

Abstract
Investing in social protection in sub-Saharan Africa has taken on a new urgency as HIVand AIDS interact with other drivers of poverty to simultaneously destabilise livelihoods systems and family and community safety nets. Cash transfer programmes already reach millions of people in South Africa, and in other countries in southern and East Africa plans are underway to reach tens and eventually hundreds of thousands more. Cash transfers worldwide have demonstrated large impacts on the education, health and nutrition of children. While the strongest evidence is from conditional cash transfer evaluations in Latin America and Asia, important results are emerging in the newer African programmes. Cash transfers can be implemented in conjunction with other services involving education, health, nutrition, social welfare and others, including those related to HIV and AIDS. HIV/ AIDS-affected families are diverse with respect to household structure, ability to work and access to assets, arguing for a mix of approaches, including food assistance and income-generation programmes. However, cash transfers appear to offer the best strategy for scaling up to a national system of social protection, by reaching families who are the most capacity constrained, in large numbers, relatively quickly. These are important considerations for communities hard-hit by HIV and AIDS, given the extent and nature of deprivation, the long-term risk to human capital and the current political willingness to act.
Keywords: social protection, cash transfers, HIV, AIDS, Africa, Latin America, maternal and child health and nutrition, education, gender
Introduction
Investing in social protection in sub-Saharan Africa has taken on a new urgency as HIV and AIDS interact with other drivers of poverty to simultaneously destabilise livelihoods systems and family and community safety nets. A focus on the vulnerability of families, and on threats to the human capital of children with lifelong and intergenerational consequences, has accelerated international, regional and national commitments to social protection. Social protection broadly, and cash transfers in particular, are increasingly receiving recognition as an important part of a comprehensive HIV/AIDS response. The importance of cash assistance for food purchases is underscored by emerging evidence indicating the effects of good nutrition on slowing the progression of AIDS, and on the effectiveness of antiretroviral therapy, with consequences not only for people living with HIVbut also their children, families and communities. Cash transfers already reach millions of people in southern Africa, and plans are underway in other countries in sub-Saharan Africa to roll out programmes reaching tens and eventually hundreds of thousands of poor people.1 While they do not use HIV and AIDS as targeting criteria, these programmes are rolling out in heavily in AIDS-affected regions, and some are targeted using multiple vulnerability criteria that aim to capture poor and AIDS-affected families and individuals.2
This article examines the potential for systems of social protection, primarily through cash transfers, to protect the human capital of vulnerable children and families. It is based on a study that reviewed over 300 documents on cash transfer programmes for poor families, and related issues, around the world. Impact assessments of 20 cash transfer programmes — 10 unconditional and 10 conditional — were reviewed,3 based on their reporting of quantitative impacts through a reasonably strong research design. Conditional cash transfer programmes (CCTs) in Latin America and Asia, which make cash benefits conditional on household members’ participation in education, health and nutrition services, are reviewed here because most strong, rigorous evidence to date on cash transfer impacts come from these programmes. CCTs thus show us what can be achieved through cash transfers. Conditionality may potentially increase impacts of cash transfers in AIDS-affected contexts, e.g., by keeping girls in secondary school, or encouraging participation in nutrition and health counselling and other services, though this is yet to be tested. In the meantime, there are several reasons why cash transfer programmes in East and southern Africa are thus far unconditional (see Adato & Bassett, 2008).
Why cash transfers?
Figure 1 presents an asset-based social protection conceptual framework.4 The programmes in the figure are loosely placed under the objectives with which they are generally associated. However, each programme can be used to achieve any of the five objectives depending on how they are designed, and the capacities that people have to take advantage of them. A cash transfer programme can thus assist vulnerable families by, for example: (1) securing basic subsistence where family illness or death reduces income; (2) keeping children from leaving school because of inability to pay fees or labour needed at home; (3) preventing the sale of animals to pay for consumption; (4) enabling investment in small livestock for food and income generation; (5) increasing women's status and child nutrition through giving cash benefits directly to women.
Figure 1.
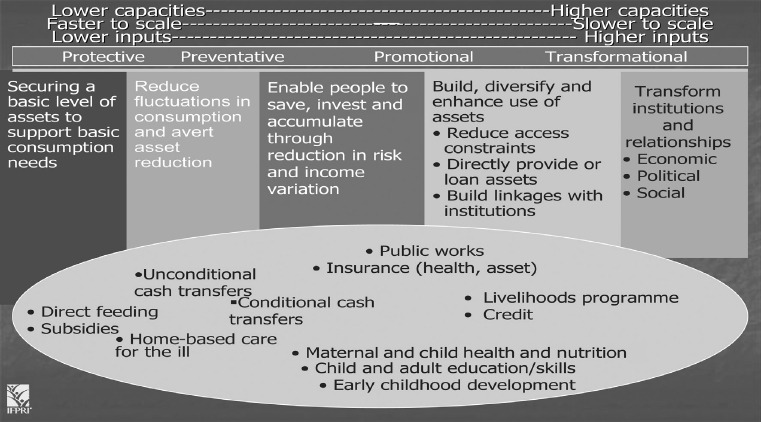
An asset-based social protection framework.
Some of the most important asset investments enabled by cash transfers are children's health, nutrition and education. During pregnancy and in the first two years of life nutritional losses take their greatest toll, causing damage that is largely irreversible. Data from over 80 countries show that poor and malnourished children are likely to start school later, and/or complete fewer years of schooling, compared to wealthier and healthier children (Alderman, Hoddinott, & Kinsey, 2003; Behrman, 2000; Behrman et al., 2003; Glewwe, Jacoby, & King, 2001; Grantham-McGregor et al., 2007). Malnourished children have shown reduced capacity to learn based on data from at least 16 countries (Grantham-McGregor et al., 2007; Martorell 1995, 1999; Pollitt, Gorman, Engle, Rivera, & Martorell, 1995). These human capital deficits in turn have demonstrated long-term impacts on earnings (Behrman, 2000; Grantham-McGregor et al., 2007; Hoddinott, Maluccio, Behrman, Flores, & Martorell, 2008), completing the cycle that transmits poverty through generations.
The dynamics between human capital losses and poverty are likely to be intensified in the context of AIDS. Poverty and food and nutrition security are critical concerns because of their powerful and mutually reinforcing relationship with HIV. In a vicious cycle, food and nutrition insecurity increases susceptibility to HIV exposure and infection, and lowers resiliency to AIDS impacts, while HIV/AIDS intensifies vulnerability to food and nutrition insecurity.5 All of these processes heavily affect children, from their own risks of infection, to the economic and psychosocial impacts of parental and other relatives’ illness and death. Improving food security through social protection can break this cycle.
Many forms of social protection can benefit AIDS-affected families. Food and nutrition assistance programmes are particularly important for nutritional rehabilitation for children and for people living with AIDS, where improved quantity and quality of food, and specific micronutrients, are needed urgently. However, logistics, international political economy, and policies limiting the duration of food support, make food assistance less appropriate as a national system of social protection. Public works programmes can be designed to include AIDS-affected families, through e.g., flexible family contracts, light work activities and care-giving activities. Livelihoods support programmes also play an important role, particularly through activities that contribute to food production, nutritional improvement and income generation, with attention to asset constraints. Even microcredit programme designs have been made sensitive to the HIV/AIDS context. However, livelihoods and credit programmes require greater capacities on the part of beneficiaries and programme implementers than do cash transfers, are slower to scale up, will have narrower reach, and are harder to target to the most disadvantaged. All of these approaches should be part of a menu that governments and NGOs can draw on in different contexts. Cash transfers are highlighted here because of the particular advantages they offer for very poor, severely AIDS-affected families who need urgent assistance.
The impacts of cash transfers on education, health and nutrition
Cash transfers and education
Cash transfers have the potential to increase and protect children's education by covering school expenses, compensating for lost income when children are sent to school rather than work, ensuring that children are better nourished at school, and providing an incentive for attendance when cash is conditional. Cash transfers can have particular advantages for girls in the context of HIV and AIDS, as girls often care for children and ill adults in HIV-affected households. Recent studies have shown a positive relationship between girls’ school enrollment and reduced sexual activity (Baird et al., 2009; Duflo et al., 2006) and reduced HIV risk (Pettifor, et al., 2008).
Table 1 summarises the results on education impacts of unconditional cash transfers in three southern African countries. In one district in South Africa, Case, Hosegood, and Lund (2005) found that receipt of the Child Support Grant (CSG) was associated with an 8.1 percentage-point increase (p <0.05) in enrolment among six-year olds, and 1.8 points (p <0.05) for seven-year olds. The larger impacts are probably due to the substantially lower overall enrolment rates at age six in the study region. Much higher impacts for boys than girls at older ages highlight the importance of attention to gender inequalities. Using national level data in South Africa, Samson et al.'s (2004) model establishes that household receipt of an Old Age Pension (OAP) or CSG is associated with a 25% reduction§ in the share of children not enrolled in school. Samson et al. also find gender differences in two datasets — in one, receipt of an OAP by a female has a greater impact than receipt by a male, and in another receipt of an OAP has greater impacts on the poorest girls’ enrolment (+ 7%, p <0.001) than on the poorest boys’ (+ 3%, p <0.05).
Table 1.
Impacts of unconditional cash transfers on education.
| Country/programme | Enrolment | Attendance |
| South Africa CSG | + 8.1 percentage points∗∗ (age 6)a + 1.8 percentage points∗∗ (age 7)a + 25%b§ |
|
| South Africa OAP | + 20–25%b§ + 3%∗∗ (poorest boys)c + 7%∗∗∗ (poorest girls)c |
|
| Zambia SCTSd§ | +10.4 percentage points (ages 5–6) + 3 percentage points (ages 7–18) + 8 percentage points (ages 14–15) −2 percentage points (ages 16–18) |
|
| Malawi Mchinji Cash Transfere | + 12 percentage points enrolment rate∗∗∗ + 5 percentage points newly enrolled∗∗∗ −3 percentage points drop-out rate∗∗∗ |
−1.3 days absent in previous month∗∗∗ |
Sources:
aCase, Hosegood, and Lund (2005), KwaZulu-Natal, Umkhanyakude District;
bSamson et al. (2004), National, Income and Expenditure Survey (2000) and The Labour Force Survey (September 2000);
cSamson et al. (2004), National, OHS data;
dMCDSS/GTZ (2006), Kalomo District;
eMiller, Tsoka, and Reichert (2008), Mchinji District.
∗p <0.10,
∗∗p <0.05,
∗∗∗p <0.01.
§p-Values not reported.
In Zambia, the pilot Social Cash Transfer Scheme (SCTS) found the largest enrolment increase for 14–15-year olds (8 percentage points), as well as 5–6-year olds (10.4 percentage points), both statistically significant. For girls, apart from the earliest years, enrolment was stagnant or decreased among recipients, but increased substantially for boys. The percentage of households not sending at least one child to school dropped from 41.4 to 33.8%,§6 suggesting that with a very small cash grant, parents may only send one child — usually a boy — to school (Ministry of Community Development and Social Services, Government of Zambia/German Technical Cooperation (MCDSS/GTZ), 2006). Data from the expanded SCTS found significant impacts on school enrolment for asset-poor households of between 6 (p <0.10) and 11.4 (p <0.05) percentage points in two of the three districts evaluated (Tembo & Freeland, 2008). Results from Malawi's expanded Mchinji Cash Transfer programme show the percentage of children newly enrolled in school more than twice as high in intervention households (8.3%) compared to comparison households (3.4%; p <0.001). Drop-out rates were also higher in the comparison group (5% vs. 2%; p <0.01) (Miller, Tsoka, & Reichert, 2008).
Other impacts from African programmes can be inferred from education expenditures (Figure 2). Given that poorer people normally spend a greater proportion of income on food, it is not surprising that a relatively small proportion of grant or overall spending is on education; nevertheless, the data does suggest that the grant helps parents to afford education.
Figure 2.
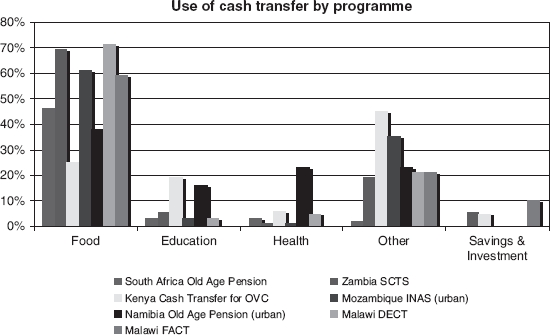
Use of unconditional cash transfers, by type of spending and programme.
Sources: Acacia Consultants (2007); Devereux (2002); Devereux et al. (2007); Devereux, Mvula, & Solomon (2006); MCDSS/ GTZ (2006); Moller and Ferreira (2003).
Note: In the case of Zambia SCTS the figure represents the proportion of overall spending by beneficiaries on health. In the case of Malawi DECT, these spending numbers refer to three months of the five-month programme period January–March 2007.
CCTs, where transfers are normally conditional on children enrolling in school and achieving around an 85% attendance rate, show strong impacts on schooling. Mexico's Programa de Educación, Salud y Alimentación (PROGRESA) had minimal impact on primary school enrolment, which was high at baseline, but at the secondary school level where enrolment started out low, impacts were high: 9.3 percentage points for girls (p =0.0002) and 5.8 points for boys (p =0.005) (transfer amounts were higher for girls to encourage their enrolment). The largest impact (14.8 percentage points, p =0.001) was on girls’ enrolment in Grade 7, the transition year when girls most often drop out (Schultz, 2001, 2004). The programme also reduced drop-out rates, grade repetition (Behrman, Sengupta, & Todd, 2001) and child labour (Parker & Skoufias, 2000), but had little impact on school attendance, achievement and school re-entry that was sustained (Behrman, Sengupta, & Todd, 2000, 2001).
Later analysis of impacts found a 23% (p <0.001) increase in secondary school enrolment from 1997 to 2002 in rural areas, and 6.5% (p <0.05) in urban areas, with effects stronger for girls than boys (Parker, 2003).
Nicaragua's Red de Protección Social (RPS) -with grants only for primary schooling — increased enrolment by a net 12.8 percentage points (p <0.001). The impacts were greatest for the extreme poor, at 25 percentage points (p <0.01). There was no significant difference between impacts on girls and boys, an outcome more likely at the primary than secondary level. RPS also increased school attendance rates by 20 percentage points (p <0.01) on average and 33 percentage points for the extreme poor (p <0.01). A follow-up survey two years after households left the programme found an enrolment drop, but still significantly higher rates than at baseline, suggesting some sustainable impact (Maluccio & Flores, 2005).
Brazil's Bolsa Escola also had some positive impacts on school attendance, drop-out rates and grade promotion (Cardoso & Souza, 2003; de Janvry, Finan, & Sadoulet, 2006), and Colombia's Familias en Acción had a small impact on enrolment in primary school, but higher secondary school enrolment impacts of 5.2 percentage points in urban areas and 10.1 points in rural areas (p <0.001) (Attanasio & Gomez, 2004). Ecuador's Bono de Desarrollo programme increased primary school enrolment by 9.8–12.8 percentage points (p <0.05), and reduced child labour by 15.4 (p <0.05) to 20.6 (p <0.001) points (Schady & Araujo, 2006). There was no impact on achievement (Ponce, 2006). Evaluations of CCT programmes in Honduras (International Food Policy Research Institute [IFPRI], 2003) and Jamaica (Levy & Ohls, 2007) showed little impact on enrolment, possibly because of high primary enrolment at baseline, or increased enrolment of the control group (in Honduras), but Honduras’ CCT did show robust increases in attendance and reductions in drop-out rates.
In Cambodia, the Scholarships for Girls Programme increased secondary enrolment by 22–33 (p < 0.001) percentage points (Filmer & Schady, 2006). An evaluation of Bangladesh's Reaching Out of School Children (ROSC) programme found no impact in areas receiving only grants to schools, but in areas with grants to schools plus cash allowances for students the project induced an average net increase in primary school enrolment of 8.9 percentage points (p <0.05) for children ages 6–14 (Ahmed, 2006). The CCT programme in Turkey raised secondary school enrolment for girls by 10.7 percentage points (p < 0.10). In rural areas the programme boosted beneficiary enrolment by 16.7 percentage points (p < 0.05) overall, especially for boys (22.8 percentage points, p <0.10) compared to non-beneficiaries (Ahmed et al., 2006). In some more socially conservative parts of southeastern Turkey, however, enrolment rates are still very low despite the CCT.7 Gender biases in sociocultural norms often overpowered the cash incentive — underscoring the importance of a contextual understanding of constraints on education, and of undertaking other approaches alongside transfers, responding to these constraints (Adato et al., 2007).
Cash transfers and health
Cash transfers can impact on health in several ways: by covering costs directly associated with accessing health care (including transportation, medical fees and the opportunity costs of time); by increasing quantity and quality of food consumed, and by incentivising participation in preventative health care and health education when cash is conditioned.
Table 2 shows impacts of unconditional cash transfers on health in Malawi, South Africa and Zambia. In Malawi, beneficiaries of the Mchinji Cash Transfer programme were more likely to receive care when sick compared to non-beneficiaries after three months in the programme (Miller & Tsoka, 2007). After one year in the programme, the percentage of beneficiary children reported to have been ill in the last month was 13 percentage points lower than non-beneficiaries (p <0.001) (Miller et al., 2008).
Table 2.
Impacts of unconditional cash transfers on health.
| Country/programme | Health outcomes |
| Malawi Mchinji Cash Transfera | Reduced illness in past month: −13 percentage points∗∗∗ (children) |
| South Africa OAPb | Improved health for all household members when income is pooled |
| Zambia SCTSc§ | Reduced incidence of illness: −12 percentage points (children 0–5 and adults 19–64) −14 percentage points (elderly) |
Sources:
∗p <0.10,
∗∗p <0.05,
∗∗∗p <0.01.
§p-Values not reported.
In South Africa, the OAP improved the health status of pensioners and other members of the household where pension income was pooled (Case, 2001). Qualitative research found that cash transfers made transportation to and fees for health services more affordable, enabled automatic qualification for health service fee exemptions, and strengthened social networks (Goudge et al., 2009).
In Zambia, the self-reported incidence of illness among beneficiaries of the SCTS fell between baseline and the evaluation, with the largest impacts among the elderly (a 14.2 percentage-point change), followed by children under five and adults of productive age (a 12 percentage-point change),§ possibly as a result of improved nutrition and hygiene (MCDSS/GTZ, 2006). Impacts on health from other country programmes could be inferred from health expenditures (see Figure 2), although these amounts were generally very small. This could also suggest reduced need for health-care services resulting from better health.
Figure 3 shows health-associated impacts of CCTs in four countries. The Honduras PRAF evaluation found a 15–21 percentage-point increase (p <0.001) in children's health check-ups, a 17–22 percentage-point (p < 0.001) increase in participation in growth monitoring, and a 13.7 percentage-point (p <0.001) to 19.5 percentage-point increase (p = 0.003) in attendance in the required protocol of antenatal care sessions (IFPRI, 2003). Despite greater health service utilisation, PRAF had no impact on health outcomes, most likely due to the small size of the transfer and implementation difficulties in attempts to improve the supply of health services (IFPRI, 2003).
Figure 3.
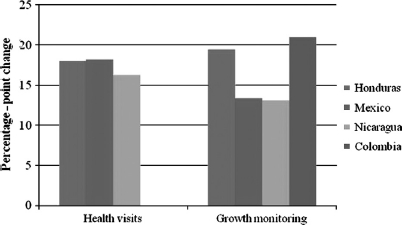
Impacts of conditional cash transfers on health service usage.
Sources: Attanasio et al. (2005); Gertler (2000); Gertler and Boyce (2001); IFPRI (2003); Maluccio and Flores (2005). Note: The mean of the range of estimates is plotted for Honduras. For Mexico the figure represents the impact on growth monitoring visits 15 months after baseline. No information on health visits separate from growth monitoring is available for Colombia.
The RPS programme in Nicaragua was able to successfully improve both health service utilisation and supply, though the evaluation did not measure health outcomes. The percentage of beneficiary children under three attending well-child visits increased by 16.3 percentage points (p <0.05) after one year, with decline in impact after two years as attendance rose within the control group. Participation in child growth promotion increased by 13.1 percentage points (p < 0.10) after two years. Impacts on attendance at both health centres and growth monitoring were larger among poorer RPS households (Maluccio & Flores, 2005).
In Jamaica, PATH increased the average number of preventive health-care visits for children 0–6by approximately 38% (p < 0.001), although this only represents one visit every 21 months. There was no impact on child immunisation rates, probably because these were high at the outset (Levy & Ohls, 2007).
Evidence from evaluations of Mexico's PROGRESA indicates that clinic visits by beneficiaries increased twice as much (p < 0.001) as visits by non-PROGRESA families over the evaluation period (Gertler & Boyce, 2001). Growth monitoring visits for beneficiary children under-two increased between 5.5 and 13.5 percentage points (p <0.05), varying with length of time in the programme (Gertler, 2000). Additionally, prenatal visits during the first semester of pregnancy increased by 8%§ among PROGRESA beneficiaries and initial visits in the second and third trimesters of pregnancy fell, a change that is recognised to improve the health of pregnant women and their infants (Skoufias, 2005).
PROGRESA significantly lowered illness rates among children under-five, as reported by mothers, but only for children who received benefits for at least 12 months (Gertler & Boyce, 2001). PROGRESA children under-five had a 12% (p <0.01) lower incidence of illness than non-PROGRESA children (Gertler, 2000). This estimate should be considered a lower bound of the impact of PROGRESA because mothers’ definitions of illness may have changed due to the health and nutrition education (a condition of the programme) and because the increased frequency of well-child preventive health visits may have made mothers more likely to report illness than before. Seventy percent of the monetary transfer, on average, was used for increased quantity and quality of household food consumption, perhaps contributing to improved health status for children and adults. Adult beneficiaries experienced fewer days incapacitated by illness, fewer days in bed due to illness and fewer days of difficulty with daily activities (Gertler & Boyce, 2001). Mexico's Oportunidades programme was associated with an 11% reduction in maternal mortality and a 2% reduction in infant mortality,§ with the stronger impacts in the poorer municipalities (Hernández, Ramírez, Moreno, & Laird, 2004).
Colombia's Familias en Acción increased attendance at growth monitoring and development checkups by 22.8 percentage points (p < 0.05) for beneficiary children below 24 months and by 33.2 percentage points (p < 0.05) for beneficiary children 24–48 months. Diarrhoea incidence fell by 11 percentage points (p <0.10) among children under-four living in rural areas. These impacts may result from health education, focusing on nutrition and hygiene, which trained mothers to better recognise symptoms of diarrhoea (Attanasio & Gomez, 2004; Attanasio, Gomez, Heredia, & Vera-Hernandez, 2005).
Impacts on food consumption and nutrition The vicious circle between HIV/AIDS and food and nutrition insecurity confers particular importance on the impacts that cash transfers have on food consumption and nutrition. Figure 2 illustrates the relative shares of cash transfer spending in seven programmes, with the highest by far on food, followed by spending on other goods (including clothing and shoes, blankets, transportation and other household expenditures) with smaller amounts spent on education, health and investments. In Free State Province, South Africa, a small survey found that grant income led to a higher rate of increase in food expenditures, compared to employment income (Booysen, 2004).
Table 3 summarises impacts of several unconditional cash transfer programmes on food consumption and nutrition. In most of the programmes evaluated, transfers were associated with reported reduced hunger and increased average meals per day, except when the transfer size was too small, as in Mozambique (Bazo, 1998 as cited in Low, Garrett, & Ginja, 1999). Under Zambia's SCTS, the number of beneficiary households having only one meal a day and reporting hunger pangs fell (MCDSS/GTZ, 2006). Short-duration cash transfer programmes in Malawi increased meals consumed per day (Devereux, Mthinda, Power, Sakala, & Suka, 2007; Devereux, Mvula, & Solomon, 2006). In South Africa, the presence of a pensioner lowered the probability that an adult had skipped a meal by approximately 25%§ if pension income was pooled (Case, 2001) and a female pensioner in the household had a greater impact on child hunger than adult hunger (Samson et al., 2004).
Table 3.
Impacts of unconditional cash transfer programmes on food consumption and nutrition.
| Country/programme | Food consumption | Hunger/meals per day | Dietary diversity | Nutritional status |
| Malawi Mchinji Cash Transfera | 83 percentage points difference in households reporting improved food intake∗∗∗ | + 23 percentage points difference in households reporting being satisfied after meal∗∗∗ −3.7 percentage points difference in households reporting very hungry∗∗ |
+ 3.2 food groups consumed per day, on average∗∗∗ | −11 percentage points child underweight∗ No change in mean WAZ |
| Mozambique GAPVUb | No impact | NA | NA | NA |
| South Africa CSG | + 1.5 percentage points (all food items)c + 1.2 percentage points (basic food items)∗∗∗c |
+ 0.2 HAZ, if received in first year of life and for at least 2/3 of first three years ∗d | ||
| South Africa OAP | + 1.5 percentage points (all foods)∗∗∗c + 10.5 percentage points in real adult food expenditure (HIV-affected households)§e |
−25% chance that adult skipped meal (if pension income pooledf −5.8% probability of hunger (young child)c | + 2.23 cms (girls) +0.88 cms (boys) if pension received by woman (national)∗g + 5 cms (Western Cape)§f | |
| Zambia SCTS§h | NA | -6 percentage points households eating one meal/day + 6 percentage points households eating three meals/ day | +12 percentage points households consuming vitamins 7x/ week +11.6 percentage points households consuming protein 7x/week +30.4 percentage points households consuming oil lx/week | Possible reduction in percentage of underweight children |
Sources:
∗p <0.10,
∗∗p <0.05,
∗∗∗p <0.01.
§p-Values not reported.
Note: The methods used in these studies are different and thus results should not be considered directly comparable.
Zambian cash transfer recipients consumed more protein, fats, fruits and vegetables, and fewer “inferior” foods associated with coping strategies used during food shortages (MCDSS/GTZ, 2006) and Malawian recipients consumed almost twice as many food groups than comparison households, and were more likely to eat higher quality foods, including fish, chicken, beans and vegetables (Miller et al., 2008).
Evidence of impacts of unconditional cash transfers on nutrition comes mainly from South Africa and Malawi. The CSG was shown to increase child height, but only if it was received early in a child's life and covered the majority of the first three years of life. A child receiving the CSG before age one, and for two-thirds of the first three years of life, has approximately 0.20 greater height-for-age (p <0.10) than a child not receiving the CSG. There is no effect for receipt covering less than 20% of the three-year window (Agüero, Carter, & Woolard, 2009). This demonstrates the importance of getting the transfer to mothers soon after the child is born, and of guaranteeing continued receipt during the critical period for child growth and development.
Evidence from South Africa also suggests that cash transfers targeting the elderly can improve children's nutritional status, especially for girls, particularly if transfers are received by female pensioners. Pensions received by women were associated with a 1.16 (p <0.10) increase in height-for-age for girls, though results were not significant for boys. There was no improvement if the pensioner was male (Duflo, 2000, 2003). Case (2001) found a one standard deviation increase in height-for-age (5 cms§) associated with a pensioner in the household, equivalent to six months worth of growth for black and coloured children age 0–6 (Case, 2001).
The Mchinji Cash Transfer Scheme demonstrated an 11 percentage-point reduction (p < 0.08) in the prevalence of underweight children (weight-for-age z-scores < −2), but no impact on mean weight (Miller, Tsoka and Reichert, 2008). Zambia's SCTS noted some impact on underweight in monitoring reports, but these figures may not be representative for large groups of children and across seasons (MCDSS/ GTZ, 2005; Sridhar & Duffield, 2006).
CCTs can affect nutrition through income, required participation in health and nutrition services, and nutrition education for mothers. In Mexico, PROGRESA households consumed 7.1% (p <0.05) more calories than control households, with the greatest impact on calories obtained from vegetable and animal products. Messages provided in nutrition education sessions to women contributed to improved eating habits among beneficiary families (Adato, Coady, & Ruel, 2000; Hoddinott, Skoufias, & Washburn, 2000).
In Nicaragua, RPS households consumed more food items than control households and consumed food with higher nutritional quality (Maluccio & Flores, 2005). In Colombia, Familias en Accion beneficiary households consumed a greater share of protein than control households (Attanasio & Mesnard, 2006). In Brazil, Bolsa Alimentação beneficiaries experienced a 9% (p < 0.01) increase in dietary diversity, equivalent to a 6% increase in per capita caloric availability and a 12% increase in caloric availability from healthier non-staples, especially fruits and vegetables (Olinto, Flores, Morris, & Viega, 2003). In Honduras, an evaluation identified no impact of PRAF on food consumption or dietary diversity; however, a more recent analysis found that households where the household head had primary school education consumed more healthier foods like meat, fish, eggs, dairy and fruits (Wiesmann & Hoddinott, 2007).
Table 4.
Unconditional cash transfer programme descriptions.
| Country | Programme | Eligibility |
| Malawi | Mchinji Cash Transfer Programme | Ultra poor (lowest expenditure quintile, below national ultra poverty line — one meal/day, cannot purchase essential non-food items, no valuable assets) and labour constrained (dependency ratio > 3, no household member 19–65 years able to work or >3 dependents per household member) |
| Mozambique | Gabinete de Apoio a População Vulnerável (GAPVU) | Absolute poor, household head unable to work and head is older woman 55+ or older man 60+, physically handicapped >18 or chronically sick >18, malnourished pregnant women, families with severely malnourished pregnant women or malnourished children |
| South Africa | Child Support Grant (CSG) | Children < 14 |
| South Africa | Old Age Pension (OAP) | Low-income men > 65, women > 60 |
| Zambia | Social Cash Transfer Scheme (SCTS) | Destitute (extremely needy, difficulties surviving, e.g., insufficient food, shelter, clothing, no assets or support) and incapacitated (no fit household member (19–64 and not ill) or one with > 3 dependents per household) |
Table 5.
Conditional cash transfer programme descriptions.
| Bangladesh | Reaching Out of School Children (ROSC) | Eligibility: Children who have not had an opportunity to attend primary school in remote areas/dropouts from primary Conditions: 75% attendance; 75% performance in exams |
| Brazil | Bolsa Alimentacäo |
Eligibility: Poor families with pregnant/lactating women and children 0–6 years with monthly per capita income below specified threshold Conditions: Minimum schedule of pre-natal and post-natal care visits; child growth monitoring; up-to-date vaccinations; participation in nutrition education |
| Bolsa Escola |
Eligibility: Families with children 6–15 years and per capita monthly incomes no greater than R$90 (US$43) Conditions: 85% school attendance |
|
| Cambodia | Japan Fund for Poverty Reduction (JFPR) Girls Scholarship Programme |
Eligibility: Girls starting Grade 7 Conditions: school enrolment; regular school attendance (no more than 10 days absence/year without “good reason”); maintaining a passing grade |
| Colombia | Familias en Acción |
Eligibility: Extremely poor families with children 0–6 years not participating in other programmes (health) and/or children 7–17 years enrolled in school (education) Conditions: Growth monitoring and development check-ups (children 0–7) |
| Ecuador | Bono de Desarrollo |
Eligibility: Households with children 0–16 years in the poorest two quintiles and poor households with elderly and/or disabled members Conditions: Bimonthly visits to health posts for growth and development check-ups and immunisations (children 0–5); School enrolment for children 6–15 years; school attendance of at least 90% |
| Honduras | Programa de Asignación Familiar (PRAF-II) |
Eligibility: Poor households with pregnant women and/or children under three (health) with children 6–12 who have not yet completed the fourth grade of primary school (education) Conditions: Check-ups at health centre (children 05); Growth monitoring and promotion for mothers with children < 2; At least five pre-natal checkups; Attendance in at least four training courses/ year (main beneficiary) |
| Jamaica | Programme of Advancement Through Health and Education (PATH) |
Eligibility: Poor children ages 0–6 (health) and 6–17 (or until completion of secondary school); persons >60 years; pregnant or lactating women up to six months after delivery; poor, disabled and destitute adults < 65; elderly > 65 Conditions: Health visits (children and adults and pregnant and lactating women); school attendance of at least 85% (children 6–17) |
| Mexico | Programa de Educación, Salud y Alimentación (Progresa)/ Opórtunidades |
Eligibility: Poor households Conditions: School attendance (80% monthly and 93% annually); compliance by all household members with schedule of preventative health check-ups; attendance at health and nutrition lectures (family member older than 15) |
| Nicaragua | Red de Protección Social (RPS) |
Eligibility: Poor households with children 0–5 (health); poor households with children 7–13 who have not yet completed fourth grade in primary school (education) Conditions: Attendance at health care visits (children 0–5); up-to-date vaccinations (children 0–5); monthly health education workshops |
| Turkey | Social Risk Mitigation Project (SRMP) |
Eligibility: Poorest 6% of the population with children 0–6 years or in primary or secondary school (ages 6–17) and pregnant mothers Conditions: Clinic visits for health check-ups; give birth in hospital; school attendance of at least 80%; cannot repeat same grade twice |
Sources: Ahmed et al. (2007); Levy and Ohls (2007); Maluccio and Flores (2005); World Bank (2009).
Figure 4 shows impacts of CCTs on nutritional status. PROGRESA reduced both stunting and anaemia. For children 0–3, stunting prevalence fell by 7.3 percentage points (p <0.10) and height-for-age z-scores increased by 0.16 standard deviations (not significant). For children 0–5, the impact is less (Hoddinott, 2008). An average beneficiary child (12–36 months) experienced a 1 cm/year increase in height (a 1.2% increase), equivalent to a 2.9% increase in lifetime earnings (Behrman & Hoddinott, 2001). Two studies found reductions in anaemia by 10.6 percentage points (p =0.03) for children 12–24 months (Rivera, Sotres-Alvarez, Habicht, Shamah, & Villalpando, 2004) and 25.5% (p = 0.01) for children 12–48 months (Gertler, 2004).
Figure 4.
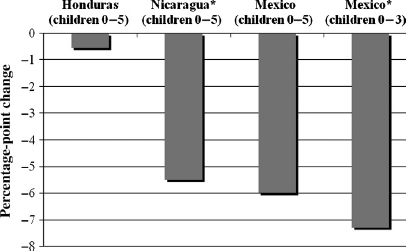
Impacts of conditional cash transfers on stunting prevalence.
∗p < 0.01.
Nicaragua's RPS brought about a 5.5 percentage-point (p < 0.10) reduction in stunting prevalence among children age 0–5 and an increase in mean height-for-age z-scores by 0.13 (not significant), perhaps because of the large transfer size (18% of average monthly household expenditure), and the inclusion of multiple nutrition-related conditions (Maluccio & Flores, 2005). However, even though RPS provided iron supplements, the programme had no impact on anaemia, perhaps due to inconsistent delivery, shortages and incomplete doses. While mothers reported receiving iron supplements, they did not always give them to children because of the perceived bad taste and negative gastrological effects (Adato & Roopnaraine, 2004).
Table 6.
Unconditional cash transfer programme evaluations reviewed.
| Country | Programme | Study area | Study sample | Time period | Study design |
| Malawi | Mchinji Cash Transfer Scheme | Mchinji District | 819 households (Round 1) 789 households (Round 2) 766 households (Round 3) |
March 2007-March/April 2008 | Longitudinal study with comparison group |
| Mozambique | GAP VU | Maputo | 41 beneficiaries 40 non-beneficiaries (who meet eligibility criteria) |
December 1997 | Control group, only elderly beneficiaries |
| South Africa | Social grants | Free State Province | 163 households | May 2001-December 2002 | Cohort study of AIDS-affected households |
| South Africa | Social grants | National | 30,000 households | 2000 | Model based on Income and Expenditure Survey, Labour Force Survey and Household Surveys |
| South Africa | Child Support Grant | KwaZulu-Natal Province | 245 children receiving the CSG before age 3 | 1993, 1998 and 2004 | Longitudinal KwaZulu-Natal Income Dynamics Study |
| South Africa | Child Support Grant | Umkhanyakude District, KwaZulu-Natal Province | 11,178 households | 2002–2004 | Longitudinal demographic surveillance (Africa Centre for Health and Population Study), no strict control group |
| South Africa | Old Age Pension | Langeberg Health District, Western Cape | 1300 individuals in 300 households | 1999 | Analysis of national survey data |
| South Africa | Old Age Pension | National | 9000 households | August-December 1993 | Analysis of health and economic survey |
| Zambia | SCTS | Two agricultural blocks in Kalomo District | Randomised sample of 303 households (274 at end line) | Kalomo: September 2004-September 2005 Kanchele: December 2004-December 2005 | Pre-post, no control group |
Sources: Acacia Consultants (2007); Agüero, Carter, and Woolard (2009); Bazo (1998); Booysen (2004); Case (2001); Case, Hosegood, and Lund (2005); Duflo (2000, 2003); MCDSS/GTZ (2006): Miller and Tsoka (2007); Miller, Tsoka, and Reichert (2008); Samson et al. (2004); Tarp et al. (2002).
Table 7.
Conditional cash transfer evaluations and analyses reviewed.
| Country | Programme | Study sample | Time period | Study design |
| Bangladesh | Reaching Out of School Childrena | 1500 households | 2006 | Quasi-experimental design; DD, PSM Ex-post quasi-randomised controlled trial |
| Brazilb | Boisa Alimentaçàoc | 2493 beneficiaries 506 excluded (but eligible) non-beneficiaries |
April 2002 (and retrospective data: six months previous) | |
| Bolsa Escolac | 2,387,677 children 10–15 | 2000 | Household data from 2000 census, PSM | |
| Bolsa Escolad | 293,800 eligible children | 2004 | Quasi-experimental, panel data from administrative records | |
| Cambodia | Japan Fund for Poverty Reductione | 3623 girls | 2003–2005 | RDD, PSM: girls with completed applications (not random) |
| Colombia | Familias en Acciónf | 10,742 households (64,500 individuals) | 2002–2003 | Cluster matched study, PSM |
| Ecuador | Bono de Desarrollo Humanog | 1306 households | 2003–2005 | Randomised longitudinal study |
| Honduras | PRAF h | 5683 households (26,866 individuals) | 2000–2002 | Randomised controlled trial |
| Jamaica | PATHI | 5000 households | 2004–2005 | Longitudinal study with comparison group, RDD |
| Mexico | Progresaj | 24,000 households | 1998–1999 | Randomised controlled trial |
| Progresak | 4000 children | 1998–1999 | Randomised controlled trial | |
| Progresal | Height: 155 children 12–36 months Anaemia: 2012 children 12–18 months | 1998–2000 | Randomised controlled trial | |
| Progresam | 650 children <12 months from low-income households (< 50th income percentile) | 1998–2000 | Randomised controlled trial | |
| Nicaragua | Red de Protección Social (RPS)n | 1581 households (baseline) 1453 households (2001) 1397 households (2002) | 2000–2002 | Cluster randomised controlled trial |
| Turkey | Social Risk Mitigation Projecto | 2905 households | 2005–2006 | Cross-sectional study, RDD, PSM |
Sources:
bMorris, Olinto, Flores, Nilson, and Figueiro (2004);
fAttanasio, Gomez, Heredia, and Vera-Hernandez (2005);
mRivera, Sotres-Alvarez, Habicht, Shamah, and Villalpando (2004);
Note: PSM, propensity score matching; RDD, regression discontinuity design; DD, difference-in-differences.
Colombia's Familias en Acción programme reduced the probability of stunting by 6.9 percentage points (p < 0.05) and increased mean height-for-age z-scores by 0.16 (p < 0.10) for children 0–24 months (Attanasio et al., 2005). Honduras’ PRAF had no significant impact on stunting or anaemia, likely due to the small transfer size (only 4% of average monthly household expenditure), sporadic transfer distribution and insufficient supply- side services (IFPRI, 2003; Maluccio, 2004). Understanding the reasons for CCT impacts on nutritional status is difficult because, to date, CCT impact evaluations have not yet disentangled the differential impact of individual programme components on observed outcomes (research on this topic could improve programme design).
Conclusion
Social protection is increasingly recognised as an essential part of a comprehensive response to the impact of HIV and AIDS on children and families. Cash transfers have demonstrated significant impacts on the human capital of children in many countries in Latin America and Asia, and evidence is building of such impacts from programmes in sub-Saharan Africa. If cash transfers succeed in increasing children's presence in school, their benefits may multiply by reducing HIVrisk, and increasing children's access to additional services. Cash transfers can be implemented in combination with other services to achieve broader objectives, building synergies in impacts and programme operations. In addition to promoting school enrolment and attendance, and preventative health-care activities, options under discussion or underway include early childhood development, after-school programmes, child protection and other social welfare services, information, education and communication activities, savings schemes, life skills training, voluntary testing and counselling, ART counselling and services, home-based care, micronutrient and food supplementation and nutrition counselling.
AIDS-affected families are diverse with respect to poverty level, education, household structure, stage of illness progression, ability to work, dependency ratios and access to assets. This argues for a mix of approaches rather than a single approach: food and nutrition programmes; public works and livelihoods support programmes are all important options for assisting families. Cash transfers appear to offer the best strategy for reaching families who are the very poorest, most capacity constrained and at-risk, in large numbers, relatively quickly, in a well-targeted and systematic manner, compared to alternative approaches. These are important considerations given the extent and nature of deprivation, the long-term risk to human capital and the current international and national political willingness to act.
Acknowledgements
Support for this research was provided by the Joint Learning Initiative on Children and AIDS (JLICA) and the Regional Network on AIDS, Livelihoods and Food Security (RENEWAL) of the International Food Policy Research Institute. We would like to thank JLICA and RENEWAL colleagues and donors, and the many programme implementers and researchers who assisted us in accessing documents.
Notes
Whether they achieve these goals depends on a number of political, economic and technical factors.
Several lines of argument and a vast amount of evidence point to the wisdom of targeting on poverty and vulnerability criteria, rather than on AIDS and orphans (see Adato & Bassett 2008).
See Tables 4through 7 later in this article for descriptions of the cash transfer programmes and evaluations reviewed.
The categories of “protective,” “preventative” and “promotional” social protection come from Guhan (1994). The category of “transformational” comes from Devereux and Sabates-Wheeler (2004).
HIV and AIDS can lead to increased food insecurity and malnutrition via undermining livelihoods, decreasing food intake and absorption and increasing energy requirements. In turn, food insecurity and malnutrition can heighten susceptibility to HIV exposure and infection via increasing transactional sex, migration, susceptibility to TB and mother-to-child transmission (For reviews of studies of these relationships see Gillespie & Kadiyala, 2005; Gillespie, Kadiyala, & Greener, 2007).
§ = Signifies that information on statistical significance is not available for the reported figure.
Survey data from Van and Diyarbakir provinces showed secondary school enrolment among beneficiaries at 11 and 65%, respectively, though this national dataset is not considered statistically representative at the provincial level (Adato et al., 2007).
References
- Acacia Consultants. Evaluation of cash transfer programme in Nairobi, Kwale, and Garissa districts: Final report. Kenya: Acacia Consultants/UNICEF; 2007. [Google Scholar]
- Adato M., Bassett L. A review of the evidence on impacts and key policy debates. Boston, MA: Joint Learning Initiative on Children and AIDS; 2008. What is the potential of cash transfers to strengthen families affected by HIV and AIDS? [Google Scholar]
- Adato M., Coady D., Ruel M. An operations evaluation of PROGRESA from the perspective of beneficiaries, promotoras, school directors, and health staff. 2000. Final report to PROGRESA, Government of Mexico. Washington, DC: International Food Policy Research Institute.
- Adato M., Roopnaraine T. A social analysis of 'Red de Protección Social' (RPS) en Nicaragua. Washington, DC: International Food Policy Research Institute; 2004. [Google Scholar]
- Adato M., Roopnaraine T., Smith N., Altinok E., Çelebioğlu N., Cemal S. An evaluation of the conditional cash transfer program in Turkey: Second qualitative and anthropological study. 2007. Final report submitted to the General Directorate of Social Assistance and Solidarity, Prime Ministry, Republic of Turkey. Washington, DC: International Food Policy Research Institute.
- Agüero J., Carter M., Woolard I. The impact of unconditional cash transfers on nutrition: The South African child support grant. 2009. Working Paper. Retrieved December 15, 2008, from http://www.aae.wisc.edu/carter/papers/acw2009.pdf. [Google Scholar]
- Ahmed A.U. Evaluating the reaching out-of-school children project in Bangladesh: A baseline study. Washington, DC: International Food Policy Research Institute; 2006. [Google Scholar]
- Ahmed A., Adato M., Kudat A., Gilligan D., Roopnaraine T., Colasan R. Impact evaluation of the conditional cash transfer program in Turkey. 2007. Final report. Washington, DC: International Food Policy Research Institute.
- Ahmed A.U., Gilligan D., Kudat A., Colasan R., Tatlidil H., Ozbilgin B. Interim impact evaluation of the conditional cash transfer program in Turkey: A quantitative assessment. Interim report. Washington, DC: International Food Policy Research Institute; 2006. [Google Scholar]
- Alderman H., Hoddinott J., Kinsey B. Long-term consequences of early childhood malnutrition. 2003. (FCND Discussion Paper No. 168) Washington, DC: International Food Policy Research Institute.
- Attanasio O., Gomez L.C. Evaluacion de impacto del programa familias en accion: Subsidios condicionados en la Red de Apoyo Social. London: Institute of Fiscal Studies; 2004. [Google Scholar]
- Attanasio O., Gomez L.C., Heredia P., Vera-Hernandez M. The short-term impact of a conditional cash subsidy on child health and nutrition in Colombia. London: Institute of Fiscal Studies; 2005. [Google Scholar]
- Attanasio O., Mesnard A. The impact of a conditional cash transfer programme on consumption in Colombia. Fiscal Studies. 2006;27(4):421–442. [Google Scholar]
- Baird S., Chirwa E., McIntosh C., Ozler B. The Short-Term Impacts of a CCT program for Schooling on the Sexual Behavior of Young Women. 2009. Unpublished manuscript. [DOI] [PubMed]
- Bazo G.A. The impact of the food subsidy program on the vulnerable elderly in the city of Maputo: A comparison of consumption levels between participants and nonparticipants. Maputo, Mozambique: Eduardo Mondlane University; 1998. [Google Scholar]
- Behrman J.R. Literature review on interactions between health, education, and nutrition and the potential benefits of intervening simultaneously in all three. Washington, DC: International Food Policy Research Institute; 2000. [Google Scholar]
- Behrman J., Hoddinott J. An evaluation of the impact of PROGRESA on child height. Washington, DC: International Food Policy Research Institute; 2001. [Google Scholar]
- Behrman J., Hoddinott J., Maluccio J., Quisumbing A., Martorell R., Stein A. The impact of experimental nutritional interventions on education into adulthood in rural Guatemala: Preliminary longitudinal analysis. Philadelphia, PA: University of Pennsylvania; 2003. Washington, DC: International Food Policy Research Institute, and Atlanta, GA: Emory University. Photocopy. [Google Scholar]
- Behrman J., Sengupta P., Todd P. The impact of PROGRESA on achievement test scores in the first year. Final report. Washington, DC: International Food Policy Research Institute; 2000. [Google Scholar]
- Behrman J., Sengupta P., Todd P. Progressing through PROGRESA: An impact assessment of a school subsidy experiment. Washington, DC: International Food Policy Research Institute; 2001. [Google Scholar]
- Booysen F. Social grants as safety net for HIV/ AIDS-affected households in South Africa. Journal of Social Aspects of HIV/AIDS Research Alliance. 2004;1(1):45–56. doi: 10.1080/17290376.2004.9724826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cardoso E., Souza A.P. The impact of cash transfers on child labor and school attendance in Brazil. Nashville, TN: Department of Economics, Vanderbilt University; 2003. [Google Scholar]
- Case A. Evidence from South African pensions. Princeton, NJ: Woodrow Wilson School of Public and International Affairs, Center for Health and Wellbeing, Princeton University; 2001. Does money protect health status? [Google Scholar]
- Case A., Hosegood V., Lund F. The reach and impact of child support grants: Evidence from KwaZulu-Natal. Development Southern Africa. 2005;22(4):467–482. [Google Scholar]
- de Janvry A., Finan F., Sadoulet E. Evaluating Brazil's Bolsa Escola program: Impact on schooling and municipal roles. Berkeley, CA: University of California at Berkeley; 2006. [Google Scholar]
- Devereux S., Sabates-Wheeler R. Transformative social protection. IDS Working Paper 232. Brighton: Institute of Development Studies, University of Sussex; 2004. [Google Scholar]
- Devereux S., Mthinda C., Power F., Sakala P., Suka A. An evaluation of concern worldwide's Dowa Emergency Cash Transfer Project (DECT) in Malawi, 2006/07. Lilongwe: Concern Worldwide; 2007. [Google Scholar]
- Devereux S., Mvula P., Solomon C. After the FACT: An evaluation of concern worldwide's food and cash transfers project in three districts of Malawi. Brighton, UK, and Lilongwe, Malawi: Institute of Development Studies (IDS), University of Sussex, and Concern Worldwide Malawi; 2006. [Google Scholar]
- Duflo E., Dupas P., Kremer M., Sinei S. Education and HIV/AIDS Prevention: Evidence from a randomised evaluation in Western Kenya. 2006. World Bank Policy Research Working Paper No. 4024. Washington, DC: World Bank.
- Duflo E. Child health and household resources in South Africa: Evidence from the old age pension program. American Economic Review. 2000;90(2):393–398. doi: 10.1257/aer.90.2.393. [DOI] [PubMed] [Google Scholar]
- Duflo E. Grandmothers and granddaughters: Old-age pensions and intrahousehold allocation in South Africa. World Bank Economic Review. 2003;17(1):1–25. [Google Scholar]
- Filmer D., Schady N. Getting girls into school: Evidence from a scholarship program in Cambodia. 2006. World Bank Policy Research Working Paper 3910. Washington, DC: World Bank.
- Gertler P. Do conditional cash transfers improve child health? Evidence from PROGRESA's control randomized experiment. American Economic Review. 2004;94(2):336–341. doi: 10.1257/0002828041302109. [DOI] [PubMed] [Google Scholar]
- Gertler P.J. The impact of PROGRESA on health. Washington, DC: International Food Policy Research Institute; 2000. [Google Scholar]
- Gertler P.J., Boyce S. An experiment in incentive-based welfare: The impact of PROGRESA on health in Mexico. 2001. Royal Economic Society (series on Royal Economic Society Annual Conference 2003). University of Warwick, Coventry, UK.
- Gillespie S., Kadiyala S. HIV/AIDS and food and nutrition security: From evidence to action. Washington, DC: International Food Policy Research Institute; 2005. Food Policy Review 7. [Google Scholar]
- Gillespie S., Kadiyala S., Greener R. Is poverty or wealth driving HIV transmission? AIDS. 2007;21(7):S5–S16. doi: 10.1097/01.aids.0000300531.74730.72. [DOI] [PubMed] [Google Scholar]
- Glewwe P., Jacoby H., King E. Early childhood nutrition and academic achievement: A longitudinal analysis. Journal of Public Economics. 2001;8:345–368. [Google Scholar]
- Goudge J., Russell S., Gilson L., Gumede T., Tollman S., Mills A. Illness-related impoverishmentin rural South Africa: Why does social protection work for some households but not others? Journal of International Development. 2009;21(2):231–251. [Google Scholar]
- Grantham-McGregor S., Cheung Y.B., Cuerto S., Glewwe P., Richter L., Strupp B. Developmental potential in the first 5 years for children in developing countries. The Lancet. 2007;369(9555):60–70. doi: 10.1016/S0140-6736(07)60032-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guhan S. Social security options for developing countries. International Labour Review. 1994;133(1):36–53. [Google Scholar]
- Hernández B., Ramírez D., Moreno H., Laird N. Resultados de la Evaluación Externa del Programa de Desarrollo Humano Oportunidades. [Results of the External Evaluation of Programa de Desarrollo Humano Oportunidades.] Cuernavaca, México: Instituto Nacional de Salud Publica/Oportunidades/CIESAS; 2004. Evaluación del impacto de Oportunidades en la mortalidad materna e infantile. [Google Scholar]
- Hoddinott J. Nutrition and conditional cash transfer (CCT) programs. Mimeo. Washington, DC: International Food Policy Research Institute (IFPRI); 2008. [Google Scholar]
- Hoddinott J., Skoufias E., Washburn R. The impact of PROGRESA on consumption: A final report. Washington, DC: International Food Policy Research Institute; 2000. [DOI] [PubMed] [Google Scholar]
- Hoddinott J., Maluccio J., Behrman J., Flores R., Martorell R. Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. The Lancet. 2008;371:411–416. doi: 10.1016/S0140-6736(08)60205-6. [DOI] [PubMed] [Google Scholar]
- International Food Policy Research Institute (IFPRI). PRAF/IBD project phase II: Intermediary impact. Washington, DC: International Food Policy Research Institute; 2003. [Google Scholar]
- Levy D., Ohls J. Evaluation of Jamaica's PATH program: Final report. Princeton, NJ: Mathematica Policy Research; 2007. [Google Scholar]
- Low J.W., Garrett J.L., Ginja V. Can cash transfer programs work in resource-poor countries? The experience of Mozambique. 1999. Food Consumption and Nutrition Division Discussion Paper 74. Washington, DC: International Food Policy Research Institute.
- Maluccio J. Effects of conditional cash transfer programs on current poverty, consumption, and nutrition. Säo Paulo, Brazil: Second International Workshop on Conditional Cash Transfer Programs; 2004. April. [Google Scholar]
- Maluccio J., Flores R. Impact evaluation of a conditional cash transfer program: The Nicaraguan Red de Proteccion Social. 2005. Research Report 141. Washington, DC: International Food Policy Research Institute.
- Martorell R. Results and implications of the INCAP follow-up study. Journal of Nutrition. 1995;125:S1127–S1138. doi: 10.1093/jn/125.suppl_4.1127S. [DOI] [PubMed] [Google Scholar]
- Martorell R. The nature of child malnutrition and its long-term implications. Food and Nutrition Bulletin. 1999;20:288–292. [Google Scholar]
- MCDSS/GTZ (Ministry of Community Development and Social Services, Government of Zambia/German Technical Cooperation) Monitoring report 2nd Edition: Pilot social cash transfer scheme, Kalomo District, Zambia. Lusaka: Author; 2005. [Google Scholar]
- MCDSS/GTZ. Evaluation report: Kalomo Social Cash Transfer Scheme. Lusaka: Author; 2006. [Google Scholar]
- MCDSS/GTZ. The pilot social cash transfer scheme - Zambia summary report. 5th ed. Lusaka: Author; 2007. [Google Scholar]
- Miller C., Tsoka M. $13 a month for half a year: Round 2 impact of the Mchinji cash transfer. 2007. December 11. PowerPoint Presentation to the National Social Protection Steering Committee, Government of Malawi, Lilongwe.
- Miller C., Tsoka M., Reichert K. Impact evaluation report: External evaluation of the Mchinji social cash transfer pilot, Draft. Boston, MA: Center for International Health and Development, Boston University, and Lilongwe: Center for Social Research, University of Malawi; 2008. [Google Scholar]
- Moller V., Ferreira M. Noncontributory pensions and poverty study. South African survey report. South Africa: Rhodes University and University of Cape Town; 2003. [Google Scholar]
- Morris S.S., Olinto P., Flores R., Nilson E.A.F., Figueiro A.C. Conditional cash transfers are associated with a small reduction in the rate of weight gain of preschool children in northeast Brazil. Journal of Nutrition. 2004;134(9):2336–2341. doi: 10.1093/jn/134.9.2336. [DOI] [PubMed] [Google Scholar]
- Olinto P., Flores R., Morris S., Viega A. The impact of the Bolsa Alimentação program on food consumption. 2003. August 16–22) Paper presented at annual meetings of the International Association of Agricultural Economists, Durban.
- Parker S. [Evaluation of the Impact of Oportunidades on school enrolment: primary, secondary and high school, Results of the External Evaluation of Programa de Desarrollo Humano Oportunidades.] México City: Secretaría de Desarrollo Social; 2003. Evaluación del impacto de Oportunidades sobre la inscripción escolar: primaria, secundaria y media superior, Evaluación de Resultados de Impacto del Programa de Desarrollo Humano Oportunidades. [Google Scholar]
- Parker S., Skoufias E. The impact of PROGRESA on work, leisure, and time allocation. Washington, DC: International Food Policy Research Institute; 2000. [Google Scholar]
- Pettifor A., Levandowski B., MacPhail C., Padian N., Cohen M., Rees H. Keep them in school: The importance of education as a protective factor against HIVinfection among young South African women. International Journal of Epidemiology. 2008;37(6):1266–1273. doi: 10.1093/ije/dyn131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollitt E., Gorman M.S., Engle P.L., Rivera J.A., Martorell R. Nutrition in early life and the fulfillment of intellectual potential. Journal of Nutrition. 1995;125(4; Suppl. 4):S1111–S1118. doi: 10.1093/jn/125.suppl_4.1111S. [DOI] [PubMed] [Google Scholar]
- Ponce J. The impact of a conditional cash transfer program on students' cognitive achievements: The case ofthe “Bono de Desarrollo Humano” of Ecuador. 2006. Unpublished work. Retrieved December 1, 2008, from www.flacso.org.ec/docs/desa_humano.pdf.
- Rivera J.A., Sotres-Alvarez D., Habicht J.P., Shamah T., Villalpando S. Impact of the Mexican program for education, health, and nutrition (PROGRESA) on rates of growth and anemia in infants and young children. Journal of the American Medical Association. 2004;291(21):2563–2570. doi: 10.1001/jama.291.21.2563. [DOI] [PubMed] [Google Scholar]
- Samson M., Lee U., Ndlebe A., MacQuene K., van Niekerk I., Gandhi V., et al. Final report: The social and economic impact of South Africa's social security system. 2004. (Research Paper #37). Cape Town, South Africa: Economic Policy Research Institute.
- Schady N., Araujo M.C. Cash transfers, conditions, school enrollment, and child work: Evidence from a randomized experiment in Ecuador. Washington, DC: World Bank; 2006. [Google Scholar]
- Schubert B., Huijbregts M. The Malawi Social Cash Transfer Pilot Scheme: Preliminary lessons learned. 2006. Paper presented at the conference on “Social Protection Initiatives for Children, Women and Families: An Analysis of Recent Experiences.” New York: United Nations Children's Fund.
- Schultz T.P. School subsidies for the poor: Evaluating a Mexican strategy for reducing poverty. Washington, DC: International Food Policy Research Institute; 2001. [Google Scholar]
- Schultz T.P. School subsidies for the poor: Evaluating the Mexican PROGRESA poverty program. Journal of Development Economics. 2004;74(1):199–250. [Google Scholar]
- Skoufias E. PROGRESA and its impacts on the welfare of rural households in Mexico. Washington, DC: International Food Policy Research Institute; 2005. [Google Scholar]
- Sridhar D., Duffield A. A review of the impact of cash transfer programmes on child nutritional status and some implications for Save the Children UK programmes. London, UK: Save the Children; 2006. [Google Scholar]
- Tembo G., Freeland N. Draft report to the Ministry of Community Development and Social Services. Lusaka: MCDSS; 2008. Impact of social cash transfers on investment, welfare and education outcomes: A retrospective study of the social cash transfer schemes in Chipata, Kalomo and Kazungula Districts of Zambia. [Google Scholar]
- UNICEF. Q&A: The Malawi social cash transfer pilot. 2007. Lusaka.
- Wiesmann D., Hoddinott J. The impact of a conditional cash transfer program on food consumption: The Honduras family allowance program (PRAF). 2007. April 29). Presentation at the Experimental Biology Conference, Washington, DC.
- World Bank. Conditional cash transfers: Reducing present and future poverty. Washington, DC: Author; 2009. [Google Scholar]