

Abstract
Sexual partner concurrency plays an important role in HIV and STD transmission. The shortage of African-American men may facilitate partner concurrency. This study evaluated whether the male-to-female ratio was associated with African-American participants' number of recent sexual partners, and whether this association differed by gender. Multilevel modeling was used to determine the influence of individual (i.e., gender) and population-level (i.e., sex ratio) variables on the number of recent sexual partners. African-American patients (N = 915; 52% male) were recruited from an STD clinic. Patients reported their number of sexual partners; the male-to-female ratio per census tract was obtained from the U.S. Census Bureau. There were fewer men than women in nearly all census tracts. The interaction between gender and the male-to-female ratio was significant. For men, there was no association between the sex ratio and their number of sexual partners. For women, as the sex ratio increased, their number of sexual partners increased; however, this association was driven by participants who reported trading sex. We found no evidence that fewer African-American men in a census tract was associated with men having more sexual partners.
Keywords: HIV/AIDS, sexually transmitted diseases, heterosexual transmission, multiple partners, concurrency
Introduction
African-Americans are disproportionately affected by STDs, including HIV. Rates of chlamydia and gonorrhea are much higher among African-Americans relative to other racial/ethnic groups (Centers for Disease Control and Prevention, 2006). Moreover, African-Americans accounted for 51% of newly diagnosed cases of HIV/AIDS from 2001 to 2004 (Centers for Disease Control and Prevention, 2007), and rates of HIV among African-American women are 21 times higher than among Caucasian women. The majority of these cases of HIV in African-American women were acquired through heterosexual contact (Centers for Disease Control and Prevention, 2007). Reducing the racial disparities in STDs requires improved understanding of the determinants of STD transmission.
One hypothesis for the disparities in HIV builds upon the smaller number of African-American men in low-income, urban communities. There, African-American women typically outnumber men because of higher rates of incarceration and premature death among African-American men. The relative shortage of men in such communities may reduce women's dyadic power1 in male-female relationships. In turn, women may feel compelled to be more tolerant of a male partner's concurrent partnerships. Although the potential impact of the shortage of men on sexual behavior is often noted (Lane et al., 2004; Logan et al., 2002; Mays and Cochran, 1988; McNair and Prather, 2004), supporting evidence is scarce.
Evolutionary theorists posit that men are predisposed genetically to prefer multiple partners, whereas women are predisposed to invest in a single partner (Buss and Schmitt, 1993). Social role theorists agree with these gender-based dispositions, but attribute these to socialization processes rather than genetics (Eagly, 1987). Researchers have found that when the male-to-female ratio is low, marriage rates are low for both men and women (Albrecht and Albrecht, 2001; Albrecht et al., 1997; Fossett and Kiecolt, 1993; Guttentag and Secord, 1983). It is hypothesized that, when the sex ratio is low, women are less likely to marry because there are fewer men, whereas men are less likely to marry because they value women less when there are many available women (Guttentag and Secord, 1983). Qualitative research has found that the lack of men leads to less power for women, and to concurrent sexual partnerships for men (Adimora et al., 2001; Ferguson et al., 2006). However, qualitative research employs small samples, and the representativeness of participants is difficult to discern (Krueger and Casey, 2000).
Quantitative investigations of the relation between the male-to-female ratio and sexual behavior have been scarce. Studies using population-level data have generally found that sex ratio and incarceration rates (a proxy for the number of available men) are associated with STD rates, although this relation is sometimes rendered nonsignificant when controlling for other variables (Kilmarx et al., 1997; Thomas and Gaffield, 2003; Thomas and Sampson, 2005). In one of the few studies to use both population-level and individual-level data, Smith and Subramanian (2006) found that the sex ratio in Australia was associated with the number of sexual partners in the previous year; however, they did not explore whether the male-to-female ratio had differential effects for men and women.
In this study, we investigate the relation between the male-to-female ratio, gender, and the number of recent sexual partners in a sample of patients attending an STD clinic. Our work advances previous research by using multilevel modeling to analyze individual-level as well as population-level data. Based on theory, we hypothesized that men would have more female sexual partners as the male-to-female ratio in a census tract decreased; for women, however, we did not predict an effect of the sex ratio on the number of male partners.
Methods
Participants
Patients attending a STD clinic in upstate New York were recruited as part of a randomized controlled trial (RCT; Carey et al., in press). Inclusion criteria for the RCT included: age 18 or older; and engaged in sexual risk behavior (past 3 months), which included having vaginal or anal intercourse with more than one partner, or having vaginal or anal intercourse with a partner who had multiple partners, who injected drugs, who had been diagnosed with an STD in the past 3 months, or who was HIV positive. Patients were excluded if they were unable to consent or to participate meaningfully in the study due to mental impairment, not willing to take an HIV test, already infected with HIV, or if they had been seen at the clinic in the prior three months (to ensure that patients had not recently received one of the interventions that was being evaluated in the RCT). For these analyses, we began with the 1003 African-American patients enrolled in the RCT. Patients were excluded if they (a) lived outside the county (n = 6); (b) provided a college, erroneous, or post office box address (n = 28); (c) did not provide complete data on the number of sexual partners (n = 1); (d) lived in census tracts that included inmates (n = 23; because inmates are unavailable as sexual partners); (e) lived in census tracts with fewer than 100 African-American adults (n = 17; because estimates of the percentage of African-American men in the census tract would not be reliable); or (f) reported only same-sex partners (n = 13). Thus, the sample size for this study was N = 915.
Procedures
Complete details for the RCT are available elsewhere. In brief, patients met with a Research Assistant (RA) in a private room, and were asked if they would be willing to answer a few brief questions. Those who agreed were screened for eligibility by the RA. The study was fully explained, and written consent was obtained. Contact information was also obtained from participants. Participants then completed a computerized survey, which included demographic and sexual behavior questions. Participants completed their clinic visit, and were randomized one of six intervention conditions in the RCT. They received $20 reimbursement for their time.
Measures
Participants were asked to report their sex, race, employment status, income, education, and marital status. In addition, participants were asked how many male and how many female sexual partners they had in their lifetime and in the past 3 months, how many episodes of unprotected sex (vaginal plus anal) they had in the past 3 months, and how many times in their lifetime they exchanged sex for money or drugs. All measures have been used extensively in previous research (Carey et al., 2000; Carey et al., 2004; Carey et al., 1997). The outcome measure used in the present study was the number of opposite-sex partners reported in the past 3 months. Because of the short time frame (i.e., past 3 months), this measure most likely reflects the number of concurrent sexual partnerships in which participants engaged; however, serially monogamous partnerships may also have been captured by this measure.
Participants' addresses were entered into the U.S. Census Bureau website to determine the census tract in which they lived. Data from the 2000 census were used to determine the number of African-American men and women (over age 18) in each census tract; to determine the ratio of African-American men to women (i.e., the sex ratio), the number of African-American men was divided by the number of African-American women in each census tract, and multiplied by 100. Thus, the sex ratio reflects the number of men for every 100 women.
Analyses
Extreme outliers on the sexual behavior variables (> 3 times the interquartile range from the 75th percentile) were trimmed. To account for the multilevel, or nested, structure of the data (i.e., people nested within census tracts), multilevel modeling was used for the main analyses (Raudenbush and Bryk, 2002; Snijders and Bosker, 1999). Gender was included as an individual-level (Level I) predictor, and the sex ratio in the census tract was included as a group-level (Level II) predictor. The criterion (i.e., number of opposite-sex partners, past 3 months) was non-normally distributed (Schroder et al., 2003); therefore, models were run with a Poisson distribution for the outcome variable. SAS (Proc Glimmix) was used to conduct the multi-level analyses.
In multilevel modeling, results consist of a fixed effect and variance-covariance parameter estimates. The fixed effect for gender (centered within group) indicates whether gender is related to the number of sexual partners within each census tract; the fixed effect for the sex ratio (centered at the grand mean) indicates whether the sex ratio in a census tract is related to the average number of partners for respondents from each tract; and the fixed effect for the interaction between gender and the sex ratio tells us whether the relation between the sex ratio and the number of partners differs for men and women. The covariance parameter estimates, or variance components, indicate whether there is variation among census tracts, which could be explained by adding predictors to the model. The covariance parameter for the intercept indicates whether there is variation among census tracts in the mean number of partners. The covariance parameter for gender centered within group indicates whether there is variation between census tracts in the relation between gender and the number of partners. Because the sex ratio does not vary among census tracts, there is no variance component associated with this variable. All fixed and covariance parameter estimates are conditional on the effects of the other predictors in the model.
Results
Individual-level data
The sample was 52% (n = 478) male (M age = 29.6 years, SD = 9.9). More than one-half of participants were unemployed (n = 532; 58%), made less than $15,000 per year (n = 572; 63%), and had a high school or less education (n = 656; 72%). Most participants (n = 859; 94%) were not married. Participants reported engaging in recent and lifetime risk behavior, with an average of 2.8 (SD = 2.3) opposite-sex sexual partners in the past 3 months, 34.3 (SD = 36.4) lifetime sexual partners, and 17.5 (SD = 21.3) episodes of unprotected sex in the past 3 months (data reported from variables with outliers trimmed). Men reported more sexual partners in the past 3 months than did women (Ms = 3.2 vs. 2.5, respectively), F(1, 914) = 20.43, p < .0001. The majority of participants reported more than one sexual partner in the past 3 months (n = 645; 70%). Men (82%) were more likely than women (58%) to report multiple sexual partners in the past 3 months, χ2(1, N = 915) = 61.52, p < .0001. One-quarter of the sample (n = 227) reported that they had exchanged sex for money or drugs, with women (36%) more likely to report exchanging sex than men (16%), χ2(1, N = 899) = 46.67, p < .0001. Those who reported ever exchanging sex for money or drugs reported more partners in the past 3 months than did those who did not exchange sex (Ms = 3.5 vs. 2.6, respectively), F(1, 898) = 26.63, p < .0001.
Census-tract level data
Participants came from 93 census tracts. There was an average of 9.8 (SD = 8.2) participants from each of the 93 census tracts (range = 1 to 38). The average sex ratio in the census tracts was 78.6 (SD = 14.1; range = 39.4 to 130.7). The sex ratio was less than 100 in the majority of census tracts (n = 87; 94%). The census tracts were characterized by high levels of unemployment and poverty. Among all African-Americans living in these census tracts, 65% had a high school education or less, 8% were unemployed, and 32% had an income at or below the poverty level (United States Census Bureau).
Multilevel models
In all models, the outcome was the number of opposite-sex sexual partners in the past 3 months. In Model 1, no predictors were included (i.e., an unconditional means model; see Table I). In this model, the covariance parameter estimate for the intercept was significant, (estimate = 0.014) Z = 1.75, p < .05 (1-tailed test), indicating that there was significant variation among census tracts in the number of sexual partners that could be explained by adding predictors to the model.
Table I.
Multilevel models predicting number of sexual partners in the past 3 months using gender and census tract male-to-female ratio
| Model 1 no predictors (unconditional means model) |
Model 2 Level 2 predictor (Sex ratio in census tract) |
Model 3 Level 1 predictor (Gender) |
Model 4 Level 1 and Level 2 predictors (Gender, Sex ratio in census tract, and Sex ratio-by-Gender interaction) |
|||||
|---|---|---|---|---|---|---|---|---|
| Estimate | SE | Estimate | SE | Estimate | SE | Estimate | SE | |
| Fixed Effects | ||||||||
| Intercept | 1.04*** | 0.02 | 1.09*** | 0.04 | 1.04*** | 0.02 | 1.09*** | 0.04 |
| Sex ratio (grand mean centered) | 0.002 | 0.002 | 0.003 | 0.002 | ||||
| Gender (group mean centered) | 0.22*** | 0.06 | 0.04 | 0.10 | ||||
| Sex ratio-by-Gender (group mean centered) interaction | −0.010* | 0.005 | ||||||
| Variance Components | ||||||||
| Intercept | 0.014* | 0.008 | 0.014* | 0.008 | 0.014* | 0.008 | 0.013* | 0.008 |
| Gender (group mean centered) | 0.073** | 0.033 | 0.065** | 0.031 | ||||
| Goodness-of-fit | ||||||||
| −2 Residual Log Pseudo-Likelihood | 2328.16 | 2337.99 | 2279.22 | 2294.32 | ||||
SE = Standard error.
p < .05,
p < .01,
p < .001
In Model 2, the Level 2 predictor, sex ratio in the census tract (grand mean centered), was included. This variable was not significant (estimate = 0.002), indicating that the sex ratio was unrelated to the number of sexual partners. There was still significant variation in the number of sexual partners among census tracts (estimate = 0.014), Z = 1.73, p < .05.
In Model 3, the Level 1 predictor, gender (centered within group), was included. This predictor was significant (estimate = 0.22), indicating that there was a relation between gender and the number of sexual partners, within each census tract (p < .001). Men had significantly more sexual partners in the past 3 months than did women, within each census tract. After including gender, the variability in the number of sexual partners among census tracts remained significant (estimate = 0.014), Z = 1.73, p < .05. There was also significant variability between census tracts in the relation between gender and the number of sexual partners (estimate = 0.073), Z = 2.24, p < .01, indicating that the gender differences in the number of sexual partners varied from tract to tract.
In Model 4, both the Level 1 and Level 2 predictors were included; thus, this model included gender, the sex ratio in each census tract, and the interaction between gender and the sex ratio, as predictors of the number of recent sexual partners. In this model, there was a significant gender-by-sex ratio interaction (estimate = −.01, p < .05). An increase in the sex ratio in the census tract was associated with a slight decrease in the number of sexual partners for men, but this decrease was not significant. An increase in the sex ratio was associated with an increase in the number of sexual partners for women. (Because data were over-dispersed, models were rerun using a negative binomial distribution, with similar results.) After including the two predictors and their interaction, the variability among census tracts remained significant (estimate = 0.013, Z = 1.67, p < .05) as did the variability among census tracts in the relation between gender and the number of sexual partners (estimate = 0.065), Z = 2.09, p < .01.
Because women were more likely to report trading sex for money or drugs, which could influence (strongly) the number of sexual partners reported, a supplemental analysis including a three-way interaction between gender, sex ratio, and sex trading was conducted. In this model, sex trading was significant (estimate = −0.31, p < .01), but gender, the sex ratio, and the interaction between gender and the sex ratio were not significant (all p's > .10). The covariance parameter for the intercept was 0, indicating that the inclusion of sex trading (and sex trading interactions) explained all the variability in the number of sexual partners between census tracts.
The three-way interaction of gender, the sex ratio, and sex trading was not significant (p > .10), indicating that the relation between the gender-by-sex ratio interaction and the number of partners did not differ for participants who did and did not trade sex. Additionally, the interaction between gender and the sex ratio was not significant for participants who did not trade sex (estimate = −.005, p > .10), or for participants who did trade sex (estimate = −.011, p > .10). However, despite the lack of a significant three-way interaction, and the lack of a significant gender by sex ratio interaction for participants who reported trading sex, the gender by sex ratio interaction was larger for participants who traded sex than for participants who did not trade sex; this interaction was very close to zero for individuals who did not trade sex. Thus, it is likely that women who traded sex largely drove the gender-by-sex ratio interaction in the initial analyses, and the nonsignificant three-way interaction and nonsignificant interaction between gender and the sex ratio for individuals who traded sex is due to a lack of power. The graph in Figure 1, which depicts the predicted number of sexual partners for men and women who do and do not engage in sex trading for census tracts of differing sex ratios, shows that the strongest association between the sex ratio and the number of sexual partners is for women who reported trading sex.
Figure 1.
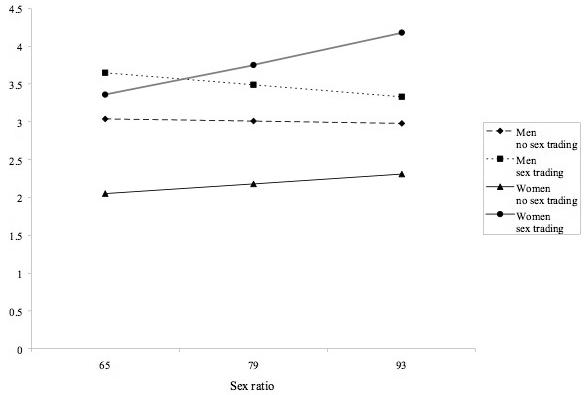
Predicted number of partners for men and women who do and do not trade sex, as a function of the sex ratio
Discussion
The low ratio of men to women among African-Americans has been hypothesized to increase sexual risk behavior, by leading to multiple sexual partners for men (Lane et al., 2004; Logan et al., 2002; Mays and Cochran, 1988; McNair and Prather, 2004); this partner concurrency is hypothesized to increase risk for female partners who tolerate “man-sharing” (Ferguson et al., 2006) rather than forgo the benefits of an intimate relationship with a male partner. This is one of the first studies to investigate the relation between percentage of men and number of recent sexual partners, quantitatively, in a large urban sample using multilevel modeling.
We found that there was a shortage of African-American men relative to women in most census tracts and, consistent with prior research, men reported more sexual partners than did women (Cubbins and Tanfer, 2000; Laumann et al., 1994). However, contrary to our hypotheses, we did not find that a lower sex ratio was associated with more sexual partners for men. The association between the sex ratio and number of sexual partners was in the hypothesized direction (i.e., a slight increase in number of sexual partners for men as the sex ratio decreased), but this association was nonsignificant. However, because the majority of census tracts had a shortage of African-American men (i.e., a restricted range), we can only conclude that in areas where there is a shortage of men, the sex ratio is unrelated to men's number of recent sexual partners. A stronger empirical test would have been possible if we had been able to include more census tracts with a surplus of men.
Also contrary to our hypotheses, there was an association between the sex ratio and the number of recent sexual partners for women; that is, as the sex ratio in a census tract increased, the number of sexual partners increased for women. However, this association seems to have been driven by women who exchanged sex; that is, as there were more men in a census tract, there were more potential clients for these women. Alternatively, as there were more women in a census tract (i.e., a low male-to-female ratio), women who traded sex may have had more difficulty attracting male clients, because there were more available sexual partners for men who did not require payment. Future research will need to investigate further the effects of sex trading on the relation between the sex ratio and the number of recent sexual partners.
The role of multiple partnerships in HIV transmission is recognized as important. Epstein (2007) provides a compelling epidemiologic case for the critical role of partner concurrency in the HIV epidemic in sub-Saharan Africa. Mathematical models have shown that concurrent partnerships increase size of an HIV outbreak (Morris and Kretzschmar, 1995). In the U.S., research suggests that concurrent partnerships accelerate heterosexual HIV transmission among African-Americans (Adimora and Schoenbach, 2005). It is known that multiple partnerships are more likely among young, unmarried men, and that there appears to be an escalating pattern of multiple partnerships in the U. S. beginning in the 1960s (Laumann et al., 1994). Research might examine the socioeconomic context that supports such patterns of sexual behavior.
A significant strength of this investigation was the large number of both Level 1 (participants) and Level 2 (census tracts) units. These sample characteristics allowed us to use multilevel modeling to estimate nested effects, and to investigate the interaction between individual- and population-level variables. Additional strengths of this study include its guidance by both theory and formative research.
We also wish to acknowledge limitations of the study. First, patients attending an STD clinic are not representative of the general population; thus, these results may not generalize to other population sub-groups. In addition, these participants met inclusion criteria for and agreed to participate in a larger RCT; thus, the sample may not be representative of all patients attending an STD clinic. Second, census tract was used as a group-level variable; however, census tracts may not reflect perfectly the social network from which participants choose their partners. Research indicates that people live in close proximity to their sexual partners (Massey and Denton, 1993; Zenilman et al., 1999), but the choice of partners may extend beyond census tract boundaries. Third, nearly all census tracts (94%) had more women than men, creating a restricted range of values on this variable; however, there are few cities in the U.S. where there are more African-American men than women. Finally, although the measure used in the study (number of sexual partners in the past 3 months) likely captured concurrent sexual partnerships, it is possible that participants had multiple non-overlapping partnerships during that time frame. Detailed data on the beginning and ending dates of sexual partnerships were not available.
Multilevel modeling is an important statistical tool to understand health and behavior because it allows the inclusion of both individual-level and group-level correlates in a single analysis (Diez-Roux, 1998; Duncan et al., 1996; Jones and Duncan, 1995). Previous analyses found an association between the male-to-female ratio and STD rates, but were unable to investigate the influence of gender (Kilmarx et al., 1997; Thomas and Gaffield, 2003; Thomas and Sampson, 2005). By utilizing multilevel analysis, we estimated both individual- and population-level effects, and explored the interaction between the individual- and population-level variables. Research on the dynamics of sexual partnerships, and the implications of these partnerships for disease transmission, can enhance understanding of the social and structural determinants of disease; this information can be used to address the disparities now evidenced in the epidemiology of all STDs.
Acknowledgments
This research was supported by NIH grant # R01-MH068171 to Michael P. Carey.
Footnotes
Guttentag and Secord (1983) describe two types of relationship power. Structural power results from greater political and economic resources whereas dyadic power accrues to members of the scarcer sex. Traditional gender roles typically afford men greater structural power relative to women (Theory of Gender and Power; Connell, 1987). Greater mortality among young adult males affords men greater dyadic power. Based on these considerations, it is hypothesized that African-American men possess greater structural and dyadic power relative to African-American women.
References
- Adimora AA, Schoenbach VJ. Social context, sexual networks, and racial disparities in rates of sexually transmitted infections. Journal of Infectious Diseases. 2005;191:S115–S122. doi: 10.1086/425280. [DOI] [PubMed] [Google Scholar]
- Adimora AA, Schoenbach VJ, Martinson FE, Donaldson KH, Fullilove RE, Aral SO. Social context of sexual relationships among rural African Americans. Sexually Transmitted Diseases. 2001;28:69–76. doi: 10.1097/00007435-200102000-00002. [DOI] [PubMed] [Google Scholar]
- Albrecht CM, Albrecht DE. Sex ratio and family structure in the nonmetropolitan United States. Sociological Inquiry. 2001;71:67–84. [Google Scholar]
- Albrecht CM, Fossett MA, Cready CM, Kiecolt KJ. Mate availability, women's marriage prevalence, and husbands' education. Journal of Family Issues. 1997;18:429–452. doi: 10.1177/019251397018004004. [DOI] [PubMed] [Google Scholar]
- Buss DM, Schmitt DP. Sexual strategies theory: An evolutionary perspective on human mating. Psychological Review. 1993;100:204–232. doi: 10.1037/0033-295x.100.2.204. [DOI] [PubMed] [Google Scholar]
- Carey MP, Braaten LS, Maisto SA, Gleason JR, Forsyth AD, Durant LE. Using information, motivational enhancement, and skills training to reduce the risk of HIV infection for low-income urban women: A second randomized clinical trial. Health Psychology. 2000;19:3–11. doi: 10.1037//0278-6133.19.1.3. [DOI] [PubMed] [Google Scholar]
- Carey MP, Carey KB, Maisto SA, Gordon CM, Schroder KE, Vanable PA. Reducing HIV-risk behavior among adults receiving outpatient psychiatric treatment: Results from a randomized controlled trial. Journal of Consulting and Clinical Psychology. 2004;72:252–268. doi: 10.1037/0022-006X.72.2.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey MP, Maisto SA, Kalichman SC, Forsyth AD, Wright EM, Johnson BT. Enhancing motivation to reduce the risk of HIV infection for economically disadvantaged urban women. Journal of Consulting and Clinical Psychology. 1997;65:531–541. doi: 10.1037//0022-006x.65.4.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey MP, Vanable PA, Senn TE, Coury-Doniger P, Urban M. Evaluating a two-step approach to sexual risk reduction in a publicly-funded STI clinic: Rationale, design, and baseline data from the Health Improvement Project--Rochester (HIP-R) Contemporary Clinical Trials. doi: 10.1016/j.cct.2008.02.001. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention . Sexually transmitted diseases surveillance, 2005. US Department of Health and Human Services; Atlanta, GA: 2006. [Google Scholar]
- Centers for Disease Control and Prevention Racial/ethnic disparities in diagnoses of HIV/AIDS: 33 States, 2001--2005. Morbidity and Mortality Weekly Report. 2007;56:189–193. [PubMed] [Google Scholar]
- Connell RW. Gender and power: Society, the person, and sexual politics. Stanford University Press; Stanford, CA: 1987. [Google Scholar]
- Cubbins LA, Tanfer K. The influence of gender on sex: A study of men's and women's self-reported high-risk sex behavior. Archives of Sexual Behavior. 2000;29:229–257. doi: 10.1023/a:1001963413640. [DOI] [PubMed] [Google Scholar]
- Diez-Roux AV. Bringing context back into epidemiology: Variables and fallacies in multilevel analysis. American Journal of Public Health. 1998;88:216–222. doi: 10.2105/ajph.88.2.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan C, Jones K, Moon G. Health-related behaviour in context: A multilevel modelling approach. Social Science and Medicine. 1996;42:817–830. doi: 10.1016/0277-9536(95)00181-6. [DOI] [PubMed] [Google Scholar]
- Eagly A. Sex differences in social behavior: A social role interpretation. Earlbaum; Hillsdale, NJ: 1987. [Google Scholar]
- Epstein H. The invisible cure: Africa, the West, and the fight against AIDS. Farrar, Straus, & Giroux; New York: 2007. [Google Scholar]
- Ferguson YO, Quinn SC, Eng E, Sandelowski M. The gender ratio imbalance and its relationship to risk of HIV/AIDS among African American women at historically Black colleges and universities. AIDS Care. 2006;18:323–331. doi: 10.1080/09540120500162122. [DOI] [PubMed] [Google Scholar]
- Fossett MA, Kiecolt KJ. Mate availability and family structure among African Americans in US metropolitan areas. Journal of Marriage and the Family. 1993;55:288–302. [Google Scholar]
- Guttentag M, Secord PF. Too many women? The sex role question. Sage; Beverly Hills, CA: 1983. [Google Scholar]
- Jones K, Duncan C. Individuals and their ecologies: Analysing the geography of chronic illness within a multilevel modelling framework. Health and Place. 1995;1:27–40. [Google Scholar]
- Kilmarx PH, Zaidi AA, Thomas JC, Nakashima AK, St. Louis ME, Flock ML, Peterman TA. Sociodemographic factors and the variation in syphilis rates among US counties, 1984 through 1993: An ecological analysis. American Journal of Public Health. 1997;87:1937–1943. doi: 10.2105/ajph.87.12.1937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger RA, Casey MA. Focus groups: A practical guide for applied research. 3rd ed. Sage; Thousand Oaks, CA: 2000. [Google Scholar]
- Lane SD, Rubinstein RA, Keefe RH, Webster N, Cibula DA, Rosenthal A, Dowdell J. Structural violence and racial disparity in HIV transmission. Journal of Health Care for the Poor and Underserved. 2004;15:319–335. doi: 10.1353/hpu.2004.0043. [DOI] [PubMed] [Google Scholar]
- Laumann EO, Gagnon JH, Michael RT, Michaels S. The social organization of sexuality: Sexual practices in the United States. University of Chicago Press; Chicago: 1994. [Google Scholar]
- Logan T, Cole J, Leukefeld C. Women, sex, and HIV: Social and contextual factors, meta-analysis of published interventions, and implications for practice and research. Psychological Bulletin. 2002;128:851–885. doi: 10.1037/0033-2909.128.6.851. [DOI] [PubMed] [Google Scholar]
- Massey DS, Denton NA. American apartheid: Segregation and the making of the underclass. Harvard University Press; Cambridge, MA: 1993. [Google Scholar]
- Mays VM, Cochran SD. Issues in the perception of AIDS risk and risk reduction activities by Black and Hispanic/Latina women. American Psychologist. 1988;43:949–957. doi: 10.1037//0003-066x.43.11.949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNair LD, Prather CM. African American women and AIDS: Factors influencing risk and reaction to HIV disease. Journal of Black Psychology. 2004;30:106–123. [Google Scholar]
- Morris M, Kretzschmar M. Concurrent partnerships and transmission dynamics in networks. Social Networks. 1995;17:299–318. [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. 2nd ed. Sage; Thousand Oaks, CA: 2002. [Google Scholar]
- Schroder KEE, Carey MP, Vanable PA. Methodological challenges in research on sexual risk behavior: I. Item content, scaling, and data analytical options. Annals of Behavioral Medicine. 2003;26:76–103. doi: 10.1207/s15324796abm2602_02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith AMA, Subramanian SV. Population contextual associations with heterosexual partner numbers: A multilevel analysis. Sexually Transmitted Infections. 2006;82:250–254. doi: 10.1136/sti.2005.018549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snijders T, Bosker R. Multilevel analysis: An introduction to basic and advanced multilevel modeling. Sage; Thousand Oaks, CA: 1999. [Google Scholar]
- Thomas JC, Gaffield ME. Social structure, race, and gonorrhea rates in the southeastern United States. Ethnicity and Disease. 2003;13:362–368. [PubMed] [Google Scholar]
- Thomas JC, Sampson LA. High rates of incarceration as a social force associated with community rates of sexually transmitted infection. Journal of Infectious Diseases. 2005;191:S55–S60. doi: 10.1086/425278. [DOI] [PubMed] [Google Scholar]
- United States Census Bureau Census 2000 summary file 3. Retrieved October 19, 2007, from www.factfinder.census.gov.
- Zenilman JM, Ellish N, Fresia A, Glass G. The geography of sexual partnerships in Baltimore: Applications of core theory dynamics using a geographic information system. Sexually Transmitted Diseases. 1999;26:75–81. doi: 10.1097/00007435-199902000-00002. [DOI] [PubMed] [Google Scholar]