

Abstract
Background:
The femoral vein is an important site for central venous access in newborns and infants. The objectives of this study are to determine whether age or weight can be used clinically to predict the size of the femoral vein in newborns and infants, and to compare the size of the vein in each individual in both the supine and reverse Trendelenburg positions.
Results:
Analysis was done in 24 euvolemic individuals, each studied in both the supine and reverse Trendelenburg positions. Twelve of these individuals were newborns and 12 were infants. We used two-factor analysis of variance to explore differences between groups and multiple linear regression analysis to estimate the strength of the relationship between variables. In the infant group, there was a correlation between femoral vein diameter and weight. There was no correlation between weight and vessel size in newborns. In both the newborn and infant groups, vessel diameter increased with subjects in the reverse Trendelenburg position (P < 0.01).
Conclusion:
Weight is predictive of femoral vein diameter in infants, but not in newborns. In infants, weight might serve as a more sensitive index for estimating size of the femoral vein in order to determine accurately the size of intravascular catheter appropriate for cannulation. The diameter of the femoral vein increases in the reverse Trendelenburg position compared with that in the supine position in both newborns and infants. A large prospective study is required to validate these findings.
Keywords: femoral vein, infants, newborns, reverse Trendelenburg, ultrasound
Introduction
With increasing utilization of the femoral vein for central venous access in critically ill neonates and infants, data on the size of the femoral vein in this patient population has become invaluable in the selection of catheters of the appropriate size during femoral vein cannulation. There are few studies [1,2] in the literature that have assessed the diameter of the femoral vein. Most of these studies were carried out in older children and adults. The present study is limited to neonates and infants, and the major thrust of the study is to define the relationship, if any, between such readily ascertainable variables as the individual's age, weight and position (supine or reverse Trendelenburg), and femoral vein diameter.
Materials and methods
Patients
Twenty-four patients (12 newborns and 12 neonates) admitted to the nursery, pediatric wards, or pediatric intensive care unit, including patients in the pediatric outpatient clinic in our institution, were recruited into the study. All of the patients recruited were euvolemic and had no history of previous attempts at femoral vein cannulation.
The study was approved by the Institutional Review Board of Tulane University, New Orleans, Louisiana, USA. Written informed consent was obtained from the parents or guardian of each study subject.
The Site~Rite® II ultrasound device
The Site~Rite® II (Dymax Corp, Pittsburgh, PA, USA) is a portable ultrasound scanner that is specifically designed for guiding percutaneous vascular access. The device is lightweight, powered by rechargeable batteries, and mounted on a mobile stand. The ultrasound image is displayed on a 2-inch square screen with a simple gain control and a choice of image depth (2 or 4 cm). An on-screen depth guide provides markers at 0.5-cm intervals. The scanner is supplied with 7.5-MHz and 9-MHz mechanical sector transducers [3].
Technique
Twenty-four patients were prospectively studied using the portable ultrasound device (Site~Rite® II; Dymax Corp). A 9.0-MHz transducer was placed approximately 1 cm below the inguinal ligament, medial to the pulsation of the femoral artery in each individual. A copious amount of ultrasound gel was applied to the skin at the site corresponding to the femoral vessels and also on the tip of the transducer. By scanning with the transducer medial to the pulse of the femoral artery, the image of both femoral vessels is displayed on the 2-inch square screen. The vein is identified by its position relative to the artery, absence of pulsatility, and demonstration of collapsibility by applying gentle pressure. Once identified, the image was photographed with an instant camera fitted to the ultrasound device. Care was taken to avoid compression of the vein when the photograph was taken by ensuring that copious amounts of gel interfaced the skin and the tip of the transducer, and by avoiding excessive pressure on the transducer. The internal diameter of the vein was measured from the lateral to the medial wall using a calliper. The ultrasound device is calibrated so that the image projected is magnified at the ratio of 2:1. Accuracy of the measurement is in order of 0.5 cm. This technique was used on each individual and repeated in both supine and reverse Trendelenberg positions. The same femoral vein was measured in both positions for each of the individuals studied.
Statistics
Simple linear regression equations were calculated to predict vessel size using different variables. Pearson's correlation coefficient (r) was calculated for each variable. An r-value of 1.0 represents perfect correlation. Multiple linear regression was used to estimate the strength of the relationship between variables. We used two-factor analysis of variance to explore the difference between groups and positions. P < 0.05 was considered statistically significant.
Results
Twenty-four euvolemic individuals were studied, including 12 newborns and 12 infants. The mean age of the newborns was 1.8 ± 0.83 days (range 1-3 days), and there were eight males and two females in the newborn group (male:female ratio 2:1). The mean age of the infants was 7.3 ± 4.60 months (range 3 months-16 months) and there were 11 males and one female in the infant group.
Mean femoral vein diameter in the infant group increased from 0.88 ± 0.20cm in the supine position to 0.93 ± 0.22cm in the reverse Trendelenburg position (Fig. 1). This increase reached statistical significance (P < 0.01).
Figure 1.
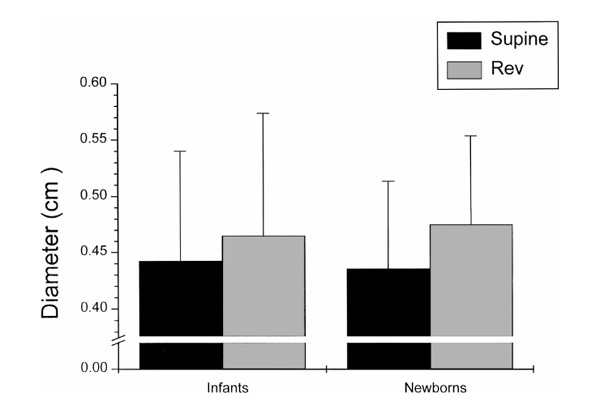
Mean femoral vein diameter in the supine versus reverse Trendelenburg positions.
In the newborn group, mean femoral vein diameter increased from 0.87 ± 0.16 cm in supine position to 0.95 ± 0.16 cm in the reverse Trendelenburg position (Fig. 1). This increase in vessel diameter was also statistically significant (P < 0.01).
A correlation existed between weight and femoral vein diameter in the infant group, with a correlation coefficient (r) of 0.80 (Fig. 2). The correlation coefficient (r) was 0.56 in the infant group when age was the variable considered. In the newborns, no correlation existed between weight or age and femoral vein diameter. The correlation coefficients (r) were 0.10 and 0.03 for age and weight, respectively, in the newborns.
Figure 2.
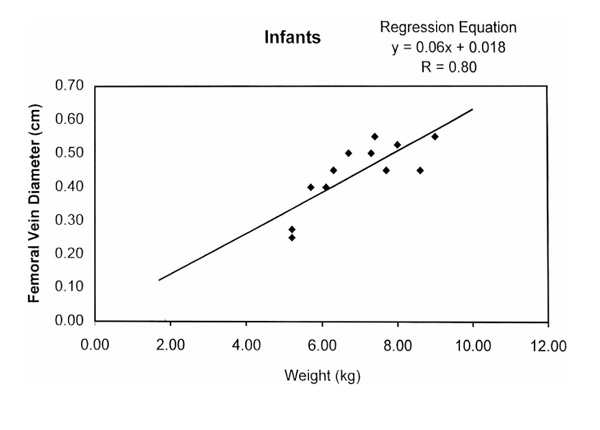
Scatter diagram showing the relationship between femoral vein diameter and weight in the infant group (♦). The line represents the linear regression equation. This line can be used to estimate the diameter of the femoral vein using a subject's weight. R, Pearson's correlation coefficient.
Discussion
The results of the present study show that a statistical correlation exists between weight and femoral vein diameter in infants. The study also shows that the femoral vein diameter increased in the reverse Trendelenburg position compared with in the supine position in both newborns and infants. These findings are comparable with those of Steinberg et al [1] and Mortensen et al [2], whose results showed a statistical correlation between body weight and internal diameter of femoral vein. Their study populations were older, however, and the technique of measurement of the internal diameter of the femoral vein differs from ours. Another major difference between the present study and those of Steinberg et al [1] and Mortensen et al [2] is that they showed a significant correlation between body surface area and the internal diameter of the femoral vein. Body surface area was not included in the present study. Femoral vein diameter increased in the reverse Trendelenburg position in our study and that of Mortensen et al [2]. This increase reached statistical significance, and might have resulted from venous pooling that occurred when central blood flow was restricted by positional dependency.
In the present study, there was no significant correlation between weight and femoral vein diameter in the newborns. Water constitutes 70% of lean body mass in newborns, and in the first few days of life an estimated 5-10% decrease in body weight occurs [4,5]. This continuous variation in weight in newborns makes it of less predictive value in the estimation of femoral vein diameter. A relatively stable body size index like surface area might be of more predictive value than weight, as shown by other studies [1,2]. A study to examine the relationship between body surface area and femoral vein diameter in the newborns is warranted.
The data produced by this somewhat limited study has potential application in clinical practice. These data can be transformed into a normogram (Fig. 2), which will provide a convenient method for estimating the cross-sectional internal diameter of the femoral vein for the purpose of selecting intravascular catheters of appropriate size. Mortensen et al [2] showed that the cross-sectional internal diameter of the femoral veins is closely related to the maximum outside diameter of the cannula or catheter that the vessel will accept. In clinical practice the outer diameter of intravascular catheters can be estimated using The Needle and Catheter Reference Chart (Cook® , Bloomington, In, USA) or the French Catheter Scale. This information together with a normogram of body weight and femoral vein internal diameter will be invaluable information for the selection of intravascular catheters of appropriate size for femoral vein cannulation in infants.
The increase in femoral vein diameter in the reverse Trendelenburg position (Fig. 1) has potential implications for clinicians attempting to cannulate femoral vein during hypovolemic states. Positioning of patients in a dependent manner increases the diameter of the femoral vein; this maneuver might increase the chance of successful cannulation during clinical hypovolemia. A comparison of femoral vein diameter in supine and reverse Trendelenburg positions between hypovolemic persons and euvolemic control individuals in a larger study with adequate power will be required to validate this theory. The present observation, although statistically significant, may not achieve clinical significance.
The main limitations of this study are the few number of patients involved and the possibility of interobserver variation in the estimation of femoral vein diameter with the ultrasound technique used. Despite the possibility of inter-observer error, the use of ultrasound techniques to estimate the internal diameter of major blood vessels has been well documented in human and animal studies [2].
In conclusion, the internal diameter of the femoral vein in infants can be estimated using weight. Also, the diameter of the femoral vein can be increased above the resting supine diameter when newborns and infants are put in reverse Trendelenburg positions, a technique that might have useful applications in clinical practice.
References
- Steinberg C, Weinstock DJ, Gold JP, et al. Measurement of central blood vessels in infants and children. Cathet Cardiovasc Diagn. 1992;27:197–201. doi: 10.1002/ccd.1810270308. [DOI] [PubMed] [Google Scholar]
- Mortensen JD, Tablot S, Burkart JA. Cross sectional internal diameters of human cervical and femoral blood vessels: relationship to subject's sex, age, body size. Anat Rec. 1990;225:115–124. doi: 10.1002/ar.1092260114. [DOI] [PubMed] [Google Scholar]
- Downie AC, Reidy JF, Adam AN. Short communication: tunnelled central venous catheter insertion via the internal jugular vein using a dedicated portable ultrasound device. Br J Radiol. 1996;69:178–181. doi: 10.1259/0007-1285-69-818-178. [DOI] [PubMed] [Google Scholar]
- Finberg L. Composition: chemical anatomy. Water and Electrolytes in Pediatrics, 2nd ed. Edited by Kravater RE, Hellerstein S. Philadelphia: WB Saunders . 1993. pp. 11–12.
- Kaplan SL. Normal growth (phases of growth). In Pediatrics, 18th ed Edited by Rudolph AM Norwalk, CT: Appleton & Lange. 1987. pp. 81–85.