbital intramuscularly. Peripheral hydration was maintained with 10% Dextrose in water at 4 ml/kg per h. Following placement of continuous monitors for heart rate, electrocardiogram (ECG), respirations, and oxygen saturation, 150 mg (15 mg/kg) pentobarbital was given intravenously.
Each pig was initially intubated with a 5.0mm cuffed endotracheal tube and mechanically ventilated with a time cycled, pressure limited ventilator [peak inspiratory pressure (PIP) 18 cmH2O, positive end-expiratory pressure (PEEP) 5 cmH2O, rate 30 breaths/min, inspiratory to expiratory ratio (I/E) 1:1, fractional inspiratory oxygen concentration (FiO2) 30%]. Central arterial and venous catheters were placed by femoral cutdown for continuous monitoring of heart rate, blood pressure and blood sampling. A tracheostomy was then performed and, immediately after removal of the initial endotracheal tube, separate cuffed 3.0 endotracheal tubes (16 cm in length) were placed through the tracheostomy stoma into the right and left mainstem bronchi. Correct placement of each endotracheal tube was verified by auscultation during independent ventilation and later confirmed by bronchoscopy and/or autopsy. Additional doses of pentobarbital were given to ensure adequate anesthesia (titrated to achieve a heart rate of < 160 beats/min, systolic blood pressure ≤ 140 mmHg, and absence of withdrawal to painful stimuli).
Each lung was independently mechanically ventilated (BP 200, Bear Medical Systems, Riverside, California, USA) simultaneously with identical settings. Pulmonary function tests (PFTs) were recorded for each lung at baseline while on heliox and nitrox using an infant/pediatric pulmonary function computer (PeDS, Medical Associated Services, Inc., Hatfield, Pennsylvania, USA), calibrated for the gas mixture being delivered to derive tidal volume, resistance and compliance. Airflow data were obtained by a Fleisch 0 (Pediatric) tachometer (OEM Medical, Richmond, Virginia, USA). Transpulmonic pressure was measured by a differential pressure transducer with an esophageal balloon. While ventilating both lungs with nitrox, methacholine (10 mg/ml × 1.5ml diluted to 3 ml with buffer) was aerosolized continuously to both lungs simultaneously over 3 min until airway resistance of each lung at least doubled from baseline. One lung was then randomized to receive nitrox and the other to receive heliox. FiO2 was not adjusted to either lung, but remained at 30% throughout the experiment. Pulmonary function testing was performed every 2 min, alternating lungs until the resistance of one lung returned to within 15% of baseline or until 16 min had elapsed. As approximately 2 min was required to complete each pulmonary function assessment and because of differences in calibration between the two gases used, right and left lung PFTs were not obtained simultaneously. Therefore, the order for each lung to be tested was determined randomly and data were compared by pulmonary function assessment number. Results of PFTs obtained at 2 min and 4 min are reported as assessment number 1; the results of PFTs performed at 6 min and 8 min are reported as assessment number 2; the results of PFTs performed at 10 and 12 min as assessment number 3; and the results of PFTs performed at 14 and 16 min as assessment number 4. The maximum number of PFTs performed for each lung was four per lung. In eight out of 10 piglets, the lung gases were then switched and PFTs were measured in each lung after 2 min. (The protocol was expanded to include the crossover after the first two piglets had been studied, and three piglets could not be evaluated due to severe cardiopulmonary compromise requiring medication intervention during induction of bronchospasm.) To correct for differences between right and left lungs in absolute values of tidal volume, resistance and compliance following induced bronchospasm, outcome variables are expressed as % improvement from the parameters recorded immediately after bronchospasm. A deterioration of lung function was assigned a negative number. Percentage improvement in tidal volume, resistance and compliance after crossover were compared to the measurement immediately before crossover of gases (heliox to nitrox or nitrox to heliox). Upon completion of the study, animals were humanely euthanized using intravenous pentobarbital, 15 mg/kg and KCl, 2 mEq/kg (see timeline, Fig. 1).
Figure 1.
Timeline for study. Following documentation of severe bronchospasm, lungs were randomized to receive either a helium-oxygen gas mixture (heliox) or a nitrogen-oxygen gas mixture (nitrox). The order in which each lung received pulmonary function tests (PFTs) was also randomized.
Statistical analysis
A Student t test was used to compare lung resistance, compliance and tidal volume at baseline (pre-bronchospasm), after methacholine induction of bronchoscopy and after crossover. In addition, 'heliox response' was prospectively defined as a greater than 15% improvement in resistance of the heliox lung compared to the nitrox lung. Using this definition, if there were no effect of heliox on resistance, we would expect no 'heliox responders'. Fisher's exact test was used to compare responders versus non-responders. A P value < 0.05 was considered to be significant. Measured outcome variables were resistance, dynamic compliance and tidal volume.
Results
Thirteen swine were anesthetized and enrolled. Ten out of 13 pigs completed the study without deviation from the protocol. Two pigs became severely hypoxemic and dysrhythmic and required resuscitation before administration of methacholine was completed and data from one pig was eliminated secondary to failure of the pulmonary function apparatus. There were no significant differences found between the two groups with respect to pulmonary function at baseline before bronchospasm or immediately following methacholine challenge. Successful methacholine-induced bronchospasm was documented by a significant deterioration of all pulmonary function parameters studied (tidal volume, resistance and compliance). The mean ± SD resistance measured after methacholine challenge was 425 ± 234 cm/H2O/l/s for the lungs randomized to receive heliox and 305 ± 199 cmH2O/l/s for the lungs randomized to receive nitrox (difference not significant). The mean ± SD compliance measured after induction of bronchospasm was for the heliox 0.15 ± 0.14 ml/cmH2O/kg group and 0.23 ± 0.14 ml/cmH2O/kg for the nitrox group (difference not significant). The mean ± SD tidal volume measured after induction of bronchospasm was 1.9 ± 1.8 ml/kg for the heliox group and 2.8 ± 1.8 ml/kg for the nitrox group (difference not significant).
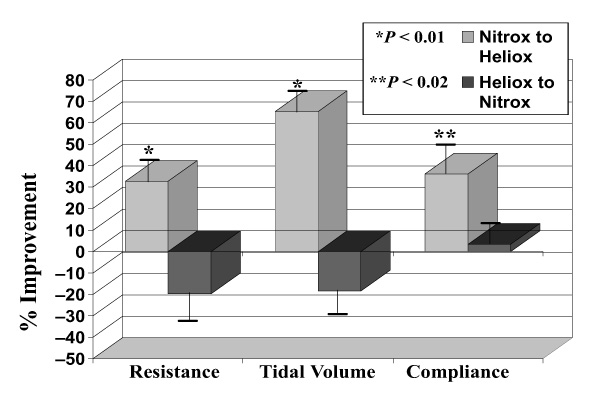
Table 1 demonstrates the number of heliox 'responders' at each time point measured, including after each lung was crossed over from nitrox to heliox. Figure 2 shows the percent improvement of each parameter measured after the gases were switched from heliox to nitrox and from nitrox to heliox. Eight out of 10 subjects had pulmonary function parameters recorded after the gases delivered to each lung were crossed over. All eight subjects showed an improvement in resistance of greater than 15% after crossover from nitrox to heliox. In addition, all lungs crossed over from heliox to nitrox showed a deterioration of resistance and tidal volume of greater than 15%. The mean ± SD improvement in resistance after crossover from nitrox to heliox was 32.6 ± 14.4% compared with -19.8 ± 20.3% after crossover from heliox to nitrox (P < 0.001). Eight out of eight pigs met prospectively defined criteria for a positive 'response' to heliox therapy with respect to tidal volume and seven out of eight pigs met prospectively defined criteria for a positive 'response' with respect to compliance after crossover from nitrox to heliox. The mean ± SD compliance and tidal volume change after crossover from nitrox to heliox was 36.2 ± 20.3% and 65.2 ± 19.1%, respectively, compared with only 3.4 ± 20.3% and -18.4 ± 14.5%, respectively, after crossover from heliox to nitrox (P < 0.001).
Table 1.
The number of helium-oxygen gas mixture (heliox) 'responders' for tidal volume, compliance and resistance for each performed including pulmonary function tests after crossover.
| Assessment | |||||
| 1 | 2 | 3 | 4 | CO | |
| Tidal Volume | 8/10* | 8/10* | 8/10* | 8/10* | 8/8* |
| Resistance | 7/10* | 6/10 | 5/10 | 8/10* | 8/8* |
| Compliance | 8/10* | 7/10* | 7/10* | 2/10 | 7/8* |
CO, positive response after crossover from a nitrogen-oxygen gas mixture (nitrox) to heliox. Note only eight piglets were crossed over. *P < 0.05.
Figure 2.
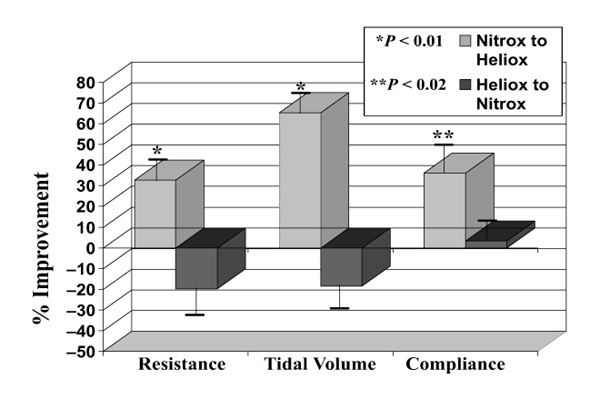
Percentage improvement of resistance, tidal volume and compliance after lungs were crossed over from a nitrogen-oxygen gas mixture (nitrox) to a helium-oxygen gas mixture (heliox) and from heliox to nitrox. A negative percentage improvement indicates a deterioration of lung function, i.e. an increase in resistance is depicted as a negative percentage improvement.
Discussion
Since Barach first described heliox as an effective treatment for diseases involving airway obstruction, there have been many studies performed in both animals and humans examining its effectiveness [10,11,12,13,14,15,16]. Although heliox has been used safely for many years in the pediatric population for the treatment of severe croup and upper airway obstruction [2,3,4,5,6,7], it has been an uncommon treatment for severe bronchospasm. The success of bronchodilators and anti-inflammatory agents as well as inconsistent results in clinical studies have resulted in limited application of heliox in the mechanically ventilated critically ill child. The complex pathophysiology of asthma and the variability of disease between patients and their response to therapy makes the study of a single agent during acute, severe bronchospasm difficult to extrapolate to the clinical setting.
Studies have shown a variable response to heliox therapy in spontaneously breathing patients with severe bronchospasm. It has been suggested that this variability may be due to the greater effectiveness of heliox in patients with predominately large airway disease [10,11,12,14,17,18,19]. Studies of heliox involving mechanically ventilated patients with severe bronchospasm are promising [8,15,16]. The beneficial effects demonstrated in these studies may be due to the decreasing turbulence of bulk gas flow with heliox during mechanical ventilation.
In mechanically ventilated patients with severe bronchospasm, the improvement in ventilation during heliox therapy may be due to the mechanism by which low density gases affect ventilation. Heliox and other low density gases decrease turbulent gas flow by lowering the Reynolds number. The Reynolds number is measured by the product of the gas velocity, airway diameter, and gas density divided by viscosity [16]. It is a unitless number that predicts whether flow is turbulent or laminar. For a given set of airway dimensions, turbulent flow results in a higher resistance than laminar flow. In addition, mechanical ventilation may further complicate the management of acute severe asthma by delivering a gas with increased velocity through a narrow endotracheal tube, particularly in pediatric and neonatal patients. This increases the Reynolds number, which indicates greater turbulent flow and airway resistance. Adequate ventilation in mechanically ventilated patients with severe bronchospasm may be more dependent on the density of the gas than in spontaneously breathing patients.
Several studies have examined the efficacy of heliox in mechanically ventilated patients with severe bronchospasm or other diseases involving narrowed airways [8,15,16]. Although these studies are small and have not included children, the results have been promising. In 1990, Gluck et al. [15] reported an immediate and significant improvement in seven intubated patients with severe bronchospasm and respiratory acidosis. All seven patients showed a significant improvement in pCO2 within 20min and six out of the seven patients showed a significant decrease in mean airway pressure during volume-limited ventilation.
The independent lung ventilation model of acute, severe bronchospasm used in this study is unique in that it allows each animal's contralateral lung to represent its own control. It eliminates the need to monitor systemic arterial blood gases, global circulating mediator or hormone levels and assures that the systemic milieu is identical for comparison of gross outcome measures. It is recognized that the model is limited in its ability to monitor and control local microcirculation. This model controls for the variable macrocirculatory responses to methacholine (e.g. hemodynamic status: heart rate, blood pressure, temperature, circulating epinephrine level) between subjects and allows comparisons of pulmonary mechanics on heliox versus nitrox gas mixtures within the same animal and during the same bronchospastic event. This model allows for a clear determination of response to heliox without the variable biological responses which may affect studies involving separate subjects or different bronchospastic events within the same subject as controls. It uses the same small (3.0) sized endotracheal tubes that might be expected to clinically increase resistance to gas flow in small infants. A 15% difference in pulmonary function between the lung receiving heliox and the lung receiving nitrox (control) was prospectively selected as the primary outcome variable suggesting a favorable response to heliox versus nitrox. It is recognized that lung function measurements in human subjects can be very variable and affected by many factors. Although the coefficient of variation is extremely small when calibrating the PFT machine (Fleisch pneumotach) using known standards within the physiologic ranges encountered in this study, patient factors can introduce intra- and intersubject variability [20]. For this reason, the calibrated PFT computer (calibrated both to 70%N/30% O and 70%He/30% O) was applied serially over a relatively short time span (30 min) and relative improvement/deterioration rather than absolute raw numbers were selected as the primary outcome measures to be compared. In addition, a 15% improvement in PFTs is generally accepted as clinically significant and is well beyond the coefficient of variance for the PFT computer and pneumotachometer when calibrated to a known standard on nitrox or heliox gas mixture.
Of particular interest was the dramatic improvement in resistance and tidal volume in all lungs after crossover from nitrox to heliox. Conversely, there was a statistically significant deterioration in PFTs for all parameters studied after crossover from heliox to nitrox. Even the subjects who did not appear to be responding to heliox therapy still showed a significant and immediate deterioration in pulmonary function when switched to nitrox.
The results of this study suggest that heliox may be effective in improving pulmonary mechanics in patients with small endotracheal tubes being mechanically ventilated for severe bronchospasm. These results also indicate that the response to heliox is potentially rapid and persistent during heliox ventilation.
Although the pediatric porcine model of independent mechanical ventilation and methacholine-induced bronchospasm used in this study is unique and offers many strengths, we acknowledge the limitations of this study. Limitations include the small number of subjects, wide variability in lung response to methacholine challenge and inability to accurately discriminate between the effect of a lower density gas on the resistance generated by the endotracheal tube, large and small airways. In addition, anesthetic agents may effect pulmonary function. Pentobarbital was chosen for this study because of its minimal effects on pulmonary mechanics compared to inhalation or alternative intravenous agents. No arterial blood gases were reported because heliox and nitrox gas mixtures were given to separate lungs simultaneously and therefore systemic arterial blood gases would not reflect unilateral lung function or microenvironment. The assessment of right and left independent pulmonary venous blood gases, although potentially useful, was beyond the scope of this pilot protocol. However, documentation of the severity of bronchospasm was confirmed by at least a 50% increase in total lung resistance in each lung, prior to the start of the experimental therapy. Percent improvement from baseline after bronchospasm was prospectively selected for outcome analysis instead of comparison of raw values for lung resistance and compliance because of recognition during pilot studies of wide variability between individual piglets right and left lung baseline lung resistance values after methacholine challenge. The crossover technique and the desire to use the fewest piglets possible to demonstrate a treatment effect dictated prospective use of the percentage improvement compared to baseline bronchospasm.
Conclusion
In a pediatric porcine model of independent lung mechanical ventilation and severe methacholine-induced bronchospasm, heliox improved pulmonary mechanics when compared to a nitrogen-oxygen gas mixture during mechanical ventilation at identical ventilator settings. This study also indicates that most subjects responded to heliox within the first 4min of therapy and that this response was sustained for at least 20 min. The authors speculate that heliox may be beneficial to critically ill children requiring mechanical ventilation with small endotracheal tubes secondary to severe bronchospasm and high airway resistance with low compliance. In these patients, heliox may be expected to improve tidal volume, lung compliance and resistance and decrease potential ventilator barotrauma while waiting for etiologic targeted therapies to take effect.
Acknowledgments
Acknowledgments
The authors would like to thank Susan Buck, Behzad Taghizadeh, Bill Hofmann, Patty Resnik, Tina Hurst, David Corddry, Ellen Deutsch, Brett Goudie, and Ilene Sivakoff for their assistance and support in completing this project.
References
- Barach A. The use of helium in the treatment of asthma and obstructive lesions in the larynx and trachea. Ann Int Med. 1935;9:739–765. [Google Scholar]
- Jordan W, Graves C, Elwyn R. New therapy for postintubation laryngeal edema and tracheitis in children. JAMA. 1970;212:585–588. [PubMed] [Google Scholar]
- Ishikawa S, Segal M. Re-appraisal of helium-oxygen therapy on patients with chronic lung disease. Ann Allergy. 1973;32:536–542. [PubMed] [Google Scholar]
- Duncan P. Efficacy of helium-oxygen gas mixture in the treatment of severe viral and post-extubation croup. Can Anaesth Soc J. 1979;26:206–212. doi: 10.1007/BF03006983. [DOI] [PubMed] [Google Scholar]
- Houck J, Keamy M, McDonough J. Effect of helium concentration on experimental upper airway obstruction. Ann Otol Rhinol Laryngol. 1990;99:556–611. doi: 10.1177/000348949009900712. [DOI] [PubMed] [Google Scholar]
- Kemper K, Ritz R, Benson M, Bishop M. Helium-oxygen mixture in the treatment of post-extubation stridor in pediatric trauma patients. . Crit Care Med. 1991;19:356–359. doi: 10.1097/00003246-199103000-00013. [DOI] [PubMed] [Google Scholar]
- Wolfson MR, Bhutani VK, Shaffer TH, Bowen FW. Mechanics and energetics of breathing helium in infants with bronchopulmonary dysplasia. . J Pediatr. 1984;104:752–757. doi: 10.1016/s0022-3476(84)80961-0. [DOI] [PubMed] [Google Scholar]
- Kass JE, Castriotta RJ. Heliox therapy in acute severe asthma. Chest. 1995;107:757–760. doi: 10.1378/chest.107.3.757. [DOI] [PubMed] [Google Scholar]
- Robin E. Death from bronchial asthma. Chest. 1988;93:614–618. doi: 10.1378/chest.93.3.614. [DOI] [PubMed] [Google Scholar]
- Chan-Yeung M, Abboud R, Ysao MS, Maclean L. Effect of helium on maximal expiratory flow in patients with asthma before and during induced bronchoconstriction. Am Rev Respir Dis. 1976;106:433–443. doi: 10.1164/arrd.1976.113.4.433. [DOI] [PubMed] [Google Scholar]
- Mink SN, Wood LDH. How does HeO2 increase maximum expiratory flow in human lungs? J Clin Invest. 1980;66:720–729. doi: 10.1172/JCI109909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss J, McFadden E, Ingram R. Bronchodilation, lung recoil, and density dependence of maximal expiratory flow. J Applied Physiol. 1982;52:874–878. doi: 10.1152/jappl.1982.52.4.874. [DOI] [PubMed] [Google Scholar]
- Christopherson S, Hlastala M. Pulmonary gas exchange during altered density gas breathing. J Appl Physiol . 1983;40:221–225. doi: 10.1152/jappl.1982.52.1.221. [DOI] [PubMed] [Google Scholar]
- Eliason O, Zuwallack RL. Density dependence of maximal expiratory air flow in asthmatics with exacerbation of their disease. . Am Rev Respir Dis. 1986;135:573–578. doi: 10.1164/arrd.1987.135.3.573. [DOI] [PubMed] [Google Scholar]
- Gluck EH, Onaorato DJ, Castriotta R. Helium-oxygen mixtures in intubated patients with status asthmaticus and respiratory acidosis. . Chest. 1990;98:693–698. doi: 10.1378/chest.98.3.693. [DOI] [PubMed] [Google Scholar]
- Shiue S-T, Gluck E. The use of helium-oxygen mixture in the support of patients with status asthmaticus and respiratory acidosis. . J Asthma. 1989;26:177–180. doi: 10.3109/02770908909070987. [DOI] [PubMed] [Google Scholar]
- Madison JM, Irwin RS. Heliox for asthma: a trial balloon. . Chest. 107:597–600. doi: 10.1378/chest.107.3.597. [DOI] [PubMed] [Google Scholar]
- Metzger WJ, Nugent K, Richerson HB. Site of airflow obstruction during early and late phase asthmatic responses to allergen bronchoprovocation. Chest. 1985;8:369–375. doi: 10.1378/chest.88.3.369. [DOI] [PubMed] [Google Scholar]
- Macnee W, Power J, Innes A, Douglas NJ, Sudlow MF. The dependence of maximal flow in man on the airway gas physical properties. . Clin Sci. 1983;65:273–279. doi: 10.1042/cs0650273. [DOI] [PubMed] [Google Scholar]
- Clayton RG, Leef KM, Stefano JL. Determination of coefficient of variance of pulmonary function tests in infants with bronchopulmonary dysplasia [abstract]. Pediatr Res. 1992;31:303A. [Google Scholar]