

Abstract
Background
Life-threatening infections are a major cause of death after allogeneic stem cell transplantation. Complement Mannose-binding lectin is a key component of innate immunity. Functional deficiency of mannose-binding lectin due to genetic polymorphism is frequent. Previous reports showed conflicting results with respect to the influence of functional mannose-binding lectin deficiency on infectious risk after allogeneic stem cell transplantation. The aim of this study was to clarify the impact of low mannose-binding lectin levels on infectious risk in a unique cohort of very long-term survivors after stem cell transplantation.
Design and Methods
Incidence of major infections was evaluable in 43 out of 44 very long-term survivors (over ten years) and studied retrospectively in relation to mannose-binding lectin serum concentrations.
Results
Recipients with mannose-binding lectin levels below 1,000 ng/mL were at increased risk to suffer from one or more major infections (P=0.002) during entire follow up. Infectious susceptibility was increased after neutrophil recovery, particularly until 24 months (Hazard Ratio 3.4) with sustained effects afterwards (Hazard Ratio 2.9). Mannose-binding lectin serum concentrations below 1,000 ng/mL were independently associated with major infections after neutrophil recovery (P=0.009). In subgroup analyses occurrence of severe herpes virus infections in particular was associated with significantly lower mannose-binding lectin levels (P=0.02).
Conclusions
Our findings indicate that low mannose-binding lectin levels may predict markedly increased susceptibility to severe infections with sustained effects even late after allogeneic stem cell transplantation. Determinations of mannose-binding lectin status should therefore be included into pre-transplantation risk assessment.
Keywords: stem cell transplantation, MBL levels, life-threatening infections
Introduction
Complement mannose-binding lectin (MBL), a member of the collectin subfamily of C-type lectins, is a key component of innate immunity.1 As a multimeric complex complement MBL is capable of recognizing carbohydrate pathogen-associated molecular patterns on a wide range of microorganisms leading to complement activation in an antibody and C1q independent manner.2,3 Functional MBL deficiency, which is probably the most common immunodeficiency, affects up to one-third of the Caucasian population and is characterized by low levels of circulating functional multimers due to a number of genetic polymorphisms within the coding and promoter regions of the MBL2 gene.4 In spite of a strong correlation between MBL genotypes and serum MBL levels,5–7 people with the same genotype may differ up to 10-fold in functionally active MBL levels,8,9 which is the major determinant of the activity of the MBL pathway.10,11 MBL serum levels are mainly influenced by genetics, whereas environmental factors have only marginal effects.12 Even during acute inflammation, MBL serum concentrations are predictive for moderate to severe deficiency.8,13,14
Evidence from several studies of the last 20 years supports a strong association between MBL deficiency and the risk of infections, particularly when adaptive immunity is either immature or compromised (e.g. during early childhood15–17 or after solid organ transplantation18–20).
The risk of severe infections in patients with functional MBL deficiency undergoing allogeneic stem cell transplantation (SCT) has been investigated in six recent studies.14,21–25 All but two studies could demonstrate an increased risk of severe infections in patients with either low MBL levels or low-producing genotype.22–25 However, the definition of functional MBL deficiency and infectious endpoints was heterogeneous and median follow-up time since allogeneic stem cell transplantation limited to two years or less. Therefore, there are few data available about the importance of MBL deficiency during different early and late time periods after transplantation. Infectious complications represent an important cause of non-relapse morbidity and mortality even more than ten years after allogeneic stem cell transplantation.26,27 Extensive chronic graft-versus-host disease (GVHD), cytomegalovirus (CMV) status, unrelated donor transplantation, irradiation in conditioning regimen and age have been established as important risk factors for late infections,28–30 but there are no objective parameters to define a dysfunction of the immune system in long-term survivors. Therefore, we investigated the association between serum MBL levels and the occurrence of severe infections during different periods after transplantation in a single center cross-sectional study of a unique cohort of very long-term survivors.
Design and Methods
Patients and donors
In a single-center, cross sectional study, 44 very long-term survivors (over ten years) who underwent allogeneic stem cell transplantation from 1980 to 1996 at the University Hospital of Basel and their respective HLA-identical sibling donors were evaluated in pairs on the same day by performing a complete clinical and biological examination. All sibling donor-recipient pairs whose recipient had a follow up of over ten years since allogeneic stem cell transplantation, was in complete remission at the last follow up, and who both agreed to attend our outpatient transplant clinic on the same day were invited. Of the 82 pairs of recipients and donors contacted, eventually 44 agreed to take part. Some of the results of this cohort have been previously described elsewhere.31 Clinical data were obtained by review of patients’ charts since stem cell transplantation until study entry (September 2005–May 2007). One donor-recipient pair was excluded because of a lack of comprehensive follow-up information. Comprehensive clinical data (consisting of clinical notes, laboratory and microbiological results, reports of radiological and histological examinations, and discharge summaries from our and other hospitals, reports from primary care physicians, and reports of all visits to our outpatient Stem Cell Transplantation Clinic) were available for 43 recipients who all had a regular follow up after transplantation at our institution. The clinical data was analyzed blinded to any MBL concentration data.
The study had been approved by the local ethical committee at the University Hospital of Basel.
Definitions of endpoints
Infectious endpoints were classified according to previously published criteria.22,24,30 Major infection was predefined as either sepsis confirmed on microbiological testing or as systemic inflammatory response syndrome (SIRS) with highly suggestive radiographic or clinical features. Moreover, specific antimicrobial treatment had to be initiated in both cases. The following conditions were excluded: single positive blood culture results for skin contaminant bacteria, upper respiratory tract infections, culture-negative interstitial pneumonitis (i.e. infiltrates on chest X-ray or computed tomography scan without documented infection in bronchoalveolar lavage culture or on histological examination), culture-negative fever in neutropenia, dermatological varicella zoster reactivation, and local herpes simplex reactivation. Severe herpes virus infection was predefined as invasive viral infections requiring prompt treatment and hospitalization. In detail, we recorded episodes of generalized varicella zoster infections, herpes simplex infections with organ involvement (e.g. pneumonitis, encephalitis, generalized skin infection), Epstein-Barr virus associated post-transplant lymphoproliferative disorder, and cytomegalovirus infections/reactivation deemed clinically significant and requiring treatment. A positive cytomegalovirus blood culture or CMV-pp65 antigenemia assay and symptoms or organ dysfunction were required to fulfill the criteria of a clinically significant cytomegalovirus infection/reactivation. Episodes of asymptomatic cytomegalovirus reactivation, primary varicella zoster virus and Epstein-Barr virus infections were excluded.
Mannose-binding lectin level analysis
Serum samples from all donors and recipients were collected between 2005 and 2007 and stored at −70°C. Quantification of functional MBL was performed by an investigator blinded to any recipient data using a commercially available Sandwich-ELISA Kit (MBL Oligomer ELISA KIT 029, Lucerna Chem, Luzern, Switzerland) as described previously.18 Primarily, functional MBL deficiency was defined as serum levels below 1,000 ng/mL as this cut-off has been shown to discriminate reasonably well between individuals with or without variant MBL genotypes.5,6,9 In addition, this cut-off has been shown to be associated with serious infections in oncological and intensive care unit patients.32,33 A secondary analysis was performed in order to better define the most relevant cut-off for the definition of functional MBL deficiency to predict the risk of infection in the setting of allogeneic stem cell transplantation.
Statistical analysis
Differences in recipients’ characteristics according to MBL serostatus were analyzed using the Fisher’s exact test or the Mann-Whitney-U-Test where appropriate. Serum MBL levels in recipients with or without infection were compared using a Mann-Whitney-U-test. Cumulative incidences of major infections and severe herpes virus infections according to MBL serum levels were calculated by the Kaplan-Meier test and compared by the log rank test. For cumulative incidences, only the first event occurring in a patient was considered. Cox’s proportional hazard models were used to estimate the effect of MBL levels on predefined endpoints in multivariate analyses after adjustment for covariables. Covariables included recipient age at transplantation, sex, diagnosis, history of total body irradiation, history of splenic irradiation or splenectomy, acute graft-versus-host disease (no/grade I vs. grades II-IV), chronic graft-versus-host disease, and duration of immunosuppression. Multiple events occurring in the same patient were considered in Cox’s models.
Results
Donors’ and recipients’ characteristics
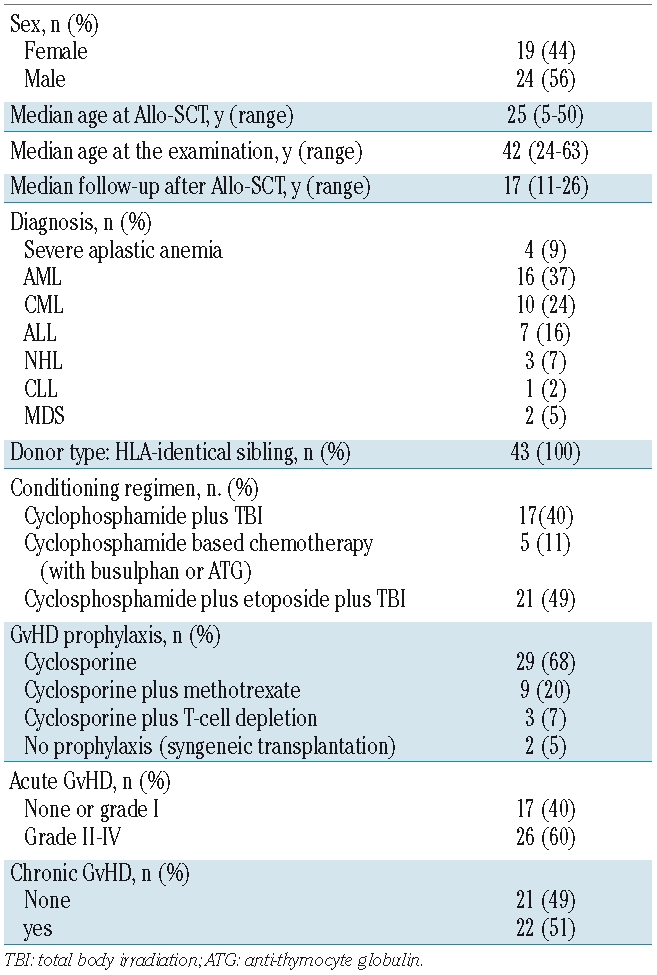
All donor-recipient pairs were of Caucasian origin. Bone marrow was the source of stem cells in all recipients with a median number of 4.2 (range 0.3–16.6)×108/kg body weight nucleated cells. Performance status demonstrated that 80 of 86 (93%) participants had a Karnofsky Score of 100%, reflecting the overall good clinical condition of both recipients and donors at the time of study. Recipients’ characteristics of this allogeneic stem cell transplantation cohort are summarized in Table 1.
Table 1.
Recipient’s characteristics.
Mannose-binding lectin serum levels
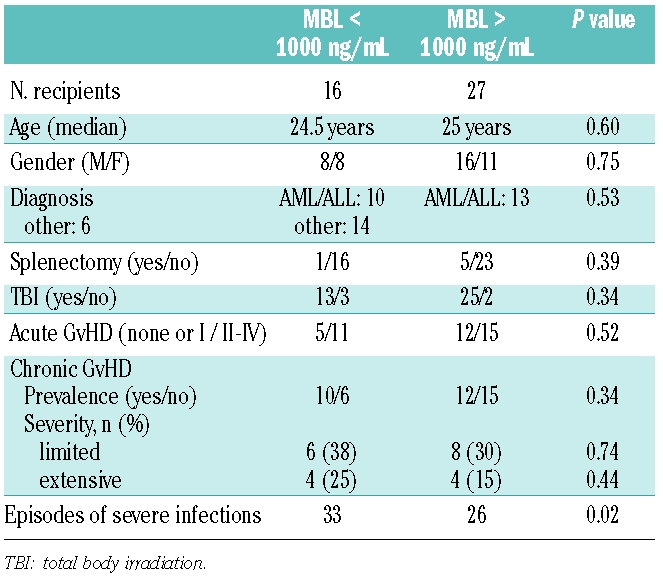
The donor and the recipient cohort consisted of 17 of 43 (39.5%) and 16 of 43 (37%) individuals with MBL levels below 1,000 ng/mL, respectively, including 6 individuals with levels below 100 ng/mL (14%) in each cohort, thereby closely resembling frequency distributions observed in the general population.4,34 With the exception of one recipient with severe MBL deficiency, none of the donors or recipients displayed significant laboratory signs of systemic inflammation or infections at the time of analysis. Patients with MBL levels below 1,000 ng/mL did not differ significantly from patients with MBL levels above 1,000 ng/mL with regard to age, sex, diagnosis, history of splenectomy or acute graft-versus-host disease, presence or history of chronic graft-versus-host disease, and history of total body irradiation as part of conditioning regimen (Table 2). We also did not observe significant differences between the two recipient groups with respect to common parameters of immune reconstitution (number of peripheral blood CD4+CD3+, CD8+CD3 and CD25+/Foxp3+ T cells and CD19+ B cells, as well as serum IgM, IgA, IgG and IgG subclass concentrations; data not shown).
Table 2.
Comparison of recipient’s characteristics according to mannose-binding lectin serostatus.
Recipients and infections
Twenty-eight recipients experienced at least one major infection during follow up. Half of them suffered from more than one episode of severe infection resulting in a total number of 59 infectious episodes. Pneumonia and gram positive sepsis were encountered most frequently (23 and 16 episodes, respectively). In contrast gram-negative sepsis and fungal infections were diagnosed rarely (3 and 2 episodes, respectively). With respect to severe viral infections, recipients experienced 12 episodes of severe herpes virus infections consisting mainly of cytomegalovirus infections/reactivations (10 episodes). More than 50% of recipients with MBL below 1,000 ng/mL suffered from 2 or more episodes of severe infections (4 of 16 individuals with one severe infection; 7 of 16 with 2 or 3; 2 of 16 with more than 3) in contrast to only 5 of 27 (19%) recipients with MBL above 1,000 ng/mL (10 of 27 individuals with one severe infection; 3 of 27 with 2 or 3; 2 of 27 with more than 3). The median time to the first episode was 32.5 days (range 3–2,682 days).
Associations with major infections
During the whole follow-up period, 13 of 16 (81%) recipients with low MBL levels, i.e. below 1,000 ng/mL, experienced at least one major infection compared to 15 of 27 (56%) recipients with high MBL concentrations, i.e. above 1,000 ng/mL. This difference did not reach statistical significance (P=0.2; Figure 1A). However, as many recipients suffered from more than one major infection during follow up, we studied the occurrence of all major infectious episodes in a Cox’s regression model. In this analysis, the presence of MBL levels below 1,000 ng/mL was associated with a 2.3-fold increased risk of major infections during the whole study period (Hazard Ratio (HR) 2.25, 95% CI 1.3–3.8; P=0.002).
Figure 1.
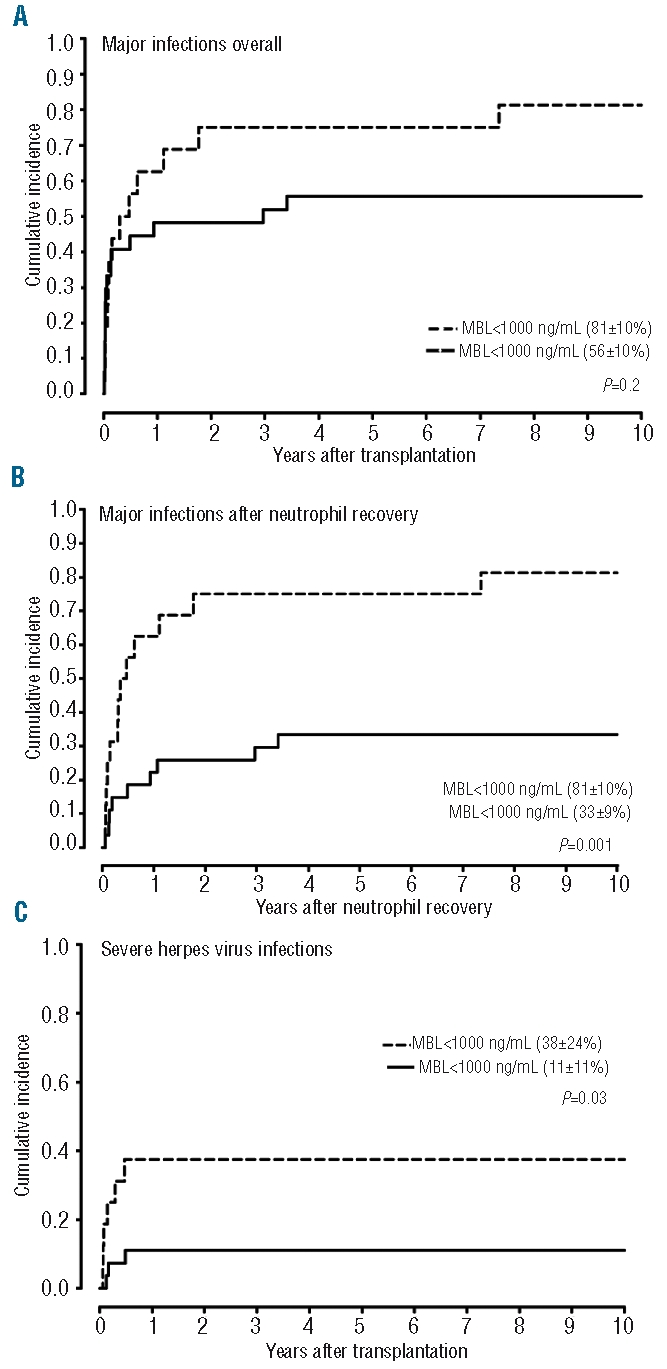
Association of functional MBL deficiency (MBL < 1000 ng/mL) with major infections after allogeneic SCT. (A and B) Cumulative incidences of major infections according to MBL serostatus during entire follow up and after neutrophil recovery. (C) Cumulative incidences of severe herpes virus infections according to MBL serostatus during entire study period.
After stratification of infective episodes as occurring before or after neutrophil recovery, a striking association between low MBL levels and major infections after but not prior to neutrophil recovery could be observed. The cumulative incidence of at least one major infection at ten years after engraftment was 81% in MBL deficient recipients compared to 33% in MBL sufficient recipients (P=0.001; Figure 1B). Including all major infective episodes into analysis, recipients with low MBL levels were subject to a more than 3-fold increased risk of major infections compared to recipients with MBL above 1,000 ng/mL (HR 3.2, 95% CI 1.7–5.9; P<0.001). In contrast, MBL levels below 1,000 ng/mL were not related to major infections during initial neutropenia (HR 0.56, 95% CI 0.12–2.5; P=0.5) and there was no association between MBL levels and the number of episodes or the duration of neutropenic fever, respectively.
Risk of major infections during different time intervals after stem cell transplantation
Since complete immune reconstitution may be delayed for years35,36 and thus may confer a risk factor for serious infections even late after allogeneic stem cell transplantation, we evaluated the impact of functional MBL deficiency over different time periods after transplantation (Figure 2). Recipients with low MBL levels were at highest risk to suffer from major infective episodes seven to 24 months after neutrophil recovery (HR 4.2, 95% CI 1.3–13.5; P=0.015). But even during the remaining very long follow-up period (median 15 years), we could continuously observe an increased susceptibility of MBL deficient recipients to major infections (HR 2.9, 95% CI 1.1–8.0; P=0.04) with almost 30% of events occurring after 24 months.
Figure 2.
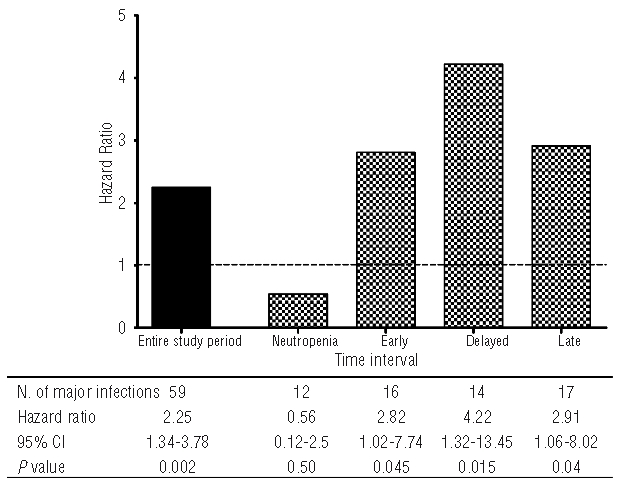
Association of low mannose-binding lectin levels with major infections during different time intervals. The reference category (horizontal dashed line) corresponds to recipients with mannose-binding lectin > 1,000 ng/mL. Neutropenia: transplantation until engraftment; early: engraftment until six months after transplantation; delayed: seven months until two years after transplantation; late: more than two years after transplantation.
Associations with severe herpes virus infections
Since MBL might play an important role in the defense against cytomegalovirus and other herpes virus infections after transplantation,18,25,37,38 we examined the association between MBL levels and herpes virus infections in more detail. Apart from localized varicella zoster infections, the frequency of severe herpes virus infections was low during the entire follow up. Nevertheless, a significant and independent association between low MBL serum concentrations and the occurrence of severe herpes virus infections could be observed. During follow up, 6 of 16 (38%) recipients with MBL levels below 1,000 ng/mL suffered from 9 episodes compared to 3 of 27 (11%) patients with MBL levels above 1,000 ng/mL with 3 episodes altogether (P=0.03; Figure 1C). On the contrary low MBL levels were not a risk factor for localized varicella zoster infections (P=0.90).
Association of major infections in dependence of serum mannose-binding lectin levels
In order to better define the clinically most relevant cutoff for deficient versus sufficient MBL levels, the occurrence of major infections and severe herpes virus infections was correlated to serum MBL levels (Figure 3). Consistent with data on the cumulative incidence, recipients with at least one episode of major infection after neutropenia showed significantly lower MBL serum concentrations than patients without major infections, while there was only a trend to lower MBL levels considering the entire follow up. Moreover, we observed a significant difference in MBL levels with respect to the occurrence of severe herpes virus infections during the entire follow up.
Figure 3.
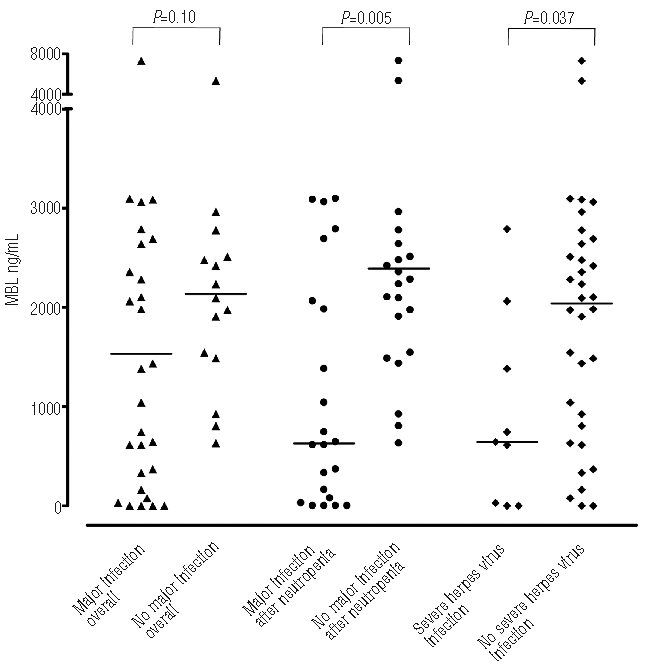
Differences in mannose-binding lectin serum levels according to occurrence of infections (yes or no) after allogeneic stem cell transplantation. Horizontal lines represent medians.
Since the definition of functional MBL deficiency was likely to be dependent on the clinical setting, different cutoffs for the distinction between deficient and sufficient serum MBL levels were examined by establishing a Receiver Operating Characteristic (ROC) curve including the whole follow-up period. In our opinion, the best threshold to distinguish between deficient and sufficient serum MBL levels was found to be 500 ng/mL showing a sensitivity of 40% and a specificity of 100% as a prognostic parameter for major infections overall. With this threshold the cumulative incidence of major infections was significantly increased in recipients with MBL below 500 ng/mL even when analyzing the entire study period (P=0.025; Figure 4A). Notably, every recipient with MBL serum concentrations below 500 ng/mL had at least one major infective episode during follow up. After exclusion of the initial time to neutrophil recovery this association became even more pronounced (Figure 4B).
Figure 4.
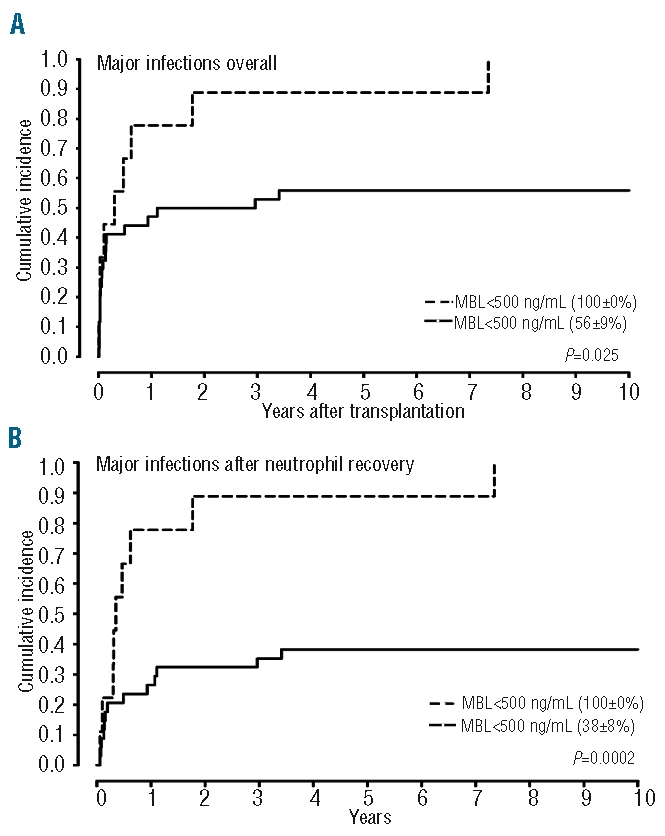
Association of very low mannose-binding lectin levels (<500 ng/mL) with the incidence of major infections according to follow up intervals. (A) Entire follow-up. (B) Period after initial neutrophil recovery.
Analysis of potential confounders
To assess the impact of possible confounders on the association between low MBL levels and major infections a multivariate analysis by Cox’s proportional hazard models was performed. Recipient MBL serum concentrations below 1,000 ng/mL were an independent risk factor for major infections after neutrophil recovery (Likelihood Ratio (LR) 3.5, 95% CI 1.3–8.9; P=0.009). Analyzing the lower threshold of 500 ng/mL, the independent prognostic value was retained even during the entire study period (LR 6.8, 95% CI 2.2–20.4; P=0.001). All other covariables were not significantly associated with major infections in this analysis with older age at transplantation (per year; LR 1.05, 95% CI 0.99–1.1; P=0.11) and extensive chronic graft-versus-host disease (LR 3.0, 95% CI 0.89–10.5; P=0.08) showing a trend towards an increased risk of major infections.
In our retrospective analysis, a selection bias due to early death might have influenced the association between low MBL levels and major infections, especially during the early phase after transplantation. In an attempt to reduce this potential confounder, we analyzed the association of low MBL levels on the incidence of major infections excluding all events which occurred during the first six months after transplantation. Limiting the analyses to this period (i.e. delayed and late infections) we could still observe a striking association between low MBL levels and major infections: 9 of 16 (56%) recipients with MBL levels below 1,000 ng/mL experienced at least one major infection compared to 7 of 27 (26%) recipients with high MBL concentrations (P=0.017). Including in the analysis all major infective episodes occurring during this period resulted in a more than 3-fold increased risk of major infections in MBL deficient recipients compared to recipients with MBL above 1,000 ng/mL (HR 3.4, 95% CI 1.6–7.3; P=0.001). However, as only 2 episodes of severe herpes virus infections occurred seven months or more after transplantation we could not demonstrate an increased risk for recipients with low MBL levels after exclusion of the early period after transplantation.
Association with donor mannose-binding lectin levels
Only 5 of the 43 donor-recipient pairs (11.6 %) showed a mismatch in MBL serostatus when applying the pre-specified threshold of 1,000 ng/mL. In 3 of these pairs the recipient had MBL levels above 1,000 ng/ml and a corresponding donor with MBL levels below 1,000 ng/mL. None of these recipients suffered from a major infective episode during follow up suggesting that donor MBL level did not influence the risk for major infections.
Discussion
In this report on a unique cohort of very long-term survivors we could demonstrate that low serum MBL levels are a strong independent risk factor for severe infections early and late after allogeneic stem cell transplantation. This finding is of importance since severe infections are still a major cause of morbidity and mortality after this type of transplant.26
Previous studies on the role of complement MBL in patients after allogeneic stem cell transplantation demonstrated conflicting results irrespective of the chosen definition of functional MBL deficiency.14,21–25 Recently, Neth et al. for the first time found an association of low MBL levels and severe infections in patients after allogeneic stem cell transplantation.25 In contrast to this study and our results the occurrence of major infections was not related to low MBL levels in the studies presented by Mullighan et al. and Chaudhry et al.14,24 However, besides differences in patients’ characteristics (e.g. pediatric patients14) and MBL cut-offs used for the definition of functional MBL deficiency, the short follow-up period of only 100 days in both studies may have been important for the discrepancy in results. During our much longer follow up of at least 11 years, we could observe that functional MBL deficiency continues to denote a higher susceptibility to major infections even more than two years after transplantation whereas we could not observe such an association during the initial time period between transplantation and neutrophil recovery.
On average, MBL deficient recipients were subject to a more than 3-fold increased risk to suffer from major infection after recovery from neutropenia. This observation is in line with previous studies22,24 and supports the view that the MBL pathway of complement alone is not sufficient to prevent serious infections during the neutropenic phase after transplantation. As soon as cellular recovery after allogeneic stem cell transplantation begins, sufficient MBL levels might be crucial for defeating certain bacteria, for example by optimizing phagocytic function.39 The relevance of serum MBL levels is strengthened by the observation that at the time of analysis recipients with low MBL and those with high levels did not differ in common parameters of immune reconstitution (peripheral blood CD4+CD3+, CD8+CD3, CD25+/Foxp3+ T cells and CD19+ B cells, as well as serum IgM, IgA, IgG and IgG subclass concentrations).
Taking into account that functionally sufficient MBL levels might be strongly dependent on the type of infection or the clinical situation, we further tried to define the optimal MBL cut-off level predicting the risk of infections after allogeneic stem cell transplantation. We found that a cut-off of 500 ng/mL might be clinically helpful for the identification of patients with functional MBL deficiency and an increased risk of infections after allogeneic stem cell transplantation. This cut-off is in line with those used in previous studies18,40,41 and leads to an even more striking association of low MBL levels with severe infections during follow up including the initial neutropenic episode.
There are limited and conflicting data on the association of MBL deficiency with viral infections after allogeneic stem cell transplantation.14,25 In our cohort, low MBL levels were associated with a markedly increased incidence of severe herpes virus infections. However, due to the low number of episodes and a lack of information on the donor and recipient cytomegalovirus serostatus, larger prospective studies are warranted to fully evaluate the impact of MBL deficiency on the occurrence of severe herpes virus infections.
The present study has some limitations. Besides the retrospective design, the recipient cohort was small and included only patients surviving more than ten years. Due to early mortality of recipients with unknown MBL serostatus, our results could have been influenced by considerable selection bias. However, limiting our analysis to infections occurring after the first six months after hematopoietic stem cell transplantation, we still observed a striking association of low serum MBL levels with the risk of major infections.
At first sight, the fact that MBL2 genotypes were not determined could appear as a limitation. However, MBL serum levels show little variation throughout life. In particular, recipient MBL levels are not influenced by donor genotypes after allogeneic stem cell transplantation.25,42 Therefore measurement of MBL serum levels by ELISA allows reliable quantification of the functional acitivity of the MBL pathway in vivo11 and identification of low-producing MBL2 genotypes after allogeneic stem cell transplantation. When evaluating associations with diseases, measurement of MBL serum levels might in fact represent a more sensitive approach than determination of genotypes, as individuals with the same genotype may vary up to 10-fold in MBL serum levels.5,8,9
In conclusion, recipient MBL serum levels were strongly associated with susceptibility to major bacterial and viral infections after neutrophil recovery during early, delayed and late follow up in this cohort of very long-term survivors after allogeneic stem cell transplantation. Due to the prolonged risk of recipients with low MBL, adaption of infectious prophylaxis and early treatment in patients at risk seem more promising than replacement therapy with recombinant human MBL. Therefore, determination of the MBL serostatus should be considered an infectious risk marker to be included in pre-transplantation risk assessment. Additional prospective trials with adequate follow up are warranted to further evaluate the importance of MBL with respect to viral and bacterial infections after allogeneic stem cell transplantation.
Footnotes
Funding: this work was supported by a SCORE fellowship (N. 3232B0-107248/2) and a grant (N. 3200B0-118176) from the Swiss National Foundation and the Werner Geissberger Foundation.
Authorship and Disclosures
MO and MT were the principal investigators and take primary responsibility for the paper. MT designed the study. MO collected and analyzed data and wrote the article. AR, AG, and AT recruited the patients and collected data. DD performed the laboratory work for this study. MS participated in the statistical analysis. AR, DD, MS, AG, AT, and MT revised the article and gave final approval.
The authors reported no potential conflicts of interest.
References
- 1.Bouwman LH, Roep BO, Roos A. Mannose-binding lectin: clinical implications for infection, transplantation, and autoimmunity. Hum Immunol. 2006;67(4–5):247–56. doi: 10.1016/j.humimm.2006.02.030. [DOI] [PubMed] [Google Scholar]
- 2.Lu JH, Thiel S, Wiedemann H, Timpl R, Reid KB. Binding of the pentamer/hexamer forms of mannan-binding protein to zymosan activates the proenzyme C1r2C1s2 complex, of the classical pathway of complement, without involvement of C1q. J Immunol. 1990;144(6):2287–94. [PubMed] [Google Scholar]
- 3.Neth O, Jack DL, Dodds AW, Holzel H, Klein NJ, Turner MW. Mannose-binding lectin binds to a range of clinically relevant microorganisms and promotes complement deposition. Infect Immun. 2000;68(2):688–93. doi: 10.1128/iai.68.2.688-693.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Garred P, Larsen F, Seyfarth J, Fujita R, Madsen HO. Mannose-binding lectin and its genetic variants. Genes Immun. 2006;7(2):85–94. doi: 10.1038/sj.gene.6364283. [DOI] [PubMed] [Google Scholar]
- 5.Garred P, Larsen F, Madsen HO, Koch C. Mannose-binding lectin deficiency--revisited. Mol Immunol. 2003;40(2–4):73–84. doi: 10.1016/s0161-5890(03)00104-4. [DOI] [PubMed] [Google Scholar]
- 6.Steffensen R, Thiel S, Varming K, Jersild C, Jensenius JC. Detection of structural gene mutations and promoter polymorphisms in the mannan-binding lectin (MBL) gene by polymerase chain reaction with sequence-specific primers. J Immunol Methods. 2000;241(1–2):33–42. doi: 10.1016/s0022-1759(00)00198-8. [DOI] [PubMed] [Google Scholar]
- 7.Eisen DP, Dean MM, Boermeester MA, Fidler KJ, Gordon AC, Kronborg G, et al. Low serum mannose-binding lectin level increases the risk of death due to pneumococcal infection. Clin Infect Dis. 2008;47(4):510–6. doi: 10.1086/590006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Herpers BL, Endeman H, de Jong BA, de Jongh BM, Grutters JC, Biesma DH, et al. Acute-phase responsiveness of mannose-binding lectin in community-acquired pneumonia is highly dependent upon MBL2 genotypes. Clin Exp Immunol. 2009;156(3):488–94. doi: 10.1111/j.1365-2249.2009.03929.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fidler KJ, Wilson P, Davies JC, Turner MW, Peters MJ, Klein NJ. Increased incidence and severity of the systemic inflammatory response syndrome in patients deficient in mannose-binding lectin. Intensive Care Med. 2004;30(7):1438–45. doi: 10.1007/s00134-004-2303-8. [DOI] [PubMed] [Google Scholar]
- 10.Roos A, Garred P, Wildenberg ME, Lynch NJ, Munoz JR, Zuiverloon TC, et al. Antibody-mediated activation of the classical pathway of complement may compensate for mannose-binding lectin deficiency. Eur J Immunol. 2004;34(9):2589–98. doi: 10.1002/eji.200324401. [DOI] [PubMed] [Google Scholar]
- 11.Petersen SV, Thiel S, Jensen L, Steffensen R, Jensenius JC. An assay for the mannan-binding lectin pathway of complement activation. J Immunol Methods. 2001;257(1–2):107–16. doi: 10.1016/s0022-1759(01)00453-7. [DOI] [PubMed] [Google Scholar]
- 12.Ytting H, Christensen IJ, Thiel S, Jensenius JC, Svendsen MN, Nielsen L, et al. Biological variation in circulating levels of mannan-binding lectin (MBL) and MBL-associated serine protease-2 and the influence of age, gender and physical exercise. Scand J Immunol. 2007;66(4):458–64. doi: 10.1111/j.1365-3083.2007.01991.x. [DOI] [PubMed] [Google Scholar]
- 13.Thiel S, Holmskov U, Hviid L, Laursen SB, Jensenius JC. The concentration of the C-type lectin, mannan-binding protein, in human plasma increases during an acute phase response. Clin Exp Immunol. 1992;90(1):31–5. doi: 10.1111/j.1365-2249.1992.tb05827.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chaudhry SH, Chaudhry S, Jansen-Hoogendijk AM, Jol van der Zijde CM, van Tol MJ, Roos A, et al. Mannose-binding lectin levels and infections in children after allogeneic hematopoietic SCT. Bone Marrow Transplant. 2010;45(2):289–93. doi: 10.1038/bmt.2009.159. [DOI] [PubMed] [Google Scholar]
- 15.Koch A, Melbye M, Sorensen P, Homoe P, Madsen HO, Molbak K, et al. Acute respiratory tract infections and mannose-binding lectin insufficiency during early childhood. Jama. 2001;285(10):1316–21. doi: 10.1001/jama.285.10.1316. [DOI] [PubMed] [Google Scholar]
- 16.Cedzynski M, Szemraj J, Swierzko AS, Bak-Romaniszyn L, Banasik M, Zeman K, et al. Mannan-binding lectin insufficiency in children with recurrent infections of the respiratory system. Clin Exp Immunol. 2004;136(2):304–11. doi: 10.1111/j.1365-2249.2004.02453.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.de Benedetti F, Auriti C, D’Urbano LE, Ronchetti MP, Rava L, Tozzi A, et al. Low serum levels of mannose binding lectin are a risk factor for neonatal sepsis. Pediatr Res. 2007;61(3):325–8. doi: 10.1203/pdr.0b013e318030d12f. [DOI] [PubMed] [Google Scholar]
- 18.Manuel O, Pascual M, Trendelenburg M, Meylan PR. Association between mannose-binding lectin deficiency and cytomegalovirus infection after kidney transplantation. Transplantation. 2007;83(3):359–62. doi: 10.1097/01.tp.0000251721.90688.c2. [DOI] [PubMed] [Google Scholar]
- 19.Worthley DL, Johnson DF, Eisen DP, Dean MM, Heatley SL, Tung JP, et al. Donor mannose-binding lectin deficiency increases the likelihood of clinically significant infection after liver transplantation. Clin Infect Dis. 2009;48(4):410–7. doi: 10.1086/596313. [DOI] [PubMed] [Google Scholar]
- 20.Verschuren JJ, Roos A, Schaapherder AF, Mallat MJ, Daha MR, de Fijter JW, et al. Infectious complications after simultaneous pancreas-kidney transplantation: a role for the lectin pathway of complement activation. Transplantation. 2008;85(1):75–80. doi: 10.1097/01.tp.0000297249.10654.f5. [DOI] [PubMed] [Google Scholar]
- 21.Rocha V, Franco RF, Porcher R, Bittencourt H, Silva WA, Jr, Latouche A, et al. Host defense and inflammatory gene polymorphisms are associated with outcomes after HLA-identical sibling bone marrow transplantation. Blood. 2002;100(12):3908–18. doi: 10.1182/blood-2002-04-1033. [DOI] [PubMed] [Google Scholar]
- 22.Mullighan CG, Heatley S, Doherty K, Szabo F, Grigg A, Hughes TP, et al. Mannose-binding lectin gene polymorphisms are associated with major infection following allogeneic hemopoietic stem cell transplantation. Blood. 2002;99(10):3524–9. doi: 10.1182/blood.v99.10.3524. [DOI] [PubMed] [Google Scholar]
- 23.Granell M, Urbano-Ispizua A, Suarez B, Rovira M, Fernandez-Aviles F, Martinez C, et al. Mannan-binding lectin pathway deficiencies and invasive fungal infections following allogeneic stem cell transplantation. Exp Hematol. 2006;34(10):1435–41. doi: 10.1016/j.exphem.2006.06.005. [DOI] [PubMed] [Google Scholar]
- 24.Mullighan CG, Heatley SL, Danner S, Dean MM, Doherty K, Hahn U, et al. Mannose-binding lectin status is associated with risk of major infection following myeloablative sibling allogeneic hematopoietic stem cell transplantation. Blood. 2008;112(5):2120–8. doi: 10.1182/blood-2007-07-100222. [DOI] [PubMed] [Google Scholar]
- 25.Neth OW, Bacher U, Das P, Zabelina T, Kabisch H, Kroeger N, et al. Influence of mannose-binding lectin genotypes and serostatus in Allo-SCT: analysis of 131 recipients and donors. Bone Marrow Transplant. 2010;45(1):13–9. doi: 10.1038/bmt.2009.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gratwohl A, Brand R, Frassoni F, Rocha V, Niederwieser D, Reusser P, et al. Cause of death after allogeneic haematopoietic stem cell transplantation (HSCT) in early leukaemias: an EBMT analysis of lethal infectious complications and changes over calendar time. Bone Marrow Transplant. 2005;36(9):757–69. doi: 10.1038/sj.bmt.1705140. [DOI] [PubMed] [Google Scholar]
- 27.Socie G, Stone JV, Wingard JR, Weisdorf D, Henslee-Downey PJ, Bredeson C, et al. Long-term survival and late deaths after allogeneic bone marrow transplantation. Late Effects Working Committee of the International Bone Marrow Transplant Registry. N Engl J Med. 1999;341(1):14–21. doi: 10.1056/NEJM199907013410103. [DOI] [PubMed] [Google Scholar]
- 28.Robin M, Porcher R, De Castro Araujo R, de Latour RP, Devergie A, Rocha V, et al. Risk factors for late infections after allogeneic hematopoietic stem cell transplantation from a matched related donor. Biol Blood Marrow Transplant. 2007;13(11):1304–12. doi: 10.1016/j.bbmt.2007.07.007. [DOI] [PubMed] [Google Scholar]
- 29.Bjorklund A, Aschan J, Labopin M, Remberger M, Ringden O, Winiarski J, et al. Risk factors for fatal infectious complications developing late after allogeneic stem cell transplantation. Bone Marrow Transplant. 2007;40(11):1055–62. doi: 10.1038/sj.bmt.1705856. [DOI] [PubMed] [Google Scholar]
- 30.Ochs L, Shu XO, Miller J, Enright H, Wagner J, Filipovich A, et al. Late infections after allogeneic bone marrow transplantations: comparison of incidence in related and unrelated donor transplant recipients. Blood. 1995;86(10):3979–86. [PubMed] [Google Scholar]
- 31.Baerlocher GM, Rovo A, Muller A, Matthey S, Stern M, Halter J, et al. Cellular senescence of white blood cells in very long-term survivors after allogeneic hematopoietic stem cell transplantation: the role of chronic graft-versus-host disease and female donor sex. Blood. 2009;114(1):219–22. doi: 10.1182/blood-2009-03-209833. [DOI] [PubMed] [Google Scholar]
- 32.Gordon AC, Waheed U, Hansen TK, Hitman GA, Garrard CS, Turner MW, et al. Mannose-binding lectin polymorphisms in severe sepsis: relationship to levels, incidence, and outcome. Shock. 2006;25(1):88–93. doi: 10.1097/01.shk.0000186928.57109.8d. [DOI] [PubMed] [Google Scholar]
- 33.Neth O, Hann I, Turner MW, Klein NJ. Deficiency of mannose-binding lectin and burden of infection in children with malignancy: a prospective study. Lancet. 2001;358(9282):614–8. doi: 10.1016/S0140-6736(01)05776-2. [DOI] [PubMed] [Google Scholar]
- 34.Gadjeva M, Takahashi K, Thiel S. Mannan-binding lectin--a soluble pattern recognition molecule. Mol Immunol. 2004;41(2–3):113–21. doi: 10.1016/j.molimm.2004.03.015. [DOI] [PubMed] [Google Scholar]
- 35.Fujimaki K, Maruta A, Yoshida M, Kodama F, Matsuzaki M, Fujisawa S, et al. Immune reconstitution assessed during five years after allogeneic bone marrow transplantation. Bone Marrow Transplant. 2001;27(12):1275–81. doi: 10.1038/sj.bmt.1703056. [DOI] [PubMed] [Google Scholar]
- 36.Martinez C, Urbano-Ispizua A, Rovira M, Carreras E, Rozman C, Montserrat E. Immune reconstitution following allogeneic peripheral blood progenitor cell transplantation. Leuk Lymphoma. 2000;37(5–6):535–42. doi: 10.3109/10428190009058505. [DOI] [PubMed] [Google Scholar]
- 37.Ghods FJ, Solgi G, Amirzargar AA, Nikbin B, Ghods AJ. High frequency of clinically significant infections and cytomegalovirus disease in kidney transplant recipients with serum mannose-binding lectin deficiency. Iran J Kidney Dis. 2009;3(1):28–33. [PubMed] [Google Scholar]
- 38.Cervera C, Lozano F, Saval N, Gimferrer I, Ibanez A, Suarez B, et al. The influence of innate immunity gene receptors polymorphisms in renal transplant infections. Transplantation. 2007;83(11):1493–500. doi: 10.1097/01.tp.0000264999.71318.2b. [DOI] [PubMed] [Google Scholar]
- 39.Neth O, Jack DL, Johnson M, Klein NJ, Turner MW. Enhancement of complement activation and opsonophagocytosis by complexes of mannose-binding lectin with mannose-binding lectin-associated serine protease after binding to Staphylococcus aureus. J Immunol. 2002;169(8):4430–6. doi: 10.4049/jimmunol.169.8.4430. [DOI] [PubMed] [Google Scholar]
- 40.Vekemans M, Robinson J, Georgala A, Heymans C, Muanza F, Paesmans M, et al. Low mannose-binding lectin concentration is associated with severe infection in patients with hematological cancer who are undergoing chemotherapy. Clin Infect Dis. 2007;44(12):1593–601. doi: 10.1086/518171. [DOI] [PubMed] [Google Scholar]
- 41.Peterslund NA, Koch C, Jensenius JC, Thiel S. Association between deficiency of mannose-binding lectin and severe infections after chemotherapy. Lancet. 2001;358 (9282):637–8. doi: 10.1016/S0140-6736(01)05785-3. [DOI] [PubMed] [Google Scholar]
- 42.Kilpatrick DC, Stewart K, Allan EK, McLintock LA, Holyoake TL, Turner ML. Successful haemopoietic stem cell transplantation does not correct mannan-binding lectin deficiency. Bone Marrow Transplant. 2005;35(2):179–81. doi: 10.1038/sj.bmt.1704746. [DOI] [PubMed] [Google Scholar]