

Abstract
Degenerative mitral valve disease often leads to leaflet prolapse due to chordal elongation or rupture, and resulting in mitral valve regurgitation. Guideline referral for surgical intervention centres primarily on symptoms and ventricular dysfunction. The recommended treatment for degenerative mitral valve disease is mitral valve reconstruction, as opposed to valve replacement with a bioprosthetic or mechanical valve, because valve repair is associated with improved event free survival. Recent studies have documented a significant number of patients are not referred in a timely fashion according to established guidelines, and when they are subjected to surgery, an alarming number of patients continue to undergo mitral valve replacement. The debate around appropriate timing of intervention for asymptomatic severe mitral valve regurgitation has put additional emphasis on targeted surgeon referral and the need to ensure a very high rate of mitral valve repair, particularly in the non-elderly population. Current clinical practice remains suboptimal for many patients, and this review explores the need for a ‘best practice revolution’ in the field of degenerative mitral valve regurgitation.
Keywords: Mitral valve, Valve repair
Introduction
Degenerative mitral valve disease is a common disorder affecting around 2% of the population.1 The most common finding in patients with degenerative valve disease is leaflet prolapse due to elongation or rupture of the chordal apparatus, resulting in varying degrees of mitral valve regurgitation due to leaflet malcoaptation during ventricular contraction. The emphasis of clinical decision-making in patients with degenerative disease centres around the severity of regurgitation and its impact on symptom status, ventricular function and dimension, the sequelae of systolic flow reversal such as atrial dilatation/fibrillation and secondary pulmonary hypertension, and the risk of sudden death.1–4
Controversy exists as to whether early surgical intervention in asymptomatic patients, before the onset of ventricular changes, improves the outcome of patients with chronic severe degenerative mitral valve disease.4–7 This debate has put emphasis on the lack of predictability of mitral valve repair, despite broad consensus that this is the procedure of choice for patients undergoing surgical intervention. The confidence gap in predicting successful mitral valve repair is one of the factors responsible for the lack of adherence to guidelines directed toward timely referral of patients with indications for surgery. An emerging accord is building that current medical and surgical practice often results in suboptimal care for the individual patient with degenerative mitral valve disease, and indeed a paradigm shift or ‘revolution’ through education is not only predictable but essential to advance the field. All practicing cardiovascular specialists should have familiarity with the ‘state of art’ in terms of degenerative disease differentiation, timing of intervention, and surgical techniques and results in order to improve patient care.8
The spectrum of degenerative mitral valve disease
Mitral valve prolapse due to degenerative disease is defined by a spectrum of lesions, varying from simple chordal rupture involving prolapse of an isolated segment (most commonly the middle scallop of the posterior leaflet) in an otherwise normally shaped valve, to multi-segment prolapse involving one or both leaflets in a valve with significant excess tissue and large annular size; thus, a spectrum of degenerative disease is evident in clinical practice, which has important clinical and surgical implications (Figure 1).8–11
Figure 1.

Spectrum of degenerative mitral disease. There is a spectrum of degenerative disease ranging from fibroelastic deficiency (FED) to Barlow's disease. In isolated FED there is a deficiency of collagen, with thin transparent leaflets and typically a ruptured thin chord. In long-standing prolapse, secondary myxomatous pathologic changes may occur in the prolapsing segment, resulting in leaflet thickening and expansion (FED+). Forme fruste designates degenerative disease with excess tissue with myxomatous changes in usually more than one leaflet segment, but usually does not involve a large valve size, distinguishing it from Barlow's disease. In the later, the hallmarks are large valve size, with diffuse myxomatous changes and excess leaflet tissue, with thickened, elongated, and often ruptured chordae.
Fibroelastic deficiency
Fibroelastic deficiency is a condition characterized by Carpentier and co-workers, who realized that not all degenerative valve disease involved giant excess tissue as originally proposed by Barlow in the 1960's.12–13 Carpentier described a condition associated with a fibrillin deficiency which often leads to a rupture of one or more thinned and elongated chordae, usually involving the middle scallop of the posterior leaflet. In selected cases valve segments may appear completely normal with the isolated finding of thinned chordae (Figure 1). In other patients, the prolapsing segment develops myxomatous changes with mucopolysaccharide accumulation in the valve mucosa, causing a proliferative condition of the affected leaflet segment (Figure 1). The key to making the distinction of fibroelastic deficiency rests in the condition of adjacent leaflet segments, which are usually normal or even thinned out with a translucent quality, and are of normal size and height (Figure 2A).9–11 The valve annular size as defined by anterior leaflet surface area (measured with commercially available ring sizers) is generally normal (28–32 mm).11 Patients are typically over the age of 60 years at the time of surgical referral, and have a relatively short clinical history. Echocardiographic findings include an isolated segmental prolapse due to chordal rupture leading to holosystolic mitral regurgitation, evident on echocardiographic imaging (Figure 2B and C).14–15
Figure 2.

Echocardiographic differentiation of degenerative mitral disease. (A) Fibroelastic deficiency with a ruptured thin chord to P3 (posterior lateral scallop). (B) Three-dimensional transoesophageal echocardiography volume rendering of the same valve. (C) Three-dimensional rendering of the same valve from a three-dimensional data set using quantitative analysis (red area corresponds to prolapsing area). (D) Barlow's disease with multi-segment prolapse and excess leaflet tissue. (E) Three-dimensional rendering volume rendering of the same valve. (F) Three-dimensional rendering of the same valve from a three-dimensional data set using quantitative analysis (red areas correspond to prolapsing areas).
Barlow's disease
In contrast to fibroelastic deficiency, Barlow's disease is characterized by diffuse excess tissue (Figure 1).9–11,16–17 Valve size is generally quite large, and multiple segments are usually affected with myxomatous pathological changes, resulting in ‘floppy leaflets’ that are thickened and distended. Diffuse chordal elongation in addition to chordal rupture is the rule as opposed to a simple isolated chordal rupture. Typically the valve size based on anterior leaflet surface area corresponds to a mitral ring size of ≥36 mm. Severe annular dilatation with varying degrees of annular calcification may be observed, and subvalvular fibrosis and calcification of the papillary muscles (usually the anterior papillary muscle) may occur.17 Patients with Barlow's disease are generally younger (<60 years of age) at the time of surgical referral, and typically have a long history of a regurgitant murmur.9–10 Forme fruste was the descriptive label Carpentier gave to certain mitral valves with some but not all pathologic features of Barlow's disease, recognizing there was a spectrum of lesions.10–11 Echocardiographic findings include mid-systolic and often complex regurgitation with multiple jets consistent with diffuse myxomatous disease (Figure 2C and D).14–15 Billowing of one or both leaflets is often seen. The posterior leaflet is often displaced toward the left atrial (LA) free wall away from the ventricular hinge, resulting in a cul-de-sac along the posterior portion of the annulus, which may be a precipitating factor for annular fissures and calcification.17–18
Echocardiographic assessment of mitral regurgitation
Echocardiography is the diagnostic method of choice to assess patients with mitral valve disease. The identification of the aetiology and underlying lesions that result in mitral valve dysfunction is of particular importance for management decisions; patients with degenerative mitral regurgitation should be differentiated from those with other forms of mitral disease such as rheumatic or functional mitral regurgitation. A precise morphologic assessment is necessary to predict the rates of successful reconstructive valve surgery. In most cases, the aetiology and localization of the pathology (assessment of the involved leaflets and segments) can be identified by transthoracic echocardiography.19 A systematic approach is recommended, since a combination of lesions may be contributing to the valve dysfunction and a satisfactory correction requires addressing all of them at the time of surgery. Transoesophageal echocardiography allows a more precise assessment and should be performed when the information obtained by transthoracic echocardiography is insufficient. Intraoperative transoesophageal echocardiography is nowadays systematically performed in mitral repair surgery and provides important information, and allows for an immediate assessment of the operative result. The availability of 3D echocardiography provides additional information to determine the exact localization of lesions.15,20
The echocardiographic quantification of mitral regurgitation severity is sometimes challenging and should comprise an integrative approach of qualitative and quantitative signs.21 Because of its clinical implication, the identification of severe mitral regurgitation is of particular importance. Several parameters that can be categorized into structural, Doppler echocardiographic and quantitative parameters should be assessed and considered together for the quantification of mitral regurgitation severity.21 In addition to quantitative parameters, specific and supportive signs of severity have been defined. Specific signs for the presence of a severe mitral regurgitation include a vena contracta width ≥0.7 cm with a large central regurgitant jet (area >40% of left atrium) or with a wall-impinging jet of any size, a large flow convergence, systolic flow reversal in the pulmonary veins and a prominent flail mitral valve leaflet or ruptured chordal apparatus. Supportive signs include a dense, triangular CW Doppler MR jet, an E-wave dominant mitral inflow (E > 1.2 m/s) as well as an enlarged left ventricular (LV) and LA (particularly with normal LV function). Among the quantitative parameters, an effective regurgitant orifice area ≥40 cm2, a regurgitant volume ≥60 mL, and a regurgitant fraction ≥50% characterize severe mitral regurgitation. Since most of the above measurements have limitations, the information of several factors should be combined. In addition, echocardiography allows assessments of pulmonary arterial pressure and LV size and function, which are all important in the timing of mitral valve surgery. The assessment of the severity of mitral regurgitation should be correlated with clinical evaluation.
Timing of surgery
Surgical intervention for chronic severe mitral valve regurgitation is usually triggered by the occurrence of symptoms, declining LV function, significant LV enlargement, or the development of atrial fibrillation or severe pulmonary hypertension.22–23 Over the past few years the concept of earlier surgical intervention has been proposed, although controversy exists whether asymptomatic patients with severe mitral regurgitation and normal LV function should undergo elective mitral valve repair.4–5,7,24–26 Although the debate regarding asymptomatic patients is ongoing, emerging data suggest a wide clinical practice gap in appropriate referral of patients with guideline-defined indications for surgical intervention; both issues are clarified below.
The debate around patients with asymptomatic severe mitral regurgitation
Enriquez-Sarano et al.4 noted high event rates, including sudden death, in 198 asymptomatic patients with quantitatively graded severe degenerative mitral regurgitation (effective regurgitant orifice area ≥40 mm2), leading them to recommend prompt surgery in such patients. However, in this study patients were not prospectively followed and included some patients with an ejection fraction between 50 and 60%, which would be operated according to recent guidelines. In contrast, Rosenhek et al. published a contemporaneous series involving 132 asymptomatic patients with semi-quantitatively graded severe degenerative mitral regurgitation and noted a good outcome with a watchful waiting strategy. During an 8-year interval, 45% of patients had an event (but not sudden death), with events occurring at a regular pace. Two-thirds of the patients fulfilling indications for surgery became symptomatic, whereas one-third of the patients required surgery because of asymptomatic LV dysfunction or enlargement, or new onset atrial fibrillation or pulmonary hypertension.7 Kang et al.5 published the results of their prospective registry involving 161 asymptomatic patients with semi-quantitatively graded severe degenerative mitral regurgitation who were subjected to early surgery, compared with 268 similar patients managed by watchful waiting over a 9 year period of follow-up. They found a 99% cardiac event-free survival in operated patients, compared with 85% in patients under a strategy of continued medical observation. The cardiac deaths occurring in the group of patients that was initially managed conservatively, however, may have not have been related to conservative strategy; urgent surgery was proposed but refused by five of the six patients who died of congestive heart failure and one sudden death occurred in a patient who had become symptomatic. Nonetheless three cases of sudden death occurred in asymptomatic patients. Montant et al.6 recently examined outcomes in patients with severe degenerative mitral regurgitation by semi-quantitative echocardiographic assessment, reporting on 67 patients managed with a conservative approach and 125 patients subjected to early mitral valve repair. Ten year survival was significantly lower in conservatively managed patients compared with those operated early (50 ± 7% vs. 86 ± 4%, P < 0.0001). Interestingly, these authors also documented better survival and higher referral to surgery in conservatively managed patients seeing cardiologists regularly compared with those with irregular follow-up, but their survival still did not match those subjected to early surgery.
Unfortunately, no attempt was made in any of these studies to differentiate the aetiology of degenerative mitral valve disease, although patients were older in Enriquez-Sarano's study (mean age 63 ± 14 years) and Montant's study (mean age 63 ± 13 years) vs. Rosenhek's study (mean age 55 ± 15 years) and Kang's study (mean age 50 ± 15 years), suggesting that more patients in the Mayo and Brussels series may have had fibroelastic deficiency. The results of Rosenhek et al. emphasized the need for careful patient and echocardiographic assessment in a dedicated valve clinic with strict adherence to guideline referral if a strategy of watchful waiting is undertaken, a point reinforced by Montant's data.
Several additional prognostic factors allowing to risk stratify asymptomatic patients with mitral valve regurgitation have been proposed. Pizarro et al.27 have shown that low brain natriuretic peptide levels (<105 pg/mL) are associated with a stable disease course whereas higher levels may predict an unfavourable outcome. A good exercise tolerance has been shown to be associated with a higher event-rate.28 Left atrial size may also be related to outcome. Recently, Tribouilloy et al.29 have shown that a LV end-systolic diameter ≥40 mm is independently associated with increased mortality under medical management and after surgery. Current European guidelines recommend mitral valve surgery when the LV end-systolic diameter is larger than 45 mm as compared with 40 mm for North American Guidelines and these data favour the latter approach.22–23 Recent data from the Mayo group also suggest superior recovery of long-term LV ejection fraction following early mitral valve repair when the preoperative ejection fraction is ≥65% (current guidelines recommend surgery when the ejection fraction is ≤60%).30
Referral of patients with symptoms and/or left ventricular dysfunction
Symptoms and LV dysfunction are guideline triggers for surgical referral of patients with severe mitral valve regurgitation.22–23 Interestingly, recent studies have documented a widespread discordance in ‘real world’ surgical referral of patients who have an obvious Class I indication for surgery. In 2007, Mirabel et al. found that 49% of patients with symptomatic mitral regurgitation of various etiologies from the Euro Heart Survey were denied surgical referral. Although frequently unjustified, advanced age, co-morbidities, and an abnormal ejection fraction were the arguments used to deny surgery.31 Detaint and colleagues later identified 101 patients within the Euro Heart Survey with isolated severe non-ischaemic mitral regurgitation and found intervention was ‘underused’ in 29 patients (29%) although they had no identified co-morbidities and fulfilled guideline recommendation criteria for surgery.23 Toledano et al.32 surveyed approximately 300 cardiologists in Canada, half of whom were in a university practice whereas the other half were in a community setting to gauge their knowledge of North American referral guidelines of patients with severe mitral valve regurgitation. Nearly 40% of those cardiologists indicated that they would wait for the ejection fraction to fall below 40% or wait for symptoms to occur before referring an asymptomatic patient for surgery with severe mitral valve regurgitation, despite a Class I guideline recommendation for referral if the ejection fraction is equal to or falls below 60%. Recently, Bach et al.33 assessed the frequency at which adult patients at the University of Michigan with severe mitral valve regurgitation documented on an echocardiogram were denied surgery. Fifty-three of 112 patients with severe degenerative mitral regurgitation were not referred for surgery, although 39 of 53 patients (74%) had one or more indications for surgical intervention according to current North American guidelines.22 Interestingly, no patients that were referred to a surgeon for evaluation were thought to have a risk too high for surgical intervention during the study period, yet several patients ‘denied surgical referral’ subsequently died. The authors concluded that much of the ‘perceived risks’ leading to a denial of referral were incorrectly interpreted by cardiologists or other referring physicians. All of these data point towards the need for continued medical education of practicing clinicians to increase familiarity with current guidelines, which will lead to more appropriate referral of patients to surgery.
Who should operate
It is well accepted that the majority of patients with degenerative mitral valve disease who require surgery will have an improved quality of life with less morbidity as well as better long-term survival if a valve repair as opposed to replacement is performed.34–37 This is related primarily to prosthesis-related morbidity, including higher re-operation rates, and the need for aggressive anticoagulation. It is sobering to note that even in developed countries, mitral valve replacement remains frequent in the setting of degenerative disease. Gammie et al.38 reported that the repair rate for patients (n = 47 126) with isolated mitral regurgitation in the Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database rose from 51 to 69% between January 2000 and December 2007. Similar repair rates in the 50% range were documented in the Euro Heart Survey. The reality is that mitral valve replacement continues to be performed far too frequently in the modern era of reconstructive valve surgery.39
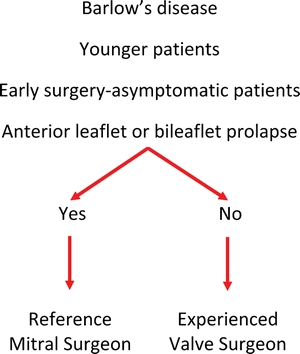
Many recent reports document repair rates in excess of 90% in centres highly skilled in mitral valve repair,40–42 suggesting an ongoing ‘gap’ in best practice surgical care of patients with degenerative disease of at least 20%, which translates into a significant incidence of unnecessary mitral valve replacement. This quality measure reinforces a recommendation in the current North American guidelines: ‘… cardiologists are strongly encouraged to refer patients who are candidates for mitral valve repair, to surgical centers experienced in performing mitral valve repair’.22 Others have suggested that patients with Barlow's valve disease (which typically present with more complex lesions) be specifically targeted for referral to mitral valve ‘reference surgeons’.43–45 Since patients with Barlow's disease are typically younger and therefore likely to have the greatest benefit from valve repair instead of replacement, this strategy seems to be particularly relevant. The localization of leaflet prolapse (posterior, anterior, or bileaflet) is also of prognostic relevance since many reported series suggest much lower repair rates for anterior or bileaflet prolapse compared with posterior leaflet prolapse.45–47 Taking these factors into consideration allows a recommendation for targeted surgeon referral of certain patients with degenerative disease (Table 1).
Table 1.
Targeted surgeon referral: degenerative mitral valve disease
 |
Recent studies have documented that operative mortality rates and perioperative morbidity are lower in high volume mitral surgical centres, providing additional emphasis on a best standard practice of trying to concentrate surgical volume of degenerative mitral valve disease in selected centres.48 Although high volume is also generally associated with higher rates of mitral valve repair, this is not always the case. In a report published early this year from the Society for Cardiothoracic Surgery in Great Britain and Ireland involving over 5000 mitral operations for degenerative disease performed in either country over a 6-year-period, one of the 10 highest volume centres had a mitral valve repair rate of <40%.49 Furthermore, even in high volume mitral repair centres, it is important to differentiate surgical expertise among individual surgeons. In a single-institution series of more than 3200 mitral surgeries, although the institutional repair rate was ∼93%, in a multivariate analysis of the individual surgeon's performances, only one surgeon in this institution was predictive of a higher rate of repair.36
Ongoing assessment of actual vs. predicted repair rates as well as quality of repair judged by residual mitral regurgitation rates are also important quality measures. Today no more than 5–10% of patients should undergo an ‘un-anticipated replacement’ or have more than mild residual regurgitation if operated on in a ‘reference centre’.40 Particularly in the asymptomatic patient, the role of such assessments of quality by means other than mortality rates (which are around 1% in contemporary practice) will take on increasing importance.
Current operative strategies and results
Mitral valve repair operative strategies and techniques continue to evolve, with significant changes seen over the past decade.
Surgical access
Traditionally, mitral valve repair procedures have been performed through a 15–20 cm skin incision and full median sternotomy. Other less invasive approaches, including limited sternotomy or small skin incision (8–10 cm)-full sternotomy, and right sided mini-thoracotomies with or without video assistance (Figure 3) are now successfully performed in many expert centres.41–42,50–52 These approaches are associated with higher patient cosmetic satisfaction; lesser blood transfusion has been reported in some series, at the expense of longer cross-clamp times.
Figure 3.

Mitral surgery via right thoracotomy. The patient is in a supine position, and cannulated for cardiopulmonary bypass via the groin vessels. The valve is exposed through a right mini-thoracotomy and visualization is assisted by a videoscope. Shown in the inset is the aorta clamped, with a caridioplegia needle inserted in the aorta, and the mitral valve as seen by the surgeon with the atrium opened.
The right thoracotomy approach is often used in the redo setting, as it avoids the need for repeat sternotomy and requires less dissection of the heart. Completely endoscopic robotic valve repair has been reported to be feasible and reproducible in expert centres53 and has been embraced in selected high volume centres, particularly in the USA. Higher costs, undocumented benefit, and the extensive learning curve associated with robotic approaches likely explain slow adoption.54
Repair techniques
The goal of a mitral valve repair procedure for degenerative disease follows two fundamental principles: restore a good surface of leaflet coaptation and correct for annular dilatation.55–56 A leaflet coaptation line of 5–8 mm is considered essential to provide a durable repair result. To select the most appropriate repair technique a complete understanding of the underlying degenerative aetiology, anatomical lesions, and leaflet dysfunction (excess or restricted leaflet motion) is mandatory. Intraoperative transoesophageal 2D and increasingly real time 3D transoesophageal echocardiography is applied to guide the procedure and confirm a good result.14–15
In terms of valve repair procedures, two paradigms have emerged with strong proponents. Carpentier's techniques which generally involve resection of abnormal or pathologic tissue with precise reconstruction toward essentially ‘normal valve anatomy’ (Figure 4) remain the most commonly performed world-wide, and are associated with excellent long-term outcomes.10,55–58 In the most common scenario, isolated prolapse of the posterior leaflet is treated by a limited triangular or quadrangular leaflet resection, including the respective elongated or ruptured chordae. The remnant leaflet margins are then readapted using interrupted sutures. If larger resections of abnormal tissue are required such as seen in Barlow's disease, then the annulus is compressed with additional interrupted sutures to narrow its circumference resulting in less tension on residual reconstructed leaflet segments.10 All resections of tissue are targeted to restore the normal height and shape of residual leaflet segments, and to restore the normal relationship of anterior and posterior leaflet surface area to the normal annular dimension for a given patient. This is critical to avoid systolic anterior motion of the anterior leaflet after valve repair.59–60 If residual prolapse remains despite tailored resections of abnormal tissue, then transfer of secondary chords to the free margin of the same segment, or chordal transposition from one segment to another is performed. For example, in the later scenario a ‘flip’ of a small segment of normal posterior leaflet with chords to an opposing segment of a prolapsing anterior leaflet segment can restore normal leaflet motion.61
Figure 4.

Triangular resection and ring annuloplasty. (A) Fibroelastic deficiency with P2 (posterior middle scallop) prolapse. (B) Dashed lines represent area of leaflet to be excised. (C) Reconstructed leaflet after triangular resection. (D) Completed repair after ring annuloplasty.
An emerging paradigm of ‘respect rather than resect’ tissue has become popular in recent years, and is based on the use of polytetrafluoroethylene (PTFE) neochordae to reconstruct support of the free edge of prolapsing segments, and ‘displacing’ abnormal excess tissue into the ventricle to ensure a good surface of coaptation without systolic motion of the anterior leaflet.62–63 Variations of this technique have been described, and a ‘loop technique’ where the PTFE is anchored into a papillary muscle tip and then branches or ‘loops’ are attached to the free edge mimicking a chordal fan is perhaps the most widely used (Figure 4). Depending on the individual anatomy the neochordae are anchored on the anterior or posterior or papillary muscle heads in their fibrous portion, respecting a policy of not crossing the midline or individual native chordae in order to prevent excess traction on the leaflet margin. In the case of significant excess posterior leaflet height, the neochordae are made short enough to displace the prolapsing segment into the left ventricle, to ensure a large surface of coaptation for the anterior leaflet while preventing anterior leaflet displacement in the outflow tract. Early results with have been encouraging and no or limited leaflet resection in combination with PTFE loops is now a preferred technique in many centres today. The simplicity of the technique is particularly relevant in small access incisions where more advanced Carpentier techniques may prove challenging (Figure 5).
Figure 5.

Gore-Tex loop technique and ring annuloplasty. (A) Fibroelastic deficiency with A3 (anterior lateral scallop prolapse). (B) Gore-Tex loops are constructed, and the apparatus is attached to the fibrous tip of the papillary muscle. (C) Individual loops are attached to the prolapsing segment margin. (D) Completed repair after ring annuloplasty.
Calcification of the chordae, papillary muscles, leaflets, and annulus may occur in the setting of degenerative valve disease.17 In general, debridement of calcified tissue is required to restore a good mobility to leaflet tissue, and to ensure an adequate surface of coaptation. Mitral annular calcification can pose a special challenge to valve reconstruction, particularly when it is diffuse. In certain circumstances it is possible to ‘respect’ the calcium, placing pledgeted sutures on the ventricular side of the calcium and passing them through the ring on the atrial side. Sometimes it is necessary to perform an ‘en bloc’ resection of the calcium bar in the annulus, separating the atrioventricular groove.17
Regardless of the leaflet and chordal techniques employed, a prosthetic ring or band annuloplasty that restores the normal circumference and shape of the mitral valve to match the available leaflet tissue is a mainstay of all repair procedures.57,64–65 The fibrous skeleton of the heart is not contiguous around the posterior aspect of the mitral annulus, so long-standing regurgitation associated with ventricular and atrial enlargement leads to pathologic dilatation of the mitral annulus, particularly along the posterior aspect of the valve. Regardless of the type of annular prosthesis (complete ring, partial posterior band; rigid, semi-rigid, or flexible), most surgeons measure the surface of the anterior leaflet with a sizer to estimate the appropriate ring size for the amount of leaflet tissue, although a ‘standard length’ band has been employed by some groups with excellent results.66 Failure to perform an annuloplasty at the time of mitral valve repair is one of the strongest predictors of failure resulting in recurrent moderate or severe mitral valve regurgitation.67 This may have important implications for percutaneous techniques that primarily attempt to address prolapse by attaching opposing leaflets without concomitantly changing the shape of the annulus.
Mitral valve replacement
In contemporary practice at the reference level, mitral valve replacement for degenerative disease in a primary operation should be a rare. Many current reports document repair rates in excess of 90%, regardless of lesions or associated leaflet dysfunction.40–42 The most common scenario for a replacement in a high-volume reference centre should be an end-stage Barlow deformity, typically seen in older patients with long-standing disease. This scenario is actually uncommon, and if identified preoperatively should lead to a careful discussion regarding the possibility of replacement, and assurance that the patient has a Class I indication for surgery. If valve replacement is necessary, annular-papillary continuity should be preserved by performing a chordal sparring procedure.68 Although calcified leaflet segments require resection, non-calcified segments with intact chords are incorporated into the annulus with sutures that are used to implant the prosthesis.
Mitral valve regurgitation following mitral valve repair
All patients undergoing mitral valve repair should have a post-repair intraoperative transoesophageal echocardiogram to determine the immediate success of the procedure.69 A finding of more than mild mitral regurgitation should lead the surgeon, except in certain high-risk patients, to consider valve re-exploration to identify the source of residual regurgitation. The most common reasons for a residual post-repair leak are uncorrected prolapse, separation of a leaflet cleft or indentation, a defect in a leaflet to leaflet closure line, or a perforation of a leaflet from a ring suture near the leaflet hinge. In each of these circumstances, an additional repair technique can address the cause of valve regurgitation leading to a successful result. The other scenario that should be ruled out in residual mitral regurgitation following mitral valve regurgitation is displacement of the anterior leaflet towards the outflow tract. Systolic anterior motion is caused by an excess of leaflet tissue in relation to the orifice area of the mitral valve, and is caused by inappropriate ring sizing, or an excess of residual leaflet height, usually involving the posterior leaflet.59,60 Occasionally systolic anterior motion resolves with volume loading and increasing afterload, but if it is persistent, evidenced by residual mitral regurgitation and a significant outflow tract gradient, the valve should be reoperated on. The main surgical strategies to address systolic anterior motion are leaflet shortening, or posterior leaflet ‘displacement’ of excess leaflet height into the ventricle and out of the orifice using a short PTFE chordae. A larger mitral ring annuloplasty device should also be inserted if there is a question about inappropriate sizing during the initial repair procedure.
All patients undergoing mitral valve repair should also have a pre-discharge transthoracic echocardiogram to assess the repair result under normal loading and pressure conditions.69 Moderate or greater regurgitation should lead the surgeon in most circumstances to consider valve re-exploration after careful risk assessment of the individual patient. It is always better to address residual significant mitral regurgitation at this point, instead of months or years down the road when the re-operation is more complicated due to adhesions.
An annual echocardiogram is usually performed in patients who have undergone successful mitral valve repair. A new mitral regurgitation not seen on early transthoracic follow-up should be categorized as recurrent mitral regurgitation. The most common cause of recurrent mitral regurgitation is progression of the degenerative process which led to the original valve dysfunction. Leaflet shortening or scarring is another potential source of recurrent regurgitation, as is a ring dehiscence. Mitral valve endocarditis, although rare, is also in the differential of recurrent regurgitation following a successful mitral valve repair. Pannus in-growth triggered by the mitral annuloplasty ring is another rare but described cause of failure following a mitral valve repair.70 Haemolysis in the setting of post-operative mitral regurgitation is another possible outcome that could lead to the need for mitral valve re-operation.
Although mitral valve re-repair in the setting of chronic recurrent mitral regurgitation has been reported, it is highly dependent on the surgical expertise of the group performing the procedure.71 In many circumstances a re-repair of the mitral valve is feasible depending on the anatomy and well identified mechanisms of the recurrent mitral regurgitation.
Surgical results
Although freedom from re-operation is very low in degenerative mitral valve surgery (15 year freedom from re-operation is around 95%),55 recent studies have documented the potential for recurrence of significant mitral valve regurgitation. Studies by Flameng et al. and David et al. suggest that a return of moderate to severe mitral regurgitation occurs in 1–2% of patients per year during mid-term follow-up.55,67,72–74 This observation places renewed emphasis on expert mitral surgical repair initially (not only mitigating mitral regurgitation procedurally, but ensuring a long surface of leaflet coaptation to minimize the risks of a late failure), and also on the need to continue to evolve surgical strategies that will optimize long-term mitral valve repair results.
Long-term survival following mitral valve repair is similar to age matched controls provided the operation is done in a timely fashion before the onset of symptoms, ventricular dysfunction or atrial fibrillation.34–35,75–76 Patients undergoing mitral valve surgery with advanced symptoms do poorly compared with less symptomatic patients, so surgery should always be recommended at the onset of symptoms in otherwise low-risk patients. An ejection fraction of ≤60% is a trigger for referral to surgery, as long-term survival is compromised in patients after mitral surgery if the initial ejection fraction is compromised beyond this point. Atrial fibrillation is a more controversial indication for surgical referral, but if present at the time of surgery, patients should probably also undergo a concomitant modified Maze procedure utilizing cryothermy or radiofrequency, although evidence-based data are lacking.77–78 Persistent atrial fibrillation after mitral valve repair is associated with long-term morbidity including stroke as well as mortality, and these patients require careful anticoagulation monitoring.79–80
Best practice revolution
Prevailing data suggest many patients with degenerative mitral valve disease do not receive state-of-the-art care. Accumulating evidence documents a reluctance of many cardiologists and physicians following patients with mitral valve regurgitation to refer them for surgery in a timely fashion, when the maximal benefit from a successful mitral valve repair would be realized. The reasons behind this are certainly multi-factorial, and probably include unawareness of basic concepts in and recent changes to guidelines and a lack of confidence in or poor understanding of modern surgical therapy and results. Both suggest the need for broad continued education with regard to the indications for intervention for mitral valve regurgitation. The implementation of dedicated valve clinics should be encouraged when feasible; a significant outcome benefit can be achieved when experience is widened with larger patient volumes. A close cooperation between internists, imagers, cardiologists, and cardiac surgeons should be promoted, centred on guideline-driven practice.
Despite surgical progress seen in increasing repair rates, lower mortality rates, and less invasive approaches, far too many patients continue to be subjected to unnecessary valve replacement procedures. In this modern era of imaging and degenerative disease differentiation, it should be very uncommon for a patient with mitral valve prolapse to have an unexpected valve replacement based on operative findings; if the surgeon or imager thinks the chances are <90% for a successful repair, they should refer the patient (particularly any asymptomatic patient or a young patient with Barlow's valve disease) to a reference surgeon in a regional reference mitral valve centre; hopefully future evidence of better patient outcomes will support these recommendations and lead to their incorporation into daily practice. There are numerous ‘medical geo-political and financial barriers’ to such a transparency in surgical referral, but the patient with degenerative mitral valve disease deserves the best possible chance for a repair procedure, which is associated with lower long-term morbidity and mortality compared with valve replacement in a majority of patients.
Funding
Funding to pay the Open access publication charges for this article was provided by the Department of Cardiothoracic Surgery, Mount Sinai School of Medicine.
Conflict of interest: D.H.A. is the inventor of mitral annuloplasty rings; has received royalty agreements from Edwards Lifesciences LLC; is co-principal investigator for Medtronic Core-Valve US Pivotal Trial.
References
- 1.Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373:1382–1394. doi: 10.1016/S0140-6736(09)60692-9. doi:10.1016/S0140-6736(09)60692-9. [DOI] [PubMed] [Google Scholar]
- 2.Anders S, Said S, Schulz F, Puschel K. Mitral valve prolapse syndrome as cause of sudden death in young adults. Forensic Sci Int. 2007;171:127–130. doi: 10.1016/j.forsciint.2006.10.011. doi:10.1016/j.forsciint.2006.10.011. [DOI] [PubMed] [Google Scholar]
- 3.Carabello BA. The current therapy for mitral regurgitation. J Am Coll Cardiol. 2008;52:319–326. doi: 10.1016/j.jacc.2008.02.084. doi:10.1016/j.jacc.2008.02.084. [DOI] [PubMed] [Google Scholar]
- 4.Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, Detaint D, Capps M, Nkomo V, Scott C, Schaff HV, Tajik AJ. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Engl J Med. 2005;352:875–883. doi: 10.1056/NEJMoa041451. doi:10.1056/NEJMoa041451. [DOI] [PubMed] [Google Scholar]
- 5.Kang DH, Kim JH, Rim JH, Kim MJ, Yun SC, Song JM, Song H, Choi KJ, Song JK, Lee JW. Comparison of early surgery versus conventional treatment in asymptomatic severe mitral regurgitation. Circulation. 2009;119:797–804. doi: 10.1161/CIRCULATIONAHA.108.802314. doi:10.1161/CIRCULATIONAHA.108.802314. [DOI] [PubMed] [Google Scholar]
- 6.Montant P, Chenot F, Robert A, Vancraeynest D, Pasquet A, Gerber B, Noirhomme P, El Khoury G, Vanoverschelde JL. Long-term survival in asymptomatic patients with severe degenerative mitral regurgitation: a propensity score-based comparison between an early surgical strategy and a conservative treatment approach. J Thorac Cardiovasc Surg. 2009;138:1339–1348. doi: 10.1016/j.jtcvs.2009.03.046. doi:10.1016/j.jtcvs.2009.03.046. [DOI] [PubMed] [Google Scholar]
- 7.Rosenhek R, Rader F, Klaar U, Gabriel H, Krejc M, Kalbeck D, Schemper M, Maurer G, Baumgartner H. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation. 2006;113:2238–2244. doi: 10.1161/CIRCULATIONAHA.105.599175. doi:10.1161/CIRCULATIONAHA.105.599175. [DOI] [PubMed] [Google Scholar]
- 8.Adams DH, Anyanwu AC. Seeking a higher standard for degenerative mitral valve repair: begin with etiology. J Thorac Cardiovasc Surg. 2008;136:551–556. doi: 10.1016/j.jtcvs.2007.10.060. doi:10.1016/j.jtcvs.2007.10.060. [DOI] [PubMed] [Google Scholar]
- 9.Anyanwu AC, Adams DH. Etiologic classification of degenerative mitral valve disease: Barlow's disease and fibroelastic deficiency. Semin Thorac Cardiovasc Surg. 2007;19:90–96. doi: 10.1053/j.semtcvs.2007.04.002. doi:10.1053/j.semtcvs.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 10.Carpentier A, Chauvaud S, Fabiani JN, Deloche A, Relland J, Lessana A, D'Allaines C, Blondeau P, Piwnica A, Dubost C. Reconstructive surgery of mitral valve incompetence: ten-year appraisal. J Thorac Cardiovasc Surg. 1980;79:338–348. [PubMed] [Google Scholar]
- 11.Fornes P, Heudes D, Fuzellier JF, Tixier D, Bruneval P, Carpentier A. Correlation between clinical and histologic patterns of degenerative mitral valve insufficiency: a histomorphometric study of 130 excised segments. Cardiovasc Pathol. 1999;8:81–92. doi: 10.1016/s1054-8807(98)00021-0. doi:10.1016/S1054-8807(98)00021-0. [DOI] [PubMed] [Google Scholar]
- 12.Barlow JB, Pocock WA. The significance of late systolic murmurs and mid-late systolic clicks. Md State Med J. 1963;12:76–77. [PubMed] [Google Scholar]
- 13.Carpentier A, Lacour-Gayet F, Camilleri J. Fibroelastic dysplasia of the mitral valve: an anatomical and clinical entity. Circulation. 1982;3:307. [Google Scholar]
- 14.Adams DH, Anyanwu AC, Sugeng L, Lang RM. Degenerative mitral valve regurgitation: surgical echocardiography. Curr Cardiol Rep. 2008;10:226–232. doi: 10.1007/s11886-008-0038-9. doi:10.1007/s11886-008-0038-9. [DOI] [PubMed] [Google Scholar]
- 15.O'Gara P, Sugeng L, Lang R, Sarano M, Hung J, Raman S, Fischer G, Carabello B, Adams D, Vannan M. The role of imaging in chronic degenerative mitral regurgitation. JACC Cardiovasc Imaging. 2008;1:221–237. doi: 10.1016/j.jcmg.2008.01.011. [DOI] [PubMed] [Google Scholar]
- 16.Barlow JB, Pocock WA. Billowing, floppy, prolapsed or flail mitral valves? Am J Cardiol. 1985;55:501–502. doi: 10.1016/0002-9149(85)90402-3. doi:10.1016/0002-9149(85)90402-3. [DOI] [PubMed] [Google Scholar]
- 17.Carpentier AF, Pellerin M, Fuzellier JF, Relland JY. Extensive calcification of the mitral valve anulus: pathology and surgical management. J Thorac Cardiovasc Surg. 1996;111:718–729. doi: 10.1016/s0022-5223(96)70332-x. discussion 729–730. [DOI] [PubMed] [Google Scholar]
- 18.Hutchins GM, Moore GW, Skoog DK. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N Engl J Med. 1986;314:535–540. doi: 10.1056/NEJM198602273140902. [DOI] [PubMed] [Google Scholar]
- 19.Monin JL, Dehant P, Roiron C, Monchi M, Tabet JY, Clerc P, Fernandez G, Houel R, Garot J, Chauvel C, Gueret P. Functional assessment of mitral regurgitation by transthoracic echocardiography using standardized imaging planes diagnostic accuracy and outcome implications. J Am Coll Cardiol. 2005;46:302–309. doi: 10.1016/j.jacc.2005.03.064. doi:10.1016/j.jacc.2005.03.064. [DOI] [PubMed] [Google Scholar]
- 20.Pepi M, Tamborini G, Maltagliati A, Galli CA, Sisillo E, Salvi L, Naliato M, Porqueddu M, Parolari A, Zanobini M, Alamanni F. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J Am Coll Cardiol. 2006;48:2524–2530. doi: 10.1016/j.jacc.2006.02.079. doi:10.1016/j.jacc.2006.02.079. [DOI] [PubMed] [Google Scholar]
- 21.Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777–802. doi: 10.1016/S0894-7317(03)00335-3. [DOI] [PubMed] [Google Scholar]
- 22.Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e1–e142. doi: 10.1016/j.jacc.2008.05.007. doi:10.1016/j.jacc.2008.05.007. [DOI] [PubMed] [Google Scholar]
- 23.Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A. Guidelines on the management of valvular heart disease: the task force on the management of valvular heart disease of the European society of cardiology. Eur Heart J. 2007;28:230–268. doi: 10.1093/eurheartj/ehl428. [DOI] [PubMed] [Google Scholar]
- 24.Adams DH, Anyanwu AC. Valve Disease: Asymptomatic mitral regurgitation: does surgery save lives? Nat Rev Cardiol. 2009;6:330–332. doi: 10.1038/nrcardio.2009.50. doi:10.1038/nrcardio.2009.50. [DOI] [PubMed] [Google Scholar]
- 25.Detaint D, Iung B, Lepage L, Messika-Zeitoun D, Baron G, Tornos P, Gohlke-Barwolf C, Vahanian A. Management of asymptomatic patients with severe non-ischaemic mitral regurgitation. Are practices consistent with guidelines? Eur J Cardiothorac Surg. 2008;34:937–942. doi: 10.1016/j.ejcts.2008.07.008. doi:10.1016/j.ejcts.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 26.Schaff HV. Asymptomatic severe mitral valve regurgitation: observation or operation? Circulation. 2009;119:768–769. doi: 10.1161/CIRCULATIONAHA.108.832626. doi:10.1161/CIRCULATIONAHA.108.832626. [DOI] [PubMed] [Google Scholar]
- 27.Pizarro R, Bazzino OO, Oberti PF, Falconi M, Achilli F, Arias A, Krauss JG, Cagide AM. Prospective validation of the prognostic usefulness of brain natriuretic peptide in asymptomatic patients with chronic severe mitral regurgitation. J Am Coll Cardiol. 2009;54:1099–1106. doi: 10.1016/j.jacc.2009.06.013. doi:10.1016/j.jacc.2009.06.013. [DOI] [PubMed] [Google Scholar]
- 28.Supino PG, Borer JS, Schuleri K, Gupta A, Hochreiter C, Kligfield P, Herrold EM, Preibisz JJ. Prognostic value of exercise tolerance testing in asymptomatic chronic nonischemic mitral regurgitation. Am J Cardiol. 2007;100:1274–1281. doi: 10.1016/j.amjcard.2007.05.046. doi:10.1016/j.amjcard.2007.05.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tribouilloy C, Grigioni F, Avierinos JF, Barbieri A, Rusinaru D, Szymanski C, Ferlito M, Tafanelli L, Bursi F, Trojette F, Branzi A, Habib G, Modena MG, Enriquez-Sarano M. Survival implication of left ventricular end-systolic diameter in mitral regurgitation due to flail leaflets a long-term follow-up multicenter study. J Am Coll Cardiol. 2009;54:1961–1968. doi: 10.1016/j.jacc.2009.06.047. doi:10.1016/j.jacc.2009.06.047. [DOI] [PubMed] [Google Scholar]
- 30.Suri RM, Schaff HV, Dearani JA, Sundt TM, Daly RC, Mullany CJ, Enriquez-Sarano M, Orszulak TA. Recovery of left ventricular function after surgical correction of mitral regurgitation caused by leaflet prolapse. J Thorac Cardiovasc Surg. 2009;137:1071–1076. doi: 10.1016/j.jtcvs.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 31.Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Detaint D, Vanoverschelde JL, Butchart EG, Ravaud P, Vahanian A. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. 2007;28:1358–1365. doi: 10.1093/eurheartj/ehm001. doi:10.1093/eurheartj/ehm001. [DOI] [PubMed] [Google Scholar]
- 32.Toledano K, Rudski LG, Huynh T, Beique F, Sampalis J, Morin JF. Mitral regurgitation: determinants of referral for cardiac surgery by Canadian cardiologists. Can J Cardiol. 2007;23:209–214. doi: 10.1016/s0828-282x(07)70746-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bach DS, Awais M, Gurm HS, Kohnstamm S. Failure of guideline adherence for intervention in patients with severe mitral regurgitation. J Am Coll Cardiol. 2009;54:860–865. doi: 10.1016/j.jacc.2009.03.079. doi:10.1016/j.jacc.2009.03.079. [DOI] [PubMed] [Google Scholar]
- 34.David TE, Ivanov J, Armstrong S, Rakowski H. Late outcomes of mitral valve repair for floppy valves: Implications for asymptomatic patients. J Thorac Cardiovasc Surg. 2003;125:1143–1152. doi: 10.1067/mtc.2003.406. doi:10.1067/mtc.2003.406. [DOI] [PubMed] [Google Scholar]
- 35.Enriquez-Sarano M, Schaff HV, Orszulak TA, Tajik AJ, Bailey KR, Frye RL. Valve repair improves the outcome of surgery for mitral regurgitation. A multivariate analysis. Circulation. 1995;91:1022–1028. doi: 10.1161/01.cir.91.4.1022. [DOI] [PubMed] [Google Scholar]
- 36.Gillinov AM, Blackstone EH, Nowicki ER, Slisatkorn W, Al-Dossari G, Johnston DR, George KM, Houghtaling PL, Griffin B, Sabik JF, 3rd, Svensson LG. Valve repair versus valve replacement for degenerative mitral valve disease. J Thorac Cardiovasc Surg. 2008;135:885–893. doi: 10.1016/j.jtcvs.2007.11.039. 893 e881–882. [DOI] [PubMed] [Google Scholar]
- 37.Suri RM, Schaff HV, Dearani JA, Sundt TM, 3rd, Daly RC, Mullany CJ, Enriquez-Sarano M, Orszulak TA. Survival advantage and improved durability of mitral repair for leaflet prolapse subsets in the current era. Ann Thorac Surg. 2006;82:819–826. doi: 10.1016/j.athoracsur.2006.03.091. doi:10.1016/j.athoracsur.2006.03.091. [DOI] [PubMed] [Google Scholar]
- 38.Gammie JS, Sheng S, Griffith BP, Peterson ED, Rankin JS, O'Brien SM, Brown JM. Trends in mitral valve surgery in the United States: results from the Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann Thorac Surg. 2009;87:1431–1437. doi: 10.1016/j.athoracsur.2009.01.064. discussion 1437–1439 doi:10.1016/j.athoracsur.2009.01.064. [DOI] [PubMed] [Google Scholar]
- 39.Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231–1243. doi: 10.1016/s0195-668x(03)00201-x. doi:10.1016/S0195-668X(03)00201-X. [DOI] [PubMed] [Google Scholar]
- 40.Adams DH, Anyanwu AC, Rahmanian PB, Abascal V, Salzberg SP, Filsoufi F. Large annuloplasty rings facilitate mitral valve repair in Barlow's disease. Ann Thorac Surg. 2006;82:2096–2100. doi: 10.1016/j.athoracsur.2006.06.043. discussion 2101 doi:10.1016/j.athoracsur.2006.06.043. [DOI] [PubMed] [Google Scholar]
- 41.Gammie JS, Bartlett ST, Griffith BP. Small-incision mitral valve repair: safe, durable, and approaching perfection. Ann Surg. 2009;250:409–415. doi: 10.1097/SLA.0b013e3181b39898. [DOI] [PubMed] [Google Scholar]
- 42.Seeburger J, Borger MA, Falk V, Kuntze T, Czesla M, Walther T, Doll N, Mohr FW. Minimal invasive mitral valve repair for mitral regurgitation: results of 1339 consecutive patients. Eur J Cardiothorac Surg. 2008;34:760–765. doi: 10.1016/j.ejcts.2008.05.015. doi:10.1016/j.ejcts.2008.05.015. [DOI] [PubMed] [Google Scholar]
- 43.Adams DH, Anyanwu AC. The cardiologist's role in increasing the rate of mitral valve repair in degenerative disease. Curr Opin Cardiol. 2008;23:105–110. doi: 10.1097/HCO.0b013e3282f4fe47. doi:10.1097/HCO.0b013e3282f4fe47. [DOI] [PubMed] [Google Scholar]
- 44.Bridgewater B, Hooper T, Munsch C, Hunter S, von Oppell U, Livesey S, Keogh B, Wells F, Patrick M, Kneeshaw J, Chambers J, Masani N, Ray S. Mitral repair best practice: proposed standards. Heart. 2006;92:939–944. doi: 10.1136/hrt.2005.076109. doi:10.1136/hrt.2005.076109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.McCarthy PM. When is your surgeon good enough? When do you need a ‘referent surgeon’? Curr Cardiol Rep. 2009;11:107–113. doi: 10.1007/s11886-009-0017-9. doi:10.1007/s11886-009-0017-9. [DOI] [PubMed] [Google Scholar]
- 46.Manda J, Kesanolla SK, Hsuing MC, Nanda NC, Abo-Salem E, Dutta R, Laney CA, Wei J, Chang CY, Tsai SK, Hansalia S, Yin WH, Young MS. Comparison of real time two-dimensional with live/real time three-dimensional transesophageal echocardiography in the evaluation of mitral valve prolapse and chordae rupture. Echocardiography. 2008;25:1131–1137. doi: 10.1111/j.1540-8175.2008.00832.x. [DOI] [PubMed] [Google Scholar]
- 47.Umakanthan R, Leacche M, Petracek MR, Kumar S, Solenkova NV, Kaiser CA, Greelish JP, Balaguer JM, Ahmad RM, Ball SK, Hoff SJ, Absi TS, Kim BS, Byrne JG. Safety of minimally invasive mitral valve surgery without aortic cross-clamp. Ann Thorac Surg. 2008;85:1544–1549. doi: 10.1016/j.athoracsur.2008.01.099. discussion 1549–1550 doi:10.1016/j.athoracsur.2008.01.099. [DOI] [PubMed] [Google Scholar]
- 48.Gammie JS, O'Brien SM, Griffith BP, Ferguson TB, Peterson ED. Influence of hospital procedural volume on care process and mortality for patients undergoing elective surgery for mitral regurgitation. Circulation. 2007;115:881–887. doi: 10.1161/CIRCULATIONAHA.106.634436. doi:10.1161/CIRCULATIONAHA.106.634436. [DOI] [PubMed] [Google Scholar]
- 49.Bridgewater B, Keogh B, Kinsman R, Walton P. Sixth national adult cardiac surgical database report of great Britain and Ireland. 2009 [Google Scholar]
- 50.Casselman FP, Van Slycke S, Dom H, Lambrechts DL, Vermeulen Y, Vanermen H. Endoscopic mitral valve repair: feasible, reproducible, and durable. J Thorac Cardiovasc Surg. 2003;125:273–282. doi: 10.1067/mtc.2003.19. doi:10.1067/mtc.2003.19. [DOI] [PubMed] [Google Scholar]
- 51.Modi P, Rodriguez E, Hargrove WC, 3rd, Hassan A, Szeto WY, Chitwood WR., Jr Minimally invasive video-assisted mitral valve surgery: a 12-year, 2-center experience in 1178 patients. J Thorac Cardiovasc Surg. 2009;137:1481–1487. doi: 10.1016/j.jtcvs.2008.11.041. [DOI] [PubMed] [Google Scholar]
- 52.Mohr FW, Falk V, Diegeler A, Walther T, van Son JA, Autschbach R. Minimally invasive port-access mitral valve surgery. J Thorac Cardiovasc Surg. 1998;115:567–574. doi: 10.1016/S0022-5223(98)70320-4. discussion 574–566. [DOI] [PubMed] [Google Scholar]
- 53.Chitwood WR, Jr, Rodriguez E, Chu MW, Hassan A, Ferguson TB, Vos PW, Nifong LW. Robotic mitral valve repairs in 300 patients: a single-center experience. J Thorac Cardiovasc Surg. 2008;136:436–441. doi: 10.1016/j.jtcvs.2008.03.053. [DOI] [PubMed] [Google Scholar]
- 54.Cheng W, Fontana GP, De Robertis MA, Mirocha J, Czer LS, Kass RM, Trento A. Is robotic mitral valve repair a reproducible approach? J Thorac Cardiovasc Surg. 2010;139:628–633. doi: 10.1016/j.jtcvs.2009.10.047. doi:10.1016/j.jtcvs.2009.10.047. [DOI] [PubMed] [Google Scholar]
- 55.Braunberger E, Deloche A, Berrebi A, Abdallah F, Celestin JA, Meimoun P, Chatellier G, Chauvaud S, Fabiani JN, Carpentier A. Very long-term results (more than 20 years) of valve repair with carpentier's techniques in nonrheumatic mitral valve insufficiency. Circulation. 2001;104:I8–I11. [PubMed] [Google Scholar]
- 56.Carpentier A. Cardiac valve surgery—the ‘French correction. J Thorac Cardiovasc Surg. 1983;86:323–337. [PubMed] [Google Scholar]
- 57.Carpentier A, Deloche A, Dauptain J, Soyer R, Blondeau P, Piwnica A, Dubost C, McGoon DC. A new reconstructive operation for correction of mitral and tricuspid insufficiency. J Thorac Cardiovasc Surg. 1971;61:1–13. [PubMed] [Google Scholar]
- 58.Filsoufi F, Carpentier A. Principles of reconstructive surgery in degenerative mitral valve disease. Semin Thorac Cardiovasc Surg. 2007;19:103–110. doi: 10.1053/j.semtcvs.2007.04.003. doi:10.1053/j.semtcvs.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 59.Jebara VA, Mihaileanu S, Acar C, Brizard C, Grare P, Latremouille C, Chauvaud S, Fabiani JN, Deloche A, Carpentier A. Left ventricular outflow tract obstruction after mitral valve repair. Results of the sliding leaflet technique. Circulation. 1993;88:II30–II34. [PubMed] [Google Scholar]
- 60.Mihaileanu S, Marino JP, Chauvaud S, Perier P, Forman J, Vissoat J, Julien J, Dreyfus G, Abastado P, Carpentier A. Left ventricular outflow obstruction after mitral valve repair (Carpentier's technique). Proposed mechanisms of disease. Circulation. 1988;78:I78–I84. [PubMed] [Google Scholar]
- 61.Gillinov AM, Cosgrove DM. Chordal transfer for repair of anterior leaflet prolapse. Semin Thorac Cardiovasc Surg. 2004;16:169–173. doi: 10.1053/j.semtcvs.2004.03.005. doi:10.1053/j.semtcvs.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 62.Falk V, Seeburger J, Czesla M, Borger MA, Willige J, Kuntze T, Doll N, Borger F, Perrier P, Mohr FW. How does the use of polytetrafluoroethylene neochordae for posterior mitral valve prolapse (loop technique) compare with leaflet resection? A prospective randomized trial. J Thorac Cardiovasc Surg. 2008;136:1205. doi: 10.1016/j.jtcvs.2008.07.028. discussion 1205–1206. [DOI] [PubMed] [Google Scholar]
- 63.Seeburger J, Kuntze T, Mohr FW. Gore-tex chordoplasty in degenerative mitral valve repair. Semin Thorac Cardiovasc Surg. 2007;19:111–115. doi: 10.1053/j.semtcvs.2007.05.003. doi:10.1053/j.semtcvs.2007.05.003. [DOI] [PubMed] [Google Scholar]
- 64.Carpentier AF, Lessana A, Relland JY, Belli E, Mihaileanu S, Berrebi AJ, Palsky E, Loulmet DF. The ‘physio-ring’: an advanced concept in mitral valve annuloplasty. Ann Thorac Surg. 1995;60:1177–1185. doi: 10.1016/0003-4975(95)00753-8. discussion 1185–1176 doi:10.1016/0003-4975(95)00753-8. [DOI] [PubMed] [Google Scholar]
- 65.Gillinov AM, Cosgrove DM, 3rd, Shiota T, Qin J, Tsujino H, Stewart WJ, Thomas JD, Porqueddu M, White JA, Blackstone EH. Cosgrove-Edwards Annuloplasty System: midterm results. Ann Thorac Surg. 2000;69:717–721. doi: 10.1016/s0003-4975(99)01543-x. doi:10.1016/S0003-4975(99)01543-X. [DOI] [PubMed] [Google Scholar]
- 66.Brown ML, Schaff HV, Li Z, Suri RM, Daly RC, Orszulak TA. Results of mitral valve annuloplasty with a standard-sized posterior band: is measuring important? J Thorac Cardiovasc Surg. 2009;138:886–891. doi: 10.1016/j.jtcvs.2009.01.022. doi:10.1016/j.jtcvs.2009.01.022. [DOI] [PubMed] [Google Scholar]
- 67.Flameng W, Herijgers P, Bogaerts K. Recurrence of mitral valve regurgitation after mitral valve repair in degenerative valve disease. Circulation. 2003;107:1609–1613. doi: 10.1161/01.CIR.0000058703.26715.9D. doi:10.1161/01.CIR.0000058703.26715.9D. [DOI] [PubMed] [Google Scholar]
- 68.David TE, Burns RJ, Bacchus CM, Druck MN. Mitral valve replacement for mitral regurgitation with and without preservation of chordae tendineae. J Thorac Cardiovasc Surg. 1984;88:718–725. [PubMed] [Google Scholar]
- 69.Anyanwu AC, Adams DH. Why do mitral valve repairs fail? J Am Soc Echocardiogr. 2009;22:1265–1268. doi: 10.1016/j.echo.2009.09.024. [DOI] [PubMed] [Google Scholar]
- 70.Ibrahim MF, David TE. Mitral stenosis after mitral valve repair for non-rheumatic mitral regurgitation. Ann Thorac Surg. 2002;73:34–36. doi: 10.1016/s0003-4975(01)03305-7. doi:10.1016/S0003-4975(01)03305-7. [DOI] [PubMed] [Google Scholar]
- 71.Suri RM, Schaff HV, Dearani JA, Sundt TM, 3rd, Daly RC, Mullany CJ, Enriquez-Sarano M, Orszulak TA. Recurrent mitral regurgitation after repair: should the mitral valve be re-repaired? J Thorac Cardiovasc Surg. 2006;132:1390–1397. doi: 10.1016/j.jtcvs.2006.07.018. [DOI] [PubMed] [Google Scholar]
- 72.David TE. Outcomes of mitral valve repair for mitral regurgitation due to degenerative disease. Semin Thorac Cardiovasc Surg. 2007;19:116–120. doi: 10.1053/j.semtcvs.2007.04.004. doi:10.1053/j.semtcvs.2007.04.004. [DOI] [PubMed] [Google Scholar]
- 73.David TE, Ivanov J, Armstrong S, Christie D, Rakowski H. A comparison of outcomes of mitral valve repair for degenerative disease with posterior, anterior, and bileaflet prolapse. J Thorac Cardiovasc Surg. 2005;130:1242–1249. doi: 10.1016/j.jtcvs.2005.06.046. doi:10.1016/j.jtcvs.2005.06.046. [DOI] [PubMed] [Google Scholar]
- 74.Flameng W, Meuris B, Herijgers P, Herregods MC. Durability of mitral valve repair in Barlow disease versus fibroelastic deficiency. J Thorac Cardiovasc Surg. 2008;135:274–282. doi: 10.1016/j.jtcvs.2007.06.040. [DOI] [PubMed] [Google Scholar]
- 75.Enriquez-Sarano M, Tajik AJ, Schaff HV, Orszulak TA, Bailey KR, Frye RL. Echocardiographic prediction of survival after surgical correction of organic mitral regurgitation. Circulation. 1994;90:830–837. doi: 10.1161/01.cir.90.2.830. [DOI] [PubMed] [Google Scholar]
- 76.Enriquez-Sarano M, Tajik AJ, Schaff HV, Orszulak TA, McGoon MD, Bailey KR, Frye RL. Echocardiographic prediction of left ventricular function after correction of mitral regurgitation: results and clinical implications. J Am Coll Cardiol. 1994;24:1536–1543. doi: 10.1016/0735-1097(94)90151-1. doi:10.1016/0735-1097(94)90151-1. [DOI] [PubMed] [Google Scholar]
- 77.Lee AM, Melby SJ, Damiano RJ., Jr The surgical treatment of atrial fibrillation. Surg Clin North Am. 2009;89:1001–1020. doi: 10.1016/j.suc.2009.06.001. x–xi. doi:10.1016/j.suc.2009.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Lee R, Kruse J, McCarthy PM. Surgery for atrial fibrillation. Nat Rev Cardiol. 2009;6:505–513. doi: 10.1038/nrcardio.2009.106. doi:10.1038/nrcardio.2009.106. [DOI] [PubMed] [Google Scholar]
- 79.Eguchi K, Ohtaki E, Matsumura T, Tanaka K, Tohbaru T, Iguchi N, Misu K, Asano R, Nagayama M, Sumiyoshi T, Kasegawa H, Hosoda S. Pre-operative atrial fibrillation as the key determinant of outcome of mitral valve repair for degenerative mitral regurgitation. Eur Heart J. 2005;26:1866–1872. doi: 10.1093/eurheartj/ehi272. doi:10.1093/eurheartj/ehi272. [DOI] [PubMed] [Google Scholar]
- 80.Itoh A, Kobayashi J, Bando K, Niwaya K, Tagusari O, Nakajima H, Komori S, Kitamura S. The impact of mitral valve surgery combined with maze procedure. Eur J Cardiothorac Surg. 2006;29:1030–1035. doi: 10.1016/j.ejcts.2006.03.028. doi:10.1016/j.ejcts.2006.03.028. [DOI] [PubMed] [Google Scholar]