

Abstract
The present study sought to uncover the relationship between risk and protective factors for depressive symptomatology among runaway youth. To that aim, three models of resiliency - the compensatory, risk-protective, and challenge models - were tested separately on girls and boys. The data came from a cross-sectional survey on a sample of 140 runaway adolescents between the ages of 12 to 17 years who were recruited from the only runaway crisis shelter in a large Midwestern city. Risk factors in the proposed model included primary caretakers’ depressive symptoms, family conflict, and adolescent’s and primary caretaker’s verbal aggression; protective factors included adolescent’s report of task oriented coping and family cohesion. Findings supported the challenge model for predicting adolescent depressive symptoms, suggesting that moderate levels of risk can be beneficial for these runaway adolescents. In addition, risk and protective factors differed by adolescent gender. Implications for preventive interventions and future research are discussed.
Introduction
Runaway youth are one of the most understudied and vulnerable homeless populations nationwide. In a given year, it is estimated that 1.6 million youth aged 12 to 17 years run away from home and sleep on the streets (SAMHSA, 2003), and one out of every seven children will run away before the age of 18 (Son, 2002). Research concludes that severe parental abuse and neglect (Thrane, Hoyt, Whitbeck, & Yoder, 2006), high rates of substance use (Bousman et al., 2005; Nyamathi, Christiani, Windokun, Jones, Strehlow, & Shoptaw, 2005), and poor physical and mental health (Kamienieck, 2001; Nyamathi, Christiani, Windokun, Jones, Strehlow, & Shoptaw, 2005) are prevalent among runaways. These youth are more susceptible to depression than adolescents without a history of running away (De Man, 2000) and are at high risk for suicide (Kidd, 2006; Whitbeck, Hoyt, Bao, 2000). In fact, studies suggest that approximately 31–89% of runaway youth met criteria for major depression according to DSM-III-R or DSM-IV criteria (Chen, Thrane, Whitbeck, & Johnson, 2006; National Coalition for the Homeless, 2006; Whitbeck, Johnson, Hoyt, & Cauce, 2004) whereas only 9–14% of non-runaway youth met these criteria (SAMHSA 2005; 2007).
Despite the high prevalence of depressive symptoms among runaways, there is little research identifying risk and protective factors for depression. Although several studies (Compas, Connor-Smith, & Jaser, 2004; Van Voorhees, Paunesku, Gollan, Kuwabara, Reinecke, Basu, 2008; Werner & Smith, 2001) have investigated individual risk factors for depression, the contribution of the family environment to depression remains unexplored. In addition, intervention efforts often take a deficit perspective that focus on decreasing youth problem behaviors (Masten, 2001), and few studies have sought to examine resilience among at risk youth using family variables. Therefore, the purpose of the present study was to determine the relationship between risk and protective factors associated with depressive symptoms among runaway youth by testing three resiliency models.
Adolescent Depression in the Family Context: Risk and Protective Factors
Prior research suggests that families with a depressed member show deficits in communication and interpersonal relations (Sander & McCarty, 2005) highlighting the importance of evaluating family-level variables associated with depressive symptoms. In particular, studies on at-risk adolescents indicate that those who have a depressed parent (Weissman & Jensen, 2002), experience parental verbal aggression and abuse (Reinherz, Paradis, Giaconia, Stashwich, & Fitzmaurice, 2003) and live in families with high levels of family conflict (Kane & Garber, 2004) are at higher risk of having depressive symptoms. In contrast, family cohesion or bonding has been consistently linked to well-being among at-risk adolescents (Sheeber, Hops, & Davis, 2001). In addition, adolescent coping skills, particularly task oriented or active coping strategies, have been found to promote family bonding (Sander & McCarty, 2005) and are associated with fewer depressive symptoms and less suicidality (Kidd & Carroll, 2007; Votta & Manion, 2003).
Research on families of runaway adolescents indicates that runaways are exposed to most of these risk factors for depression. These families are characterized by high levels of hostility, conflict (Mallett, Rosenthal, & Keys, 2005), and verbal abuse (Hyde, 2005). Parental depression and family distress are prevalent (Lindsey, Kurtz, Jarvis, Williams, & Nackerud, 2000). However, the strengths of runaway youth to cope with risks within this context should be evaluated further. The present study aims to address this gap in the literature.
Theoretical Perspective: Construct of Resilience
As Kumpfer and Alvarado (2003) suggested, interventions that promote strengths in the family, such as enhancing parenting skills and communication, are most effective at decreasing youth problem behavior. This strategy, to learn from the strengths of families coping with stress, might help identify effective prevention strategies to enhance positive youth development and family functioning (Zimmerman & Arunkumar, 1994). To that aim, the resiliency perspective was utilized in the current study as a framework for understanding the relationship between risk and protective factors associated with depressive symptoms among runaway youth.
Resilience refers to the individual’s successful utilization of available social, familial or personal resources in order to achieve normative development in the context of adversity (Fraser, Richman, & Galinsky, 1999). In this study, operationalization of resilience was based on Masten’s (2001) definition; that is, resilience is defined as “a class of phenomena characterized by good outcomes in spite of serious threats to adaptation or development” (p. 228). According to this framework, resilience is a contextual, dynamic construct that requires individuals to (1) be exposed to adversity in multiple domains that put them “at risk” and (2) have good functioning, adjustment and achieve normative development (Masten, 2001). The risk side of Masten’s definition was operationalized in this study as problems in the family environment and interactions, while positive outcome was operationalized as significantly lower levels of adolescent depressive symptoms.
Models of Resiliency
Several models of resiliency, the Compensatory, Risk-Protective, and Challenge models, were developed to understand how risk and protective factors function in relation to each other in the context of adversity (Garmezy, Masten, & Tellegen, 1984). In an effort to investigate the relationship between risk and protective factors, three models of resiliency commonly tested in the literature were utilized in this study (Figure 1).
Figure 1.
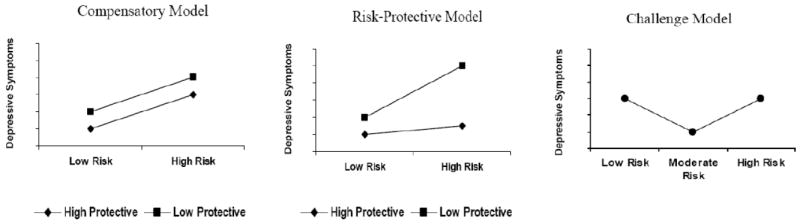
Models of Resiliency
The Compensatory Model suggests that risk and protective factors combine additively to predict the outcome variable, and they have independent and direct effects on the outcome variable. Risk factors increase risk for negative outcome while protective factors counteract or neutralize the effects of risk by positively affecting the outcome (Garmezy, Masten, & Tellegen, 1984).
The Risk-Protective Model is the most widely studied model in the literature (Masten, 2001). In this model, protective factors interact with risk factors creating a buffering effect that either dampens or amplifies the impact of the risk factor on the outcome (Garmezy, Masten, & Tellegen, 1984). Due to this interaction between risk and protective factors, this model suggests that protective factors have a greater effect on the outcome at one particular level of risk than at other levels of risk.
The Challenge Model is a model suggesting that a moderate amount of risk exposure is more beneficial than no exposure to risk in reducing the negative outcome (Garmezy, Masten, & Tellegen, 1984). That is, risk factors function as potential enhancers of the positive outcome variable. Zimmerman and Arunkumar (1994) argue that moderate rather than low or high levels of risk may be “protective” because moderate risk provides a ‘challenge’ for the individual – which is not easy, but is possible to overcome. This model claims that once the challenge is met, one has the potential to strengthen his or her competence to prepare for the next difficulty (Zimmerman & Arunkumar, 1994). This model has rarely been tested in the resiliency literature because researchers typically focus on functions of protective factors, whereas the primary concern of the challenge model is the effect of different levels of risk on outcome (Masten, 2001).
Current Study
Although the association between adolescent depression and family functioning is well established in the literature, research on at-risk youth primarily takes a deficit perspective, focusing on risk factors and negative outcomes. This study addresses the need in the literature to reveal the strengths, rather than deficits, in the family system among substance-abusing runaway adolescents. Identification of the strengths of runaway youth can provide useful information about how they resist risks. Information regarding adolescent resilience can be used to help other at-risk youth to enhance their strengths and strategies to overcome risk. Thus, the major objectives of the current study were to (1) explore the risk and protective factors associated with runaways’ depressive symptoms, and (2) examine how the protective factors function in relation to available risk factors to predict their depressive symptoms. To that aim, potential risk factors (family conflict, verbal aggressiveness of the adolescent and primary caretaker, and depressive symptoms of the primary caretaker) as well as protective factors (family cohesion, and adolescent’s task oriented coping) were selected to predict adolescents’ depressive symptoms. Then, three models of resiliency were tested to determine which model was most useful in explaining adolescent resiliency in depressive symptomatology. Because resiliency research on adolescents has consistently found gender differences (e.g. Christiansen & Evans, 2005; Gomez &McLaren, 2006; Hollister-Wagner, Foshee, & Jackson, 2001), models were tested separately for boys and girls. To our knowledge, this exploratory study is unique in the sense that resiliency models have never been empirically tested among runaway adolescents.
Method
Participants
Participants were recruited as part of a larger randomized clinical trial testing adolescent substance abuse interventions. Baseline data from that study were utilized for the current project. Youth were recruited from the only runaway crisis shelter in a Midwestern city from February 2005 to April 2007. To be eligible for the study, youth had to be residing at the crisis shelter, be between the ages of 12 to 17 years, have the legal option of returning to a home situation (including foster home or with another family member), meet DSM-IV diagnostic criteria for Psychoactive Substance Use or Alcohol disorder as assessed by the computerized Diagnostic Interview Schedule for Children (CDISC; Shaffer, 1992), and have at least one parent, or a surrogate parent (primary caretaker) willing to participate in the study. Of the 467 youth who were approached at the shelter, 62.7% (N = 293) were eligible and 61.4% (N = 180) of eligible youth were successfully engaged into the study. Because data entry and cleaning are still in progress for the 180 youth, a total of 140 youth had complete data at the time of the analysis and comprised the sample for the current study.
Sample characteristics
Of the 140 youth, the mean age was 15.5 years (SD = 1.2), and 72 (51.4%) were female (Table 1). The majority of youth were African American (62.9%), approximately one-third were White, non-Hispanic (31.4%), 1.4% were Hispanic and 1.4% were American Indian/Alaskan Native. Adolescents reported repetitive runaway episodes (M = 3.2, SD = 6.3), and high alcohol and substance use with an average of 28.8% days of use in the prior 90 days (Range = 3.42-100, SD = 27.2) (Table 2). Adolescent’s average Beck Depression Inventory-II score was 14.7 (Range = 0-48, SD = 12.5). Girls reported significantly more severe symptoms of depression (M = 17.5) than did boys (M = 12.3) [t(131) = 2.42, p < .05].
Table 1.
Sample Characteristics (N = 140)
| (%) | |
|---|---|
| Gender | |
| Female | 51.4 |
| Male | 48.6 |
| Age | |
| 12 | 1.4 |
| 13 | 5.0 |
| 14 | 10.0 |
| 15 | 34.3 |
| 16 | 27.9 |
| 17 | 21.4 |
| Race/ethnicity | |
| African American | 62.9 |
| White, non-Hispanic | 31.4 |
| Native American | 1.4 |
| Hispanic | 1.4 |
| Mixed/other | 2.9 |
Table 2.
Intercorrelations of Measures of Depressive Symptoms, Risk Factors and Protective Factors
| O | R1 | R2 | R3 | R4 | P1 | P2 | |
|---|---|---|---|---|---|---|---|
| O- Adolescent’s depressive symptoms † | 1 | .28** | .28** | .15 | .19* | -.02 | -.31** |
| R1- Primary caretaker’s depressive symptoms ‡ | 1 | .24** | .18* | .08 | .04 | -.09 | |
| R2- Adolescent’s verbal aggression † | 1 | .71** | .27** | .06 | -.24** | ||
| R3- Primary caretaker’s verbal aggression † | 1 | .37** | .09 | -.22* | |||
| R4- Family conflict † | 1 | -.05 | -.51** | ||||
| P1- Adolescent’s task-oriented coping † | 1 | .21* | |||||
| P2- Family cohesion † | 1 |
Note: O=Outcome, R=Risk factor, P=Protective factor.
p < .05.
p < .01.
Adolescent report.
Primary caretaker report.
Procedure
Youth at the runaway shelter who were identified as potentially eligible for participation were interviewed in-person by a research assistant (RA). Recruitment took place in the first 24 hours of the youth’s arrival to the shelter. Youth were screened by a RA and those passing eligibility criteria were engaged into the project. Prior to the youth’s assessment, RAs contacted the adolescent’s parent or legal guardian via phone to arrange an appointment to meet, review the study requirements, sign the consent statement, and complete their evaluation. Once the parent provided consent, the adolescent’s signed assent was obtained. The interviewer administered the CDISC (Shaffer, 1992) to the adolescent, which included sections on alcohol, marijuana and other substance use to determine formal eligibility. Those who were not eligible continued with the shelter program whereas those who met the diagnostic criteria for substance abuse were included in the study and were administered the self-report and interview questionnaires. The adolescent’s assessment required approximately three hours to complete and adolescents were offered a $40 gift card at the completion of the interview. The parent’s assessment was conducted at their home and each parent was offered $25 cash for completing the interview. All procedures in the study were approved by the university’s Institutional Review Board.
Measures
A demographic questionnaire was used to assess adolescent’s age, gender, ethnicity, in addition to runaway behavior and homeless experiences.
As noted earlier, Shaffer’s CDISC (1992) was utilized in the study for determining formal eligibility. CDISC is a computerized instrument, consisting of 263 items that measure the criteria for DSM IV diagnoses among children and adolescents. In the current study, only the sections on alcohol, substance use, and psychosis were utilized.
The Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996) was administered to youth and their primary caretakers to assess depressive symptoms. The BDI-II is comprised of 21 items rated on a 4-point scale. These items were summed to create an index of depressive symptoms (range 0 to 63) with higher scores indicating higher levels of depressive symptoms. In the current study, Cronbach alphas for adolescents and primary caretakers were .94 and .93, respectively.
The Family Environment Scale (FES; Moos & Moos, 1986) was utilized to assess adolescents’ perceptions of the family environment and family relations. The 90 true-false items identify ten subscales which measure the following social-environmental characteristics of families: Cohesion, Expressivity, Conflict, Independence, Achievement-Orientation, Cultural-Religious Emphasis, Organization, and Control. Given that family Conflict and Cohesion have been shown to predict negative communication exchanges in delinquent and clinic-referred families (Mas, 1986), these two subscales were used to assess family functioning and disturbance in the current study. The Conflict and Cohesion subscales were each composed of nine items. Possible scores ranged from 0 to 9 for each subscale, with higher scores indicating higher levels of Cohesion and Conflict. Internal consistency of the Conflict subscale was .55 and was .73 for the Cohesion subscale.
The Conflict Tactics Scale (CTS; Straus, 1979) was administered to adolescents to assess the occurrence of various methods of conflict resolution in their relationships with their primary caretakers. The CTS includes 36 items, rated on a 0 (never) to 6 (more than 20 times) 7-point scale. The scale has three subscales that measure the extent to which reasoning, verbal aggression, and physical violence are employed as a means to resolve disagreements. One advantage of using the CTS is that the adolescent reports not only his or her own conflict tactics, but also his or her perception of parents’ reasoning, verbal aggressiveness, and violence. Given the high level of conflict and high verbal aggression among runaway youth and families (Patel & Greydanus, 2002; Thompson, Maguin, & Pollio, 2003), the verbal aggression subscale was utilized in this study. Each verbal aggressiveness subscale (verbal aggressiveness of self and verbal aggressiveness of other) included six items. These items were summed to compute the adolescents’ perceptions of his/her verbal aggressiveness and of his/her primary caretaker. Scores can range from 0 to 36, with higher scores indicating higher levels of verbal aggressiveness. Cronbach alpha for adolescent’s report of their own verbal aggressiveness was .67, and was .65 for their report of their parents; verbal aggressiveness.
The Coping Inventory for Stressful Situations-Adolescent version (CISS-A; Endler & Parker, 1990) was used to measure youth’s coping. The CISS-A consists of 48 items rated on a 1 (not at all) to 5 (very much) scale. The three factor analytically derived subscales are task-oriented, emotion-oriented, and avoidance-oriented coping. Adolescent task oriented coping was utilized for the current study because research shows that task-oriented coping is a positive coping strategy which is related to resilience (Billings & Moos, 1982). The reliability of the scale for this sample was .97.
Statistical Analysis
In an attempt to address the first research objective, initial analysis focused on specific risk and protective factors associated with depressive symptoms. To that aim, all risk and protective factors were entered into the multiple regression equation in an enter method to test for the independent effects of each variable for predicting adolescents’ depressive symptoms. This type of regression analysis was preferred because it is advantageous to test models of association as well as partition the variance for each variable (Cohen & Cohen, 1983). Because gender differences in risk and protective factors of depressive symptoms were expected, statistical analysis was conducted separately for boys and girls.
Next, further analysis was conducted to address the second research objective. The analysis focused on testing the resiliency models via the cumulative effects of risk and protective factors on depressive symptomatology. Based on Pollard and Hawkins’ (1999) statistical analysis approach, standardized z-scores were calculated for each of the specific predictors because scales had different ranges. Then, z-scores of risk factors for adolescent depression (adolescent’s report of verbal aggression of himself/herself, adolescent’s report of verbal aggression of his/her primary caretaker, adolescent’s report of family conflict, and primary caretaker’s report of their own depressive symptoms) were summed and the mean was labeled as “risk index.” The reliability coefficient of the risk index was .72.
The same procedure was utilized for computing protective indices for which z-scores of protective factors for adolescents (adolescent’s report of family cohesion, adolescent’s task oriented coping) were added and means were calculated to indicate “protective index.” Because the protective index included only two variables, the reliability coefficient was not computed. These risk and protective indices estimate the cumulative effects of risk and protective factors, as suggested in similar studies (i.e. Christiansen & Evans, 2005).
Finally, the interaction terms were computed following the suggested procedure in the literature (Garmezy, Masten, & Tellegen, 1984). The risk index and protective index were multiplied to create risk and protective interaction. Similarly, the risk index was multiplied with itself to compute risk and risk interaction (the quadratic term). These indices were utilized to test for the risk-protective and challenge models of resiliency, respectively (Fergus & Zimmerman, 2005; Pollard, Hawkins, & Arthur, 1999).
Hierarchical linear regression analysis was utilized to test for the compensatory, risk-protective and challenge models of resiliency. This statistical approach was preferred because it allowed the unique effects of each variable in the model to be controlled. The order of entry relied on strategies recommended in the literature (Fraser & Richman, 1999; Pollard, Hawkins, & Arthur, 1999). The risk index was entered first, followed by the protective index in the second step (compensatory model). For the third block, the interaction term of the risk and protective index was included to test for the risk-protective model. Finally, the risk and risk index was included in the model as a fourth step to test for the challenge model of resiliency.
As Fraser and Richman (1999) suggest, this approach takes an “immunization” perspective. That is, the risk index serves as a “pathogen” and the protective index serves as a vaccine, therefore the protective index would be meaningful only if risk was present. Interaction terms were entered stepwise in the final blocks because they would be meaningful only after controlling for the main effects of the risk and protective indices.
Results
Correlational Analysis
Most of the intercorrelations between key study variables were low to medium in magnitude (Table 2). Specifically, adolescents’ depressive symptoms were significantly associated with primary caretakers’ depressive symptoms (r = .28). Adolescent’s perceived verbal aggression of his/her primary caretaker was highly correlated with adolescent’s own verbal aggression (r = .71). In addition, perceived family conflict and family cohesion were negatively correlated (r = -.51).
Research Objective 1: Independent Effects of Risk and Protective Factors
In an effort to predict adolescents’ depressive symptoms, multiple linear regression was utilized (Table 3). Results revealed that high family cohesion predicted lower levels of depressive symptoms for girls (p = .000), functioning as a protective factor within the family system. On the other hand, depressive symptoms of primary caretakers functioned as a risk factor only for boys’ depressive symptoms (p = .034). Girls’ depressive symptoms were associated with perceived verbal aggression of their primary caretakers (p = .035). The full model with all variables explained 18% and 39% of the variance in boys’ and girls’ depressive symptoms, respectively.
Table 3.
Results of Multiple Linear Regression Analysis for the Prediction of Adolescent’s Depressive Symptoms
| Boys | Girls | |||
|---|---|---|---|---|
| Predictors | B (SE) | B | B (SE) | β |
| Risk Factors | ||||
| Constant | 13.1 (7.96) | - | 14.61 (1.91) | - |
| Primary caretaker’s depressive symptoms ‡ | .42 (.19) | .32* | -2.74 (2.09) | -.17 |
| Adolescent’s verbal aggression † | -.15 (.39) | -.09 | -.94 (4.0) | -.03 |
| Primary caretaker’s verbal aggression ‡ | .31 (.37) | .19 | 6.03 (2.77) | .37* |
| Family conflict † | .01 (1.13) | .000 | 1.33 (3.39) | .07 |
| Protective Factors | ||||
| Adolescent’s task-oriented coping † | -.09 (.09) | -.14 | 1.33 (3.39) | .07 |
| Family cohesion † | -.62 (.84) | -.12 | -14.61 (1.91) | -.86*** |
| Full model | ||||
| Overall F | 1.64 (NS) | 4.9** | ||
| Total R2 | .18 | .39 | ||
| Adjusted R2 | .07 | .31 | ||
NOTE: B, SE, ß̣ are presented for the final model after all predictor variables have been entered.
p < .05.
p < .01.
p < .001.
Adolescent report.
Primary caretaker report.
In summary, results suggested that boys were more likely to report depressive symptoms if their primary caretakers also reported depressive symptoms. Family cohesion was associated with lower levels of depression for girls but not for boys, indicating gender differences in those variables predicting depressive symptoms.
Research Objective 2: Test of Resiliency Models
Hierarchical linear regression analysis was utilized to test the models of resiliency. Results showed significant gender differences in predicting depressive symptoms among adolescents (Table 4). For girls, neither the risk nor the protective index was significant in predicting depressive symptoms. Because there was no main effect for either index, the compensatory model of resiliency was not supported. The only significant predictor in girls’ depressive symptoms model was the quadratic term (risk X risk) (p = .035). Thus, there was support for the challenge model of resiliency, which accounted for an additional 7.5% variance in depressive symptoms.
Table 4.
Results of Hierarchical Regression Analysis for the Prediction of Adolescent’s Depressive Symptoms: Test of Resiliency Models
| Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|
| Predictors | B (SE) | β | ΔR2 | B (SE) | β | ΔR2 | |
| Step | |||||||
| Constant | 10.5 (2.05) | - | - | 14.61 (1.91) | - | - | |
| 1 | Risk Index | 5.25 (2.42) | .33* | .07 | 1.33 (3.39) | .06 | .12* |
| 2 | Protective Index | -4.2 (2.25) | -.26 | .05 | -2.74 (2.09) | -.17 | .02 |
| 3 | Risk X Protective Index | .92 (2.95) | .05 | .00 | -.94 (4.00) | -.032 | .01 |
| 4 | Risk X Risk Index | 6.74 (2.5) | .36* | .12* | 6.03 (2.78) | .37* | .08* |
| Full model | |||||||
| Overall F | 3.61* | 3.46* | |||||
| Total R2 | .23 | .22 | |||||
| Adjusted R2 | .16 | .16 | |||||
NOTE: B, SE, ß̣ are presented for the final model after all predictor variables have been entered, ΔR2 is presented for the model after each step.
p < .05.
p < .01.
p < .001.
Contrary to the results for girls, the risk index was a significant predictor of depressive symptoms for boys (p = .035). That is, boys’ depressive symptoms were likely to increase as their levels of exposure to risk increased. However, the challenge model was also supported for boys (p = .01) and the quadratic term suggested a 12% increase in the explained variance in depressive symptoms. Thus, low and high levels of risk were associated with higher depressive symptoms among adolescents regardless of gender. In other words, adolescents were more resilient to depression at medium levels of risk exposure. The final model of resiliency explained 22% and 23% of variance in depressive symptoms of girls and boys, respectively (Table 4).
Discussion
The goals of the current study were to determine the risk and protective factors of depressive symptoms, and test the effectiveness of three resiliency models among runaway adolescents. Results suggested that the risk and protective factors associated with depressive symptoms were different for girls and boys. In addition, the challenge model of resiliency was supported in regard to understanding the relationship between cumulative risk and protective factors and depressive symptomatology among these adolescents.
Risk and Protective Factors in the Family Context
This study showed that primary caretaker depressive symptomatology was a risk factor for boys’ depressive symptoms but not for girls’ depressive symptoms. However, previous research suggested that girls, compared to boys, were more susceptible to depression if their parents were depressed (Weissman & Jensen, 2002). Furthermore, findings revealed that primary caretaker’s verbal aggression was a risk factor for girls’ depressive symptoms. Possibly, there are gender differences in the way that runaway girls and boys respond to or interact with their parents when under stress. Girls may be more likely to internalize stress when there is aggression in the family environment. Boys may tend to display depressive symptoms when their parents have higher depressive symptoms. However, due to the cross-sectional design of this study, causal interpretations about family interaction patterns cannot be concluded. More research is needed to examine the dynamic relationship between runaway youth and their parents.
In addition, the current study revealed that girls in more cohesive families were less likely to be depressed. Given that family cohesion refers to a feeling of togetherness and connectedness in the family (Vandewater & Lansford, 2005), it is possible that girls utilize the family to help them cope with distress. However, there were no protective factors associated with boys’ depressive symptoms. Possibly, boys utilize other protective factors which are external to the family, including alternative social resources (prosocial peers, adult mentors), which were not assessed in the current study.
Finally, contrary to previous research (Unger et al., 1998), task-oriented coping skills were not associated with depressive symptoms for girls or boys. This finding was surprising because several researchers define resilience among runaway and homeless youth primarily through the active coping strategies that they utilize (Bender, Thompson, McManus, Lantry, & Flynn, 2007; Kidd & Carroll, 2007; Kidd & Shahar, 2008). However, the current study’s findings suggest that the immediate social environment, in particular, the family environment, might be more salient to runaway youth than are other factors when understanding depressive symptoms.
Test of Resiliency Models
This study provided support for the challenge model, but not for the compensatory or risk-protective models of resiliency. Support for the challenge model revealed that runaway girls and boys were least likely to be depressed when the cumulative risks within the family system, such as parental verbal aggression, parental depression, and family conflict, were in the moderate range, rather than in the severe range. These results indicate that the levels of risk factors, rather than the availability of protective factors, were associated with runaway adolescents’ depressive symptoms.
Support for the challenge model of resiliency is controversial because this model asserts that a moderate level of risk is functional. Few studies to date have tested and found support for this model of resiliency (Christiansen & Evans, 2005; Gomez & McLaren, 2006; Holister-Wagner, Foshee, & Jackson, 2001; McLaren, Gomez, Bailey, & Van Der Horst, 2007). In addition, prior research found gender differences in the challenge model of resiliency in which girls, compared to boys, were more resilient to aggression (Holister-Wagner, Foshee, & Jackson, 2001), victimization (Christiansen & Evans, 2005), and anxiety/depression (Gomez & McLaren, 2006) at moderate levels of risk. However, these studies relied on samples recruited from either high schools or universities and these youth were exposed to wide range risk and protective factors. Therefore, the present findings for the challenge model of resiliency in a specific sample of high risk, substance abusing runaway youth is striking. The challenge model appears to work for both samples; however the perceived ‘risk’ for runaways is different from the perceived ‘risk’ for normative samples. Possibly, runaway youth of verbally abusive, conflictual, and distressed families develop specific skills to cope with these adverse conditions (as long as their parents were not severely abusive or clinically depressed). Consequently, this risk itself may have provided an “opportunity” for the runaways to resist depressive symptoms effectively. Therefore, the current study revealed that at least in regards to depressive symptoms, runaway youth functioned relatively well, even if protective factors were not available or adequate in their family context.
Furthermore, the challenge model of resiliency to depression among runaways can be interpreted according to recent findings of strength-based qualitative studies on homeless youth. Consistent with the challenge model, qualitative studies suggest that youth who are victimized and neglected by their parents develop strategies for survival and acquire “street smarts.” These youth successfully identify those they can trust and request assistance from, differentiating them from those who are exploitative (Bender, Thompson, McManus, Lantry, & Flynn, 2007; Lindsey, Kurtz, Jarvis, Williams, & Nackerud, 2000). Similarly, some runaways may develop the social competence to master depression and the stress in their lives as long as the risks are not extreme.
Prevention researchers have focused on either reducing risk factors or increasing protective factors to promote positive youth development (Catalano et al., 2001). However, the current study suggests that risks, at least in this sample, are not necessarily ‘negative;’ rather, the functioning of risk is complex and depends not only on the presence of risk, but also on how risks relate to other risks. The intensity, or level of risk, is also crucial to consider when implementing prevention and treatment strategies for runaway youth.
Limitations
Several limitations of the current study need to be considered when evaluating the findings. First, the current study used a cross sectional design but a longitudinal design would offer the ability to assess how relationships among risk and protective factors change over time (Garmezy, Masten, & Tellegen, 1984). Also, the current study focused on resilience only at the family and individual level and did not assess resilience across different systems. Evaluation of resilience among runaway youth at the community and societal levels would provide a more comprehensive view, but was beyond the scope of the current study.
Second, the present study utilized measures whose norms were not established for this population. Although measures of verbal aggression (CTS), and family conflict (FES) show excellent reliability and validity for normative and clinical samples (Moos & Moos, 1986; Straus, 1979), these scales had low reliability coefficients for the current sample. However, they were included in the analysis for theoretical reasons even though measurement error may have biased the current findings. Furthermore, the statistical analysis relied on creating composite scores to examine the cumulative effects of risk and protective factors. This strategy inevitably results in the loss of information regarding the effects of each individual variable (Fraser, Richman, & Galinsky, 1999). Each risk and protective factor was given an equal weight in contributing to the outcome when risk and protective indexes were computed. However, there is no consensus in the resiliency literature for utilizing a specific statistical procedure (Masten, 2001). To address this problem, full models that included all risk and protective factors were run before the cumulative risk and protective factors were tested in relation to resiliency. This strategy was utilized to clarify the results and validate interpretation of the findings.
Finally, the extant literature on resilience does not provide an agreed upon operationalization and measurement of adolescent resilience (Fraser, Richman, & Galinsky, 1999; Masten, 2001). In addition to that, resiliency, by definition, is a context-specific phenomenon that makes it difficult to operationalize, analyze and evaluate for research (Luthar, Cicchetti, & Becker, 2000). One common problem is that findings across studies differ due to the definitions of risk and protective factors.
Conclusions and Future Directions
Despite these limitations, the current study is unique in its focus on resilience to depression among at-risk youth. To our knowledge, this is the first study that attempts to systematically conceptualize, operationalize and test resiliency models among runaway adolescents. Findings provide support for the challenge model of resiliency which is controversial in terms of implications for interventions because it suggests that some level of risk may be positive, beneficial, and functional.
Another contribution is that the present study used a more balanced approach which considered both the strengths and risks inherent in the family. This approach is preferable to problem-oriented research which ignores context and labels the population as deviant and deficient. Instead, this study captures the available protective mechanisms within the family system of substance abusing runaway youth in relation to depressive symptoms. Even though at-risk families are ‘vulnerable’ to experiencing higher levels of depressive symptoms, successful coping mechanisms are also present within these family contexts.
Implications for practice
Taking into account the findings of the current study, several implications for preventive interventions and family therapy can be offered. Given the potentially protective role of family cohesion on girls’ depressive symptoms, interventions that enhance connectedness, belonging, and support in the family context might be particularly effective for girls. Preventative programs and family therapy should target building capacity and competence among family members which might then promote resilience to distress.
Despite the possible resources in families, some runaways may be at higher risk of severe abuse and neglect in their families than others, and protective mechanisms in the family context may be limited. Specific interventions for these high risk adolescents should be designed and implemented by applying the challenge model of resiliency. This model suggests that these youth may have the potential to ‘borrow strength from the risk’ in their lives. Thus, therapy approaches should explore adolescents’ areas of competence and survival skills while also giving them room to tell their painful stories of stress and victimization (Bender, Thompson, McManus, Lantry, & Flynn, 2007).
Finally, it is important to note that researchers, mental health professionals, and service providers need to be cautious about not falling for the “myth of the golden child” – runaway youth and their families are not superhuman beings (Beauvais & Oetting, 1999). Every environment, including the family context of runaways, consists of a complex array of potential risks, dangers, assets, and protections. Researchers and mental health professionals should strive to consider both the strengths and risks that runaway youth face as they pursue research and intervention efforts with this population. While the relationship between risk and protective factors on behavior is complex, the focus on one without the other provides a one dimensional perspective of multidimensional phenomena.
Acknowledgments
This work was supported by the National Institute on Drug Abuse, grant R01 DA 013549.
Contributor Information
Gizem Erdem, Department of Human Development and Family Science, The Ohio State University.
Natasha Slesnick, Department of Human Development and Family Science, The Ohio State University.
References
- Beauvais F, Oetting ER. Drug use, resilience, and the myth of the golden child. In: Johnson JL, editor. Resilience and development: Positive life adaptations. New York: Kluwer Academic/Plenum Press; 1999. pp. 101–107. [Google Scholar]
- Bousman CA, Blumberg EJ, Shillington AM, Hovell MF, Ji M, Lehman S, Clapp J. Predictors of substance use among homeless youth in San Diego. Addictive Behaviors. 2005;30:1100–1110. doi: 10.1016/j.addbeh.2004.10.006. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK. BDI-II, Beck Depression Inventory: Manual. 2. Boston, MA: Harcourt Brace; 1996. [Google Scholar]
- Bender K, Thompson SJ, McManus H, Lantry J, Flynn PM. Capacity for Survival: Exploring Strengths of Homeless Street Youth. Child and Youth Care Forum. 2007;36:25–42. doi: 10.1007/s10566-006-9029-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Billings A, Moos R. Psychosocial theory and research on depression: An integrative framework and review. Clinical Psychology Review. 1982;2:213–237. [Google Scholar]
- Catalano RF, Hawkins JD, Berglund ML, Pollard JA, Arthur MW. Prevention science and positive youth development: Competitive or cooperative frameworks? Journal of Adolescent Health. 2001;31:230–239. doi: 10.1016/s1054-139x(02)00496-2. [DOI] [PubMed] [Google Scholar]
- Chen X, Thrane L, Whitbeck LB, Johnson K. Mental Disorders, Comorbidity, and Postrunaway Arrests Among Homeless and Runaway Adolescents. Journal of Research on Adolescence. 2006;16:379–402. [Google Scholar]
- Christiansen EJ, Evans WP. Adolescent Victimization Testing Models of Resiliency by Gender. Journal of Early Adolescence. 2005;25:298–316. [Google Scholar]
- Cohen J, Cohen P. Applied multiple regression-correlation analysis for the behavioral sciences. Hillsdale, NJ: L Erlbaum Associates; 1983. [Google Scholar]
- Compas BE, Connor-Smith J, Jaser SS. Temperament, Stress Reactivity, and Coping: Implications for Depression in Childhood and Adolescence. Journal of Clinical Child & Adolescent Psychology. 2004;33:21–31. doi: 10.1207/S15374424JCCP3301_3. [DOI] [PubMed] [Google Scholar]
- de Man AF. Predictors of adolescent running away behavior. Social Behavior and Personality. 2000;28:261–268. [Google Scholar]
- Endler NS, Parker JDA. Coping Inventory for Stressful Situations(CISS): Manual. Multi-Health Systems; Toronto: 1990. [Google Scholar]
- Fergus S, Zimmerman MA. Adolescent Resilience: A Framework for Understanding Healthy Development in the Face of Risk. Annual Review of Public Health. 2005;26:399–419. doi: 10.1146/annurev.publhealth.26.021304.144357. [DOI] [PubMed] [Google Scholar]
- Fraser M, Richman J, Galinsky M. Risk, protection, and resilience: Toward a conceptual framework for social work practice. Social Work Research. 1999;23:131–144. [Google Scholar]
- Garmezy N, Masten AS, Tellegen A. The study of stress and competence in children: A building block for developmental psychopathology. Child Development. 1984;55:97–111. [PubMed] [Google Scholar]
- Gomez R, McLaren S. The association of avoidance coping style, and perceived mother and father support with anxiety/depression among late adolescents: Applicability of resiliency models. Personality and IndividualDifferences. 2006;40:1165–1176. [Google Scholar]
- Hollister-Wagner GH, Foshee VA, Jackson C. Adolescent aggression: Models of resiliency. Journal of Applied Social Psychology. 2001;31:445–466. [Google Scholar]
- Hyde J. From home to street: Understanding young people’s transitions into homelessness. Journal of Adolescence. 2005;28:171–183. doi: 10.1016/j.adolescence.2005.02.001. [DOI] [PubMed] [Google Scholar]
- Kamieniecki G. Prevalence of psychological distress and psychiatric disorders among homeless youth in Australia: a comparative review. Australian and New Zealand Journal of Psychiatry. 2001;35:352–358. doi: 10.1046/j.1440-1614.2001.00910.x. [DOI] [PubMed] [Google Scholar]
- Kidd SA. Factors Precipitating Suicidality among Homeless Youth: A Quantitative Follow-Up. Youth & Society. 2006;37:393–422. [Google Scholar]
- Kidd SA, Carroll MR. Coping and suicidality among homeless youth. Journal of Adolescence. 2007;30:283–296. doi: 10.1016/j.adolescence.2006.03.002. [DOI] [PubMed] [Google Scholar]
- Kidd SA, Shahar G. Resilience in homeless youth: the key role of self-esteem. American Journal of Orthopsychiatry. 2008;78:163–172. doi: 10.1037/0002-9432.78.2.163. [DOI] [PubMed] [Google Scholar]
- Kumpfer KL, Alvarado R. Family strengthening approaches for the prevention of youth problem behaviors. American Psychologist. 2003;58:457–465. doi: 10.1037/0003-066X.58.6-7.457. [DOI] [PubMed] [Google Scholar]
- Lindsey EW, Kurtz D, Jarvis S, Williams NR, Nackerud L. How runaways and homeless youth navigate troubled waters: Personal strengths and resources. Child and Adolescent Social Work Journal. 2000;17:115–140. [Google Scholar]
- Luthar SS, Cicchetti D, Becker B. The construct of resilience: A critical evaluation and guidelines for future work. Child Development. 2000;71:543–562. doi: 10.1111/1467-8624.00164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS. Ordinary Magic: Resilience Processes in Development. American Psychologist. 2001;56:227–238. doi: 10.1037//0003-066x.56.3.227. [DOI] [PubMed] [Google Scholar]
- McLaren S, Gomez R, Bailey M, Van Der Horst RK. The association of depression and sense of belonging with suicidal ideation among older adults: Applicability of resiliency models. Suicide and Life-Threatening Behavior. 2007;37:89–102. doi: 10.1521/suli.2007.37.1.89. [DOI] [PubMed] [Google Scholar]
- Moos RH, Moos BS. Family Environment Scale manual. Palo Alto, CA: Consulting Psychologists Press; 1986. [Google Scholar]
- National Coalition for the Homeless. Fact Sheet #5: Mental Illness and Homelessness. 2006 Available at http://www.nationalhomeless.org/publications/facts/Mental_Illness.html.
- Nyamathi AM, Christiani A, Windokun F, Jones T, Strehlow A, Shoptaw S. Hepatitis C virus infection, substance use and mental illness among homeless youth: a review. AIDS. 2005;19(3):34–40. doi: 10.1097/01.aids.0000192068.88195.27. [DOI] [PubMed] [Google Scholar]
- Patel DR, Greydanus DE. Homeless Adolescents in the United States: An Overview for Pediatricians. International Pediatrics. 2002;17:71–75. [Google Scholar]
- Pollard JA, Hawkins JD, Arthur MW. Risk and protection: Are both necessary to understand diverse behavioral outcomes in adolescence? Social Work Research. 1999;23:145–158. [Google Scholar]
- Reinherz HZ, Paradis AD, Giaconia RM, Stashwich CK, Fitzmaurice G. Childhood and adolescent predictors of major depression in the transition to adulthood. American Journal of Psychiatry. 2003;160:2141–2147. doi: 10.1176/appi.ajp.160.12.2141. [DOI] [PubMed] [Google Scholar]
- Sander JB, McCarty CA. Youth Depression in the Family Context: Familial Risk Factors and Models of Treatment. Clinical Child and Family Psychology Review. 2005;8:203–219. doi: 10.1007/s10567-005-6666-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaffer D. The Diagnostic Interview Schedule for Children -2.3 Version. New York: Columbia University; 1992. [Google Scholar]
- Sheeber L, Hops H, Davis B. Family processes in adolescent depression. Clinical Child & Family Psychology Review. 2001;4:19–35. doi: 10.1023/a:1009524626436. [DOI] [PubMed] [Google Scholar]
- Son AJ. Information Packet: Runaway and homeless youth. New York, NY: Hunter College School of Social Work, National Resource Center for Foster Care and Permanency Planning; 2002. [Google Scholar]
- Straus MA. Measuring intrafamily conflict and violence: The Conflict Tactics (CT) Scales. Journal of Marriage & the Family. 1979;41:75–88. [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Office of Applied Studies. Results from the 2002 National Survey on Drug Use and Health: National findings. Rockville, MD: 2003. [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Office of Applied Studies. Results from the 2004 National Survey on Drug Use and Health: National findings. Rockville, MD: 2005. [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Office of Applied Studies. The NSDUH Report: State Estimates of Depression: 2004 and 2005. Rockville, MD: 2007. [Google Scholar]
- Thompson SJ, Maguin E, Pollio DE. National and regional differences among runaway youth using federally-funded crisis services. Journal of Social Service Research. 2003;30:1–17. [Google Scholar]
- Thrane LE, Hoyt DR, Whitbeck LB, Yoder KA. Impact of family abuse on running away, deviance, and street victimization among homeless rural and urban youth. Child Abuse. 2006;30:1117–1128. doi: 10.1016/j.chiabu.2006.03.008. [DOI] [PubMed] [Google Scholar]
- Vandewater EA, Lansford JE. A family process model of problem behaviors in adolescents. Journal of Marriage and Family. 2005;67:100–109. [Google Scholar]
- Van Voorhees BW, Paunesku D, Gollan J, Kuwabara S, Reinecke M, Basu A. Predicting future risk of depressive episode in adolescents: The Chicago Adolescent Depression Risk Assessment (CADRA) Annals of Family Medicine. 2008;6:503–511. doi: 10.1370/afm.887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Votta E, Manion IG. Factors in the psychological adjustment of homeless adolescent males: the role of coping style. Journal of the American Academy of Child and Adolescent Psychiatry. 2003;42:778–785. doi: 10.1097/01.CHI.0000046871.56865.D9. [DOI] [PubMed] [Google Scholar]
- Weissman MM, Jensen P. What research suggests for depressed women with children. The Journal of Clinical Psychiatry. 2002;63:641–647. doi: 10.4088/jcp.v63n0717. [DOI] [PubMed] [Google Scholar]
- Werner E, Smith R. Journeys from childhood to the midlife: Risk, resilience, and recovery. New York: Cornell University Press; 2001. [Google Scholar]
- Whitbeck LB, Hoyt DR. Nowhere to grow: Homeless and runaway adolescents and their families. Hawthorne, NY: Aldine de Gruyter; 1999. [Google Scholar]
- Whitbeck LB, Hoyt DR, Bao W. depressive symptoms and co-occurring depressive symptoms, substance abuse, and conduct problems among runaway and homeless adolescents. Child Development. 2000;71:721–732. doi: 10.1111/1467-8624.00181. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Johnson KD, Hoyt DR, Cauce AM. Mental disorder and comorbidity among runaway and homeless adolescents. Journal of Adolescent Health. 2004;35:132–140. doi: 10.1016/j.jadohealth.2003.08.011. [DOI] [PubMed] [Google Scholar]
- Yoder KA. Comparing suicide attempters, suicide ideators, and nonsuicidal homeless and runaway adolescents. Suicide and Life-Threatening Behavior. 1999;29:25–36. [PubMed] [Google Scholar]
- Zimmerman MA, Arunkumar R. Resiliency research: Implications for schools and policy. Society for Research in Child Development. 1994;8:1–19. [Google Scholar]