

Abstract
Background
It is not well understood how sedentary women who wish to engage in regular exercise adhere to interventions during pregnancy and what factors may influence adherence over time.
Objective
To examine longitudinal patterns of pregnant women’s adherence to exercise.
Methods
Exploratory secondary data analyses were carried out with 124 previously sedentary pregnant women (ages 31 ± 5 years; 85% non-Hispanic White) from a randomized controlled trial. Daily exercise logs (n = 92) from 18 through 35 weeks of gestation were explored using linear regression, functional data, and principal component analyses.
Results
Adherence decreased as gestation week increased (p < .001); the top adherers maintained levels of adherence, and the bottom adherers decreased levels of adherence; and adherence pattern was influenced by types of exercise throughout the study period.
Discussion
Exercise behavior patterns were explored in a randomized controlled trial study, using chronometric data on exercise attendance. A new analytic approach revealed that sedentary pregnant women may adopt exercise habits differently from other populations.
Keywords: exercise, methods, statistical data interpretation
Promoting physical activity during pregnancy is an important part of prenatal care because physical inactivity is associated with risks of excessive weight gain (Stuebe, Oken, & Gillman, 2009), gestational diabetes (Liu, Laditka, Mayer-Davis, & Pate, 2008), preeclampsia (Sorensen, et al., 2003), and other conditions that may adversely affect maternal and child well-being. Exercise is defined as a planned, structured, and repetitive physical activity to improve or maintain physical fitness (Caspersen, Powell, & Christenson, 1985). Unfortunately, interventions to increase physical activity levels, or to increase the level of exercise, among pregnant women have been minimally successful (Meher & Duley, 2006). The majority of pregnant women (84.2%) do not initiate (Ning, et al., 2003) or increase their level of exercise (Domingues & Barros, 2007; Hinton & Olson, 2001; Ning, et al., 2003; Yeo, 2009).
For physical activity interventions to be effective for sedentary pregnant women, clinicians require a clear understanding of the specific nature of the intervention (Sidani & Braden, 1997). That is, the intervention must reflect specific problems presented by sedentary pregnant women who recognize the need for exercise or to increase general physical activity; providers need to understand processes involved in the delivery of the intervention. For example, in a study with elderly populations physical frailty and poor health were perceived as the greatest barriers to exercise adoption and adherence (Rhodes, et al., 1999). However, these factors may be minimally relevant to young and healthy populations. Physical activity is a unique lifestyle modification, and no single factor can predict the adoption and maintenance of exercise and physical activity interventions across populations (Dishman, Washburn, & Heath, 2004).
A few barriers to physical activity among pregnant women have been reported, including obesity (Damm, Breitowicz, & Hegaard, 2007), occupation (Spinillo, et al., 1995), educational attainment, income, race or ethnicity, age, and early child-rearing (Chasan-Taber, et al., 2007). However, these reports do not reflect how sedentary pregnant woman learn to adhere to interventions to adopt and maintain exercise habits during pregnancy. Specifically not addressed is what prohibits sedentary pregnant women from exercising, and under what conditions. Thus, little information exists to create effective interventions.
A criticism of many theoretical approaches has been the failure of researchers to examine exercise adoption and maintenance as a process, rather than as a static phenomenon (McAuley, 1992). To overcome this criticism valid and accurate description of factors that correlate with nonadherence (e.g., personal factors, program type, social influence on cognition) and study designs allowing investigators to capture longitudinal changes are needed. Few existing studies have met these criteria.
Lacking in the literature is information on the processes of sustaining adherence to exercise regimens once they have begun. Studies consistently indicate that the attrition rate from exercise programs is approximately 50% within the first 6 months (Dishman et al., 2004). The inability to understand the processes involving adoption and maintenance of exercise may stem from the limitation of available longitudinal data, and flexible and accurate data analysis methods. Often use of static, single-comparison designs result in a failure to show different aspects of behavior that is continually changing.
For example, using path analysis, McAuley (1992) examined the role played by self-efficacy cognitions in the process of adopting and maintaining exercise behavior by sedentary adults over 5 months. Path analytic techniques allowed the investigator to examine the role over time of efficacy, perceptual and behavioral indicators of frequency, and intensity of exercise. However, the use of panel or autoregressive models might be problematic ((McAuley, 1992). In order to circumvent such problems, variables needed to be measured as chronometric factors or reference curves and latent mean structures used to assess model fit. This requires frequent assessment of the variable over time, something not possible with respect to McAuley’s study.
In addition to methodological issues, pregnancy brings about a major lifestyle change for women, which may compete with or complement their intentions to make other lifestyle change. Dishman et al. (2004) stated that adoption and maintenance of exercise programs are subject to psychological, biobehavioral, and social-environmental influences. Several behavioral theories and models have been applied to exercise behavior of pregnant women. Among these theories, the concept of self-efficacy is assigned a central role as in Bandura’s (1977) social cognitive theory for analyzing changes achieved in fearful and avoidance behavior. Self-efficacy is the conviction that one can successfully execute the behavior required to produce desired outcomes. This is a focal variable in several other theories of motivated behavior such as Health Belief Model (Rosenstock, 1974), Theory of Planned Behavior [TPB] (Ajzen, 1991), or Transtheoretical Model (DiClemente & Prochaska, 1982).
Using the TPB, Hausenblas, Downs, Giacobbi, Tuccitto, and Cook (2008) examined exercise intention--of which exercise self-efficacy is a prerequisite--and behavior during pregnancy in a longitudinal study. With the advantage of applying Hierarchical Linear Modeling prospectively to examine the ability of the TPB to predict women’s exercise intention and behavior, they measured attitude, intention, perceived control, and exercise behavior at each trimester in a sample of 61 healthy pregnant women. They reported a statistically significant association between exercise intention and the behavior at each measurement (i.e., cross-sectional data), but failed to detect meaningful longitudinal associations between any factors and behavior over the duration of pregnancy. While Hausenblas et al. (2008) studied exercise behavior among pregnant women, their model failed to recognize behavior changes related to pregnancy beyond timing (at three data points during pregnancy). It is unknown whether this inability to predict the exercise adherence was due to the type of statistical analysis or due to the use of the TPB. Previously, Godin, Valois, Jobin, and Ross (1991) viewed the exercise intention in the application of TPB as necessary for exercise behavior, but not at a sufficient level to predict action (Dishman, 1994).
Pregnancy brings changes in weight gain, physical symptoms, body balance, and body shape to women. Women also face social and psychological issues, including self-identity or social changes, fear of labor and birth, and the need to navigate complex health care systems. It is this wide range of behavioral change processes that need to be recognized in effective exercise interventions to facilitate regular exercise. For example, in a study with a sedentary but nonpregnant population, McAuley (1992) found that self-efficacy was a significant predictor of frequency in the early or adoption stage of exercise participation. However, as exercise became habitual, efficacy cognitions with respect to barriers to participation cease to play such an important function. Pregnant women’s physiological and physical conditions continue to change throughout pregnancy, and different symptoms and life events challenge their willingness to adhere to exercise. This may suggest unique requirements for exercise interventions for sedentary pregnant women.
To begin to understand how sedentary women initiate and maintain exercise programs during pregnancy, data from an existing randomized controlled trial in which exercises were used as interventions were explored. The primary purpose of the original study was to compare the effects of walking and stretching on the incidence of preeclampsia, controlling for other daily physical activities. The primary outcomes have been published elsewhere (Yeo, 2009b; Yeo, et al., 2008).
A total of 124 eligible women were randomized at 18 weeks of gestation to either a walking (n = 64) or stretching (n = 60) exercise program as the intervention. Walkers were trained to walk at moderate intensity, and stretchers were trained to do prenatal stretching exercises that consisted solely of slow muscle movements (no aerobic or muscle resistance components). Of the 124 participants, 13 (10%) developed preeclampsia. The walking group had a higher incidence of preeclampsia than the stretching group (10 cases [16%] vs. 3 cases [5%]; exact conditional analysis, p = .054). Given the population estimate of 18% for preeclampsia in women with a history of the disease (Caritis, et al., 1998), the 10 preeclampsia cases in the walking group were within the expected range of incidence, but the 3 cases in the stretching group was significantly lower than expected (p < .005). The purpose of the study was to examine longitudinal patterns of adherence to exercise programs by previously sedentary pregnant women and to identify factors that influence these patterns.
Methods
This was an exploratory secondary data analysis to determine how types of exercise used as the intervention influence adherence patterns to the assigned exercise program. Available data were daily logs of monitored exercise recorded by a group of these women who started an exercise program during pregnancy. Adherence was defined as whether or not a participant exercised on a given day. If the answer was yes, 1 was assigned. If the answer was no, 0 was assigned. The total number of exercise days for each gestation week was expressed as the adherence of the week.
A relatively new exploratory analysis method, functional data analysis (Ramsay & Silverman, 2002), was used to examine complex patterns over time (i.e., patterns of exercise adherence as pregnancy progresses).
Procedures
Both stretchers and walkers visited the research exercise lab once a week and exercised under the supervision of an exercise specialist to ensure they were performing the exercises properly. Both groups were asked to perform their assigned exercise routine five times a week for the remainder of the pregnancy--1 day at the lab and 4 days on their own. They were asked to call a designated phone line immediately after exercising for monitoring purposes, and to complete an exercise log documenting the days they exercised. Women submitted a weekly exercise log when they visited the lab. A research staff member verified the phone record and the log. When a discrepancy was noted, the woman was consulted during the visit. An exercise log form was used to show the days of the week individual women exercised. In a few cases, when the women could not make a scheduled visit, they entered exercise information from the missed week on the same form as the subsequent week. However, the data were used as reported by the women, where the information presented on each form was considered a single week. Though not reported in this secondary data analysis, other daily physical activities (leisure time, occupational, domestic, and transportation) were assessed using an objective measure (daily step counters) and subjective scales. No group differences were detected in other daily physical activities.
Data Analysis
To maximize the strength of the longitudinal data, a three-step statistical analysis was performed.
Linear regression
The purpose of this step was to determine which of the variables had a statistically significant relationship with exercise program adherence.
Functional data analysis
To explore the adherence data, which is viewed as a collection of data patterns over time, a functional data analysis (FDA) method called principal component analysis (PCA) was used.
An important focus of this study was how the exercise program adherence changed during the duration of pregnancy. For this part of the statistical analysis, adherence for each participant was considered to be a pattern--a time function of gestation weeks 18 through 35. A standard approach to analyzing functional data sets is to plot the data as curves, then carry out a PCA to interpret the results as curves.
The key to FDA is to think of each pattern as a single data point in a high dimensional space. Each observation over the continuum of the function (e.g., time) is considered an additional dimension. Spaces with greater than three dimensions are difficult to visualize, but can be analyzed mathematically. The analysis is performed in that space, and then the results are interpreted in the original space of curves. PCA is an exploratory data analysis method often used to simplify high dimensional, or functional, data. Directions in the high dimensional space are found that explain the most variability in the data. Frequently, important aspects of the data (i.e., the primary differences among a set of curves) are highlighted in these directions. The first principal component is the direction of maximum variation within the data, the second principal component is the direction with the highest amount of variation unrelated (geometrically orthogonal) to the first principal component, the third component is the direction with the highest amount of variation unrelated to the first two components, and so on. Important insights about the data often are revealed by studying the projections of the data onto the PCA direction vectors, and then interpreting those as curves. For a more detailed discussion of PCA, see Jolliffe, 2002. The FDA in this study was performed using MATLAB subroutines available from Marron (Marron, 2009).
Hypothesis testing
These tests were performed to validate the suggested trends from the above exploratory analysis. Certain hypotheses concerning trends in adherence were tested using a hierarchical, or mixed, linear model. Mixed models are used to account for variation across groups or between individual participants. Gestation week was used as a predictive variable of weekly exercise adherence, and the intercept for each individual was treated as a random component to account for variation across women. Mixed models were fit by restricted maximum likelihood estimation using the R statistical software package (R Foundation for Statistical Computing, Wien, Austria).
Results
Sample Characteristics
Most of the women (85%) identified themselves as non-Hispanic White, and were on average 31 +/- 5 years of age with 15 +/- 2 years of education. Fifty-two percent reported household incomes above $75,000, and most were employed (80%) at an average of 30 +/- 13 hours per week. The majority (82%) had one child at home. A pregnant woman is classified as obese if she has a body mass index (BMI) greater than 29 kg/m, as recommended by the Institute of Medicine (Institute of Medicine, 1990). At the time of their first visit, 42% of women were classified as obese. At baseline, there were no significant differences between the stretching and walking groups on any variables (Yeo, et al., 2008). For this study, weekly exercise logs from both groups were analyzed.
There were 124 eligible women, but due to missing values in exercise log data and mismatching of several identification numbers between data sets, this number was reduced to 92.
Linear Regression
Simple linear regression was used to determine whether the assigned exercise group (stretching or walking) and other physical and demographic factors correlated significantly with adherence. Exercise program adherence was measured by the number of times the participant exercised during the specified gestation week. Linear regression was used as a guide to determine which variables had the strongest relation with ADHERENCE. Because each participant had daily ADHERENCE measurements (1 if the participant exercised, 0 if the participant did not exercise), for the linear regression, ADHERENCE is the average number of times the participant exercised during gestation weeks 18 to 35. The participants entered the study around 14 to 16 weeks of gestation, and exited around 38 weeks of gestation. The range from 18 to 35 weeks of gestation was selected as a period with data for the women, and also sufficiently reflected their adherence to the assigned exercise program.
To perceive the general information in the data, a linear regression model was run on the measure ADHERENCE using the variables listed in Table 1. The estimated model is summarized in Table 2. Some of the levels of GRAVID (number of previous pregnancies) appeared to have a statistically significant relation with ADHERENCE, as did GRP (exercise group). Most of the covariates (AGE, EDUCATION, WORK, WEIGHT, BMI, and INCOME) did not appear to have a statistically significant relationship with ADHERENCE. Specifically, the estimated coefficient of 0.861 for stretchers suggests that the women assigned to the stretching exercise program adhere better than those assigned to the walking exercise program.
Table 1.
Summary of All Variables Initially Included in the Linear Analysis
| Variable Name | Explanation | Summary Statistics |
|---|---|---|
| ADHERENCE | Average count of exercise sessions during gestation weeks 18-35 | M = 3.61, SD = 1.32 |
| AGE | Age of participant | M = 31.55, SD = 4.75 |
| GRAVID | Number of previous pregnancies (1, 2, 3, 4 or more) |
n [1] = 37, n [2] = 28, n [3] = 13, n [4+] = 14 |
| EDUCATION | Years of education | M = 15.55, SD = 2.19 |
| WORK | Number of hours worked per week | M = 21.57, SD = 17.90 |
| INCOME | Household income (1 = less than $25,000, 2 = $25,000-50,000, 3 = $50,000-74,999, 4 = $75,000 or greater) |
n [1] = 0, n [2] = 9, n [3] = 25, n [4] = 55, NA = 3 |
| WEIGHT | Initial weight (in pounds) | M = 178.45, SD = 44.81 |
| BMI | Initial body mass classification (1 = underweight, 2 = normal, 3 = overweight, 4 = obese, 5 = morbidly obese) |
n [1] = 1, n [2] = 33, n [3] = 20, n [4] = 16, n [5] = 19, NA = 3 |
| GRP | Exercise group (walking, stretching) |
n [walking] = 51, n [stretching] =41 |
Note. The means (M) and standard deviations (SD) are provided in column three for the continuous variables, and the counts (n) are provided for each level of the categorical variables. NA gives the number of missing values.
Table 2.
Estimated Model with All Variables
| Estimate | SE | t | Pr(>|t|) | |
|---|---|---|---|---|
| (Intercept) | 4.803 | 2.007 | 2.394 | 0.020 |
| AGE | -0.010 | 0.035 | -0.278 | 0.782 |
| EDUCATION | 0.012 | 0.076 | 0.158 | 0.875 |
| WORK | -0.009 | 0.009 | -0.964 | 0.339 |
| WEIGHT | -0.004 | 0.007 | -0.565 | 0.574 |
| BMI: 2 (normal) | -0.944 | 1.246 | -0.758 | 0.451 |
| BMI: 3 (overweight) | -1.301 | 1.291 | -1.008 | 0.317 |
| BMI: 4 (obese) | -1.286 | 1.356 | -0.948 | 0.346 |
| BMI: 5 (morbid) | -0.898 | 1.488 | -0.603 | 0.549 |
| GRAVID: 2 | 0.404 | 0.360 | 1.123 | 0.266 |
| GRAVID: 3 | -0.075 | 0.435 | -0.174 | 0.863 |
| GRAVID: 4+ | -1.036 | 0.486 | -2.133 | 0.037 |
| INCOME | 0.162 | 0.252 | 0.641 | 0.524 |
| GRP: stretching | 0.861 | 0.306 | 2.813 | 0.006 |
Note. This is the output of the linear model of ADHERENCE regressed on all the covariates listed in Table 1. SE and t give the standard error and t-statistic respectively, and Pr(>|t|) gives the corresponding p-value.
After fitting a number of linear models, it appeared that the only variable with a statistically significant relationship with ADHERENCE was GRP. The initial weight of the participant had a moderately significant relationship with ADHERENCE (Table 3). The exercise group to which a participant was assigned appeared to have the strongest relationship with adherence to the exercise program. Specifically, women assigned to the stretching exercise group adhered better to their program than those assigned to the walking group. The overall model is statistically significant (p = .003), and the adjusted R-squared value of 0.102 suggests that about 10% of the variation of ADHERENCE was explained by WEIGHT and GRP. The model of ADHERENCE regressed only on GRP has a statistically significant estimated coefficient of 0.835 (p = .002). The adjusted R-squared value is 0.089, which suggests about 8.9% of the variation of ADHERENCE is explained by GRP.
Table 3.
Estimated Model for Weight and Exercise Type on Adherence
| Estimate | SE | t | Pr(>|t|) | |
|---|---|---|---|---|
| (Intercept) | 4.182 | 0.547 | 7.645 | 2.45e-11 |
| WEIGHT | -0.005 | 0.003 | -1.729 | 0.087 |
| GRP: stretching | 0.794 | 0.260 | 3.048 | 0.003 |
Note. This is the output of the linear model of ADHERENCE regressed on initial weight and exercise group. Exercise group has a statistically significant estimated coefficient, and initial weight has a moderately statistically significant estimated coefficient. SE and t give the standard error and t-statistic respectively, and Pr(>|t|) gives the corresponding p-value.
Functional Data Analysis
The data are plotted as patterns (i.e., functions) in Figure 1 (see Figure, Supplemental Digital Content 1, which illustrates the data in color). Each function represents 1 of the 92 participants and is colored according to the participants’ assigned exercise group (gray for walkers and black for stretchers). The bold lines on Figure 1 are the average adherences for each exercise group. This plot shows the value of an FDA approach in contrast to a classical linear model analysis. In particular, plotting the patterns and the averages reveals that over the duration of the study, for each gestation week, on average stretchers (black line) performed better than walkers (gray line), which is consistent with the regression result above. Furthermore, there is some apparent decline in adherence, with perhaps a stronger decline for the walking group. These impressions will be reviewed more rigorously below.
Figure 1.
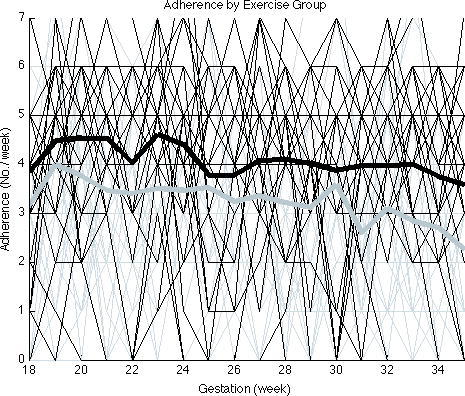
Adherence by exercise group. The plot displays weekly exercise program adherence during gestation weeks 18 through 35. Each curve is an observation, and the thick, bold lines are the average adherences for each exercise group. From the bold curves, it is visually apparent that, on average during the length of the study, the stretchers (black) adhered better to their exercise program.
Principal Component Analysis
In this stage of the analysis, a PCA is performed. The first two principal components are shown in Figure 2 (see Figure, Supplemental Digital Content 2, which is illustrated in color) (same as above) by exercise group. The Figure 2A contains a plot of the raw data; Figure 2B contains the pattern interpretation of the projections on the first PC direction; and similarly, Figure 2C contains a plot for the second PC direction. The overall mean of the data for each week is shown in Figure 2D. The mean adherence decreased as gestation week increased; that is, women generally adhered less to their exercise program over time. The dominant mode of variation in this data set is vertical shift, as indicated in Figure 2B. The greater prevalence of blue patterns at the top and red patterns at the bottom is consistent with the better overall adherence of the stretching (blue) group. The curves in Figure 2B are not completely parallel, and fan out more in later times. This suggests that the top adherers (i.e., the women with above average adherence) appear to maintain their level of adherence during the study, and the bottom adherers (i.e., the women with below average adherence) appear to decrease their level of adherence during the study. Another interpretation of principal component 1 is given in Figure 2E, which shows the mean pattern using the solid line, the mean plus the smallest curve in Figure 2B as the dashed line, and the mean plus the largest pattern in Figure 2B as the dotted line. The solid line is roughly horizontal, consistent with the stretching group having a rather flat average, and the dashed line is sloped more strongly, consistent with poorer adherence over time for the walking group. This suggests that the stretchers maintained a high level of adherence, while walkers adhered less and actually decreased in adherence throughout the duration of the study. These hypotheses were tested, and the results are summarized in the next section.
Figure 2.
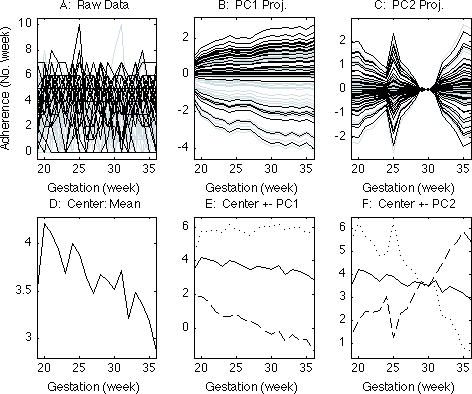
The first row displays the raw data and the pattern interpretation of the projections on the first two PC (principal component) directions of the data colored by exercise group assignment (walkers: gray; stretchers: black).
Principal component 2 represents the degree to which participants changed their level of adherence (starting at a higher level of adherence and then switching to a lower level of adherence, or vice versa). It is apparent in Figure 2C that there was not a high degree of switching, which can be inferred by the aggregation of horizontal lines around 0 in this plot. In Figure 2F the dotted and dashed lines outline the exterior of the lines presented in Figure 2C added back to the mean. These dotted and dashed lines in Figure 2F outline the subjects who changed the most for the worse and for the better, respectively.
Hypothesis Testing
To test the significance of a trend in adherence, a mixed model was fit to the weekly data, using gestation week as a predictive variable. The intercept for each individual was treated as a random component in the model. The variable WEEK was the number of weeks after gestation week 18. When this model was fit to the entire data set, estimates for the overall intercept and slope give Adherence = 4.044-0.051*WEEK (Table 4). The small p-value for the coefficient of WEEK (p < .001) indicates that, on average, participants adhered significantly less over time.
Table 4.
Estimated Model for Adherence by Gestation Week (All Participants, Walkers Only, and Stretchers Only)
| Estimate | SE | t | Pr(>|t|) | |
|---|---|---|---|---|
| All | ||||
| (Intercept) | 4.044 | 0.150 | 26.980 | < .001 |
| WEEK | -0.051 | 0.007 | -7.380 | < .001 |
| Walkers Only | ||||
| (Intercept) | 3.771 | 0.196 | 19.254 | < .001 |
| WEEK | -0.062 | 0.009 | -6.731 | < .001 |
| Stretchers Only | ||||
| (Intercept) | 4.384 | 0.212 | 20.630 | < .001 |
| WEEK | -0.036 | 0.011 | -3.543 | < .001 |
Note. SE and t give the standard error and t-statistic respectively, and Pr(>|t|) gives the corresponding p-value.
Separate models were fit for women in the walking group and those in the stretching group. In both cases, the coefficient for WEEK was negative and significant, indicating that adherence decreased on average for both walkers and stretchers (Table 4). These models also indicate that adherence may have dropped off more quickly for walkers than for stretchers, as discussed in the previous section. An interaction term between WEEK and exercise group was not significant (p = .058).
Discussion
The results of this study suggest that women who demonstrated high adherence at the beginning of the intervention tended to remain high adherers, while the women who started as low adherers generally did not improve their adherence. This is contrary to current understanding. People gradually learn to adhere (Marcus, Simkin, Rossi, & Pinto, 1996) but eventually adhere less to exercise programs until they drop out (Dishman et al., 2004). In this exploratory analysis, less than 10% of the variation was explained by a statistically significant factor (i.e., exercise type). Adherence tended to drop off more rapidly among those with a low initial adherence. Furthermore, no other previously identified factors, such as age, educational attainment, and baseline obesity, were a significant determinant of adherence patterns.
The largest amount of variation in the data was due to individual differences and large fractions of variation remained unexplained (individual errors). A similar trend was reported by others (McAuley, 1992). This may suggest a need to better understand individual processes involved with behavior modification. The two groups (high vs. low adherence) may need different interventions, or different approaches. FDA results showed that although more stretchers were found among higher adherers, there were stretchers who were low adherers and walkers who were high adherers.
However, the final hypothesis tested using mixed models showed that an interaction term between the pregnancy and exercise groups was not significant. The study had a number of limitations, which may be addressed in future research. The research was based on a secondary data analysis. Behavioral factors contributing to exercise adherence were not collected in the original study, thus interpretation of results using behavioral theories was limited. Subject report was used to assess adherence; further research that addresses this limitation is needed. For example, pedometer or accelerometer has been used to provide relatively reliable data for daily physical activity and could be used in future studies.
According to the Transtheoretical Model of Stages of Change, when people try to change behavior they move through stages of precontemplation, contemplation, preparation, action, and maintenance in a sequential manner (Marcus, et al., 1996). The average period for exercise behavior adoption is reported between 3 and 6 months in nonpregnant populations. Often behavior change takes several attempts, so the stages can be cyclical instead of linear, and the processes of change presumably are unique to each stage. The results of the current study did not show many switching incidences (i.e., low adherence to high adherence or vise versa) during the 4 months of the study period, which would have indicated different stages.
The Theory of Planned Behavior, a modification of the Theory of Reasoned Action (Ajzen, 2001), was the model used by Hausenblas et al. (2008) among pregnant women. The theory posits that attitudes toward exercise and social norms about exercise influence the intention to exercise. Although willpower and self-motivation may influence intention, more than intention is necessary for exercise adherence. Most likely women in the current study had intention to exercise because they voluntarily entered into the study and demonstrated their ability to attend regular visits during the prerandomization period (Anonymous, 2006).
The majority of factors influencing adherence in the current study were unknown. These factors may include pregnancy-related symptoms and social, environmental, setting, and individual or personal factors. These factors could influence the implementation of interventions (Sidani & Braden, 1997).
Functional data analysis can be used in other nursing research. For example, medication adherence or daily food intake may have patterns when their behaviors were observed over time. Advanced exploratory data analysis methods, along with qualitative analysis methods contribute to the development of theory-driven exercise interventions for pregnant women.
Supplementary Material
Acknowledgments
This study was supported by National Institutes of Health grant # R01-NR05002.
Contributor Information
SeonAe Yeo, Associate Professor of Nursing, School of Nursing, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Jessi Cisewski, PhD Candidate, Department of Statistics and Operation Research, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Eric F. Lock, PhD Candidate, Department of Statistics and Operation Research, University of North Carolina at Chapel Hill, Chapel Hill, NC
J. S. Marron, Amos Hawley Professor of Statistics and Operations Research, Professor of Biostatistics, Department of Statistics and Operation Research and Department of Biostatistics, University of North Carolina at Chapel Hill, Chapel Hill, NC.
References
- Ajzen I. The theory of planned behavior. Organizational behavior and human decision processes. 1991;50:179–211. [Google Scholar]
- Ajzen I. Nature and operation of attitudes. Annual Review of Psychology. 2001;52:27–58. doi: 10.1146/annurev.psych.52.1.27. [DOI] [PubMed] [Google Scholar]
- Caritis S, Sibai B, Hauth J, Lindheimer M, VanDorsten P, Klebanoff M, et al. Predictors of pre-eclampsia in women at high risk. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. American Journal of Obstetrics and Gynecology. 1998;179:946–951. doi: 10.1016/s0002-9378(98)70194-2. [DOI] [PubMed] [Google Scholar]
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131. [PMC free article] [PubMed] [Google Scholar]
- Chasan-Taber L, Schmidt MD, Pekow P, Sternfeld B, Manson J, Markenson G. Correlates of physical activity in pregnancy among Latina women. Maternal and Child Health J. 2007;11(4):353–363. doi: 10.1007/s10995-007-0201-8. [DOI] [PubMed] [Google Scholar]
- Damm P, Breitowicz B, Hegaard H. Exercise, pregnancy, and insulin sensitivity--what is new? Applied Physiology, Nutrition, and Metabolism. 2007;32(3):537–540. doi: 10.1139/H07-027. [DOI] [PubMed] [Google Scholar]
- DiClemente CC, Prochaska JO. Self change and therapy change of smoking behavior. A comparison of processes of change in cessation and maintenance. Addictive behavior. 1982;7:133–142. doi: 10.1016/0306-4603(82)90038-7. [DOI] [PubMed] [Google Scholar]
- Dishman R, Washburn RA, Heath GW. Physical Activity Epidemiology. Champaign, IL: Human Kinetics; 2004. Adopting and maintaining a physically active lifestyle; pp. 391–437. [Google Scholar]
- Dishman RK. The measurement conundrum in exercise adherence research. Medicine and Science in Sports and Exercise. 1994;26(11):1382–1390. [PubMed] [Google Scholar]
- Domingues MR, Barros AJ. Leisure-time physical activity during pregnancy in the 2004 Pelotas Birth Cohort Study. Revista de Saude Publica. 2007;41(2):173–180. doi: 10.1590/s0034-89102007000200002. [DOI] [PubMed] [Google Scholar]
- Godin G, Valois P, Jobin J, Ross A. Prediction of intention to exercise of individuals who have suffered from coronary heart disease. Journal of Clinical Psychology. 1991;47(6):762–772. doi: 10.1002/1097-4679(199111)47:6<762::aid-jclp2270470606>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- Hausenblas H, Downs DS, Giacobbi P, Tuccitto D, Cook B. A multilevel examination of exercise intention and behavior during pregnancy. Social Science & Medicine. 2008;66(12):2555–2561. doi: 10.1016/j.socscimed.2008.02.002. [DOI] [PubMed] [Google Scholar]
- Hinton PS, Olson CM. Predictors of pregnancy-associated change in physical activity in a rural white population. Maternal and Child Health Journal. 2001;5(1):7–14. doi: 10.1023/a:1011315616694. [DOI] [PubMed] [Google Scholar]
- Institute of Medicine, Food and Nutrition Boad, Committee on Nutritioal Status During Pregnancy, Part I: Nutritional Status and Weight Gain. Washington, DC: National Academy Press; 1990. [Google Scholar]
- Jolliffe IT. Principal component analyis. 2. New York: Springer; 2002. [Google Scholar]
- Liu J, Laditka JN, Mayer-Davis EJ, Pate RR. Does physical activity during pregnancy reduce the risk of gestational diabetes among previously inactive women? Birth. 2008;35(3):188–195. doi: 10.1111/j.1523-536X.2008.00239.x. [DOI] [PubMed] [Google Scholar]
- Marcus BH, Simkin LR, Rossi JS, Pinto BM. Longitudinal shifts in employees’ stages and processes of exercise behavior change. American Journal of Health Promotion. 1996;10(3):195–200. doi: 10.4278/0890-1171-10.3.195. [DOI] [PubMed] [Google Scholar]
- Marron JS. MATLB routines. 2009 Available from www.unc.edu/~marron/marron_software.html.
- McAuley E. The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. Journal of Behavioral Medicine. 1992;15(1):65–88. doi: 10.1007/BF00848378. [DOI] [PubMed] [Google Scholar]
- Meher S, Duley L. Cochrane Database of Systematic Reviews(2) 2006. Exercise or other physical activity for preventing pre-eclampsia and its complications. CD005942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ning Y, Williams MA, Dempsey JC, Sorensen TK, Frederick IO, Luthy DA. Correlates of recreational physical activity in early pregnancy. Journal of Maternal-Fetal & Neonatal Medicine. 2003;13(6):385–393. doi: 10.1080/jmf.13.6.385.393. [DOI] [PubMed] [Google Scholar]
- Ramsay JO, Silverman MW. Applied Functional Analysis: Methods and case studies. New York: Springer; 2002. [Google Scholar]
- Rhodes RE, Martin AD, Taunton JE, Rhodes EC, Donnelly M, Elliot J. Factors associated with exercise adherence among older adults. An individual perspective. Sports Medicine. 1999;28(6):397–411. doi: 10.2165/00007256-199928060-00003. [DOI] [PubMed] [Google Scholar]
- Rosenstock IM. The health belief model and preventive health behavior. Health Education Monographs. 1974;2(4):354–386. doi: 10.1177/109019817800600406. [DOI] [PubMed] [Google Scholar]
- Sidani S, Braden CJ. Evaluating nursing interventions: A theory-driven approach. SAGE Publications, Inc; 1997. [Google Scholar]
- Sorensen TK, Williams MA, Lee IM, Dashow EE, Thompson ML, Luthy DA. Recreational physical activity during pregnancy and risk of preeclampsia. Hypertension. 2003;41(6):1273–1280. doi: 10.1161/01.HYP.0000072270.82815.91. [DOI] [PubMed] [Google Scholar]
- Spinillo A, Capuzzo E, Colonna L, Piazzi G, Nicola S, Baltaro F. The effect of work activity in pregnancy on the risk of severe preeclampsia. The Australian & New Zealand Journal of Obstetrics & Gynaecology. 1995;35(4):380–385. doi: 10.1111/j.1479-828x.1995.tb02146.x. [DOI] [PubMed] [Google Scholar]
- Stuebe AM, Oken E, Gillman MW. Associations of diet and physical activity during pregnancy with risk for excessive gestational weight gain. American Journal of Obstetrics and Gynecology. 2009 doi: 10.1016/j.ajog.2009.02.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeo S. Adherence to walking or stretching, and risk of preeclampsia in sedentary pregnant women. Research in Nursing & Health. 2009;32(4):379–390. doi: 10.1002/nur.20328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeo S, Davidge ST, Ronis DL, Antonakos CL, Hayashi R, O’Leary S. A Comparison of Walking Versus Stretching Exercise to Reduce the Incidence of Preeclampsia: A Randomized Clinical Trial. Hypertension in Pregnancy. 2008;27(2):113–130. doi: 10.1080/10641950701826778. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.