

Abstract
This article focuses on results of the systematic review from the Guide for Useful Interventions for Activity in Latin America project related to school-based physical education (PE) programs in Latin America. The aims of the article are to describe five school-based PE programs from Latin America, discuss implications for effective school-based PE recommendations, propose approaches for implementing these interventions, and identify gaps in the research literature related to physical activity promotion in Latin American youth. Following the US Community Guide systematic review process, five school-based PE intervention studies with sufficient quality of design, execution and detail of intervention and outcomes were selected for full abstraction. One study was conducted in Brazil, two studies were conducted in Chile and two studies were conducted on the US/Mexico border. While studies presented assorted outcomes, methods and duration of interventions, there were consistent positive increases in physical activity levels for all outcomes measured during PE classes, endurance and active transportation to school in all three randomized studies. Except for one cohort from one study, the non-randomized studies showed positive intervention effects for moderate and vigorous physical activity levels during PE classes. The core elements of these five interventions included capacity building and staff training (PE specialists and/or classroom teachers); changes in the PE curricula; provision of equipment and materials; and adjustment of the interventions to specific target populations. In order to translate the strong evidence for school-based PE into practice, systematic attention to policy and implementation issues is required. (Global Health Promotion, 2010; 17(2): pp. 05–15)
Keywords: Latin America, physical activity, physical education, school-based intervention, systematic review, youth
Introduction
Regular physical activity (PA) reduces the risk of chronic disease, including some types of cancer, diabetes, obesity and cardiovascular disease (1). Despite this evidence, PA levels continue to be far from ideal in most parts of the world (2). Of special concern is the evidence indicating that children, particularly in the developed world, establish a sedentary lifestyle early in life (3). Some developing countries are experiencing similar patterns associated with lifestyle changes, such as sedentary habits and high caloric intake that contribute in part to the worldwide obesity epidemic (4). The Latin American region is experiencing increasing rates of obesity among youth (5–9). In developing countries, high prevalence of overweight and obesity lead to early mortality in adulthood (10).
Children today have fewer opportunities to be active in a safe and independent manner, especially in large cities in developing countries that are rapidly urbanizing (11). According to a birth cohort study conducted in Pelotas, Brazil, the prevalence of sedentary lifestyles, characterized by excessive TV viewing and lack of PA, among youth is as high as 58% (12). Factors that decrease energy expenditure, such as the declining time for physical education (PE) in schools, may play an important role in the prevalence of overweight among children. Because students spend large amounts of time in school, there is a great potential for increasing their level of PA through school-based interventions (13,14). In a systematic review of 14 evidence-based PA promotion strategies, the US Guide to Community Preventive Services (Community Guide) found strong supporting evidence that school-based PE programs increased PA among school children (15). The school-based PE interventions included modified PE classes, generally with more classroom time and more moderate-to-vigorous PA (16).
The recommendations of the Community Guide and its process of systematic review have not yet been systematically examined and applied in developing countries. Many promising PA interventions are being carried out in Latin America (17); however, their effectiveness has generally not been evaluated. The Guide for Useful Interventions for Activity in Latin America (GUIA) was initiated in 2005 to examine and promote evidence-based strategies, with the intention of increasing PA in Latin America (18). The purpose of the initial phase of GUIA was to conduct a review of the Latin American literature on community-based PA promotion strategies and to determine the applicability of the Community Guide recommendations in this region. According to Community Guide criteria, school-based PE was found to be the only type of PA intervention with a strong enough body of evidence to make a practice recommendation (18). This article focuses on the results of the GUIA systematic review related to school-based PE programs in Latin America. The aims of the article are to (i) describe selected school-based PE interventions from the GUIA review; (ii) discuss implications of effective school-based PE recommendations in the Latin America region; (iii) propose approaches for implementing these interventions in Latin America; (iv) identify gaps in the research literature related to PA promotion in Latin American youth.
Methods
Although this article focuses specifically on the school-based PE findings of the GUIA literature review, the method used to search, categorize and abstract the papers for the present study were the same used in the overall review. Therefore, in order to understand the process of reviewing and evaluating the Latin America literature related to PA interventions, it is necessary to review the methods previously described (18). First, five databases of peer-reviewed literature and Brazilian theses were systematically searched for studies of PA community interventions by using search terms in Portuguese, Spanish and English. Intervention studies were then synthesized in one-page summary tables, categorized by the 14 Community Guide PA intervention categories (16) and screened for inclusion in a full abstraction process. This process followed the Community Guide procedures (19), with some modifications (18). On the basis of previously described criteria (15), studies were evaluated by two measures: design suitability (classified as greatest, moderate and least [Appendix 1]) and quality of intervention execution (classified according to the number of limitations to assess the strength of the evidence [Appendix 2]).
Relative effect sizes for the school-based PE intervention studies were calculated as the net percentage change from baseline for all reported measures of aerobic capacity and physical activity levels and for all time periods. The formula for calculating the net effect (Figure 1) varied depending on the study design – with or without a control group or pre-intervention outcome measurement (16). To identify common characteristics of the school-based PE interventions, the authors reviewed each of the school-based PE articles and abstraction forms in detail, categorizing and listing intervention components. These ‘core components’ were determined according to frequency of use by most of the studies and also by taking into account the intervention activities recognized by the Community Guide (16).
Figure. 1.
Net percentage change in physical activity from baseline for the school-based physical education intervention studies

Source: Adapted from Kahn E, Ramsey L, Brownson R, et al. The Effectiveness of interventions to increase physical activity: a systematic review. Am J Prev Med. 2002; 22(4): 73–107.
Additionally, Brazilian experts provided input to address issues related to PE typically not available in the literature. These experts made available additional literature sources, such as peer-non-reviewed manuscripts and meeting reports, not included in the evidence-based review.
Results
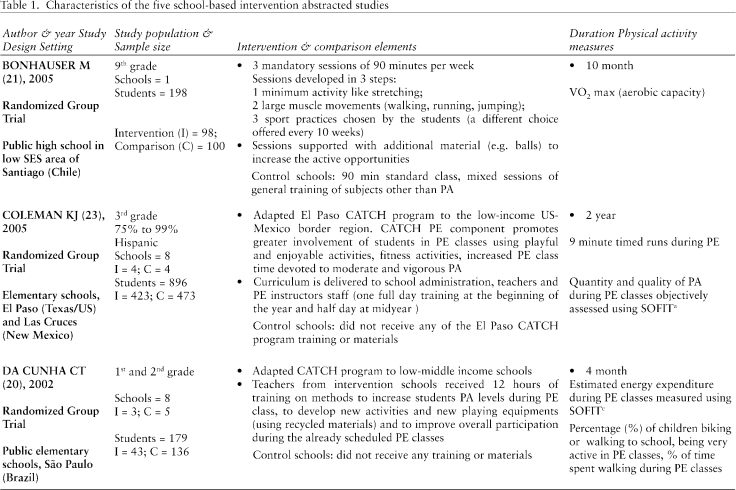
The systematic literature review yielded five school-based PE intervention studies (20–24), out of six that met all of the inclusion criteria (18). The excluded study was a duplicate of one included thesis (20), which contained more details about the intervention and evaluation for the abstraction process than the peer-reviewed article. All five studies had sufficient quality of design, execution and detail regarding the intervention and outcomes to undergo the second phase of the abstraction process. Three studies used randomized group design (20,21,23) and two used a non-randomized group design with a concurrent comparison group (Table 1) (22,24). One study was conducted in elementary public schools in Brazil (children aged 7–10 years) (20), two were carried out in public schools in Chile (first- through ninth-grade classes) (21,22) and the remaining two took place in US elementary schools mainly attended by Latino students and located on the US/Mexico border (23,24).
Table 1.
Characteristics of the five school-based intervention abstracted studies
 |
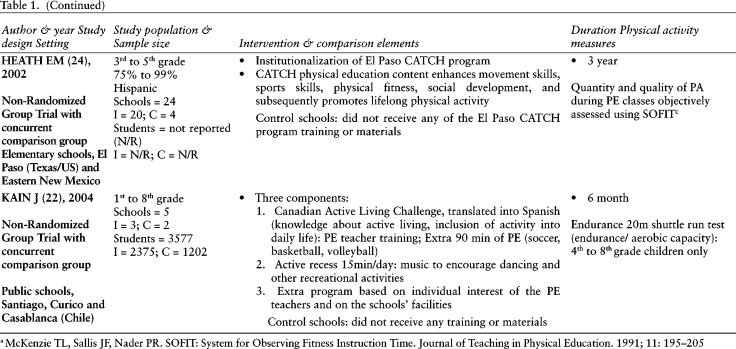 |
Two studies (23,24) reported minutes spent in moderate and vigorous PA, and one study (20) reported four different outcomes related to behavior: percentage of children biking or walking to school, estimated energy expenditure based on observed PA behavior of children, percentage of children who were very active during PE classes and percentage of time spent walking during PE classes. Further reported outcomes were aerobic capacity as estimated by maximal oxygen uptake (VO2 max) (21), results from timed runs (23) or endurance testing (shuttle runs) (22).
Although the outcomes, ascertainment methods, and duration of interventions varied between studies, there were consistent positive increases in PA levels for all outcomes measured during PE classes (relative net effects ranged from 7% to 307%) in all three randomized studies (20,21,23) (Figure 1). The extreme magnitude of the 307% net effect is explained by the low baseline walking levels in the intervention group versus the control group (5.6 vs. 14.4%, respectively). At post-test the intervention group increased time spent walking during PE classes nearly 5–6 times that of baseline, while the control group increased walking time by only 1.5 times baseline. Likewise, endurance (23) and active transportation to school (20) outcomes showed small but positive net effects for the same group of studies. With the exception of one cohort in Heath (24), the non-randomized studies increased moderate and vigorous PA levels during PE classes. These increases ranged from 5% to 69% for moderate and 50% to 55% for vigorous PA levels during PE classes. The results from the shuttle run test (22) demonstrated increased endurance performances among boys (35%) and girls (37%).
After reviewing the details of each study (Table 1), four types of intervention activities were identified and summarized as the ‘core components’ presented in Table 2. Core components included the provision of information about the benefits and importance of health and active living (20,22); types of PA suitable for a particular age range (20); overall PE class planning (lesson plan development, class and environment management) and methods of PA practice (23,24); increases in the duration of the already scheduled PE classes (23,24); addition of extra PE classes per week (21,22); use of age-specific and enjoyable activities (20–24) (such as balance exercises, dancing, jumping, and running); availability of new materials for classes (balls, basketball boards) (20–22); and adaptable, flexible and culturally sensitive activities based on ethnicity or socioeconomic status (20,22–24).
Table 2.
Core components summarized from the five intervention studies.
| Intervention Strategy | ||||
|---|---|---|---|---|
| Study | Capacity building and staff training – PE specialists and/or classroom teachers | Changes in the PE curricula | Provision of equipment and materials | Adjustment of the interventions to specific target populations |
| Bonhauser M21, 2005 | X | X | ||
| Coleman KJ23, 2005 | X | X | X | |
| Da Cunha CT20, 2002 | X | X | X | X |
| Heath EM24, 2002 | X | X | X | |
| Kain J22, 2004 | X | X | X | X |
Discussion
Our results identified several common characteristics, the core components (Table 2), of successful school-based PE interventions in Latin America that were comparable to some of those used in the Community Guide. These included the addition of supplementary PE classes, the lengthening of existing PE classes, and an increase in time spent in moderate and vigorous PA without necessarily changing duration of PE classes (16). Four (20,22–24) out of the five studies reviewed in the current study were adaptations of North American school-based interventions and therefore delivered analogous activities to the 13 studies reviewed by the Community Guide, both in terms of content and quality. With appropriate adjustments for national, local, and cultural contexts, the identified core components from interventions from two schools in Chile, a Brazilian elementary school and two elementary schools on the US/Mexican border could be a logical approach to guide PE recommendations and implementation across diverse countries, cultures and populations such as those found in Latin America.
High-quality school-based PE programs, combining all or some of the core components described here, increase PA among children in Latin America in the same way as they do in the USA (18). Similar to the GUIA literature review (18), the 13 US qualifying studies revealed consistent increases in time spent in PA at school (16), The net increase in the amount of PE class time spent in moderate and vigorous PA was 50%, ranging from 6% to 125%. The percentage of class time increase in moderate and vigorous PA was 10%, ranging from 3% to 15%, although one study reported a 762% increase from a very small baseline value. Two studies showed increases in energy expenditure, and 11 studies reported increases in aerobic capacity with a median of 8% (interquartile range 3% to 19%) (16).
When comparing intervention effects for the same outcomes, the five studies from the present study are generally consistent with the US CG results, both in direction and effect size. Some of the US CG net effects also had a wide range, particularly for the amount and percentage of PE class time spent in moderate and vigorous PA. The three studies that reported increased levels of PA during PE class (20,23,24) used the same observational method (16) to measure the amount of PE class time spent in moderate and vigorous PAi, but for different outcomes, such as the time spent being very active and the amount of walking during PE classes (20). The wide range in net effect sizes reflects differences in the degree of change in the outcome measures for intervention and comparison (if applicable) groups before and after the intervention. They also reflect the magnitude of the pre-intervention measures (see Figure 1 note).
Insufficient evidence supported recommending classroom-based health education to increase PA, mainly because of an insufficient number of qualified studies (n = 3) (18). These interventions consist of multicomponent health education classes in elementary, middle, or high schools that aim to help students to develop the skills they need to make rational decisions about adopting healthier behaviors (16).
Among the three reviewed studies, the net effects for various outcomes (e.g. frequency of exercise-related behaviors, any moderate and vigorous PA in the previous week) ranged from 0.0 to 0.2; net effects for 11 of the 14 outcomes were between 0 and 0.1. These net effects tended to be much lower in magnitude than those observed for the school-based PE interventions, which suggests that merely providing health information and promoting behavioral skills for healthy decision-making may be insufficient to significantly change PA behavior. However, more research of classroom-based health education, both in the USA (16) and in Latin America, is needed to confirm this finding.
The impact of an intervention is determined not only by its reach and efficacy but also by the extent to which the intervention is adopted, implemented as intended and maintained at the system and individual level (25). An effective intervention needs to have broad reach and be feasible to implement in ‘real-world’ settings in order to make a public health impact (25). Some of the major challenges for interventions are finding creative and cost-effective ways to implement evidence-based programs and policies at the population level, while providing adequate information and resources (e.g. infrastructure, training, proper economic and social environments) (26). This is particularly important in a region where legislation to promote school-based PE is highly variable. In addition, it is key to consider differences in terms of social influences that may affect children's and adolescents’ behavior (e.g. family, social networks, culture) when adapting programs that are effective in a specific setting or population (27). Although the purpose of school-based PE is larger than enhancing physical fitness only, it also has great potential for PA promotion because of its effectiveness in increasing PA among children (18) and because school programs reach virtually all children at relatively low cost with preexisting infrastructure.
In a context of increased academic and political credibility for PA promotion and PE during the past decade (28), supportive school PE policies appear to exist in many Latin American countries (29,30). In these countries, even though PE is mandatory for students in public and private elementary and secondary schools, the requirements concerning frequency and duration of classes is generally low (31). An optimal PE curriculum should include a variety of learning and practice experiences that will provide the basis for active living in the adult years (32). However, according to experts in the area, PE programs in Latin America are often of low quality and quantity. Therefore, a comprehensive school policy to increase PA practice during school-based PE and enhance its quality is required. In addition, frequency and duration of classes is often less than optimal because of challenges related to salary, work environment, physical space and curriculum structure (31); consequently, barriers to implementation exist primarily within the school systems and need to be addressed as well.
According to Melo (28), there is a call for academic institutions where PE teachers are trained to push for an adequate transition from what is learned in the academic world to what is needed in everyday practice in the schools. Often, the fields of academic knowledge production (e.g. universities/research institutes) and policy formulation/implementation are very different, frequently with incompatible goals and methods (33). Therefore, collaborative partnerships between researchers and practitioners, along with regulatory and legislative enforcement and political commitment and support for PE, are particularly desirable to help bridge the gap between theory and practice and for successful and sustainable program implementation.
Some limitations of this review should be considered. The five identified studies applied diverse ways to measure similar or same outcomes (e.g. moderate and vigorous PA levels during PE classes), which limited the ability of the previous review to derive a summary measure for the effect of school-based PE across the five reviewed studies. The net effect plot is an effort to be transparent in illustrating the variability in measures and lack of a gold standard in PA measurement in kids. By computing the net intervention effect, we were able to standardize and compare the effects. Although the literature search was conducted to identify interventions delivered in Latin America, we discuss findings from only five studies, two of which were implemented on the US/Mexican border (23,24). However, because these interventions took place in schools attended mainly by Hispanic children of low socioeconomic status, and since information on quality or availability of equipments and facilities was not available in the reviewed papers, we considered this population and setting comparable to those from other Latin American countries. The three remaining studies were limited to Chile (21,22) and Brazil (20). This limitation should be taken into account when disseminating school-based PE interventions in Latin America. Another consideration is the variability in the interventions’ duration (4 months to 3 years). The two longest studies (23,24) are funded adaptations of a broad, well-designed, tested and documented intervention studyii, which could justify in part the length of these two interventions. The three remaining studies (20–22) were much less supported and were single initiatives largely developed by academic institutions (University of Chile, Catholic University of Chile and Federal University of Sao Paulo) in collaboration with local health or education sectors. Nevertheless, the two longest interventions (23,24) did not result in larger net effect for similar outcomes when compared with the study with shortest duration (20).
Identifying interventions to increase PA levels in school settings is particularly important in Latin America because of the rapid demographic, epidemiologic and nutritional transitions associated with the increase in risk factors for chronic disease, including obesity and physical inactivity (4). These problems are unequally distributed across populations, and they disproportionately affect the most impoverished Latin Americans. Given the limited literature on evidence-based interventions for PA promotion in Latin American countries, developing recommendations to address physical inactivity among youth is essential.
The five studies in the GUIA review (18) and the 13 studies from the Community Guide review (16) were of sufficient quality to be included in the evidence-based review process and form the basis for the recommendation of school-based PE for PA promotion among children and adolescents in Latin America. Even though this may appear to be a small number of studies upon which to base global public health policy, relatively few other public health intervention recommendations are supported by systematic reviews of the scientific literature (27). Further implementation of school-based PE interventions could greatly benefit from systematic evaluation and publication of peer-reviewed studies on schools’ PE efforts to promote PA.
Conclusions
Given the importance of promoting PA in youth to improve the health of Latin Americans, our results provide the impetus to implement high-quality school-based PE interventions in this region. Enhancing the quality of PE in the schools and increasing the level of PA among youth depends on capacity building and training for PE teachers and instructors, appropriate changes in the PE curricula, proper infrastructure including equipment and materials, and adjustments to various political, cultural and socioeconomic characteristics. Additionally, future research is needed to identify other practical key elements, such as legislation, policy, barriers and facilitators for promoting school-based PE in Latin America.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgement
This study was funded through the Centers for Disease Control and Prevention contract U48/DP00 0060–01 (Prevention Research Centers Program).
Appendices
Appendix 1.
Suitability of study design for assessing effectiveness in the Community Guide, adapted from Briss et ala.
| Suitability | Examples | Attributes |
|---|---|---|
| Greatest | Randomized group or individual trial; prospective cohort study; time series study with comparison group | Concurrent comparison groups and prospective measurement of exposure and outcome |
| Moderate | Case-control study; time series study without comparison group | All retrospective designs or multiple pre- or post-measurements but no concurrent comparison group |
| Least | Cross-sectional study; case series; ecological study | Before-after studies with no comparison group or exposure and outcome measured in a single group at the same point in time |
Briss PA et. al. Developing an evidence-based Guide to Community Preventive Services – methods. The Task Force on Community Preventive Services. Am J Prev Med. 2000; 18(1 suppl): 35–43.
Appendix 2.
Assessing the strength of a body of evidence on effectiveness of population-based interventions in the Community Guide, adapted from Briss et ala.
| Evidence of effectivenessb | Quality executionc | Design suitability | Number of studies | Consistentd | Effect sizee |
|---|---|---|---|---|---|
| Strong | Good | Greatest | At least 2 | Yes | Sufficient |
| Good | Greatest or moderate | At least 5 | Yes | Sufficient | |
| Good or fair | Greatest | At least 5 | Yes | Sufficient | |
| Meets execution, suitability, number and consistency criteria for sufficient but not strong evidence | Large | ||||
| Sufficient | Good | Greatest | 1 | Not applicable | Sufficient |
| Good or fair | Greatest or moderate | At least 3 | Yes | Sufficient | |
| Good or fair | Greatest, moderate, or least | At least 5 | Yes | Sufficient | |
| Insufficientf | A. Insufficient design or execution | B. Too few studies | C. Inconsistent | D. Small |
Briss PA et. al. Developing an evidence-based Guide to Community Preventive Services – methods. The Task Force on Community Preventive Services. Am J Prev Med. 2000; 18(1 suppl): 35–43.
The categories are not mutually exclusive; a body of evidence meeting criteria for more than one of these should be categorized in the highest possible category.
Studies with limited execution are not used to assess effectiveness.
Generally consistent in direction and size.
Sufficient and large effect sizes are defined on a case-by-case basis and are based on the GUIA advisory team opinion.
These categories are not mutually exclusive and one or more of these will occur when a body of evidence fails to meet the criteria for strong or sufficient evidence.
Notes
McKenzie TL, Sallis JF, Nader PR. SOFIT: System for Observing Fitness. Instruction Time. Journal of Teaching in Physical Education. 1991; 11: 195–205.
Perry CL et al. The Child and Adolescent Trial for Cardiovascular Health (CATCH): Intervention, Implementation, and Feasibility for Elementary Schools in the United States. Health Educ Behav. 1997; 24(6): 716–35.
References
- 1.US Department of Health and Human Services Physical activity and health: a report of the Surgeon General Atlanta, GA, US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Pro-motion; 1996.
- 2.World Health Organization Obesity: preventing and managing the global epidemic World Health Organization; WHO Technical Report Series No. 894. Geneva; 1998 [PubMed] [Google Scholar]
- 3.Gordon-Larsen P, Nelson MC, Popkin BM. Longitudinal physical activity and sedentary behavior trends: adolescence to adulthood. Am J Prev Med. 2004; 27: 277–83 [DOI] [PubMed] [Google Scholar]
- 4.Raymond SU, Leeder S, Greenberg HM. Obesity and cardiovascular disease in developing countries: a growing problem and an economic threat. Curr Opin Clin Nutr Metab Care 2006; 9: 111–16 IUHPE - Global Health Promotion Vol.17, No. 2 2010 [DOI] [PubMed] [Google Scholar]
- 5.Veiga GV, Cunha AS, Sichieri R. Trends in overweight among adolescents living in the poorest and richest regions of Brazil. Am J Public Health 2004; 94: 1544–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.IBGE Pesquisa de orçamentos familiares 2002-2003. Tendência secular do estado nutricional. Gráfico 28 Indicadores antropométricos para adolescentes entre 10 e 19 anos de idade por sexo. Rio de Janeiro: Ministério da Saúde/IBGE/Ministério do planejamento, Orçamento e Gestão; 2006.
- 7.Hernández B. et al. Factores asociados con sobrepeso y obesidad en niños mexicanos de edad escolar: Resultados de la Encuesta Nacional de Nutrición 1999. Salud Publica Mex 2003; 45: s551–S55714746049 [Google Scholar]
- 8.Gomez et al. Television viewing and its association with overweight in Colombian children: results from the 2005 National Nutrition Survey: a cross sectional study. Int J Behav Nutr Phys Act 2007; 4: 41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kain J, Uauy R, Vio F, Albala C. Trends in overweight and obesity prevalence in Chilean children: comparison of three definitions. Eur J Clin Nutr 2002; 56: 200–4 [DOI] [PubMed] [Google Scholar]
- 10.World Bank Enfrentando o desafio das doenças não transmissíveis no Brasil 15 de Novembro de 2005. Relatório No. 32576-BR.
- 11.Popkin BM, Gordon-Larsen P. The nutrition transition: worldwide obesity dynamics and their determinants. Int J Obes 2004; 28: S2–S9 [DOI] [PubMed] [Google Scholar]
- 12.Hallal PC, Wells JCK, Reichert FF, Anselmi L, Victora C. Early determinants of physical activity in adolescence: prospective birth cohort study BMJ; 10.1136/bmj.38776.434560.7C [DOI] [PMC free article] [PubMed]
- 13.Mendlein J, Baranowski T, Pratt M. Physical activity and nutrition in children and youth: opportunities for performing assessments and conducting interventions. Prev Med 2000; 31: S150–3 [Google Scholar]
- 14.Pate RR, Davis MG, Robinson TN, Stone EJ, McKenzie TL, Young JC. Promoting physical activity in children and youth: a leadership role for schools: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism (Physical Activity Committee) in collaboration with the Councils on Cardiovascular Disease in the Young and Cardiovascular Nursing Circulation 2006; 114(11): 1214–24 [DOI] [PubMed] [Google Scholar]
- 15.Briss PA. et al. Developing an evidence-based Guide to Community Preventive Services-methods. The Task Force on Community Preventive Services. Am J Prev Med 2000; 18 (1 Suppl): 35–43 [DOI] [PubMed] [Google Scholar]
- 16.Kahn E. et al. The effectiveness of interventions to increase physical activity: a systematic review. Am J Prev Med 2002; 22(4): 73–107 [DOI] [PubMed] [Google Scholar]
- 17.CELAFISCS, Centers for Disease Control and Prevention. Best practices for physical activity promotion around the world 2006.
- 18.Hoehner CM. et al. Physical activity interventions in Latin America: a systematic review. Am J Prev Med 2008; 34(3): 224–33 [DOI] [PubMed] [Google Scholar]
- 19.Zaza S. et al. Data collection instrument and procedure for systematic reviews in the Guide to Community Preventive Services. Task Force on Community Preventive Services. Am J Prev Med 2000; 18(1 Suppl): 44–74 [DOI] [PubMed] [Google Scholar]
- 20.Da Cunha CT. Impacto de Programa Educativo no Gasto Energético de Escolares nas aulas de Educação Física: Ensaio randomizado controlado São Paulo, Master Thesis. Universidade Federal de São Paulo; 2002
- 21.Bonhauser M. et al. Improving physical fitness and emotional well-being in adolescents of low socioeco-nomic status in Chile: results of a school-based controlled trial. Health Promot Int 2005; 20(2): 113–22 [DOI] [PubMed] [Google Scholar]
- 22.Kain J, Uauy R, Albala, Vio F, Cerda R, Leyton B. School-based obesity prevention in Chilean primary school children: methodology and evaluation of a controlled study. Int J Obes Relat Metab Disord 2004; 28(4): 483–93 [DOI] [PubMed] [Google Scholar]
- 23.Coleman KJ. et al. Prevention of the epidemic increase in child risk of overweight in low-income schools: the El Paso coordinated approach to child health. Arch Pediatr Adolesc Med 2005; 159(3): 217–24 [DOI] [PubMed] [Google Scholar]
- 24.Heath EM, Coleman KJ. Evaluation of the institutionalization of the coordinated approach to child health (CATCH) in a US/Mexico border community. Health Educ Behav 2002; 29(4): 444–60 [DOI] [PubMed] [Google Scholar]
- 25.Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health 1999; 89: 1322–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rabin BA, Brownson RC, Kerner JF, Glasgow RE. Methodologic challenges in disseminating evidence-based interventions to promote physical activity. Am J Prev Med 2006; 31(4S): S24–S34 [DOI] [PubMed] [Google Scholar]
- 27.Anderson LM. et al. Evidence-based public health policy and practice: promises and limits. Am J Prev Med 2005; 28 (5 Suppl): 226–30 [DOI] [PubMed] [Google Scholar]
- 28.Melo JP. Perspectivas da educação física escolar: reflexão sobre a educação física como componente curricular. Revista Brasileira de Educ Fís Esp 2006; 20: 188–90 [Google Scholar]
- 29.Brasil Ministério da Educação e do Desporto Lei de diretrizes e bases da educação nacional, Lei n° 9.394 [Online] Available at: www.planalto.gov.br/CCIVIL_03/LEIS/L9394.htm
- 30.Ministerio de Educación de Colombia Política de desarrollo nacional de la educación física Ley 934 [Online]. Available at: http://www.mineducacion.gov.co/1621/article-85833.html
- 31.Darido SC. Professores de rducação física: procedimentos, avanços e dificuldades. Revista Brasileira de Ciências do Esporte 1997; 18: 192–206 [Google Scholar]
- 32.Pratt M, Jacoby ER, Neiman A. Promoting physical activity in the Americas. Food Nutr Bull 2004; 25(2): 183–92 [DOI] [PubMed] [Google Scholar]
- 33.Almeida C, Báscolo E. Use of research results in policy decision-making, formulation, and implementation: a review of the literature. Cad Saúde Pública 2006; 22: S7–S33 [DOI] [PubMed] [Google Scholar]