

Abstract
Blastomyces dermatitidis is a fungus that is found primarily in endemic areas of the midwestern and southcentral USA. Blastomycosis pneumonia may develop after the inhalation of spores. While blastomycosis may lead to acute or chronic pneumonitis, it will rarely result in the development of the acute respiratory distress syndrome (ARDS). In this situation, mortality rates are 50–80%. Patients who survive, however, commonly show good recovery of pulmonary function. Extracorporeal membrane oxygenation (ECMO), a modified form of cardiopulmonary bypass that allows systemic perfusion, oxygenation, and carbon dioxide removal, may be used to support patients with cardiorespiratory failure that is refractory to conventional therapies. The use of ECMO allows the reduction of high levels of mechanical ventilatory support that may cause iatrogenic injury to the diseased lung. Fungal diseases are often contraindications for ECMO use, since systemic fungal organisms may bind to the ECMO circuit and be difficult to eradicate. It may be reasonable to utilize ECMO, however, if the fungal infection is isolated to the respiratory system. We report the case of a patient with ARDS secondary to blastomycosis pneumonia who was treated with ECMO due to the failure of conventional cardiorespiratory supports. To our knowledge, this is the first report of the use of ECMO for this condition.
Introduction
Blastomyces dermatitidis, a fungus that is endemic to the midwestern and southcentral USA, is a relatively common cause of pulmonary and cutaneous mycosis in these areas. Both respiratory and extrapulmonary infections are commonly initiated with the inhalation of fungal spores. Following the introduction of amphotericin B, the fatality rate has fallen from 78% to between 21–28%. If a total dose of 2 g amphotericin B is given, the cure rate may rise to 97% [1]. However, if blastomycosis pneumonia is associated with the development of the acute respiratory distress syndrome (ARDS), the mortality rate rises to 50%–80% [2].
Extracorporeal membrane oxygenation (ECMO) has been used successfully to support newborn, pediatric and adult patients with cardiac and respiratory diseases that are refractory to conventional therapy. Survival rates of 80% have been achieved in the 13000 neonates who have been supported with ECMO, while survival in the 1500 pediatric patients listed in the International Extracorporeal Life Support Registry who have received ECMO for respiratory failure is 53%. Of the 547 adults listed in the registry, 47% have survived [3].
In general, a primary fungal infection, especially when the infection is hematogenous, is a contraindication to the use of ECMO. Historically, patients with hematogenous fungal infections do poorly on ECMO, primarily because the mycosis cannot be eradicated from the synthetic surfaces of the ECMO circuit. The restriction against ECMO support for cardiorespiratory failure secondary to fungal pneumonia without hematogenous spread is less certain. In theory, this condition should not preclude the use of ECMO, but no reports about the use of ECMO in this situation are available.
We report our experience with the use of ECMO to support a previously healthy adolescent with respiratory failure secondary to blastomycosis pneumonia to raise awareness of this disease as a cause of pneumonia and better understand the use and limitation of extracorporeal support in this condition.
Case summary
A 15-year-old, 100kg black male developed fever, cough, and headache 12 days prior to admission to Georgetown University Hospital. Prior to this, the patient had been in good health with no evidence of immunodeficiency. There was no history of unusual travel or exposure to unusual environments. He was treated with amoxicillin for presumed sinusitis but his symptoms persisted and he was hospitalized for 2 days with erythromycin treatment for presumed atypical pneumonia. His chest radiograph revealed a left lower lobe infiltrate. After hospital discharge, the patient's private physician prescribed amantadine after his condition failure to improve. The patient was readmitted to the hospital 3 days later with respiratory distress and complete opacification of the right hemithorax and left lower hemithorax on chest radiograph (Fig. 1). Emergent intubation and institution of mechanical ventilatory support was performed.
Figure 1.
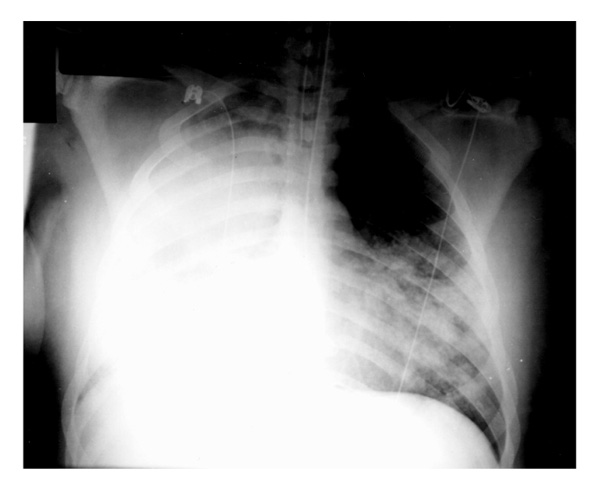
Chest radiograph on day of intubation. Note consolidation of right hemithorax and left lower thorax.
Despite supportive care and the institution of broad-spectrum antibiotic therapy, the patient's respiratory failure progressed. Mean airway pressures of 30–40 cmH2O 48 h after his readmission were required to maintain arterial partial pressure of carbon dioxide (PaCO2) 70torr and oxygen (PaO2) 50torr. Calculation of the oxygenation index (OI), a measure that relates airway pressure and PaO2 to presumed mortality, revealed that his OI was 36. OI is the product of mean airway pressure (MAP) and fraction of inspired oxygen concentration (FiO2) divided by the PaO2 [OI=(MAP × FiO2 × 100)/PaO2]. Treatment with inverse ratio ventilation, permissive hypercapnia, prone positioning and pulmonary surfactant instillation failed to improve oxygenation.
A tracheal aspirate and subsequent bronchoscopy specimen revealed broad-based fungal elements consistent with Blastomyces dermatitidis. No other organ involvement with blastomycosis was evident. Amphotericin B was added to the treatment regimen. By day 5 of readmission (day 11 of illness), continued deterioration in respiratory function led to referral for ECMO rescue.
The patient was transported to Georgetown University Hospital without complication. Despite multiple manipulations of mechanical ventilatory support (peak inspiratory pressure to 54 cmH2O, peak end-expiratory pressure to 18cm H2O) and a trial of inhaled nitric oxide, the OI remained >40, PaCO2 >99torr, PaO2 50–75torr and pulmonary artery pressure more than one-half systemic. Hemodynamic instability developed, requiring treatment with dopamine and dobutamine infusions. Progressive renal insufficiency, as demonstrated by rising creatinine and the development of anuria, was also present.
In an attempt to provide cardiorespiratory support while treatment for blastomycosis pneumonia was completed, and to allow time for potential lung recovery, ECMO was instituted. Modified venoarterial ECMO was chosen because of the cardiopulmonary instability of the patient. Cannulation was achieved using a 29 F catheter introduced into the right femoral vein and a 19F catheter placed into the right femoral artery. The ECMO circuit has been previously described [4]. Since adequate ventilation and oxygenation can be maintained by the ECMO circuit, the peak inspiratory pressure, rate, and inspired oxygen concentration can be reduced to lessen iatrogenic lung injury and to provide a better environment for potential lung healing.
Initial ECMO flows of 50–60 cm3/kg per min maintained mixed venous oxygen saturations of >70% and allowed a reduction in ventilator settings. After 24 h stabilization, the patient underwent bronchoscopy, which revealed denuded airway mucosa and purulent material filling the airways. Over the next few days, repeat bronchoscopy was performed to remove debris. On ECMO day 3, the patient became hyperdynamic and developed leukocytosis and decreasing mixed venous oxygen saturations. Sepsis was presumed, although cultures remained sterile. Membrane oxygenators on the ECMO circuit were changed without complication. The patient continued to have episodes of decreased mixed venous oxygen saturation despite increased ECMO circuit flow. Restriction of additional increases in circuit flow over the next few days led to the placement of a right internal jugular venous cannula and right carotid arterial cannula on ECMO day 10. All other organ systems remained intact and all cultures (blood, bronchial washing and tissue, urine) remained sterile. The patient was responsive to commands and questions while pharmacologic sedation was maintained. By ECMO day 14, minimal clearing of right and left lung fields was noted with concurrent increases in exhaled tidal volumes. Bronchoscopy was performed to remove airway debris with good results over the next few days and efforts to slowly re-expand the lungs were initiated. On ECMO day 18, bilateral tension pneumothoraces developed and the patient suffered cardiac arrest. Despite prompt resuscitation and continued support with ECMO, the patient deteriorated over the next 24h and ECMO support was electively withdrawn. Native pulmonary function was insufficient and the patient expired.
Postmortem findings
Despite systemic antifungal therapy and extracorporeal life support, postmortem examination revealed almost complete replacement of normal lung parenchyma with fungal elements and chronic inflammatory reaction. Extensive necrosis, acute and chronic inflammatory cells, abscesses, fibrin deposition and hemorrhage were seen (Fig. 2). Broad-based budding fungal organisms consistent with Blastomyces dermatitidis are seen in Figure 2 throughout the lung parenchyma. They are not seen in association with vascular structures. The left lung had regions of interstitial fibrosis. The central nervous system showed multiple areas of acute infarction and global ischemic encephalopathy. No evidence of invasion by Blastomyces dermatitidis was noted in the bloodstream or in any other organs outside of the lungs. The final pathologic cause of death was listed as fungal pneumonia with extensive destruction of lung tissue.
Figure 2.
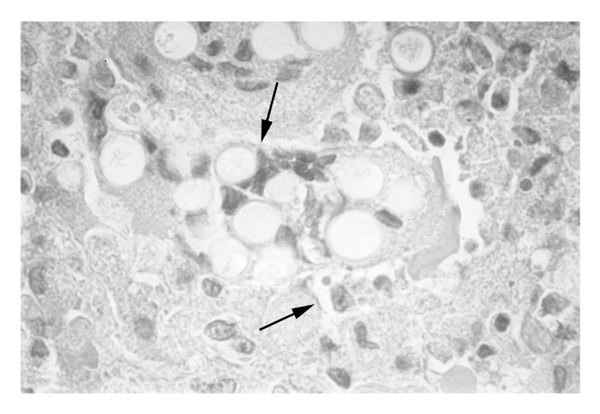
Section of lung tissue from post-mortem examination. H/E stain, magnification 200 ×. Note multinucleated giant cells consistent with blastomycosis and extensive destruction of lung.
Comments
Unlike many fungal infections, blastomycosis often occurs in immunocompetent hosts and many persons recover without antifungal treatment [5]. The typical patient with blastomycosis is male, aged 25–50 years, and habitually exposed to the outdoor environment. Children are rarely diagnosed with blastomycosis (epidemics excepted). The occurrence of blastomycosis in this patient, without living in an endemic area or with a history of prolonged outdoor activity, is extremely unusual.
The development of ARDS in association with pulmonary blastomycosis is exceedingly rare. However, when it does occur, mortality rates have been reported to be 50–80%. It is likely that this rate of mortality is reduced with prompt recognition of the disease, aggressive supportive therapies, and administration of a total of 2 g amphotericin B [1,6].
Our patient was referred to us as a potential candidate for ECMO. Historical data (respiratory failure unresponsive to conventional therapies and an OI > 40) suggested that this patient had a mortality risk of >80% [4]. In our experience with pediatric respiratory failure, patients receiving mechanical ventilation for less than 7 days prior to ECMO initiation have a 67% survival rate.
In general, ECMO is not utilized during an active fungal infection, since fungal elements in the bloodstream adhere to the synthetic elements of the ECMO circuit, making it impossible to eradicate them with antifungal agents. Pulmonary blastomycosis, however, is often localized to the respiratory tract, making contamination of the ECMO circuit less likely. Since this patient was previously healthy, had single-organ disease and had failed less invasive forms of pulmonary support, ECMO was instituted to limit further iatrogenic lung injury from mechanical ventilation during completion of amphotericin B treatment. Despite ECMO support, eradication of blastomycosis and healing of diseased lung tissue did not occur and the patient did not survive.
While blastomycosis was never isolated from the bloodstream and was only isolated from the respiratory tract prior to institution of amphotericin B therapy, it was identified throughout the lungs on postmortem examination. In otherwise healthy individuals, it is common to see lung recovery after treatment with systemic antifungal therapy. In fact, treatment with oral antifungal agents is sufficient for organism eradication and pulmonary recovery in most cases of blastomycosis [7].
There are several potential explanations for this lack of response to antifungal therapy. One explanation is that ECMO itself impacted on the effectiveness of antifungal therapy. Venoarterial ECMO has been shown to reduce pulmonary blood flow at high levels of bypass, and there is experimental evidence of pulmonary capillary bed ischemia with total bypass [8]. In this situation, severe lung injury may occur. Another potential problem with high levels of bypass is the potential limitation of drug delivery to the infected area; inadequate pulmonary blood flow reaching the lungs will lead to impaired fungal eradication. In this case, however, care was taken to limit the extent of cardiopulmonary bypass and to maintain pulmonary blood flow. It is possible that local blood flow was limited by tissue and vascular injury from the pneumonia, resulting in subtherapeutic tissue levels of amphotericin B. This would be consistent with the pathologic findings of heavy concentrations of fungal elements in injured lung parenchyma that was not in proximity to normal vascular structures.
Another potential pitfall of ECMO is the capacity of the membrane oxygenators to remove certain medications [9]. We monitored serum levels of amphotericin B in the patient and the ECMO circuit for standard peak and trough drug levels and when components of the circuit were changed. All levels were within or exceeded the recommended therapeutic range and were not affected by changes of the membrane oxygenator or circuit tubing [10].
It is also possible that this case was referred for ECMO too late in the course of disease to achieve any substantial benefit with the 'lung rest' provided by ECMO.
In summary, we present the first description of the use of ECMO to support respiratory failure in an adolescent with ARDS secondary to blastomycosis pneumonia. Despite the use of adequate antifungal agents, the reduction of ventilatory settings to non-toxic ranges, and adequate oxygen delivery to other organ systems, eradication of the blastomycosis did not occur and no lung recovery took place.
References
- Lockwood WR, Allison F, Jr, Batson BE, Busey JF. The treatment of North American blastomycosis: ten years' experience. Am Rev Respir Dis. 1969;100:314–320. doi: 10.1164/arrd.1969.100.3.314. [DOI] [PubMed] [Google Scholar]
- Meyer KC, McManus EJ, Maki DG. Overwhelming pulmonary blastomycosis associated with the adult respiratory distress syndrome. . N Engl J Med. 1993;329:1231–1236. doi: 10.1056/NEJM199310213291704. [DOI] [PubMed] [Google Scholar]
- Beck R, Anderson KD, Pearson GD, et al. Criteria for extracorporeal membrane oxygenation in a population of infants with persistent pulmonary hypertension of the newborn. J Pediatr Surg . 1986;21:297. doi: 10.1016/s0022-3468(86)80188-9. [DOI] [PubMed] [Google Scholar]
- Dalton HJ, Thompson AE. Extracorporeal membrane oxygenation. Pediatric Critical Care. Edited by Fuhrman BP, Zimmerman JJ. St Louis: Mosby. 1992. pp. 545–557.
- Bradsher RW. Blastomycosis. Clin Infect Dis. 1992;14 (suppl 1):S82–S90. doi: 10.1093/clinids/14.supplement_1.s82. [DOI] [PubMed] [Google Scholar]
- Parker JD, Doto IL, Tosh FE. A decade of experience with blastomycosis and its treatment with amphotericin B. Am Rev Respir Dis. 1972;105:812–818. doi: 10.1164/arrd.1969.99.6.895. [DOI] [PubMed] [Google Scholar]
- Bradsher RW, Rice DC, Abernathy RS. Ketoconazole therapy for endemic blastomycosis. Ann Intern Med. 1985;103:872–879. doi: 10.7326/0003-4819-103-6-872. [DOI] [PubMed] [Google Scholar]
- Kolobow T, Spragg RG, Pierce JE. Massive pulmonary infarction during total cardiopulmonary bypass in unaesthetized spontaneously breathing lambs. Int J Artif Organs. 1981;4:76–81. [PubMed] [Google Scholar]
- Arnold JH, Truog RD, Orav EJ, Scavone JM, Hershenson MB. Tolerance and dependence in neonates sedated with fentanyl during extracorporeal membrane oxygenation. Anesthesiology. 1990;73:1136–1140. doi: 10.1097/00000542-199012000-00011. [DOI] [PubMed] [Google Scholar]
- Hertzog JH, Brackett E, Sale M, Hauser GJ, Dalton HJ. Amphotericin Pharmacokinetics during ECMO. J Extracorp Technol. 1996;28:94–98. [Google Scholar]