

Abstract
Crouch gait, one of the most prevalent movement abnormalities among children with cerebral palsy, is frequently treated with surgical lengthening of the hamstrings. To assist in surgical planning many clinical centers use musculoskeletal modeling to help determine if a patient's hamstrings are shorter or lengthen more slowly than during unimpaired gait. However, some subjects with crouch gait walk slowly, and gait speed may affect peak hamstring lengths and lengthening velocities. The purpose of this study was to evaluate the effects of walking speed on hamstrings lengths and velocities in a group of unimpaired subjects over a large range of speeds and to determine if evaluating subjects with crouch gait using speed matched controls alters subjects' characterization as having “short” or “slow” hamstrings. We examined 39 unimpaired subjects who walked at five different speeds. These subjects served as speed-matched controls for comparison to 74 subjects with cerebral palsy who walked in crouch gait. Our analysis revealed that peak hamstrings length and peak lengthening velocity in unimpaired subjects increased significantly with increasing walking speed. Fewer subjects with cerebral palsy were categorized as having hamstrings that were “short” (31/74) or “slow” (38/74) using a speed-matched control protocol compared to a non-speed-matched protocol (35/74 “short”, 47/74 “slow”). Evaluation of patients with cerebral palsy using speed-matched controls alters and may improve selection of patients for hamstrings lengthening procedures.
Introduction
Crouch gait is one of the most prevalent pathological walking patterns among children with cerebral palsy (CP). It is characterized by excessive knee flexion during the terminal swing and stance phases of the gait cycle. Hamstrings dysfunction, including spasticity or contracture (Baumann, et al., 1980; Sutherland and Davids, 1993), is thought to cause excessive knee flexion in some cases, and surgical lengthening of the hamstrings, in combination with other procedures, is commonly performed to treat crouch gait.
Surgical lengthening of contracted hamstrings is thought to improve knee extension by slackening the stretched muscle fibers and decreasing the passive tension in the muscles (Delp and Zajac, 1992). However, the outcome for patients who undergo hamstrings lengthening is variable and difficult to predict. Previous studies have attempted to address this difficulty by categorizing patients on the basis of preoperative gait kinematics and comparing postoperative changes in knee, hip, and pelvis angles during walking (Abel, et al., 1999; DeLuca, et al., 1998; Kay, et al., 2002; Novacheck, et al., 2002). Other studies have used gait kinematics together with musculoskeletal modeling to determine which subjects with crouch gait have hamstrings that are shorter than normal or lengthen more slowly than during gait of typically developing children (Arnold, et al., 2001; Arnold, et al., 2006; Delp, et al., 1996; Hoffinger, et al., 1993; Schutte, et al., 1997; van der Krogt, et al., 2007). Analyses of muscle-tendon lengths and velocities have been used to help distinguish individuals who have “short” or “slow” hamstrings from those who do not, which may help identify patients who are at risk for unsatisfactory postsurgical changes (Arnold, et al., 2006).
In many cases, the decision to surgically lengthen the hamstrings is made after comparison of the patient's joint kinematics, joint moments, and muscle-tendon lengths with those of typically developing subjects walking at their self-selected speeds. Children with crouch gait may walk more slowly than typically developing children, and this may affect hamstring muscle-tendon length and lengthening velocity. Joint kinematics are affected by walking speed (Schwartz, et al., 2008), and hamstrings lengths and velocities depend on joint kinematics and on the muscle's moment arms about both the hip and knee. A study of 8 typically developing subjects walking in voluntary crouch gait revealed that these subjects did not have reduced hamstring muscle-tendon lengths or lengthening velocities compared to measurements during normal gait (van der Krogt, et al., 2007). Decreasing walking speed in these typically developing subjects reduced peak hamstring lengths and lengthening velocities (van der Krogt, et al., 2007). It has also been shown in a group of 11 typically developing subjects walking at three different speeds that hamstrings lengths and velocities increase with walking speed (van der Krogt, et al., 2009). These findings highlight the interaction between walking speed, muscle length, and muscle velocities, and suggest alternative explanations for the apparent shortness/slowness of muscles observed in subjects with CP who walk in crouch gait.
The present study examines whether changes in walking speed affect peak muscle-tendon lengths and lengthening velocities of the hamstrings during walking in a group of 39 typically developing subjects walking at five different speeds. We also analyzed the gait kinematics and muscle-tendon lengths of 74 subjects with CP and crouch gait. These analyses enabled us to answer the following questions.
Is the peak hamstrings length at a slow walking speed significantly different from peak length at free and fast walking speeds in typically developing subjects?
Is the peak hamstrings lengthening velocity at a slow walking speed significantly different from peak velocity at free and fast walking speeds in typically developing subjects?
What fraction of subjects with crouch gait walk more slowly than typically developing subjects?
Does evaluation of subjects with crouch gait compared to speed matched control subjects alter the characterization of patients as having “short” or “slow” hamstrings?
Methods
To examine the effect of walking speed on hamstrings lengths and velocities, motion capture data were collected for 83 typically developing subjects (Schwartz, et al., 2008). Of these 83 subjects, 39 had at least one trial in each of five speed groups (very slow, slow, free, fast, very fast); only these 39 typically developing subjects were included in this study. These 39 subjects had a mean height of 1.36 m, mean mass of 32.9 kg, and a mean age of 8.8 years. Walking speed from each trial was normalized using nondimensional walking velocity (ν*) defined as:
Where ν is absolute walking velocity, Lleg is leg length, and g is gravitational acceleration (Hof, 1996). The normalized speed was used to categorize trials into speed groups, which was done post-hoc as follows:
where and are the mean and standard deviation, respectively, of the nondimensional free walking speeds of the 39 typically developing subjects. If more than one trial for a particular speed group existed for one subject, the trial for analysis was randomly selected. All joint kinematics from motion capture trials were normalized to 100% gait cycle before analysis, and only the right leg was analyzed.
Joint kinematics from each of the 39 subjects were applied to a three-dimensional musculoskeletal model of the lower extremity that is based on the geometry of an average-sized adult male (Arnold, et al., 2001). Kinematic constraints to represent the hip and knee joints were included in the musculoskeletal model (Delp et al., 1990) to reduce errors that arise from soft tissue artifact (Lu and O'Connor, 1999). The model was used to calculate semimembranosus muscle-tendon lengths for a complete gait cycle. Previous studies have shown that semimembranosus lengths are representative of medial hamstrings lengths due to similarity in length changes of the semimembranosus and semitendinosus during walking (Schutte, et al., 1997). Previous studies also have shown that normalized lengths of the medial hamstrings estimated with the generic model used here were not systematically longer or shorter than the lengths calculated with MR-based models of individual subjects (Arnold, et al., 2001). Muscle-tendon lengthening velocities were approximated for each subject at each of the five speeds by numerical differentiation of muscle-tendon lengths using finite differences with three-point estimation. The muscle-tendon lengths and lengthening velocities at each point in the gait cycle for each speed were averaged across the 39 typically developing subjects. Also, for each speed category, the mean and standard deviation of the peak muscle-tendon lengths and peak lengthening velocities were computed for the typically developing subjects. All of the muscle-tendon length values were normalized to the peak mean muscle-tendon length at free walking speed (0.44 m), and all muscle-tendon lengthening velocity values were normalized to the peak mean lengthening velocity at free walking speed (0.30 m/s).
Repeated measures analysis of variance was conducted to determine whether walking speed had a significant effect on peak muscle-tendon length and lengthening velocity. Post-hoc paired t-tests with a Bonferroni correction were used to analyze the differences between mean peak values for muscle-tendon lengths and lengthening velocities in each speed category (α = 0.01).
Muscle-tendon lengths and velocities were also calculated for 74 subjects with CP who walked in a crouch gait. Motion capture data were collected in the same gait analysis laboratory as for the control group. The kinematic data for the subjects with crouch gait, walking at their self selected walking speed, were part of the data reported by Arnold, et al. (2006). All subjects had been diagnosed with spastic CP, were able to walk without assistance, had not undergone surgery, and received a gait analyses as part of their routine medical care. Of the 74 subjects with CP, 23 were diagnosed with hemiplegia, 33 with diplegia, 12 with triplegia, and 6 with quadriplegia. Subjects were 6 years of age or older with a mean age of 10 years, mean height of 129.7 cm, mean weight of 30.5 kg, and had at least 20° of knee flexion in one or both limbs at initial contact (averaged over 0-4% of the gait cycle) or terminal swing (averaged over 96-100% of the gait cycle). Subjects were excluded if botulinum toxin had been injected into the hamstrings, psoas, or adductors 6 months prior to the gait analysis, had received a selective dorsal rhizotomy or a neurectomy, or were on baclofen. The semimembranosus muscle-tendon lengths and lengthening velocities for each subject with crouch gait were calculated for the right leg using the same analysis described for the typically developing subjects. All subjects gave informed consent for the collection of their gait data. Institutional review board approval was obtained for retrospective analysis of the data.
The peak hamstrings length and peak velocity for each subject with crouch gait were compared to the typically developing subjects' mean peak hamstrings length and velocity at free walking speed. A CP subject's hamstrings were categorized as “short” and/or “slow” if the muscle's length and/or velocity was at least two standard deviations less than the mean for the typically developing subjects. Next, each subject with crouch gait was assigned to one of the five speed categories based on his or her nondimensional walking speed during the motion capture trial. Then the peak muscle-tendon length and lengthening velocity for each subject with crouch gait was compared to the mean for the typically developing subjects' in the matched speed group. Subjects with crouch gait were classified as “short” and/or “slow” based on this speed-matched comparison. Differences were recorded in the number of subjects categorized as “slow”, “short”, “both short and slow”, or “neither short nor slow” between the non-speed-matched and speed-matched evaluations.
The difference between the mean nondimensional walking speed for the 39 typically developing subjects at free speed and the mean nondimensional walking speed for the subjects with crouch gait was analyzed using an unpaired t-test (α = 0.05).
Results
The peak muscle-tendon length of the typically developing subjects occurred at approximately 95% of the gait cycle and the peak lengthening velocity at approximately 80% of the gait cycle, regardless of walking speed (Figure 1). As walking speed increased, mean peak hamstrings length and mean peak hamstrings lengthening velocity increased in typically developing subjects (Figure 2). The mean peak hamstring length and mean peak hamstring lengthening velocity for each speed group was found to be significantly different from the mean peaks of neighboring speed groups (p<0.01).
Figure 1.
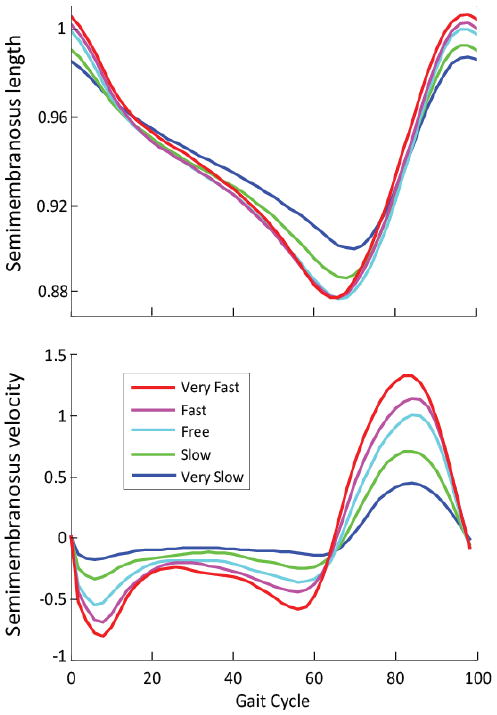
Mean semimembranosus muscle-tendon lengths (top) and velocities (bottom) vs. gait cycle for 39 unimpaired subjects at five speeds. Muscle-tendon lengths are normalized to the peak semimembranosus length at free speed. Velocities are normalized to the peak semimembranosus velocity at free speed.
Figure 2.
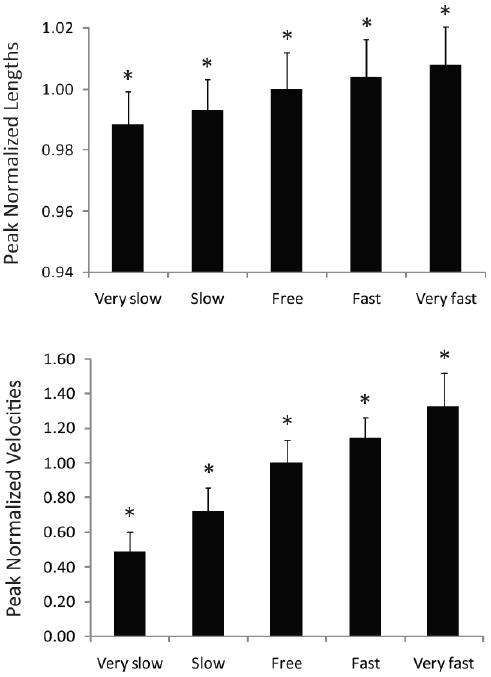
Mean peak semimembranosus muscle-tendon lengths (top) and velocities (bottom) for each speed. Mean peak muscle-tendon length and lengthening velocity increased between each walking speed. Error bars show one standard deviation. The * indicates that the mean is significantly different (p < 0.01) from neighboring means. Peak muscle-tendon lengths are normalized to the peak semimembranosus length at free speed. Peak velocities are normalized to the peak semimembranosus velocity at free speed.
Analysis of the CP group revealed differences in walking speed compared to the control group (Figure 3). Mean nondimensional walking speed for the CP group at free speed (0.40±0.11) was significantly slower (p=0.006) than the mean nondimensional walking speed for the control group (0.44±0.04). Of the 74 subjects with crouch gait, 38 walked within one standard deviation of the mean speed for the typically developing subjects. There were 25 subjects with crouch gait who walked more than one standard deviation slower than the mean free speed of the typically developing subjects, and 11 subjects who walked more than one standard deviation faster than the mean free speed of the typically developing subjects.
Figure 3.

Nondimensional walking speeds of crouch gait subjects. Number of subjects with crouch gait who walked at very slow (4), slow (21), free (38), fast (10), and very fast (1) speeds. Mean walking speed of 39 unimpaired subjects at free speed was 0.44±0.04, compared to the mean walking speed for subjects with crouch gait at 0.40±0.11. Note that the majority of subjects with crouch gait (47/74) walked slower than the mean unimpaired free speed.
Interpretation of muscle-tendon lengths and velocities for the subjects with crouch gait differed depending on whether or not a speed-matched control was used (Figure 4). After speed-matching the proportion of subjects with hamstrings categorized as “neither short nor slow” increased from 26% (19 subjects) to 35% (26 subjects), while the proportion of subjects evaluated as having “both short and slow” hamstrings decreased from 36% (27 subjects) to 28% (21 subjects). About a third of the CP group (23/74) had different classification of their hamstrings lengths or lengthening velocities using speed-matching. Categorization changed for two subjects from “short” to “neither”, for five subjects from “slow” to “neither”, for eight subjects from “both” to “short”, for two subjects from “both” to “neither”, for two subjects from “neither” to “slow”, and for four subjects from “short” to “both”.
Figure 4.
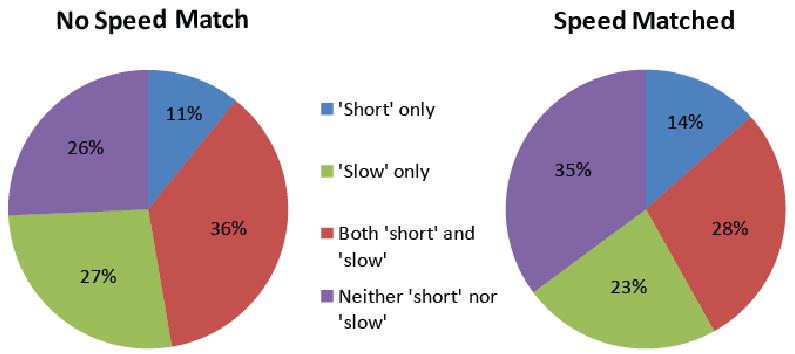
Categorization of peak semimembranosus muscle-tendon lengths and lengthening velocities for 74 subjects with cerebral palsy who walked with crouch gait. Categorization was conducted without speed-matched controls (left) and with speed-matched controls (right).
Discussion
Several studies have suggested that examination of hamstrings lengths during walking may help determine which subjects with crouch gait have hamstrings that are shorter than normal or lengthen more slowly than during gait of typically developing children (Arnold, et al., 2001; Arnold, et al., 2006; Delp, et al., 1996; Hoffinger, et al., 1993; Schutte, et al., 1997; van der Krogt, et al., 2007). Our results support the findings of van der Krogt et al. (2009) who reported systematic increases in hamstring peak muscle-tendon length and peak lengthening velocity with increasing walking speed. Our results also demonstrate that the classification of a subject as having hamstrings that are “short” or “slow” depends, in some cases, on whether or not the subject with crouch gait is compared to typically developing subjects walking at the same speed.
Some subjects with crouch gait walked more slowly than the typically developing free speed (Figure 3). This suggests the need to investigate the value of a speed-matched control when assessing patients with crouch gait, especially for more severely affected subjects who walk very slowly.
Results of our non-speed-matched analysis were compared to Arnold et al. (2006), in which a different control population and a larger CP subject group were studied. The proportions of subjects whose muscles were categorized without speed matching as “short”, “slow”, or neither “short” nor “slow” differed from the results of Arnold et al. (2006), who reported 35% of subjects with crouch gait had hamstrings classified as “short” (vs. 47% in the current study), 57% were classified as “slow” (vs. 47%), and 35% were neither “short” nor “slow” (vs. 26%). The differences in the proportions between categories can partly be attributed to differences in the control subject pools. In this study, the mean peak hamstrings length at free speed for the control subjects (0.437±0.005 m) was higher than the mean peak length calculated by Arnold et al. (2006) (0.433±0.004 m). Also, the mean peak hamstrings lengthening velocity in this study (0.29±0.039 m/s) was slightly faster than the mean lengthening velocity from Arnold et al. (0.27±0.037 m/s), likely due to differing walking speeds. The sensitivity of the categorization of the CP subjects to walking speed of the control group suggests the need for speed matching.
Some limitations of this study should be considered. First, due to the sensitivity of the results to the control sample, further work may be warranted to develop a larger control group. Second, possible errors in the measured joint motions arising from soft tissue artifacts (Oberhofer, et al., 2009) may lead to errors in calculated muscle-tendon lengths and velocities. Changes in hamstrings lengths arise primarily from hip and knee flexion-extension (Delp, et al., 1996). Motion of these degrees of freedom is relatively large compared to other degrees of freedom, such as hip rotation and hip adduction, which are more difficult to estimate. Errors in muscle-tendon lengths and velocities that arise from soft tissue artifact can be reduced with a musculoskeletal model (Lu and O'Connor, 1999) that includes kinematic constraints to represent the hip and knee joints (Delp, et al., 1990), as we have done here.
A smaller number of subjects were categorized as having “short” or “slow” muscles using a speed-matched protocol. If applied to a clinical setting, use of a speed-matched protocol for evaluation of patients with crouch gait might result in fewer patients being deemed appropriate candidates for hamstrings lengthening procedures. However, it is important to note that this study does not address the impact that neuromuscular pathology may have on walking speed. It is possible that hamstring contractures or spasticity may cause a reduction in walking speed, thereby allowing the muscle to function at shorter lengths or at slower lengthening velocities. This would be masked by comparing the subject to a speed-matched control, which may categorize the muscle as operating at an appropriate length or velocity given a slow walking speed.
Further research must be done to help determine whether a patient's reduced walking speed is caused by hamstrings pathology or other impairments. Many factors may contribute to crouch gait including short or spastic hamstrings (DeLuca, et al., 1998; Gage, 1990), spastic hip flexors (Reimers, 1973; Roosth, 1971), weak knee extensors (Beals, 2001), weak ankle plantarflexors (Gage, 2004), torsional deformities of the tibia (Hicks, et al., 2007; Schwartz and Lakin, 2003), problems with balance, or other neurological issues (Rab, 1992). Spasticity has been observed to correlate with shorter and slower hamstrings (van der Krogt, et al., 2009). Thus, a broad range of possible contributing factors should be evaluated before performing surgical procedures to correct crouch gait.
This study demonstrates that peak hamstrings lengths and lengthening velocities increase significantly with walking speed in typically developing subjects. The results also reveal that a speed-matched comparison may alter the classification of a patient with crouch gait as having short and/or slow hamstrings. This has significant clinical implications when considering muscle lengthening surgery to correct crouch gait. Whether a speed-matched control protocol demonstrates greater power in predicting change in knee motion after hamstrings lengthening surgery remains an open question, and future work should assess this possibility.
Acknowledgments
We are grateful to May Liu for help with data analysis. This work was supported by the National Institutes of Health through the Roadmap for Medical Research U54 GM072970 and NIH R01 HD046814.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abel MF, Damiano DL, Pannunzio M, Bush J. Muscle-tendon surgery in diplegic cerebral palsy: functional and mechanical changes. J Pediatr Orthop. 1999;19:366–75. [PubMed] [Google Scholar]
- Arnold AS, Blemker SS, Delp SL. Evaluation of a deformable musculoskeletal model for estimating muscle-tendon lengths during crouch gait. Ann Biomed Eng. 2001;29:263–74. doi: 10.1114/1.1355277. [DOI] [PubMed] [Google Scholar]
- Arnold AS, Liu MQ, Schwartz MH, Ounpuu S, Delp SL. The role of estimating muscle-tendon lengths and velocities of the hamstrings in the evaluation and treatment of crouch gait. Gait Posture. 2006;23:273–81. doi: 10.1016/j.gaitpost.2005.03.003. [DOI] [PubMed] [Google Scholar]
- Arnold AS, Liu MQ, Schwartz MH, Ounpuu S, Dias LS, Delp SL. Do the hamstrings operate at increased muscle-tendon lengths and velocities after surgical lengthening? J Biomech. 2006;39:1498–506. doi: 10.1016/j.jbiomech.2005.03.026. [DOI] [PubMed] [Google Scholar]
- Baumann JU, Ruetsch H, Schurmann K. Distal hamstring lengthening in cerebral palsy. An evaluation by gait analysis. Int Orthop. 1980;3:305–9. doi: 10.1007/BF00266026. [DOI] [PubMed] [Google Scholar]
- Beals RK. Treatment of knee contracture in cerebral palsy by hamstring lengthening, posterior capsulotomy, and quadriceps mechanism shortening. Dev Med Child Neurol. 2001;43:802–5. doi: 10.1017/s0012162201001451. [DOI] [PubMed] [Google Scholar]
- Delp SL, Arnold AS, Speers RA, Moore CA. Hamstrings and psoas lengths during normal and crouch gait: implications for muscle-tendon surgery. J Orthop Res. 1996;14:144–51. doi: 10.1002/jor.1100140123. [DOI] [PubMed] [Google Scholar]
- Delp SL, Loan JP, Hoy MG, Zajac FE, Topp EL, Rosen JM. An interactive graphics-based model of the lower extremity to study orthopaedic surgical procedures. IEEE Trans Biomed Eng. 1990;37:757–67. doi: 10.1109/10.102791. [DOI] [PubMed] [Google Scholar]
- Delp SL, Zajac FE. Force- and moment-generating capacity of lower-extremity muscles before and after tendon lengthening. Clin Orthop Relat Res. 1992:247–59. [PubMed] [Google Scholar]
- Deluca PA, Ounpuu S, Davis RB, Walsh JH. Effect of hamstring and psoas lengthening on pelvic tilt in patients with spastic diplegic cerebral palsy. J Pediatr Orthop. 1998;18:712–8. [PubMed] [Google Scholar]
- Gage JR. Surgical treatment of knee dysfunction in cerebral palsy. Clin Orthop Relat Res. 1990:45–54. [PubMed] [Google Scholar]
- Hicks J, Arnold A, Anderson F, Schwartz M, Delp S. The effect of excessive tibial torsion on the capacity of muscles to extend the hip and knee during single-limb stance. Gait Posture. 2007;26:546–52. doi: 10.1016/j.gaitpost.2006.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hof AL. Scaling gait data to body size. Gait and Posture. 1996;4:222–223. [Google Scholar]
- Hoffinger SA, Rab GT, Abou-Ghaida H. Hamstrings in cerebral palsy crouch gait. J Pediatr Orthop. 1993;13:722–6. doi: 10.1097/01241398-199311000-00006. [DOI] [PubMed] [Google Scholar]
- Kay RM, Rethlefsen SA, Skaggs D, Leet A. Outcome of medial versus combined medial and lateral hamstring lengthening surgery in cerebral palsy. J Pediatr Orthop. 2002;22:169–72. [PubMed] [Google Scholar]
- Lu TW, O'Connor JJ. Bone position estimation from skin marker co-ordinates using global optimisation with joint constraints. J Biomech. 1999;32:129–34. doi: 10.1016/s0021-9290(98)00158-4. [DOI] [PubMed] [Google Scholar]
- Novacheck TF, Trost JP, Schwartz MH. Intramuscular psoas lengthening improves dynamic hip function in children with cerebral palsy. J Pediatr Orthop. 2002;22:158–64. [PubMed] [Google Scholar]
- Oberhofer K, Mithraratne K, Stott NS, Anderson IA. Error propagation from kinematic data to modeled muscle-tendon lengths during walking. J Biomech. 2009;42:77–81. doi: 10.1016/j.jbiomech.2008.10.007. [DOI] [PubMed] [Google Scholar]
- Rab G. Consensus on crouched gait. In: Sussman M, editor. The Diplegic Child: Evaluation and Management. Park Ridge, Illinois: 1992. pp. 337–339. [Google Scholar]
- Reimers J. Static and dynamic problems in spastic cerebral palsy. J Bone Joint Surg Br. 1973;55:822–7. [PubMed] [Google Scholar]
- Roosth HP. Flexion deformity of the hip and knee in spastic cerebral palsy: treatment by early release of spastic hip-flexor muscles. J Bone Joint Surg Am. 1971;53:1489–510. [PubMed] [Google Scholar]
- Schutte LM, Hayden SW, Gage JR. Lengths of hamstrings and psoas muscles during crouch gait: effects of femoral anteversion. J Orthop Res. 1997;15:615–21. doi: 10.1002/jor.1100150419. [DOI] [PubMed] [Google Scholar]
- Schwartz M, Lakin G. The effect of tibial torsion on the dynamic function of the soleus during gait. Gait Posture. 2003;17:113–8. doi: 10.1016/s0966-6362(02)00058-9. [DOI] [PubMed] [Google Scholar]
- Schwartz MH, Rozumalski A, Trost JP. The effect of walking speed on the gait of typically developing children. J Biomech. 2008;41:1639–50. doi: 10.1016/j.jbiomech.2008.03.015. [DOI] [PubMed] [Google Scholar]
- Sutherland DH, Davids JR. Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res. 1993:139–47. [PubMed] [Google Scholar]
- van der Krogt MM, Doorenbosch CA, Harlaar J. Muscle length and lengthening velocity in voluntary crouch gait. Gait Posture. 2007;26:532–8. doi: 10.1016/j.gaitpost.2006.11.208. [DOI] [PubMed] [Google Scholar]
- van der Krogt MM, Doorenbosch CA, Harlaar J. The effect of walking speed on hamstrings length and lengthening velocity in children with spastic cerebral palsy. Gait Posture. 2009;29:640–4. doi: 10.1016/j.gaitpost.2009.01.007. [DOI] [PubMed] [Google Scholar]