

Abstract
During the 20th century, infectious disease morbidity and mortality generally waned while chronic degenerative diseases posed a growing burden at the global level. The population on Saba, Netherlands Antilles, has recently experienced such an epidemiologic transition, and hypertension was reported to be extraordinarily high, although no prevalences have been reported and relationships with lifestyle factors associated with rapid modernization have not been explored. In this study, a medical and demographic questionnaire, as well as body composition and blood pressure measures were collected from 278 Saban men and women aged 18-91 years. When age and sex adjusted, 48% of the population was hypertensive. Age, BMI and Afro-Caribbean descent were all associated with higher blood pressures. In a second phase, 124 individuals of the 278 were invited to receive a longer questionnaire on individual exposure to modernizing influences such as travel and education. Higher blood pressure was associated with having lived in fewer different places in the past; those who stayed only on Saba or Statia had higher blood pressures than those who had also lived in more modernized areas. However, this was no longer statistically significant after adjustment for age and BMI. Lifestyle incongruity was positively associated with higher blood pressure in that those with more discord between material wealth and income were more likely to be hypertensive, and this remained statistically significant after adjustment for age and adiposity. In summary, hypertension is highly prevalent on Saba, and tended to be associated with greater age, adiposity, Afro-Caribbean ancestry and lifestyle incongruity.
Keywords: hypertension, Netherlands Antilles, Saba, modernization, genetic isolates
Introduction
Natural experimental models of disease are becoming increasingly useful to biomedical scientists (Garruto et al., 1999). By studying a population in a relatively homogeneous environment, such as island isolates, it is possible to eliminate some factors, and focus on others thought to contribute to a specific disease. Island models of modernization and chronic disease have been successfully developed for Samoa (Baker, 1986), Trinidad (Miller et al., 1996) and St. Lucia (Dressler, 1982) among others. These models may overcome problems of confounding, bias and heterogeneity created by large scale epidemiological research designs among large, highly diverse (genetically, environmentally and/or culturally) populations.
The island of Saba, Netherlands Antilles, is an example of a natural experimental model area, being of small size (5.2 square miles, 1200 residents) and unique population history (Figure 1 and Figure 2). Until the 1960's, Saba was relatively isolated due to lack of air service and little tourism or other sources of revenue. Following a population boom in the late 19th century, Saba subsequently experienced rapid depopulation, as men (predominantly) left the island for work (MacQueen, 1989). The surnames Hassell, Johnson and Every have been the most common surnames throughout most of the history of the island and, even today, are now used by over 30% of the current island residents (MacQueen, 1989; Soloway, 2005 unpublished observations). Because of the high prevalence of hypertension that has been reported on the island (Miller et al., 1992), as well as its relatively recent settlement in the 17th and 18th century by a small number of founders and long history of isolation, Saba provides a potentially useful setting for disentangling genetic and behavioral aspects of this important chronic disease.
Figure 1.
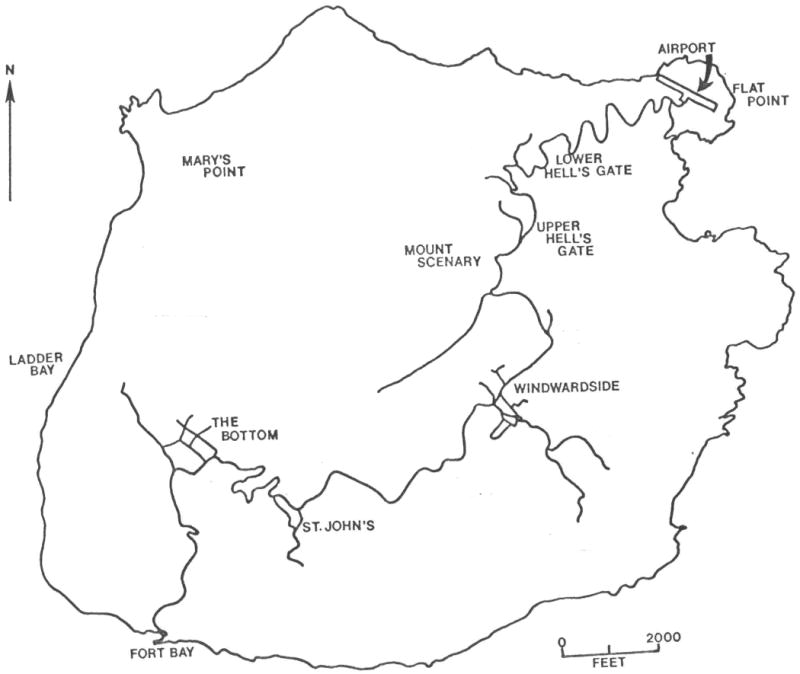
Map of Saba. Reprinted with permission from MacQueen 1989.
Figure 2.
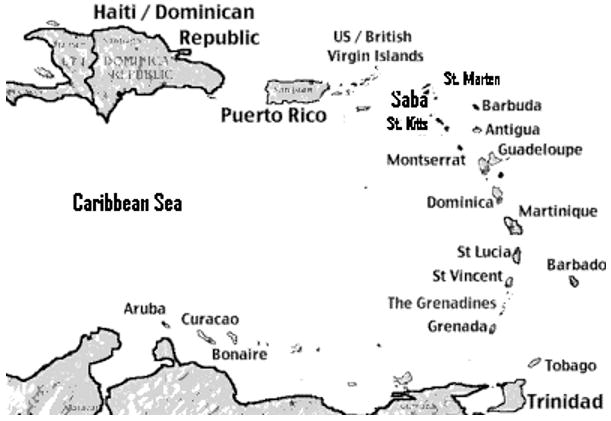
Map of The Caribbean with Saba position noted. From Crane, 1971.
Of particular importance in the epidemiology of hypertension, Saba has proceeded through a period of rapid economic modernization over the past 40-50 years. Populated initially by a small group of Arawak people, the first European settlement of the island occurred in 1632 by a small group of shipwrecked Englishmen (Figure 3) (Hartog, 1982). This was followed shortly by Dutch settlement in 1640. Unable to support a large population due to its thin soil and steep terrain, the island had at its peak only 2500 people. Travel between villages was precarious and travel to the island from other islands was limited. This, and the frequent out-migrations for work that occurred over the past 100 years (especially for men) may have resulted in population bottlenecks over the years. Our analysis of vital records covering over 9000 individuals born on Saba since 1880 indicate that more than 8000 of them belong to one, large, extended pedigree. Since the 1960's, a road, electricity and an airfield have been introduced on the island (Mol, 1989), and Saba today caters to a small ecotourism market seeking an “unspoiled” rugged island experience.
Figure 3.
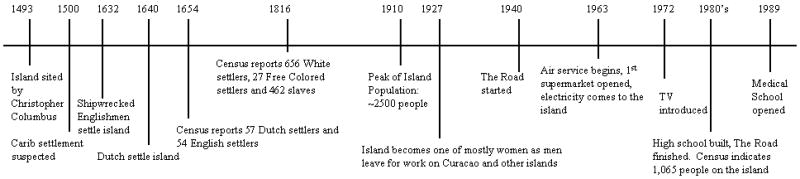
Timeline of Saban history
Previous accounts of the health of the people on Saba include a book written by a physician on the island (Mol, 1989) and a study on diet diversity in relation to hypertension (Miller et al., 1992). Mol (1989) cited hypertension, skin tumors and Type II diabetes mellitus as the primary medical conditions. He also described the demographic characteristics of the island and detailed his work with the residents. Miller et al (1992) attempted to link the high prevalence of hypertension in the population with a lack of diet diversity among the islanders, specifically a lack of legumes. This theory has not been corroborated elsewhere. While hypertension was reportedly prevalent, no studies have yet ascertained if there is a relationship between modernization of the island and high rates of hypertension. Through a survey of hypertension and obesity on the island and examination of lifestyle factors, this study aims to examine the interrelationship between hypertension and economic modernization.
Methods
Study Sample
The most current census in 2000 estimated a population of 1,195 indigenous residents (i.e., not including approximately 200 foreign medical students) on the island of Saba. Of these, approximately 900 were adults over 18 years of age. The population lives in two large villages (The Bottom and Windwardside) and two smaller villages (St. John's and Hell's Gate). Based on a census conducted in 1980, we estimated the adult population of Saba to be approximately 49% Afro-Caribbean, 49% Caucasian and 1-2% other (predominately Hispanic and Asian). A sample of 300 Saban adults was targeted for this study. The subjects were recruited through open houses at the local community centers and through house-to-house and workplace visits. Out of approximately 450 households, we knocked on the doors of 400. Someone eligible for the study answered at approximately 250 of those houses and someone agreed to participate at approximately 170 houses. A total of 278 adults participated in the first phase of the study. These participants completed brief demographic (age, sex, ethnicity, employment) and medical questionnaires (personal and familial history of hypertension and obesity along with questions on personal use of anti-hypertensives and oral contraceptives). The protocol and procedures used were approved by the Institutional Review Board of Binghamton University (SUNY).
For the second phase of the study, we contacted th4e original 278 participants to determine whether they would be interested in continuing with the study. The continuation consisted of a longer questionnaire and an interview focused on lifestyle and activity habits, income and educational level. Out of the original 278 participants, 124 agreed to participate in a follow-up interview. Those who participated in this second phase were slightly older than those who did not (mean age of 53 years as opposed to 47 years, p=0.0019). No other traits (gender, ethnicity, employment) differed between those who participated in Phase 2 and those who did not.
Measurements
For the first phase of the study, height was measured, in bare feet, on a flat surface with a standard anthropometer. Weight was measured with a Tanita BF scale with subjects wearing light, tropical clothing. Triceps skinfolds were measured with Lange skinfold calipers. Resting, seated systolic and diastolic blood pressures were measured with a Welch Allyn sphygmomanometer, using the appropriate cuff size. Hypertension was coded as 0 (no medication for high blood pressure and no blood pressure measurement over 140/90 mmHg) or 1 (medication for blood pressure or a blood pressure measurement over 140/90 mmHg). Ethnicity was coded as Afro-Caribbean, Caucasian, or other. Employment was scored, for both the interviewee and his/her spouse, as no work/retired, non-office (manual) employment, or office employment.
Questions in the second phase were grouped into the following categories: activity level, material wealth, travel, education, residence history, social contacts and family contacts. A modernization score was determined for each category and for the individual overall The activity level category produced a score that was composed of questions on work activity, whether they walk to work or to shop and what kinds of extracurricular activities they do (such as sports, or lace work, etc) (range of values = 4-8). The material wealth score was a sum of the number of household appliances and valuable items (houses, cars, TVs, dishwashers, etc) plus how long they had been owned in years (range of values=0-13). The travel score represented the frequency of travel both within and off the island (range of values=0-6). The most common travel off island was to St. Maarten, St. Eustatius (Statia), the US and the Netherlands. The education score was calculated as the number of years of schooling multiplied by where the school was (on the island =1 or off the island=2) (range of values=4-25). This was done to reflect the greater value historically placed on off-island education. The residential history code was divided into four categories, one for living only on Saba or Statia (code=0), one for living on other islands in the Caribbean (code=1), one for living outside the Caribbean in Westernized countries only for a short time (code=2) and one for living in mainly Westernized countries all their life (code=3). The social contacts score was based on the frequency of visiting with friends (range of values=3-8). The family contact score was calculated based on the proximity of family members, the frequency of visiting with family and the number of children, parents and in-laws that lived in the household (range of values=0-70). These last two categories were scored backwards so that the more social and family contacts an individual had, the lower the modernization score.
Data Analysis
Independent t tests were used to test sex differences. Multivariate linear and logistic regression models were constructed to test body composition and lifestyle factors related to the level of systolic and diastolic blood pressure and risk of hypertension. Initially, each variable was entered singly, and those that were statistically significant were sequentially added into larger models containing other significant variables. Age- and sex-adjusted prevalence estimates for hypertension were obtained using the β terms from a linear regression model: Hypertension (%) = (intercept) + (βage*mean age*100) + (βsex=male*proportion of males).
Lifestyle incongruity was measured using a model published previously (Bindon et al., 1997). Hypertension status was examined as the dependent variable and age, triceps skinfold, activity level, sex, aggregate socioeconomic rank (defined as: material wealth + household economic resources), lifestyle incongruity (defined as: material wealth - household economic resources), household employment, sex*lifestyle incongruity and household employment*lifestyle incongruity were included as independent variables.
Results
Table 1 shows the descriptive statistics for the original sample population. Subjects were 49.7 years of age on average, and mean BMI was in the overweight range for both men and women. Expected sex differences in body composition and blood pressure were observed. Among men, almost 30% of the population studied was Afro-Caribbean, 58% were Caucasian and 14% were designated as other (mostly mixed ethnicity). Among females, 38% were Afro-Caribbean, 41% were Caucasian and 21% were designated as other. A large proportion of the subjects (35% of men and 34% of women) were unemployed or retired.
Table 1.
Descriptive Statistics: Saba Adults (N=278)
| Variable | Males | Females | |||
|---|---|---|---|---|---|
| N | 86 | 192 | |||
| Mean | St dev | Mean | St dev | P value (sex difference) |
|
| Age | 52.29 | 16.93 | 48.52 | 17.15 | 0.0912 |
| Weight (kg) | 84.05 | 19.47 | 73.80 | 17.65 | <.0001 |
| Height (cm) | 173.62 | 7.65 | 160.35 | 6.95 | <.0001 |
| BMI (kg/m2) | 27.89 | 5.51 | 28.70 | 6.85 | 0.3639 |
| Triceps skinfold (mm) | 14.28 | 7.14 | 28.18 | 8.76 | <.0001 |
| Systolic Blood Pressure (mmHg) | 127.7 | 15.49 | 121.3 | 15.67 | 0.0018 |
| Diastolic Blood Pressure (mmHg) | 82.1 | 11.60 | 78.8 | 11.05 | 0.0235 |
| % ethnicity | 27.9%/ 58.1%/ 14% | 38%/ 41.1%/ 20.9% | 0.8246 | ||
| % occupation | 34.9%/ 36.0%/ 29.1% | 33.9%/ 31.3%/ 34.9% | 0.5211 | ||
BMI: Body Mass Index
Ethnicity: %Afro-Caribbean/ %Caucasian/ %other
Occupation: % with no work or retired/ % with non-office or manual job/ % with office job
The crude prevalence of hypertension was determined to be 41%, including the 69 individuals who reported having been diagnosed by a physician with hypertension and undergoing treatment (mean blood pressure=136/88 mmHg). Forty-five individuals reported no treatment for hypertension, but had blood pressure levels above 140/90 mmHg, indicating that nearly 40% of hypertensive adults (45/114) on Saba were untreated. When adjusted for age and sex, the prevalence of hypertension increased to 48%. There was no difference between treated and untreated groups based on age, gender, ethnicity or village of residence and thus these groups were combined into one group (hypertensives) for further analysis. In addition there were 10 individuals who reported that they had been told they were hypertensive once, or only when pregnant, and were not on anti-hypertensive medication. These 10 subjects had normal (below 140/90 mmHg) measured blood pressure levels and were not considered hypertensive for this study.
Univariate analysis of systolic blood pressure showed significant statistical associations between sex, age, BMI, occupation and ethnicity, with those being male, older, heavier, those having no employment, or being of Afro-Caribbean ancestry having higher systolic blood pressures than women, younger, leaner individuals and those holding office employment or being of non-Caucasian or non-Afro-Caribbean ancestry (Table 2). The relationships with diastolic blood pressure were similar (data not shown). When occupation and ethnicity were adjusted for age, sex and BMI, however, their effects on systolic blood pressure levels were diminished. Afro-Caribbean subjects also had higher risk of hypertension, but this was no longer statistically significant after adjustment for age and BMI.
Table 2.
Predictors of Systolic Blood Pressure level and Risk of Hypertension (β± SE), N=278.
| Predictors | Systolic Blood Pressure | Hypertension | ||
|---|---|---|---|---|
| β± SE | P value | β± SE | P value | |
| Model 1: Sex | ||||
| Female | -6.39±2.03 | 0.0018 | -0.23±0.29 | 0.6696 |
| Male | (referent) | (referent) | ||
| Model 2: Age | 0.30±0.05 | <0.0001 | 0.04±0.01 | <0.0001 |
| Model 3: BMI | 0.71±0.15 | <0.0001 | 0.10±0.02 | <0.0001 |
| Model 4: Occupation | ||||
| No Work/retired | 6.41±2.30 | 0.0056 | -0.12±0.48 | 0.0614 |
| Manual/non-office | 2.68±2.32 | 0.2486 | 0.36±0.44 | 0.6776 |
| Office job | (referent) | (referent) | ||
| Model 5: Ethnicity | ||||
| Afro-Caribbean | 5.74±2.71 | 0.0352 | 0.91±0.36 | 0.0118 |
| Caucasian | 4.70±2.59 | 0.0709 | 0.25±0.35 | 0.4698 |
| Other/Mixed | (referent) | (referent) | ||
| Model 6: Sex, Age, BMI | ||||
| Sex (F) | -6.47±1.92 | 0.0009 | -0.51±0.43 | 0.2287 |
| Age | 0.28±0.05 | <0.0001 | 0.04±0.01 | <0.0001 |
| BMI | 0.71±0.14 | <0.0001 | 0.12±0.02 | <0.0001 |
| Model 7: Occupation, Sex, Age, BMI | ||||
| No work/Retired | 2.05±2.34 | 0.3832 | -0.15±0.60 | 0.8043 |
| Manual/non-office | 3.24±2.13 | 0.1305 | 0.50±0.49 | 0.3030 |
| Sex (F) | -6.32±1.93 | 0.0012 | -0.45±0.43 | 0.2903 |
| Age | 0.27±0.06 | <0.0001 | 0.04±0.01 | <0.0001 |
| BMI | 0.73±0.14 | <0.0001 | 0.12±0.03 | <0.0001 |
| Model 8: Ethnicity, Sex, Age, BMI | ||||
| Afro-Carib | 1.32±2.57 | 0.6080 | -0.42±0.42 | 0.3163 |
| Caucasian | 1.38±2.39 | 0.5651 | 0.08±0.40 | 0.8390 |
| Sex (F) | -6.38±1.96 | 0.0013 | 0.52±0.32 | 0.1004 |
| Age | 0.27±0.05 | <0.0001 | -0.04±0.01 | <0.0001 |
| BMI | 0.71±0.14 | <0.0001 | -0.11±0.02 | <0.0001 |
For the models from the Phase 2 survey of socioeconomic factors and exposure to modernizing influences, residential history was statistically significant, with adults who had lived only on Saba or nearby Statia island having 7 mm Hg higher systolic blood pressure (and higher risk of hypertension) than those who had lived in the larger, more affluent St. Maarten or outside the Caribbean region (Table 3). Adults who reported no social contacts tended to have statistically significant lower mean blood pressure (by 15 mm Hg) than those who reported many/daily social contacts. However, when residential history and social contact were adjusted for age and BMI, their effects on systolic blood pressure and the risk of hypertension were no longer statistically significant. Again, diastolic blood pressure showed similar trends as systolic blood pressure and so were not shown. Although our study was not powered or designed to simultaneously examine age versus birth cohort effects, we attempted to explore this by stratifying the sample on year of birth (before and after 1955, the median birth year), and comparing the risk of hypertension associated with residence history, social contact and occupation in the two cohorts. We found a stronger relationship between off-island residence history and hypertension in the older cohort, but no difference in the effects of social contact and occupation.
Table 3.
Lifestyle Factors as Predictors of Systolic Blood Pressure and the Risk of Hypertension (β± SE), N=124.
| Predictors | Systolic Blood Pressure | Hypertension | |||
|---|---|---|---|---|---|
| Level | β ± SE | P value | β ± SE | P value | |
| Model 1: Travel | 1 (no travel) | -0.29±10.45 | 0.98 | -0.32±1.46 | 0.82 |
| 2 | -6.34±10.30 | 0.54 | -0.14±1.44 | 0.92 | |
| 3 | -5.25±10.54 | 0.62 | -0.17±1.47 | 0.91 | |
| 4 | -17.57±11.48 | 0.13 | -14.24±467.7 | 0.98 | |
| 5 | -9.00±14.32 | 0.53 | -14.24±875.0 | 0.99 | |
| 6 (extensive travel) | (referent) | (referent) | |||
| Model 2: Material Wealth | 0 (low) | -10.00±16.08 | 0.54 | -12.86±1237.4 | 0.99 |
| 1 | 4.40±6.74 | 0.52 | 1.02±1.14 | 0.37 | |
| 2 | 2.92±7.19 | 0.69 | 1.47±1.19 | 0.22 | |
| 3 (high) | (referent) | (referent) | |||
| Model 3: Residence History | 0 (Only Saba or Statia) | 7.00±2.95 | 0.02 | 1.37±0.43 | 0.001 |
| 1 (Other Caribbean) | 2.76±2.84 | 0.33 | 1.19±0.42 | 0.005 | |
| 2 (Some Westernized residence) | -1.82±3.43 | 0.60 | 0.03±0.53 | 0.95 | |
| 3 (Long-term in Westernized nation/s) | (referent) | (referent) | |||
| Model 4: Cigarette smoking | 0 (non-smoker) | 1.49±4.50 | 0.74 | 1.41±0.80 | 0.08 |
| 1 (current smoker) | (referent) | (referent) | |||
| Model 5: Alcohol consumption | 0 (None) | -7.89±5.41 | 0.15 | -0.73±0.76 | 0.34 |
| 1 | -4.83±7.10 | 0.50 | -0.29±0.99 | 0.77 | |
| 2 | -10.63±6.00 | 0.08 | -1.79±0.89 | 0.04 | |
| 3 (High) | (referent) | (referent) | |||
| Model 6: Educational level | 0 (Grade school) | 2.44±6.92 | 0.72 | 0.92±1.02 | 0.37 |
| 1 (High school) | -4.22±5.68 | 0.46 | 0.59±0.86 | 0.49 | |
| 2 (Post-secondary) | (referent) | (referent) | |||
| Model 7: Family contacts | 0 (None/little) | -0.57±10.02 | 0.95 | -14.53±714.4 | 0.98 |
| 1 (Some) | 8.42±5.69 | 0.14 | -0.71±0.79 | 0.36 | |
| 2 (Moderate) | 11.17±6.26 | 0.08 | -0.20±0.87 | 0.82 | |
| 3 (Daily/frequent) | |||||
| Model 8: Social contacts | 0 (None/little) | -14.96±6.09 | 0.02 | -1.65±1.14 | 0.15 |
| 1 (Some) | -2.49±3.38 | 0.46 | -0.33±0.47 | 0.49 | |
| 2 (Moderate) | -2.34±3.61 | 0.52 | 0.09±0.50 | 0.86 | |
| 3 (Daily/frequent) | (referent) | (referent) | |||
| Model 9: Residence history, Age and BMI | 0 (Only Saba or Statia) | 1.55±2.91 | 0.60 | 0.89±0.49 | 0.07 |
| 1 (Other Caribbean) | -0.14±2.68 | 0.96 | 0.86±0.47 | 0.07 | |
| 2 (Some Westernized residence) | -4.15±3.21 | 0.20 | -0.17±0.59 | 0.78 | |
| Age | 0.27±0.06 | <0.0001 | 0.04±0.01 | <0.0001 | |
| BMI | 0.66±0.14 | <0.0001 | 0.10±0.02 | <0.0001 | |
Greater lifestyle incongruity (the disparity between income and expenditures on material goods, in particular car, house and electronics) was associated with increased risk of hypertension (p=0.002), and this effect was found to vary based upon household employment, such that greater household employment (office-job vs no job or non-office job) reduced the risk of hypertension at a given level of lifestyle incongruity (p=0.001) (Table 4). This was true even when age was controlled for in the model.
Table 4.
Relationship between lifestyle incongruity and risk of hypertension, logistic regression model.
| Estimate | Standard Error | p (chi-square) | |
|---|---|---|---|
| Age (Years) | 0.06 | 0.02 | 0.001 |
| Sex (F) | -0.49 | 0.67 | 0.46 |
| Triceps (mm) | 0.05 | 0.03 | 0.12 |
| Activity Level | -0.01 | 0.22 | 0.98 |
| Aggregate Socioeconomic rank | -0.30 | 0.21 | 0.16 |
| Lifestyle incongruity | 3.38 | 1.08 | 0.002 |
| Household employment | -1.17 | 0.41 | 0.005 |
| Lifestyle incongruity * sex | -0.34 | 0.41 | 0.41 |
| Lifestyle incongruity * household employment | -1.20 | 0.37 | 0.001 |
Activity level: range of values= 4-8, based on activity level at work and home
Aggregate socioeconomic rank: material wealth + household income
Lifestyle Incongruity: material wealth- household income
Household Employment: occupational rank (retired/not employed, employed in a non-office job, employed in an office job) of everyone in the household
Discussion
More than 25% of the world's adult population was hypertensive in 2000 (Kearney et al., 2005), totaling nearly 1 billion adults. The highest prevalences were in the Latin America and Caribbean region and the lowest in Asia and the Pacific Islands (Kearney et al., 2005). Chronic hypertension was first recognized as a problem in the Caribbean in the 1940's (Halberstein, 1999). One of the major findings of this study, to our knowledge the first measured blood pressure and anthropometric survey conducted on the island, was a very high prevalence of hypertension among Saban adults (48% when age and sex adjusted). A previous study of self-reported hypertension as part of the Saba Health Study in 2000 found the prevalence of the disease to be 24% (Grievink et al., 2001). We suggest that due to the high rate of untreated/undetected hypertension (40% of hypertensives in the present study), the previous figure was an underestimate. To contextualize this figure, the United States currently has an age-adjusted prevalence rate of hypertension of approximately 33% (Rosamond 2007). In the US, hypertension is seen more in people of African-American descent than in Caucasians (Dressler and Bindon 2000; Collins and Winkleby, 2002), and this ethnic disparity was also evident in the current study.
One of the aims of this study was to examine economic modernization and lifestyle influences on blood pressure and hypertension in Saba. Hypertension and obesity have been implicated in several studies as a result of rapid modernization (Shapiro, 1939; Chiang et al., 1969; Reed et al., 1970, Bindon and Baker, 1985; Dressler et al., 1987; McGarvey and Schendel, 1986; Page et al., 1974; Poulter et al., 1985). With the introduction and increased accessibility of processed food and other modern conveniences, the relative rates of both hypertension and obesity tend to increase.
Counter to our expectations, we found that a history of extended residency outside the Caribbean region (e.g., in Westernized countries), as well as current employment in an office job and fewer/rarer social contacts were all associated with lower blood pressure and lower risk of hypertension in this population. None of the other individual measures of affluence or exposure to Western cultural influences were associated with risk of hypertension. Thus, while most of the lifestyle factors that we examined in this study were not associated with elevated blood pressure, there was some indication that relative affluence/Western style of life (characterized by office employment, infrequent social contact and extensive travel residency outside the Caribbean) was protective. One possible explanation is that individuals who were younger and leaner had higher scores on affluence and Western style of life, yet lower risks of hypertension. We suspect that the apparent protection of affluence and exposure to Western influences may be due to the negative correlation of age and those factors. When age and BMI were accounted for, occupation, residence history and extent of social contact were no longer statistically significant. Since office workers and those who have lived off-island also tended to be younger than their unemployed/retired/non-migrant counterparts, it was perhaps not possible to disentangle these factors from the strong influence of age on hypertension. Thus, we suspect that the relationship between Western influence/modernization and hypertension may be confounded by age in these models. Although the cross-sectional nature of the data does not allow us to clearly distinguish cohort and age effects from one another, we explored differences in the relationship of lifestyle factors on blood pressure and hypertension between those born before 1955 and those born after 1955 (median split). These results suggest that while the association between hypertension and residence history may differ between the earlier cohort and the most recent cohort, other variables such as occupation and social contacts did not differ. This may be because of the more recent changes in occupation and social contacts compared to those changes in residence history among people on the island, where there has been a large amount of migration on and off the island since the 1900's. It would be important to re-examine Saban adults in 10-20 years to see if deleterious effects of occupation, residential history and a more “Western” lifestyle may emerge as these individuals age, or if, indeed, the less affluent, less traveled individuals are experiencing a greater risk of hypertension. This is important because there has been a substantial shift in affluence, access to different types of food and cars since the 1970's. These factors became more widespread in the 1980's and the younger cohort has been exposed to much more of these factors than previous cohorts.
Lifestyle incongruity (that is, having many ‘modern’ amenities without the income to comfortably afford them) was found to be a statistically significant risk factor for hypertension, and that this risk was reduced as the household employment score increased. This finding is in line with that of Dressler, who found that status inconsistency (that is, having differing scores on categories of modernization using scales of social factors), led to an increase in blood pressure (Dressler, 1982). Specifically, owning more things than one could afford led to an increase in blood pressure. However, more social contact was found to be protective, which was not found here. It is possible that the extensive government welfare support on Saba is creating a picture of hypertension that more greatly resembles that of a developed nation, in which chronic disease risk is concentrated in the lower socioeconomic strata.
Many of the lifestyle and modernization factors hypothesized to be associated with elevated blood pressure (e.g., educational status, travel history, family contact) were not statistically significant, or were explained by age and adiposity (BMI) in this population, and therefore the high prevalence of hypertension on Saba remains largely unexplained. Hypertension has been shown to have a moderately strong genetic component (h2= 0.15-0.40) (van Rijn et al, 2007; Knuiman et al., 1996; Mitchell et al., 1996; North et al., 2003; Hsueh et al., 2000; Ober et al., 2001; Adeyemo et al., 2002). Given the relative isolation of the island and possible founder/ genetic bottleneck effects that would have reduced genetic diversity on the island, it is possible that hypertension-promoting alleles may be in higher frequency in Saba than in other populations. Salt or mineral intake through the water catchment system and diet may also be to blame for the unusually high blood pressures seen on the island, although sodium chloride as a factor has been far from conclusive in other studies (James et al., 1996). Continuing work focuses on estimating the heritability of blood pressure and obesity on Saba, and the interaction of genetic predisposition and lifestyle factors on hypertension risk.
Strengths and Limitations
This study represents the only known report of measured blood pressure and anthropometrics conducted on the island of Saba, and therefore represents a unique contribution to the study of lifestyle change, economic modernization and chronic disease epidemiology in the Caribbean. The sampling frame, while intended to be a random sample of residents and including a full 31% of all adult Saba residents, does contain the possibility of selection bias. We suspect that younger residents were less likely to participate and were also more likely to work outside the home. Both of these factors may have biased the estimates toward higher prevalences of hypertension. In contrast, the lower participation rate of males than females in our study would have likely resulted in lower estimates of hypertension prevalence. Therefore, we age- and sex-adjusted the prevalence estimates. In the second phase of the study, the age of the participants was slightly older than in the first phase of the study (p<0.05). Because the older Saban residents tended to have lower employment and travel status, this may have made it more difficult to disentangle age effects from lifestyle effects. Another limitation of the study is the lack of dietary information for the study sample, as nutritional factors may play an important role in hypertension.
Conclusion
In this first survey of chronic disease risk factors and lifestyle on Saba, hypertension and a BMI status in the overweight category were found to be highly prevalent and associated with increased lifestyle incongruity. Contrary to a number of previous reports on the effects of modernization on blood pressure, but similar to what is found in developed nations, we found that relative economic advantage (at least as represented by current white-collar employment and extensive travel) was associated with lower blood pressure compared to that of more disadvantaged subjects. The greater age, greater BMI and Afro-Caribbean ethnicity of disadvantaged individuals may explain the direction of this relationship. Further work will examine genetic influences on blood pressure and their interaction with variations in diet and lifestyle in this rapidly changing island population.
Literature Cited
- Adeyemo AA, Omotade OO, Rotimi CN, Luke AH, Tayo BO, Cooper RS. Heritability of blood pressure in Nigerian families. J Hypertens. 2002;20:859–863. doi: 10.1097/00004872-200205000-00019. [DOI] [PubMed] [Google Scholar]
- Baker P. Rationale and Research Design. In: Baker P, Hanna J, Baker T, editors. The Changing Samoans: behavior and health in transition. New York: Oxford University Press; 1986. pp. 3–18. [Google Scholar]
- Bindon J, Baker P. Modernization, migration and obesity among Samoan adults. Ann Hum Biol. 1985;12:67–76. doi: 10.1080/03014468500007571. [DOI] [PubMed] [Google Scholar]
- Bindon JR, Knight AL, Dressler WW, Crews DE. Social Context and Psychosocial Influences on Blood Pressure among American Samoans. Am J Phys Amthropol. 1997;103:7–18. doi: 10.1002/(SICI)1096-8644(199705)103:1<7::AID-AJPA2>3.0.CO;2-U. [DOI] [PubMed] [Google Scholar]
- Chiang B, Perlman L, Epstein F. Overweight and hypertension: a review. Circulation. 1969;39:403–421. doi: 10.1161/01.cir.39.3.403. [DOI] [PubMed] [Google Scholar]
- Collins R, Winkleby MA. African-American women and men at high and low risk for hypertension: a signal detection analysis of NHANES III, 1988-1994. Prev Med. 2002;35:303–312. doi: 10.1006/pmed.2002.1081. [DOI] [PubMed] [Google Scholar]
- Crane J. Educated to emigrate: the social organization of Saba. Netherlands: Royal VanGorcum Ltd; 1971. [Google Scholar]
- Dressler W. Hypertension and Culture Change: Acculturation and Disease in the West Indies. New York: Redgrave Publishing Company; 1982. [Google Scholar]
- Dressler W, Dos Santos J, Gallagher PJ, Viteri F. Arterial blood pressure and modernization in Brazil. Am Anthropol. 1987;89:398–410. [Google Scholar]
- Dressler WW, Bindon J. The Health Consequences of Cultural Consonance: Cultural Dimensions of Lifestyle, Social Support and Arterial Blood Pressure in an African American Community. Am Anthropol. 2000;102:244–260. [Google Scholar]
- Garruto R, Little M, James G, Brown D. Natural experimental models: The global search for biomedical paradigms among traditional, modernizing, and modern populations. PNAS. 1999;96 August:10536–10543. doi: 10.1073/pnas.96.18.10536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grievink L, Fuchs G, O'Niel J, van Sonderen E, Gerstenbluth I, Alberts J. The Saba Health Study: How healthy is Saba? Methodology and main results. Curacao: ISOG; 2001. [Google Scholar]
- Halberstein R. Blood pressure in the Caribbean. Hum Biol. 1999;71:659. [PubMed] [Google Scholar]
- Hartog J. History of Saba. Saba, Netherlands Antilles: Saba Artisan Foundation; 1982. [Google Scholar]
- Hsueh WC, Mitchell BD, Aburomia R, Pollin T, Sakul H, Gelder EM, Michelsen BK, Wagner MJ, St Jean PL, Knowler WC, Burns DK, Bell CJ, Shuldiner AR. Diabetes in the Old Order Amish: characterization and heritability analysis of the Amish Family Diabetes Study. Diabetes Care. 2000;23:595–601. doi: 10.2337/diacare.23.5.595. [DOI] [PubMed] [Google Scholar]
- James GD, Pecker MS, Pickering TG. Sex differences in casual and ambulatory blood pressure responses to extreme changes in dietary sodium. Blood Press Monit. 1996;1:397–401. [PubMed] [Google Scholar]
- Kearney P, Whelton M, Reynolds K, Muntner P, Whelton P, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- Knuiman MW, Divitini ML, Welborn TA, Bartholomew HC. Familial correlations, cohabitation effects and heritability for cardiovascular risk factors. Ann Epidemiol. 1996;6:188–194. doi: 10.1016/1047-2797(96)00004-x. [DOI] [PubMed] [Google Scholar]
- MacQueen KM. PhD Dissertation. Binghamton University; 1989. Migration in Saba Island: An Historical Demographic Analysis of a Multigenerational Process. [Google Scholar]
- McGarvey S, Schendel D. Blood Pressure of Samoans. In: Baker P, Hanna J, Baker T, editors. The Changing Samoans: behavior and health in transition. New York: Oxford University Press; 1986. pp. 351–393. [Google Scholar]
- Miller G, Maude G, Beckles G. Incidence of hypertension and non-insulin dependent diabetes mellitus and associated risk factors in a rapidly developing Caribbean community: the St. James survey, Trinidad. J Epidemiol Community Health. 1996;50:497–504. doi: 10.1136/jech.50.5.497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller W, Crabtree B, Evans D. Exploratory study of the relationship between hypertension and diet diversity among Saba Islanders. Public Health Rep. 1992;107:426–432. [PMC free article] [PubMed] [Google Scholar]
- Mitchell BD, Kammerer CM, Blangero J, Mahaney MC, Rainwater DL, Dyke B, et al. Genetic and environmental contributions to cardiovascular risk factors in Mexican Americans: The San Antonio Family Heart Study. Circulation. 1996;94:2159–2170. doi: 10.1161/01.cir.94.9.2159. [DOI] [PubMed] [Google Scholar]
- Mol R. Doctor on Saba: health care and disease in a Caribbean family practice. Delft: Eburon; 1989. [Google Scholar]
- North KE, Howard BV, Welty TK, Best LG, Lee ET, Yeh JL, Fabsitz RR, Roman MJ, MacCluer JW. Genetic and environmental contributions to cardiovascular risk in American Indians: the strong heart family study. Am J Epidemiol. 2003;157:303–314. doi: 10.1093/aje/kwf208. [DOI] [PubMed] [Google Scholar]
- Ober C, Abney M, McPeek MS. The genetic dissection of complex traits in a founder population. Am J Hum Genet. 2001;69:1068–1079. doi: 10.1086/324025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Page L, Damon A, Moellering R. Antecedents of cardiovascular disease in six Solomon Island societies. Circulation. 1974;49:1132–1146. doi: 10.1161/01.cir.49.6.1132. [DOI] [PubMed] [Google Scholar]
- Poulter N, Khaw K, Hopwood B, Mugambi M, Peart W, Rose G, Sever P. Blood pressure and associated factors in a rural Kenyan community. Hypertension. 1985;6:810–816. doi: 10.1161/01.hyp.6.6.810. [DOI] [PubMed] [Google Scholar]
- Reed D, Labarthe D, Stallones R. Health effects of westernization and migration among Chamorros. Am J Epidemiol. 1970;92:94–112. doi: 10.1093/oxfordjournals.aje.a121190. [DOI] [PubMed] [Google Scholar]
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, Haase N, Ho M, Howard V, Kissela B, et al. Heart disease and stroke statistics—2007 update: a report from the American heart Assocaition Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115(5):e69–171. doi: 10.1161/CIRCULATIONAHA.106.179918. [DOI] [PubMed] [Google Scholar]
- Shapiro H. Migration and Environment. New York: Oxford University Press; 1939. [Google Scholar]
- van Rijn MJE, Schut AFC, Aulchenko YS, Deinum J, Sayed-Tabatabaei FA, Yazdanpanah M, Isaacs A, Axenovich TI, Zorkoltseva IV, Zillikens MC, Pols HAP, Witteman Cm, Oostra BA, van Duijn CM. Heritability of blood pressure traits and the genetic contribution to blood pressure variance explained by four blood-pressure-related genes. J Hypertens. 2007;25:565–570. doi: 10.1097/HJH.0b013e32801449fb. [DOI] [PubMed] [Google Scholar]