

Abstract
Objective
To identify trajectories of behavioral adjustment from ages 6 to 14 for youth placed in early foster care, and to examine links between trajectories and early cognitive ability and social competence; caregiver stability; and frequency, timing, and type of maltreatment.
Method
Participants were 279 youth from the Southwest site of the Consortium for Longitudinal Studies of Child Abuse and Neglect (LONGSCAN). All youth had spent at least 5 months in out-of-home care prior to age 4 due to substantiated reports of maltreatment. Behavioral adjustment was assessed using caregiver reports on the Child Behavior Checklist at ages 6, 8, 10, 12, and 14. Cognitive ability and social competence were assessed at age 6. Caregiver stability was recorded every two years from age 6 to 14 and summed. Child protective services (CPS) maltreatment reports were coded for type and frequency.
Results
Growth mixture modeling identified 3 internalizing trajectories: stable adjustment (66.7%), mixed/decreasing adjustment (25.4%), and increasing adjustment (7.9%). Four externalizing trajectories were identified: stable adjustment (46.6%), mixed adjustment (28.7%), increasing adjustment (8.2%), and stable maladjustment (16.5%). Trajectories of stable or increasing adjustment were predicted by social competence, cognitive ability, placement stability, and low frequency of physical abuse from ages 6 to 14.
Conclusions
Many youth who have spent time in early out-of-home care evidence stable, long-term positive behavioral adjustment. Trajectories reflecting more positive adjustment are associated with early child cognitive ability and social competence, long-term caregiver stability, and low frequency of physical abuse in middle childhood and adolescence.
Keywords: maltreatment, child welfare, growth mixture modeling, behavioral adjustment
Nearly 50% of youth placed in out-of-home care by child protective services experience behavior problems in the clinical range, according to the results of cross-sectional research.1-3 This high rate of behavioral disorder is consistent with the multiple adversities experienced by youth who spend time in foster care, including maltreatment, removal from the home, and disruption at the levels of family, school, and neighborhood. At the same time, this statistic suggests that despite exposure to multiple threats to development, more than half of youth in child welfare do not evidence behavior problems, i.e., they can be said to be experiencing positive behavioral adjustment.
In response to the urgency suggested by high rates of behavioral disorder among youth with child welfare involvement,1-3 the present study examined trajectories of behavioral adjustment from age 6 to 14 among youth who spent at least five months in out-of-home foster care before the age of 4 years as a result of substantiated maltreatment. Within the domain of behavioral adjustment, we distinguished between internalizing and externalizing behaviors, based on evidence that – despite their typical covariance – they demonstrate distinct trajectories.4
While a handful of studies have examined rates and predictors of behavioral adjustment among individuals who have experienced child welfare involvement,5, 6 we know very little regarding the course of such adjustment. The results of short-term prospective research suggest that behavioral adjustment may be unstable for youth in child welfare. A study with data from the National Survey of Child and Adolescent Well-Being (NSCAW) found that for youth in child welfare aged 8 to 16 years at baseline, only 19% experienced positive behavioral adjustment (defined using cutoffs from the Child Behavior Checklist and other measures) consistently during the three years following a completed child welfare investigation.5 However, no research has examined individual trajectories of behavioral adjustment across developmental periods for youth following involvement with child welfare. We do not know whether behavioral adjustment is characterized by stability or change over the course of development among this high-risk population, nor what factors may influence its course. Long-term prospective research is critical for identifying factors that can promote positive adjustment as well as “bouncing back” from earlier maladjustment.
There is broad consensus that for high-risk groups, promoting adaptive functioning is preferable to treating disorders after they develop. In order to achieve this, researchers must identify mutable factors with the potential for modifying the impact of adverse life experiences and promoting positive adjustment. To this end, it has been recommended that risk and resilience research focus on specific risk circumstances, such as child welfare involvement, in order to identify issues of particular salience to specific populations.7
Results from maltreatment research suggest that the course of behavioral adjustment may be heterogeneous, and associated with a number of mutable factors at the levels of child and environment. At the level of the child, cognitive ability8-10 and social competence11, 12 have been linked to behavioral adjustment. At the level of the environment, characteristics of children's maltreatment experiences, such as frequency, type, and developmental timing, have also been associated with behavioral outcomes.13, 14 For youth who have spent time in out-of-home care, caregiver stability is a particularly salient factor that has been associated with positive adjustment.15 Evidence from prospective research suggests that this latter relationship may be bidirectional, with caregiver instability acting as both a cause and a consequence of youth behavior problems.16-18
Given the high rates of documented behavioral disorder for youth in child welfare, it is important to ask whether individuals who experience positive behavioral adjustment at one point during childhood are likely to maintain that adjustment, and to identify factors related to changes or stability in adjustment over time. This study contributes to the literature by utilizing prospective measurement at five time points to model trajectories of behavioral adjustment over an 8-year period from middle childhood through early adolescence in a sample of youth who spent time in early foster care.
The present study used a person-centered approach, latent variable growth mixture modeling (GMM),19, 20 to identify trajectories of behavioral adjustment using data collected when youth were 6, 8, 10, 12, and 14 years old. Positive behavioral adjustment in this high-risk sample was defined as the absence of borderline or clinically significant behavior problems, and was examined separately for externalizing and internalizing behaviors. We hypothesized that heterogeneous trajectory classes would be identified (e.g., subgroups of youth with differing patterns of behavioral adjustment over time). We further hypothesized that early cognitive ability, early social competence, and caregiver stability would be associated with trajectories characterized by stable or increasing positive adjustment, while maltreatment (examined in terms of frequency, timing, and type) would be associated with trajectories reflecting poorer adjustment.
Method
Sample
The present analysis is based on data from the Southwest site of the Consortium for Longitudinal Studies of Child Abuse and Neglect (LONGSCAN).21 All children at this site (n = 330) entered the child welfare system by the age of three and a half years as a result of a substantiated report of maltreatment during an 18-month period (May 1990 through October 1991), and remained in out-of-home foster care for at least five months. The analyses reported here were limited to participants with completed measures for at least 3 of 5 possible time points at ages 6, 8, 10, 12, and 14 (n = 279; 53.4% female). Of the cases excluded, eight had no data for any of the 5 time points, 23 had data at only 1 time point, and 20 had data at two time points. Excluded and non-excluded cases did not differ with regard to any study variables or demographic variables (i.e., gender, ethnicity, family income, or age at first referral).
For the present study sample, the median age at first referral was 3.9 months, and the modal type of maltreatment substantiation was neglect (53.3%). At the baseline assessment (age 4), 35.4% of youth had been reunited with the biological parent, 19.7% had been adopted, and 44.8% were in foster care (including 20.4% in kinship care, 23.7% in non-relative care, and 0.4% in a group home). The sample is ethnically diverse and representative of the children in the San Diego County child welfare system (38.4% African American, 28.3% Caucasian, 16.1% Hispanic, 17.2% mixed or other). Median annual household family income for participants was fairly stable from age 6 to age 14 at approximately $20,000 to $25,000.
Data were collected through bi-annual face-to-face interviews. Additionally, CPS records were reviewed and coded for official reports of child maltreatment every two years since birth. This study was conducted with IRB approval. Informed consent was obtained from caregivers, and assent was obtained from the child participants. Youth and their caregivers were paid a fixed, nominal amount for their participation at each interview.
Measures
Internalizing and externalizing behaviors
Primary caregivers rated youth on the Child Behavior Checklist (CBCL/ages 4-18)22 at ages 6, 8, 10, 12, and 14. Caregivers reported the frequency of 113 child behaviors during the six months previous to each interview, using a 3-point Likert scale (0 = not true, 1 = sometimes true, 2 = often true). The CBCL is an empirically validated measure of child and adolescent behavior problems with acceptable reliability and validity.22 CBCL broadband scales (internalizing and externalizing) were used for main study analyses. Additionally, the total problem scale was examined in descriptive analyses.
Early social competence
Child social competence was measured at age six using the 15-item socialization scale from the Vineland Screener Socialization Subtest.23 Caregivers rated children on each item using a 3-point Likert scale (2 = child performs activity satisfactorily and habitually, 1 = emergent performance of a skill or activity, 0 = too young/immature to perform the activity). Correlation between the Vineland Screener and the full Vineland Adaptive Behavior Scale for the domain of socialization is reported as .92.24
Early cognitive ability
Child cognitive ability was measured at age six using the Block Design subtest of the Wechsler Preschool and Primary Scale of Intelligence – Revised (WPPSI-R): Short Form Vocabulary and Block Design.25 The WPPSI-R is designed to briefly assess the general intellectual functioning of children aged 3 to 7 years and 3 months. The Block Design subtest asks the child to reproduce designs using 3 or 4 flat, 2-colored blocks. The WPPSI-R is reported to have adequate and concurrent construct validity, and has a reported average reliability coefficient of .85 for the Block Design.25
Caregiver stability
At each bi-annual interview (at 4, 6, 8, 10, 12, and 14 years) the primary caregiver's relationship to the child was recorded. For ages 6-14, caregiver stability was coded as “1” when the caregiver was the same individual as the previous interview, and “0” when the caregiver had changed since the previous interview. Caregiver stability codes for ages 6-14 were summed across time points to create a continuous measure of stability that ranged from 0 (child was never living with the same primary caregiver) to 5 (child was living with the same primary caregiver across all 5 time points). Youth experienced a range of values on the caregiver stability variable regardless of baseline (age 4) placement type. The nature of the caregiver changes were diverse; while some remained reunified with or adopted by the same caregiver, others bounced back and forth between reunification and foster care, from foster family to foster family, between biological parents, or from failed adoption back to foster care.
Maltreatment
CPS records were reviewed every two years. Reports alleging maltreatment were coded for date of referral and type of maltreatment using the Modified Maltreatment Classification System.26, 27 For the current analyses, frequency of allegation reports for three types of maltreatment were analyzed (physical abuse, sexual abuse, and neglect). The number of CPS allegations for each type was summed from birth to age 6 (prior to the study period) and from age 6 to 14 (concurrent with the study period) to create the continuous variables indicating frequency of early and late physical abuse, sexual abuse, and neglect.
Data Analysis
Conceptual and operational overview of Growth Mixture Modeling (GMM)
Building on the conceptual underpinnings of latent growth curve modeling and latent class analysis, growth mixture modeling19, 20 identifies classes/profiles of individuals that share a common growth trajectory over time for a target variable (e.g., internalizing score). This approach is similar to the former because individual values for a target variable of interest are modeled longitudinally (i.e., each individual has his/her own growth trajectory); this approach is similar to the latter in that a categorical latent variable is created that represents individuals who share a common growth trajectory (and thus would be assigned to the same class) but differ from individuals other who have been assigned to other classes (i.e., those that have different growth trajectories). Thus, for example, individuals who have increasing scores for a target outcome variable over time of interest would be assigned to the same class, whereas individuals who have decreasing scores for the target outcome variable over time would be assigned to a different class.
The determination of the optimal number of classes/profiles (referred to as class enumeration) is initiated. This requires the specification and testing of multiple class solutions (1-class, 2-class, 3-class, etc.). From these models, the designation of the “best-fitting” model is determined using a variety of statistical indicators. Evaluation of the best fitting models was accomplished using both statistical and theoretical criteria. Statistically, key considerations included the Akaike Information Criterion (AIC), the sample-size adjusted Bayesian Information Criterion (SSAdj BIC), the Lo-Mendell-Rubin likelihood ratio test (LMR), and entropy. For the AIC and SSAdj. BIC, lower values signify a better fitting model. For the LMR, a low p-value (p < .05) indicates that the k trajectory model is a better fit to the data compared to the k-1 trajectory model. Entropy is a measure of classification accuracy with values closer to 1 indexing greater precision (range 0-1). Theoretical criteria included adequate class size and interpretability of classes. We defined adequate class size as at least 5% of the sample, a value typically considered the threshold for a meaningful class.28
In the current study two target outcome variables were of interest: behavioral adjustment with regard to internalizing and externalizing behaviors, respectively. Each outcome variable was evaluated in a separate GMM analysis. At each time point, youth were categorized as experiencing positive adjustment in the domain of internalizing or externalizing if their age and gender-standardized T score on the respective CBCL broadband scale was less than the borderline cutoff of 60, indicating the absence of clinically significant problem behaviors.22
Main study analyses
GMM trajectory classes were evaluated using the Mplus Version 5.0 program.29 Models were estimated independently for internalizing and externalizing behaviors using data from age 6 to 14 for these variables. Full-information maximum-likelihood (FIML) estimation was used to account for missing data.19, 30 Analyses were limited to cases with data for at least 3 of 5 possible time points in order to maximize the stability of the solution and to permit the exploration of nonlinear trajectories; comparison models with the full sample did not differ from those presented here. Following exploratory analyses that supported the linearity of the trajectories observed, all models constrained growth across time to be linear.
A series of models with progressively greater numbers of trajectory classes were estimated. Once the optimal number of classes was determined for the internalizing and externalizing GMM, respectively, and the classes were substantively interpreted, logistic regression was used to predict trajectory classes with function of early cognitive ability, early social competence, caregiver stability, and frequency of early and late physical abuse, sexual abuse, and neglect entered as predictor variables simultaneously.
Results
Descriptive Statistics
Descriptive statistics for all predictors are presented in Table 1. Mean scores for early social competence and cognitive ability were nearly one standard deviation below published norms. Caregiver stability varied considerably: 54.7% of youth experienced stability across all 5 time points, whereas 20.5% experienced it across 3 or less time points. All youth experienced at least one type of early maltreatment, and 49.5% experienced some type of late maltreatment. Neglect was the most frequent type of maltreatment reported.
Table 1. Descriptive Statistics for All Predictor Variables.
| Standard | |||
|---|---|---|---|
| Mean | Deviation | Range | |
| Early Cognitive Ability (Age 6) | 7.62 | 2.71 | 0-16 |
| Early Social Competence (Age 6) | 89.62 | 15.03 | 57-128 |
| Placement Stability (Age 6 - 14) | .79 | 1.12 | 0-5 |
| Frequency of Early Maltreatment (Birth - Age 6) | |||
| Physical Abuse | .57 | .92 | 1-5 |
| Sexual Abuse | .22 | .52 | 1-3 |
| Neglect | 1.95 | 1.75 | 1-12 |
| Frequency of Late Maltreatment (Age 6 - 14) | |||
| Physical Abuse | .57 | .96 | 0-5 |
| Sexual Abuse | .19 | .57 | 0-4 |
| Neglect | .81 | 1.63 | 0-10 |
Rates of positive behavioral adjustment at each time point, based on the percentage of youth scoring in the normal range on the CBCL internalizing and externalizing scales and on the total problem scale, are presented in Figure 1. For the overall sample, the percentage of youth experiencing internalizing positive behavioral adjustment declined over time ranging from 80.0% at age 6 to 70.7% at age 14. For externalizing, the percentage of youth experiencing positive behavioral adjustment remained relatively stable over time ranging from 59.5% to 64.2 %. Positive adjustment measured by the total problem scale followed nearly an identical pattern over time to that of adjustment measured with the externalizing scale, with the percentage of youth experiencing positive overall adjustment (according to the total problem scale) ranging from 57.9% to 64.4%.
Figure 1.
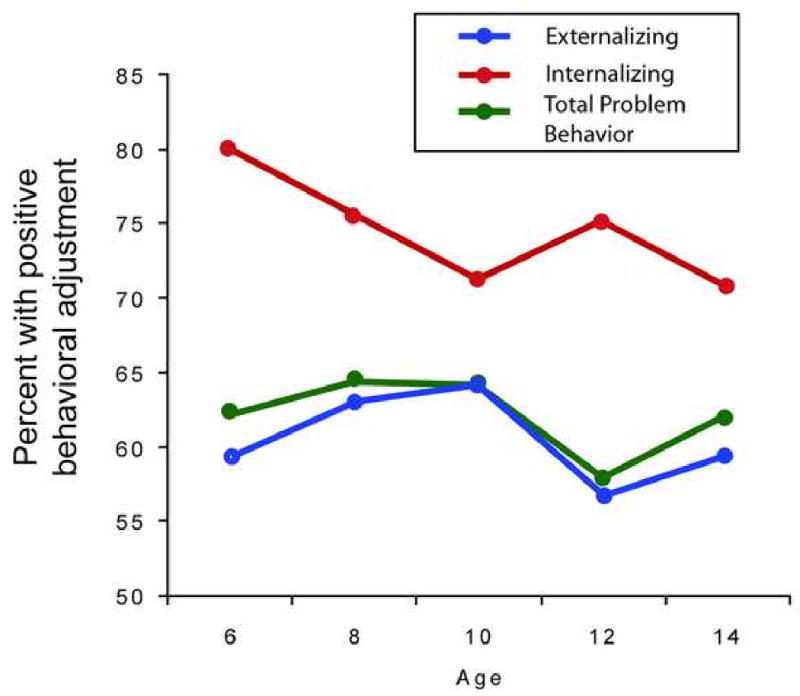
Rates of positive behavioral adjustment over time based on internalizing, externalizing, and total problem behavior scores.
Trajectory Classes
Internalizing
As shown in Table 2, a 3-class solution had the most support based on our statistical criteria: Two fit indicators supported a 3-class solution (AIC and SSAdj BIC), one supported a 2-class solution (LMR), and one was ambiguous (entropy). In selecting the 3-class solution, we were influenced in part by recent simulation studies that have identified SSAdj BIC as the most accurate index in deciding on number of classes.31, 32 A 3-class solution also had the most support based on our two theoretical criteria (adequate class size and interpretability of classes). The 3-class model had adequate class sizes and was more interpretable than the 2-class model, in that it yielded a relatively small but interesting class of individuals who experienced change in their adjustment; this change was obscured in the two-class solution, which subsumed these youth in a larger class that also contained individuals who did not experience change.
Table 2.
Fit Indices for Growth Models, n = 279
| Classes | AICa | SSAdj BICa | Entropyb | LMRc |
|---|---|---|---|---|
| Internalizing | ||||
| 1 | 1376.23 | 1377.15 | NA | NA |
| 2 | 1205.23 | 1207.53 | 0.73 | 167.11* |
| 3 | 1199.13 | 1202.81 | 0.72 | 11.42 |
| 4 | 1203.04 | 1208.10 | 0.69 | 1.98 |
| 5 | 1208.39 | 1214.83 | 0.71 | 0.61 |
| Externalizing | ||||
| 1 | 1632.62 | 1633.54 | NA | NA |
| 2 | 1374.74 | 1377.05 | 0.79 | 249.13* |
| 3 | 1364.44 | 1368.12 | 0.79 | 15.39* |
| 4 | 1358.67 | 1363.73 | 0.71 | 11.11* |
| 5 | 1360.26 | 1366.70 | 0.76 | 7.42 |
Note: AIC = Akaike information criterion; BIC = Bayesian information criterion; LMR = Low-Mendell-Rubin adjusted likelihood ratio test; SSAdj = sample-size adjusted.
Lower AIC and SSAdj. BIC values indicate better fit
Values should be greater than 0.7; values closer to one are better. Entropy refers to the average classification accuracy in assigning individuals to classes.
Significant values indicate k-classes fit better than k-1 classes.
p < 0.05
The three classes identified for internalizing (Figure 2a) were (1) stable adjustment (66.7% of the sample), whose members experienced consistently high levels of positive adjustment; (2) mixed/decreasing adjustment (25.4%), with youth who alternated between positive adjustment and maladjustment, with decreasing levels of positive adjustment over time; and (3) increasing adjustment (7.9%), whose members experienced high levels of initial maladjustment with moderate increases in adjustment beginning at age 10.
Figure 2.
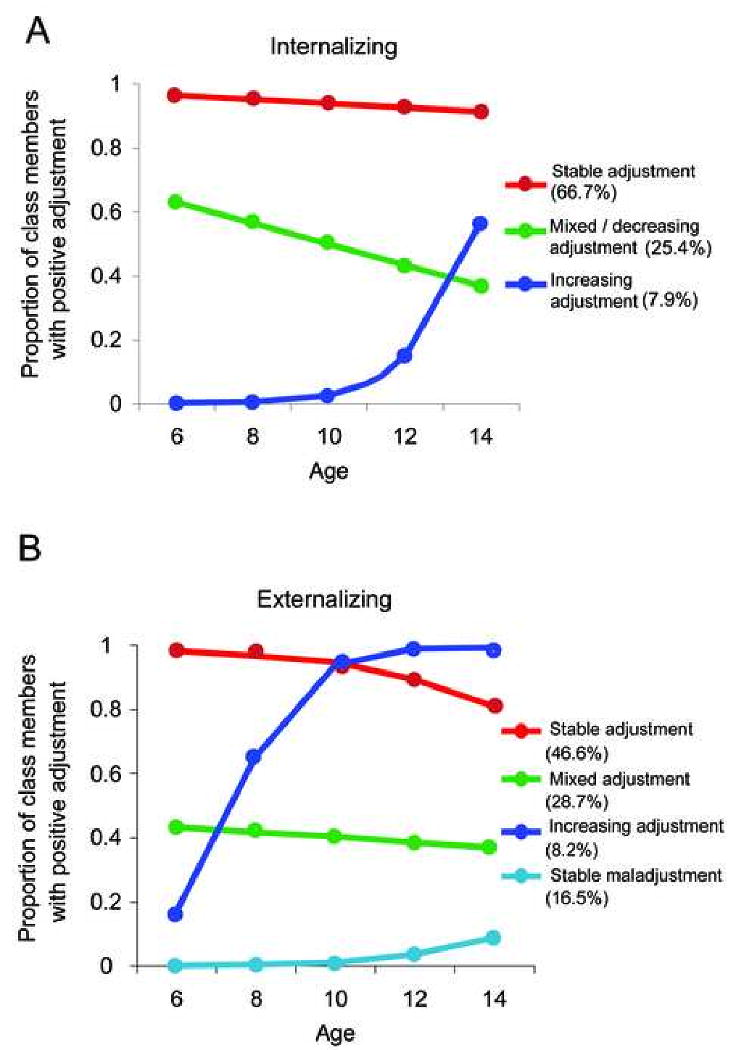
Latent growth mixture model trajectories of behavioral adjustment from ages 6 to 14.
Externalizing
For externalizing, the AIC and SSAdj. BIC, and LMR values indicated that a 4-class model fit the data best (Table 2). The 4-class solution did have a lower entropy value than the 3-, and 5-class models; however, the difference between the entropy values was minimal. The 4-class model had adequate class sizes and was more interpretable than the 3-class model.
The four classes identified for externalizing (Figure 2b) were (1) stable adjustment (46.6%), with consistently high levels of positive adjustment, (2) mixed adjustment (28.7%), whose members alternated between positive adjustment and maladjustment consistently over time, (3) increasing adjustment (8.2%), whose members experienced high levels of initial behavioral maladjustment with steep increases in positive adjustment beginning at age 6; and (4) stable maladjustment (16.5%), whose members consistently experienced behavioral maladjustment across all time points.
Predicting Trajectory Class Membership
Multinomial logistic regression analyses to predict trajectory class membership were conducted separately for internalizing and externalizing. Based on evidence that fluctuations in adjustment may be the norm for youth with child welfare involvement,5 the mixed adjustment class was used as the reference group for both types of behaviors. Hypothesized predictors were entered simultaneously into the models.
For internalizing, membership in the stable adjustment class was predicted by caregiver stability and low frequency of late physical abuse (Table 3). Odds of membership in the increasing adjustment class were increased by early cognitive ability and decreased by early social competence.
Table 3.
Predictors of Trajectory Classes – Multinomial Logit Models
| Internalizing | Externalizing | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Stable adjustment | Increasing adjustment | Stable adjustment | Increasing adjustment | Stable disorder | ||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Early cognitive ability | 1.11 | 0.99-1.26 | 1.30** | 1.07-1.59 | 1.15* | 1.02-1.30 | 1.01 | 0.84-1.22 | 1.03 | 0.88-1.20 |
| Early social competence | 1.01 | 0.99-1.03 | 0.96* | 0.92-1.00 | 1.02 | 1.00-1.04 | 0.99 | 0.96-1.03 | 0.97* | 0.94-1.00 |
| Placement stability | 1.44* | 1.06-1.95 | 1.57 | 0.90-2.73 | 1.47* | 1.05-2.05 | 1.32 | 0.75-2.34 | 1.22 | 0.82-1.72 |
| Frequency of Early Maltreatment | ||||||||||
| Physical abuse | 1.37 | 0.92-2.05 | 1.18 | 0.60-2.33 | 1.04 | 0.72-1.49 | 0.71 | 0.33-1.54 | 0.94 | 0.56-1.43 |
| Sexual abuse | 0.57 | 0.30-1.07 | 0.79 | 0.27-2.28 | 0.69 | 0.35-1.34 | 0.23 | 0.03-1.99 | 1.26 | 0.58-2.89 |
| Neglect | 1.09 | 0.89-1.31 | 0.92 | 0.65-1.32 | 0.97 | 0.81-1.17 | 1.21 | 0.91-1.61 | 0.86 | 0.63-1.06 |
| Frequency of Late Maltreatment | ||||||||||
| Physical abuse | 0.64* | 0.46-0.90 | 0.57 | 0.27-1.20 | 0 .79 | 0.54-1.16 | 0.34 | 0.11-1.02 | 1.45 | 0.96-2.48 |
| Sexual abuse | 1.36 | 0.62-1.81 | 1.66 | 0.78-3.50 | 0.89 | 0.50-1.59 | 0.62 | 0.17-2.28 | 0.95 | 0.55-1.89 |
| Neglect | 0.95 | 0.77-1.16 | 0.93 | 0.64-1.35 | 0.99 | 0.76-1.28 | 1.22 | 0.88-1.68 | 1.15 | 0.48-1.50 |
Note: CI = confidence interval; OR = odds ratio;
p < .05.
p < .01.
For externalizing, early cognitive ability and caregiver stability predicted membership in the stable adjustment class, and early social competence decreased odds of membership in the stable maladjustment class (Table 3). In addition to the multinomial regression analyses presented in Table 3, an additional multinomial logistic regression was conducted with the same predictors using the externalizing stable maladjustment class as the reference group, in order to distinguish it from the increasing adjustment class. This comparison was of particular interest given that both of these groups had similarly high initial levels of maladjustment, and one group maintained that level of maladjustment while the other one experienced a sharp increase in positive adjustment. Results indicated that higher frequency of late physical abuse decreased the odds of membership in the increasing adjustment group by a factor of .23 (CI = .08-.72; p < .05).
Discussion
This is the first long-term longitudinal study we know of to examine the course of behavioral adjustment at multiple time points across developmental periods for youth who have spent time in out-of-home care. As hypothesized, considerable heterogeneity was found in eight-year trajectories of both internalizing and externalizing behaviors. While subgroups of youth experienced stable positive adjustment or maladjustment across all five time points, others experienced increases or decreases in positive adjustment over time, or alternated between adjustment and maladjustment.
We found evidence of long-term stability of behavioral adjustment for a sizable portion of our sample. The largest trajectory classes for both internalizing and externalizing behaviors consisted of youth who experienced stable positive adjustment over the course of eight years. This is remarkable, considering that children placed in out-of-home care by child protective services represent one of the highest-risk groups in the U.S. in terms of exposure to multiple adverse experiences, severe forms of maltreatment, and the development of problem behaviors. This finding contrasts with the results of prior research using NSCAW data, which found that behavioral adjustment was unstable.5 An important distinction is that we assessed adjustment beginning 3 years after children's initial child welfare involvement and continuing for an eight-year period, whereas NSCAW assessed adjustment beginning six months after children's investigation and continuing for three years. It may be the case that behavioral adjustment is initially unstable following child welfare involvement and the resulting disruption and stress, but becomes more stable with the passage of time. Another important finding was the identification of small subgroups of youth who “bounced back” from early behavioral maladjustment. For internalizing, these youth experienced increases in positive adjustment beginning at age 12. For externalizing, increases in adjustment began much earlier (age 6). The identification of a substantial subgroup of youth (16.5%) who experienced stable externalizing behavior problems provided a sobering counterpoint to the groups experiencing stable or increasing adjustment.
With regard to prediction of trajectories, the most consistent effect identified was that of caregiver stability. For both internalizing and externalizing behaviors, stable positive adjustment was associated with caregiver stability. This is consistent with prior research that has linked positive adjustment to caregiver stability15 and internalizing and externalizing problems to caregiver instability.20, 25 However, with some exceptions,15 most prior research on caregiver instability has focused on short-term disruptions and re-referrals. The association of eight-year trajectories of stable positive adjustment with caregiver stability over the same period suggests that these variables continue to influence one another in the long-term. Because our measurement of behavioral adjustment and caregiver stability were concurrent, we cannot infer the direction of the effect. Caregiver changes are common among maltreated children who have been placed in foster care, and represent a significant disruption of family, neighborhood, peer, and school ties. In our sample, youth experienced up to five caregiver changes during the eight-year study period. On the other hand, initial levels of child externalizing problem behaviors have been supported as predictors of subsequent caregiver instability.18 Results from recent prospective studies suggest a bidirectional effect in which youth behavioral maladjustment can be both a consequence and a cause of caregiver instability.16-18
The strongest effect identified was for physical abuse between age 6 and 14, which significantly decreased probability of membership in the stable adjustment group for internalizing (relative to the mixed group) by a factor of .63 and decreased membership in the increasing adjustment group for externalizing (relative to the stable maladjustment group) by a factor of .23. These findings are consistent with prior research on the effects of maltreatment recurrence and chronicity on child behavior problems,33-35 and support the importance of continued monitoring for youth with early substantiated maltreatment.
It is notable that findings regarding the role of early cognitive ability and early social competence were somewhat equivocal. On the one hand, both early cognitive ability and early social competence significantly predicted membership in the expected direction for some internalizing and externalizing classes. On the other hand, early social competence appeared to decrease the probability of membership in the internalizing increasing adjustment class. However, the effect was modest, and although this class experienced gains in adjustment over time, it did show extremely low rates of positive adjustment at most time points, perhaps indicating that overall this small group was less well adjusted than the mixed adjustment reference group. It is also interesting that early cognitive ability predicted membership in this increasing adjustment group. It may be the case that early cognitive ability emerged as an agent of change later in childhood, despite the lower early social competence that may have been related to the initial levels of internalizing problems.
Also of note, frequency of early physical abuse, sexual abuse, and neglect failed to predict membership in any group. However, all youth in this sample were removed from the home due to substantiated maltreatment, and many were reported for multiple types of maltreatment, whereas fewer youth experienced ongoing maltreatment after age 6. It may also be the case that frequency of late maltreatment, or recurrence, exerted a more proximal influence on adjustment trajectories.
Our overall rates of positive behavioral adjustment were slightly higher than those published in prior research.1-3, 5 This is likely due to methodological differences among the studies (i.e., use of different measures, cut-points, and informants). Interestingly, descriptive analyses showed that overall rates of positive adjustment (measured with the CBCL total problem scale) followed a nearly identical pattern over time to those of positive adjustment specific to the domain of externalizing behaviors. This finding raises the possibility that previously published rates of behavioral adjustment or mental health need based on total problem scores may reflect externalizing problems more than internalizing problems.1-3
The present study has several limitations. First, we only examined adjustment in a single domain of functioning (behavioral). Youth may experience positive adjustment in one domain (e.g., behavioral) and still struggle in others (e.g., school or peer group adjustment).7 We chose to focus on behavioral resilience due to the urgency suggested by high rates of behavioral disorder in this population.1 Within this domain, we distinguished between internalizing and externalizing behavior problems, based on evidence that – despite their typical covariance36 – they demonstrate distinct trajectories.4 However, because data were only analyzed within one domain of adjustment, the results presented should be interpreted as part of a broader process that encompasses multiple domains and competencies.
Second, we relied on caregiver reports of child internalizing and externalizing behaviors. For youth who displayed behavioral differences over time, changes in problem behavior scores were not limited to incidences of caregiver change. However, variation in the participating caregiver may have led to differences in reporting from one time point to the next for some youth.
Third, while dichotomizing internalizing and externalizing scores allowed us to make distinctions between positive adjustment versus maladjustment, the use of a cutoff value may raise questions as to whether the youth with trajectories displaying change in adjustment over time experienced clinically significant change, or whether their scores simply varied slightly around the chosen cutoff score. However, among youth in the three longitudinal classes characterized by change, the average change in T score from age 6 to age 14 was approximately 14 points.
Finally, because our main outcome variables in the present study were discrete trajectory classes based on adjustment patterns over the course of eight years, we were limited in our ability to examine predictors that fluctuate over time in this sample. For example, we do not disentangle the relationship between caregiver stability and behavioral adjustment, nor do we examine the impact of caregiver type (whether the youth is living with a biological parent, adopted parent, or foster caregiver) on adjustment at different points. Stability reflects only one dimension of a youth's caregiving environment, and does not provide information regarding the type of environment nor its quality, both of which we would expect to influence trajectories of youths' behavioral adjustment.
Despite these limitations, the present results provide the first long-term analysis of the course of behavioral adjustment among youth who were placed in early foster care. Our study has several strengths that enhance its contribution to the literature: the use of prospective data on maltreatment and behavioral adjustment collected every two years through age 14; a diverse sample with regard to placement; the examination of internalizing and externalizing behavioral adjustment longitudinally over an 8-year period spanning childhood and adolescence; and the integration of a person-centered approach, which models heterogeneity in trajectories, with a variable-centered approach, which permits the prediction of trajectory class membership from salient risk and protective factors.
With regard to mutable factors amenable to intervention, the present results support a relationship between environmental factors such as caregiver stability and maltreatment recurrence and long-term behavioral adjustment patterns for youth who were placed in early foster care. Policy and interventions that target these factors may promote the maintenance of positive behavioral adjustment as well as the “bouncing back” from earlier maladjustment. The present findings support the current emphasis on stability and permanency in child welfare law, and extend prior short-term findings on the importance of stability to child mental health. They also support both early and continued screening and treatment for behavior problems; there is ample evidence documenting the disparity between mental health need and receipt of services for youth in child welfare,37 and closing this gap could result in more youth moving into the “increasing adjustment” classes.
The present results suggest that considerable heterogeneity exists with regard to long-term patterns of behavioral adjustment for youth who were placed in early foster care. Future research utilizing measures from multiple informants would strengthen the current results. Also, the use of similar methodology with samples who were placed in foster care during diverse developmental stages would permit an examination of age effects. Future studies are also needed to examine trajectories of behavioral adjustment in conjunction with adjustment and competencies in other developmentally salient areas of functioning, such as school, peer group, work, substance use, friendships, romantic and sexual relationships. Additionally, longitudinal research is needed to disentangle the potentially bidirectional effects of caregiver stability and behavioral adjustment in the long term. Given the evidence of a gap between mental health need and receipt of services for youth in child welfare,37 it would also be of interest to examine longitudinal relationships between mental health service use and adjustment trajectories. Finally, while the present results provide evidence of heterogeneity in adjustment patterns, they also raise questions regarding factors that may account for the observed differences. Future research could use growth modeling approaches that permit the inclusion of time-varying covariates to examine the effects on adjustment trajectories of caregiver changes, caregiver type, and other salient characteristics of the caregiving environment, as well as time-varying factors in youths' school and peer environments. The predictors of stability and change of behavioral adjustment in the population are likely complex and involve multiple proximal processes.
Acknowledgments
This work was supported by K01DA21674 from the National Institute on Drug Abuse to Laura J. Proctor and 90CA1458, 90CA1566, 90CA1676 and 90CA1748 from the Office of Child Abuse and Neglect, Administration for Children, Youth, and Families, U.S. Department of Health and Human Services to the Consortium of Longitudinal Studies on Child Abuse and Neglect (LONGSCAN)-Southwest site.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Burns BJ, Phillips SD, Wagner HR, et al. Mental health need and access to mental health services by youths involved with child welfare: a national survey. J Am Acad Child Adolesc Psychiatry. 2004;43:960–970. doi: 10.1097/01.chi.0000127590.95585.65. [DOI] [PubMed] [Google Scholar]
- 2.Clausen JM, Landsverk J, Ganger W, Chadwick D, Litrownik A. Mental health problems of children in foster care. J Child Fam Stud. 1998;7:283–296. [Google Scholar]
- 3.Leslie LK, Hurlburt MS, Landsverk J, Barth R, Slymen DJ. Outpatient mental health services for children in foster care: a national perspective. Child Abuse Negl. 2004;28:699–714. doi: 10.1016/j.chiabu.2004.01.004. [DOI] [PubMed] [Google Scholar]
- 4.Leve L, Kim H, Pears K. Childhood temperament and family environment as predictors of internalizing and externalizing trajectories from ages 5 to 17. J Abnorm Child Psychol. 2005;33:505–520. doi: 10.1007/s10802-005-6734-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jaffee SR, Gallop R. Social, emotional, and academic competence among children who have had contact with child protective services: prevalence and stability estimates. J Am Acad Child Adolesc Psychiatry. 2007;46:757–765. doi: 10.1097/chi.0b013e318040b247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McGloin JM, Widom CS. Resilience among abused and neglected children grown up. Dev Psychopathol. 2001;13:1021–1038. doi: 10.1017/s095457940100414x. [DOI] [PubMed] [Google Scholar]
- 7.Luthar SS. Resilience in development: A synthesis of research across five decades. In: Cicchetti D, Cohen DJ, editors. Developmental Psychopathology, Vol 3: Risk, Disorder, and Adaptation. 2nd. Hoboken, NJ: Wiley; 2006. pp. 739–795. [Google Scholar]
- 8.Cicchetti D, Rogosch FA, Lynch M, Holt KD. Resilience in maltreated children: processes leading to adaptive outcome. Dev Psychopathol. 1993;5:629–647. [Google Scholar]
- 9.Cicchetti D, Rogosch FA. The role of self-organization in the promotion of resilience in maltreated children. Dev Psychopathol. 1997;9:797–815. doi: 10.1017/s0954579497001442. [DOI] [PubMed] [Google Scholar]
- 10.Herrenkohl EC, Herrenkohl RC, Egolf B. Resilient early school-age children from maltreating homes: outcomes in late adolescence. Am J Orthopsychiatry. 1994;64:301–309. doi: 10.1037/h0079517. [DOI] [PubMed] [Google Scholar]
- 11.Lansford JE, Malone PS, Stevens KI, Dodge KA, Bates JE, Pettit GS. Developmental trajectories of externalizing and internalizing behaviors: factors underlying resilience in physically abused children. Dev Psychopathol. 2006;18:35–55. doi: 10.1017/S0954579406060032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kim J, Cicchetti D. A longitudinal study of child maltreatment, mother-child relationship quality and maladjustment: the role of self-esteem and social competence. J Abnorm Child Psychol. 2004;32:341–354. doi: 10.1023/b:jacp.0000030289.17006.5a. [DOI] [PubMed] [Google Scholar]
- 13.English DJ, Upadhyaya MP, Litrownik AJ, et al. Maltreatment's wake: the relationship of maltreatment dimensions to child outcomes. Child Abuse Negl. 2005;29:597–619. doi: 10.1016/j.chiabu.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 14.Keiley MK, Howe TR, Dodge KA, Bates JE, Petti GS. The timing of child physical maltreatment: a cross-domain growth analysis of impact on adolescent externalizing and internalizing problems. Dev Psychopathol. 2001;13:891–912. [PMC free article] [PubMed] [Google Scholar]
- 15.DuMont KA, Widom CS, Czaja SJ. Predictors of resilience in abused and neglected children grown-up: the role of individual and neighborhood characteristics. Child Abuse Negl. 2007;31:255–274. doi: 10.1016/j.chiabu.2005.11.015. [DOI] [PubMed] [Google Scholar]
- 16.Rubin DM, O'Reilly AL, Luan X, Localio AR. The impact of placement stability on behavioral well-being for children in foster care. Pediatrics. 2007;119:336–344. doi: 10.1542/peds.2006-1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Aarons GA, James S, Monn AR, Raghavan R, Wells RS, Leslie LK. Behavior problems and placement change in a national child welfare sample: A prospective study. Journal of the American Academy of Child and Adolescent Psychiatry. 2010;49:70–80. doi: 10.1097/00004583-201001000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Newton RR, Litrownik AJ, Landsverk JA. Children and youth in foster care: disentangling the relationship between problem behaviors and number of placements. Child Abuse Negl. 2000;24:1363–1374. doi: 10.1016/s0145-2134(00)00189-7. [DOI] [PubMed] [Google Scholar]
- 19.Muthén B. Latent variable analysis: growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. Handbook of Quantitative Methodology for the Social Sciences. Newbury Park, CA: Sage; 2004. pp. 345–368. [Google Scholar]
- 20.Nagin DS. Group-based modeling of development. Cambridge, MA: Harvard University Press; 2005. [Google Scholar]
- 21.Runyan DK, Hunter WM, Socolar RR, et al. Children who prosper in unfavorable environments: the relationship to social capital. Pediatrics. 1998;101:12–18. doi: 10.1542/peds.101.1.12. [DOI] [PubMed] [Google Scholar]
- 22.Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- 23.Sparrow SS, Bella DA, Cicchetti DV. Vineland Adaptive Behavior Scales: Interview Edition, Survey Form Manual. Circle Pines, MN: American Guidance Service; 1984. [Google Scholar]
- 24.Sparrow SS, Carte AS, Cicchetti DV. Vineland Screener: Overview, Reliability, Validity, Administration, and Scoring. New Haven, CT: Yale Child Study Center; 1993. [Google Scholar]
- 25.Wechsler D. Wechsler Preschool and Primary Scale of Intelligence—Revised. San Antonio: The Psychological Corporation; 1989. [Google Scholar]
- 26.English D, LONGSCAN_Investigators. Modified Maltreatment Classification System (MMCS) [December 10, 2009];1997 http://www.iprc.unc.edu/longscan/
- 27.Barnett D, Manly JT, Cicchetti D. Defining child maltreatment: the interface between policy and research. In: Cicchetti D, Toth SL, editors. Child Abuse, Child Development, and Social Policy. Norwood, NJ: Ablex; 1993. pp. 7–73. [Google Scholar]
- 28.Hipp JR, Bauer DJ. Local solutions in the estimation of growth mixture models. Psychological Methods. 2006;11:36–53. doi: 10.1037/1082-989X.11.1.36. [DOI] [PubMed] [Google Scholar]
- 29.Muthén L, Muthén B. Mplus Version 4 User's Guide. Los Angeles: Muthen & Muthén;; 2006. [Google Scholar]
- 30.Bauer DJ. Observations on the use of growth mixture models in psychological research. Multivariate Behavioral Research. 2007;42:757–786. [Google Scholar]
- 31.Yang C. Evaluating latent class analyses in qualitative phenotype identification. Computational Statistics and Data Analysis. 2006;50:1090–1104. [Google Scholar]
- 32.Tofighi D, Enders CK. Identifying the correct number of classes in growth mixture models. In: Hancock GR, Sameulsen KM, editors. Advances in latent variable mixture models. Greenwich, CT: Information Age; 2007. pp. 317–341. [Google Scholar]
- 33.Ethier LS, Lemelin JP, Lacharite C. A longitudinal study of the effects of chronic maltreatment on children's behavioral and emotional problems. Child Abuse Negl. 2004;28:1265–1278. doi: 10.1016/j.chiabu.2004.07.006. [DOI] [PubMed] [Google Scholar]
- 34.English DJ, Graham JC, Litrownik AJ, Everson M, Bangdiwala SI. Defining maltreatment chronicity: are there differences in child outcomes? Child Abuse Negl. 2005;29:575–595. doi: 10.1016/j.chiabu.2004.08.009. [DOI] [PubMed] [Google Scholar]
- 35.Thornberry TP, Ireland TO, Smith CA. The importance of timing: the varying impact of childhood and adolescent maltreatment on multiple problem outcomes. Dev Psychopathol. 2001;13:957–979. [PubMed] [Google Scholar]
- 36.Gjone H, Stevenson J. The association between internalizing and externalizing behavior in childhood and early adolescence: genetic or environmental common influences? J Abnorm Child Psychol. 1997;25:277–286. doi: 10.1023/a:1025708318528. [DOI] [PubMed] [Google Scholar]
- 37.Stahmer AC, Leslie LK, Hurlburt M, et al. Developmental and behavioral needs and service use for young children in child welfare. Pediatrics. 2005;116:891–900. doi: 10.1542/peds.2004-2135. [DOI] [PMC free article] [PubMed] [Google Scholar]