

Abstract
Objective:
To evaluate the relationships between the changes in stroke volume index (SVI), measured in both the aorta and the pulmonary artery, and the changes in intrathoracic blood volume index (ITBVI), as well as the relationship between changes in aortic SVI and changes in the pulmonary artery wedge pressure (PAWP).
Design:
Prospective study with measurements at predetermined intervals.
Setting:
Medical intensive care unit of a university hospital.
Patients and methods:
One hundred and fifty-four measurements were taken in 45 critically ill patients with varying underlying disorders. Aortic SVI and pulmonary arterial SVI were determined with thermodilution. PAWP was measured using a pulmonary artery catheter. ITBVI was determined with thermal-dye dilution, using a commercially available computer system.
Results:
A good correlation was found between changes in ITBVI and changes in aortic SVI. However, this correlation weakened when changes in ITBVI were plotted against changes in pulmonary arterial SVI, which was in part probably due to mathematical coupling between ITBVI and aortic SVI. A good correlation between changes in ITBVI and changes in aortic SVI could also be established in most of the individual patients. No correlation was found between changes in PAWP and changes in aortic SVI.
Conclusion:
ITBVI seems to be a better predictor of SVI than PAWP. ITBVI may be more suitable than PAWP for assessing cardiac filling in clinical practice.
Keywords: cardiac output, intrathoracic blood volume, pulmonary artery wedge pressure, stroke volume, thermal dye dilution
Introduction
Assessing the volume status of critically ill patients is a routine task for intensivists. Clinical assessment by history taking, physical examination, fluid balance or radiographic findings provides belated or unreliable information [1,2,3,4]. Apart from clinical skills, invasive monitoring is widely applied as a tool for assessment of volume status. In its simplest form, central venous pressure (CVP) can be measured, by using a central venous catheter. In more complicated cases a pulmonary artery catheter is often used, with PAWP as the variable for determining cardiac filling. Because CVP and PAWP depend not only on cardiac filling, but also on ventricular compliance, these pressures are only poor reflections of a patient's volume status [5,6,7]. Moreover, CVP and PAWP are absolute intravascular pressures, meaning that changes in intrathoracic pressures will influence the recorded values of CVP and PAWP. This applies in particular to mechanically ventilated patients who are ventilated with positive end-expiratory pressure. Thus, therapeutic decisions based on CVP and/or PAWP may be based on inaccurate measures of a patient's volume status.
The thermal-dye dilution technique was originally introduced as a method to measure extravascular lung water (EVLW) [8]. In recent years the emphasis has moved to the ITBVI as the most important variable that can be determined using this technique. In a limited number of studies, ITBVI has been shown to correlate well with the cardiac index (CI), and it appears to be a better measure of cardiac filling than CVP or PAWP [7,9,10,11]. Lichtwarck-Aschoff et al [7] showed a correlation coefficient of 0.65 between changes in ITBVI and SVI in 21 patients with acute respiratory failure. Gödje et al [9] showed a correlation coefficient of 0.87 between changes in ITBVI and changes in CI in cardiac surgery patients. Recently, Sakka et al [10] showed a correlation coefficient of 0.67 between changes in ITBVI and changes in SVI during the early phase of haemodynamic instability in patients with sepsis or septic shock.
In a mixed group of critically ill patients we studied the correlations between SVI and PAWP, measured using a pulmonary artery catheter, and the correlations between SVI and ITBVI, measured with a commercially available computer system using the thermal-dye dilution technique.
Methods
The data presented in this study were prospectively obtained from 45 critically ill patients. All patients concomitantly participated in four other studies. In those studies, haemodynamic patterns of specific clinical entities, with the emphasis on EVLW, were investigated. ITBV, however, was measured specifically for the present study. The groups consisted of patient with acute respiratory distress syndrome (ARDS), patients with acute cardiogenic pulmonary oedema [12], patients with a septic shock [13], and patients with hepatic cirrhosis requiring a transjugular intrahepatic portosystemic shunt (TIPS). In all of these studies, patients were monitored using a pulmonary artery catheter (7.5-F Swan Ganz-catheter, Model VS 1721; Ohmeda, Swindon, UK) and a 4-Fr fiberoptic catheter (Pulsiocath PV 2024; Pulsion, Munich, Germany), introduced into the descending aorta through a 6-Fr introducer sheath (Model 616150A; Ohmeda) and connected to a computer system (COLD Z-021 system; Pulsion) for determination of ITBVI.
Haemodynamic measurements, both with the pulmonary artery catheter and the thermal-dye dilution technique, were made at regular intervals during the first 24 h after admission to the intensive care unit. Fluid therapy was given as long as every seperate fluid bolus (500 ml colloids over 20 min) resulted in an increase of CI of 10% or more. PAWP was not allowed to exceed 18 mmHg in patients with acute cardiogenic pulmonary oedema, however, and was not allowed to exceed 16 mmHg in the other categories. Whenever CI increased by less than 10%, fluid challenges were stopped, regardless of the PAWP at that point, and inotropes and/or vasopressors were given when appropriate.
All study protocols were approved by the Local Ethics Committee, and informed consent was given by each patient or his/her next of kin.
The pulmonary artery catheter was used for measurements of CVP and PAWP, with the midchest level as zero reference. The heart rate was recorded continuously with one of the standard leads of the electrocardiogram. PAWP was measured exclusively by the investigators and not by the nursing staff, taking problems associated with PAWP measurement and recommendations from the literature into account [14].
The COLD system was connected both to the pulmonary artery catheter and to the fibreoptic catheter in the aorta, which enabled us to determine CI in the pulmonary artery and in the aorta in one measurement. SVI was calculated by dividing the respective CIs by the accompanying heart rate. The COLD system was also used for determination of ITBVI. Measurements were done by injecting 10 cm3 of an ice-cold indocyanin green (ICG) solution (2 mg/ml). The mean value of two measurements was used for analysis.
For details concerning the thermal-dye dilution method, see Lewis et al [8] and Pfeiffer et al [15]. Briefly, the method uses two indicators (ie ice-cold water and ICG). Cold is distributed throughout both intravascular and extravascular volume, whereas ICG remains in the intravascular volume. Both indicators are injected into the right atrium, and concentration changes with time are recorded in the descending aorta. Thus, dilution curves are obtained for both indicators. From the thermodilution curve aortic CI is determined. From each indicator's dilution curve a mean transit time (MTT) can be derived. MTT is composed of the appearance time, which is the time until the first indicator particle has arrived at the point of detection, and the mean time difference between the occurrence of the first particle and all the following particles [15]. The product of CI and MTT is the volume between the site of injection and the site of detection. ITBVI can be calculated using the following formula:
ITBVI (ml/m2) = CI × MTTaorta (ICG)
The correlations between the variables, as well as correlations between the changes in these variables, were studied using linear regression analysis. Changes in the variables were calculated by subtracting the first from the second measurement, the second from the third, and so on. To reduce the influence of changes in contractility and afterload, we used only those values for the analysis for which no supportive adjustments were made with inotropes and/or vasopressors between the measurements. Both pooled and intraindividual relationships were studied. The method described by Bland and Altman [16] was used for assessing differences between pulmonary arterial CI and aortic CI.
Results
A total of 283 haemodynamic measurements were made in 45 critically ill patients (10 patients with ARDS, 10 patients with acute cardiogenic pulmonary oedema, 15 patients with septic shock and 10 patients with hepatic cirrhosis requiring TIPS). After discarding the measurements in which supportive adjustments were made with inotropes and/or vasopressors, 154 changes between measurements were left for analysis. Details concerning the subgroups are shown in Table 1. Thirty-six patients were mechanically ventilated throughout the study protocol.
Table 1.
Patients and measurement details in the various disease categories
| Disease category | n | Mechanical ventilation | Inotropes and/or vasopressors | Measurement points (h) |
| ARDS | 10 | 10 | 3 | 0, 0.5, 1.5, 2.5, 3.5, 4.5 |
| Acute cardiogenic pulmonary oedema | 10 | 10 | 10 | 0, 1, 3, 6, 12, 18, 24 |
| Sepsis | 15 | 13 | 15 | 0, 1, 3, 6, 12, 18, 24 |
| TIPS | 10 | 3 | 2 | -1, 0, 2, 4, 6, 24 |
| Total | 45 | 36 | 30 |
Pulmonary arterial CI and aortic CI correlated well (Fig. 1). In a Bland-Altman analysis, a mean difference of 0.49 l/min per m2 (95% confidence interval 0.45-0.53) was found, with a lower limit of -0.41 l/min perm2 and an upper limit of +1.39 l/min per m2.
Figure 1.
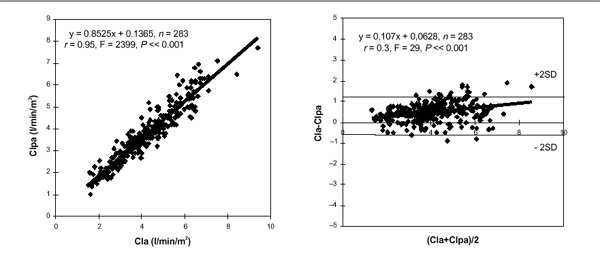
Correlation between CI measured in the pulmonary artery (CIpa) and CI measured in the aorta (CIa) in the left panel. Right panel shows Bland-Altman analysis. SD, standard deviation.
Figure 2 shows the regression analysis of the pooled data. A strong correlation was found between the changes in ITBVI and changes in aortic SVI. This correlation weakened significantly when changes in ITBVI were plotted against changes in pulmonary arterial SVI, however (Fisher Z test P < 0.001).
Figure 2.
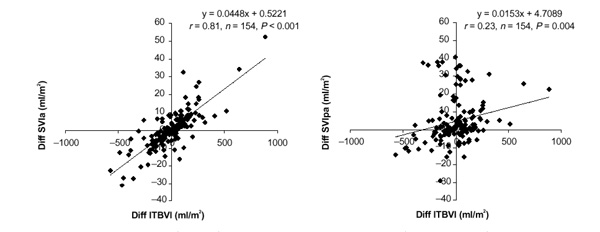
The correlation between changes in ITBVI (Diff ITBVI) and changes in SVI measured in the aorta (Diff SVIa; left panel), and the correlation between changes in ITBVI (Diff ITBVI) and changes in SVI measured in the pulmonary artery (Diff SVIpa; right panel).
Figure 3 shows the individual regression lines of PAWP versus aortic SVI of the patients in the various disease categories. From the graphs it is clear that there are large interindividual differences in correlation in all of the disease categories.
Figure 3.
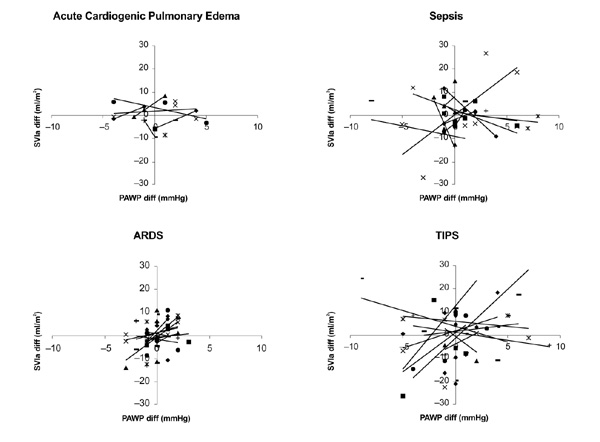
Individual regression of PAWP versus aortic SVI (SVIa) in the various disease categories.
Figure 4 shows the individual regression lines of ITBVI versus aortic SVI of the patients in the various disease categories. In three disease categories (sepsis, ARDS and TIPS) a positive correlation was noted in almost all patients, although interindividual differences exist in the steepness of the regression lines. Only in the patients with acute cardiogenic pulmonary oedema could such a relationship not be confirmed. It has to be noted, however, that in this patient group many supportive adjustments were made with inotropes and/or vasopressors during the course of the measurements, so that the relationships were based on a small number of measurements.
Figure 4.
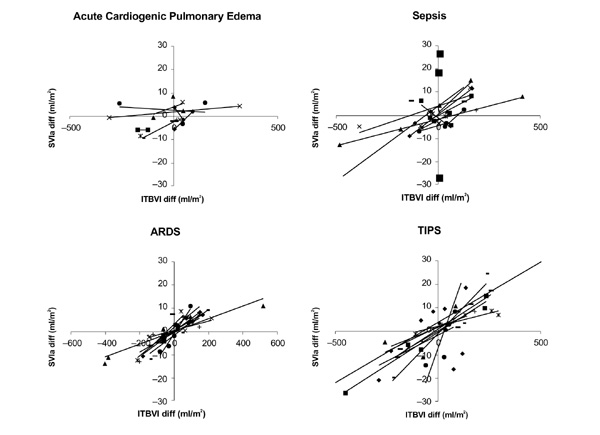
Individual regression lines of ITBVI versus aortic SVI (SVIa) in the various disease categories.
Discussion
The present study shows a good correlation between changes in ITBVI and aortic SVI. This correlation could also be found in the individual patients in three of the four disease categories studied. However, the correlation weakened when, in the pooled data, ITBVI was plotted against pulmonary arterial SVI. No consistent correlation could be established between PAWP and aortic SVI.
CVP and PAWP are pressures that are used in clinical practice to assess cardiac filling or cardiac preload. Under experimental conditions, the so-called ventricular performance curves show a close curvilinear relationship between the end-diastolic pressure of the ventricle and the stroke volume or cardiac output, provided that contractility and afterload are held constant. In clinical practice this relationship may be distorted for several reasons.
The first reason is that several assumptions have to be made for PAWP to reflect the end-diastolic volume of the ventricle. PAWP must be accurately measured, it must reflect left atrial pressure (LAP), LAP must reflect left ventricular end-diastolic pressure (LVEDP), and then LVEDP must relate directly to left ventricular end-diastolic volume to be a true measure of cardiac filling.
In clinical practice there are many doubts about the accuracy of the PAWP measurement. Accurate measurements are frequently prevented by technical aspects. There is also an astonishing lack of basic knowledge among clinicians and nurses on how the measurement should be performed [17,18,19,20]. Apart from the technical factors, there are also clinical entities that interfere with the reliability of PAWP in reflecting LAP accurately. Pulmonary venous obstruction (eg tumours, atrial myxomas, mediastinal fibrosis, pulmonary venous thrombosis) increases PAWP, without an accompanying increased LAP. Disparity between LAP and LVEDP is found in the case of mitral stenosis, and, perhaps more often, in the presence of a decreased left ventricular compliance. A change in ventricular compliance, often met in critically ill patients, may also distort the assumed relationship between LVEDP and left ventricular end-diastolic volume. Furthermore, interventricular dependence also influences the pressure-volume curve of the left ventricle. Hence, disease states with an increased right ventricular afterload (eg acute pulmonary hypertension) will also impair left ventricular compliance. Finally, all intrathoracic pressure changes will affect the recorded values of CVP and PAWP, because these pressures are measured relative to ambient air pressure. Therefore, the measured pressures are not transmural pressures, which is especially true in case the tip of the pulmonary artery catheter is located outside a West zone III [21].
The second reason for the distorted relationship between the cardiac filling pressures and the stroke volume in clinical practice is that the requirement for the contractility and the afterload to be constant is hardly ever met in clinical practice. Leaving aside the question of whether this requirement is verifiable, practically all interventions interfere either with the myocardial contractility (eg inotropes) or with the ventricular afterload (eg vasoconstrictors, vasodilators). Although we tried to make an approximate correction for this phenomenon, by leaving out those measurements in which supportive changes were made with inotropes or vasoactive medications, it cannot be ruled out that this phenomenon played a role in the results we found.
Taking into account the reasons indicated above, it is not surprising that we did not find a consistent correlation between PAWP and aortic SVI in the individual patients. The present results confirm those of earlier studies [7,9,10,11]. In the patients we studied there were no major differences in the correlation of PAWP and aortic SVI between the different disease states, regardless of whether all patients were ventilated mechanically (ARDS), or only a minority of patients (TIPS) was on mechanical ventilation. In conclusion, PAWP is influenced by so many factors other than cardiac filling that it is not a reliable indicator of cardiac filling in clinical practice. Therefore, the absolute values of these two variables are not an adequate reflection of the cardiac filling conditions of an individual patient.
Changes in ITBVI showed better correlations with changes in aortic SVI than did changes in PAWP, which is also in accordance with earlier findings [7,9,10,11]. From the individual regression lines (Fig. 4), however, it is clear that differences between the individual slopes and, likewise, differences between the distinct disease categories may exist. The interindividual differences may be the consequence of the fact that aortic SVI not only depends on preload, but also on contractility and afterload. Contractility may differ from patient to patient, and from disease to disease. Also, afterload may influence aortic SVI to an extent that depends on the underlying disease. Especially in the case of a diminished contractility, afterload may be a decisive factor in the final aortic SVI. Hence it is understandable that the correlations between ITBVI and aortic SVI in patients with acute cardiogenic pulmonary oedema were not as firm as in the other subgroups. In conclusion, it may still be hard to predict whether an individual patient has reached optimal cardiac filling when a certain value of ITBVI is measured.
By connecting the Swan-Ganz catheter to the COLD system, time differences between pulmonary arterial CI and aortic CI were precluded. Pulmonary arterial CI and aortic CI were closely correlated, with a mean higher value of aortic CI of 0.49 l/min per m2. This is in accordance with an earlier report [11]. However, the difference in the correlation between ITBVI and pulmonary arterial SVI, and the correlation between ITBVI and aortic SVI (Fig. 2) was striking. This could be due to mathematical coupling, because the formula used to determine ITBVI includes aortic CI, and thus aortic SVI indirectly, as a variable [22]. Lichtwarck-Aschoff et al [23], however, showed that under experimental conditions an increase in aortic CI by inotropes, with a constant ITBVI, did not influence the measured value of ITBVI, because the MTT decreased concomitantly.
The thermal-dye dilution technique was originally developed to determine EVLW. As a consequence, validation of the method is based on comparison of measured values of EVLW with gravimetrically determined EVLW. These values correlate well, with an overestimation of the thermal-dye technique in the lower range and an underestimation in the higher range of EVLW values [24,25,26]. In a recent study [27], circulating (total) blood volume measured with the COLD system correlated well with standard methods for measuring circulating blood volume. From these results, it has been assumed that measured ITBVI also correlates well with the actual intrathoracic volume. This has not been validated formally, however. On the other hand, the correlations we found are those one would expect on the basis of physiological knowledge. This implies that ITBVI, at least, is a reflection of the actual intrathoracic volume.
In conclusion, the present study shows that the cardiac filling in critically ill patients may not adequately be predicted by PAWP. ITBVI seems to be a more reliable predictor of cardiac filling, because changes in ITBVI closely relate with changes in aortic SVI. Partially, however, this may be due to mathematical coupling. Whether the use of ITBVI for guidance of fluid therapy will improve patient outcome should be subject to further studies.
Acknowledgments
Acknowledgements
The authors would like to thank Professor Jean-Louis Vincent (Free University of Brussels, Belgium) for his comments on earlier versions of this manuscript.
References
- Roos AN, Westendorp RGJ, Frölich M, Meinders AE. Weight changes in critically ill patients evaluated by fluid balances and impedance measurements. Crit Care Med. 1993;21:871–877. doi: 10.1097/00003246-199306000-00015. [DOI] [PubMed] [Google Scholar]
- Roos AN, Westendorp RGJ, Brand R, Souverijn JHM, Frölich M, Meinders AE. Predictive value of tetrapolar body impedance measurements for hydration status in critically ill patients. Intensive Care Med . 1995;21:125–131. doi: 10.1007/BF01726535. [DOI] [PubMed] [Google Scholar]
- Sivak ED, Bradford JR, O'Donovan PB, Bockowski GP. Value of extravascular lung water measurement vs portable chest X-ray in the management of pulmonary edema. Crit Care Med. 1983;11:498–501. doi: 10.1097/00003246-198307000-00003. [DOI] [PubMed] [Google Scholar]
- Laggner A, Kleinberger G, Haller J, Lenz K, Sommer G, Druml W. Bedside estimation of extravascular lung water in critically ill patients: comparison of the chest radiograph and the thermal-dye technique. . Intensive Care Med. 1984;10:309–313. doi: 10.1007/BF00254322. [DOI] [PubMed] [Google Scholar]
- Shippy CR, Appel RL, Shoemaker WC. Reliability of clinical monitoring to assess blood volume in critically ill patients. Crit Care Med. 1984;12:107–112. doi: 10.1097/00003246-198402000-00005. [DOI] [PubMed] [Google Scholar]
- Zarins CK, Virgillio RW, Smith DE, Peters RM. The effect of vascular volume on positive endexpiratory pressure induced cardiac output depression and wedge-left atrial discrepancy. J Surg Res. 1977;23:348–360. doi: 10.1016/0022-4804(77)90072-5. [DOI] [PubMed] [Google Scholar]
- Lichtwarck-Aschoff M, Zeravik J, Pfeiffer UJ. Intrathoracic blood volume accurately reflects circulatory volume status in critically ill patients with mechanical ventilation. Intensive Care Med. 1992;18:142–147. doi: 10.1007/BF01709237. [DOI] [PubMed] [Google Scholar]
- Lewis FR, Elings VB, Sturm JA. Bedside measurement of lung water. . J Surg Res. 1979;27:250–261. doi: 10.1016/0022-4804(79)90138-0. [DOI] [PubMed] [Google Scholar]
- Gödje O, Peyerl M, Seebauer T, Lamm P, Mair H, Reichart B. Central venous pressure, pulmonary capillary wedge pressure and intrathoracic blood volumes as preload indicators in cardiac surgery patients. Eur J Cardiothorac Surg. 1998;13:533–540. doi: 10.1016/s1010-7940(98)00063-3. [DOI] [PubMed] [Google Scholar]
- Sakka SG, Bredle DL, Reinhart K, Meier-Hellmann Comparison between intrathoracic blood volume and cardiac filling pressures in the early phase of hemodynamic instability of patients with sepsis or septic shock. J Crit Care. 1999;14:78–83. doi: 10.1016/s0883-9441(99)90018-7. [DOI] [PubMed] [Google Scholar]
- Hoeft A. Transpulmonary indicator dilution: an alternative approach for hemodynamic monitoring. 1995 Yearbook of Intensive Care and Emergency Medicine. 1995:593–605. [Google Scholar]
- Bindels AJGH, van der Hoeven JG, Meinders AE. Pulmonary artery wedge pressure and extravascular lung water in patients with acute cardiogenic pulmonary edema requiring mechanical ventilation. Am J Cardiol. 1999;84:1158–1163. doi: 10.1016/s0002-9149(99)00527-5. [DOI] [PubMed] [Google Scholar]
- Bindels AJGH, van der Hoeven JG, Meinders AE. Extravascular lung water in patients with septic shock during a fluid regimen guided by cardiac index. Neth J Med. 2000 doi: 10.1016/s0300-2977(00)00056-5. [DOI] [PubMed] [Google Scholar]
- Bennett D, Boldt J, Brochard L, et al. Expert panel: the use of the pulmonary artery catheter. Intensive Care Med. 1991;17 (Suppl):I–VIII. doi: 10.1007/BF01704735. [DOI] [PubMed] [Google Scholar]
- Pfeiffer UJ, Backus G, Blümel G, et al. A fiberoptics based system for integrated monitoring of cardiac output, intravascular blood volume, extravascular lung water, O2-saturation and a-v differences. Practical Applications of Fiberoptics in Critical Care Monitoring. 1990:114–125. [Google Scholar]
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;i:307–310. [PubMed] [Google Scholar]
- Iberti TJ, Fischer EP, Leibowitz AB, et al. A multicenter study of physicians' knowledge of the pulmonary artery catheter. . JAMA. 1990;264:2928–2932. [PubMed] [Google Scholar]
- Gnaegi A, Feihl F, Perret C. Intensive care physicians' insufficient knowledge of right-heart catheterization at the bedside: time to act? Crit Care Med. 1997;25:213–220. doi: 10.1097/00003246-199702000-00003. [DOI] [PubMed] [Google Scholar]
- Iberti TJ, Daily EK, Leibowitz AB, et al. Assessment of critical care nurses' knowledge of the pulmonary artery catheter. . Crit Care Med. 1994;22:1674–1678. [PubMed] [Google Scholar]
- Burns D, Burns D, Shively M. Critical care nurses' knowledge of pulmonary artery catheters. Am J Crit Care. 1996;5:49–54. [PubMed] [Google Scholar]
- Versprille A. The pulmonary circulation during mechanical ventilation. Acta Anaestesiol Scand. 1990;34 (Suppl 94):51–62. doi: 10.1111/j.1399-6576.1990.tb03223.x. [DOI] [PubMed] [Google Scholar]
- Wickerts CJ, Jakobson J, Frostell C, Hedenstierna G. Measurement of extravascular lung water by thermal-dye dilution technique: mechanisms of cardiac output dependence. Intensive Care Med. 1990;16:115–120. doi: 10.1007/BF02575305. [DOI] [PubMed] [Google Scholar]
- Lichtwarck-Aschoff M, Beale R, Pfeiffer UJ. Central venous pressure, pulmonary artery occlusion pressure, intrathoracic volume, and right ventricular end-diastolic volume as indicators of cardiac preload. . J Crit Care. 1996;11:180–188. doi: 10.1016/s0883-9441(96)90029-5. [DOI] [PubMed] [Google Scholar]
- Effros RM. Lung water measurements with the mean transit time approach. J Appl Physiol. 1985;59:673–683. doi: 10.1152/jappl.1985.59.3.673. [DOI] [PubMed] [Google Scholar]
- Slutsky RA, Higgins ChB. In vivo validation of the thermal-green dye technique for measuring extravascular lung water. Crit Care Med . 1985;13:432–435. doi: 10.1097/00003246-198505000-00014. [DOI] [PubMed] [Google Scholar]
- Staub NC. Clinical use of lung water measurements. Report of a workshop. Chest. 1986;90:588–594. doi: 10.1378/chest.90.4.588. [DOI] [PubMed] [Google Scholar]
- Kisch H, Leucht S, Lichtwarck-Aschoff M, Pfeiffer UJ. Accuracy and reproducibility of the measurement of actively circulating blood volume with an integrated fiberoptic monitoring system. Crit Care Med . 1995;23:885–893. doi: 10.1097/00003246-199505000-00017. [DOI] [PubMed] [Google Scholar]