

Abstract
Objective
American Indian youth experience a greater prevalence of obesity compared with the general U. S. population. One avenue to reverse the trend toward increasing obesity prevalence is through promoting physical activity. The goal of this project was to understand tribal youth’s current patterns of physical activity behavior and their beliefs and preferences about physical activity.
Design
This assessment used a community-based participatory research approach.
Sample
Thirty-five Native youth ages 8-18.
Measurements
A Community Advisory Board was created that developed an exercise survey specifically for this assessment to explore physical activity patterns, preferences, and determinants. Twenty-six youth completed the survey. Descriptive statistics were analyzed, exploring differences by age group. Nine youth participated in 2 focus groups. Qualitative data were analyzed with thematic analysis.
Results
Youth distinguished between sports and exercise with each possessing different determinants. Common motivators were friends, coach, school and barriers were lack of programs and school or work. None of the youth reported meeting the recommended 60 minutes of strenuous exercise daily.
Conclusions
This tribal academic partnership responded to a tribal concern by developing an exercise survey and conducting focus groups that addressed tribal specific questions. The results are informing program development.
Keywords: Community-based participatory research, American Indian, physical activity, youth, tribal communities
American Indians (AIs) suffer a disparity in health; in particular, AIs suffer a greater burden from diabetes compared to the general US population (Indian Health Service [IHS], 2003; Liao et al., 2004). Historically, AIs had low rates of diabetes; however, during the last 20 years their rate of diabetes has risen dramatically and diabetes is now their fourth leading cause of death (IHS, 2003). The prevalence of diabetes is approximately 3 times greater and the death rate from diabetes is threefold higher in AIs compared with non-Hispanic whites (Denny, Holtzman, & Cobb, 1998; IHS, 2002). In the last 20 years, AI adolescents also have experienced disproportionate disease burden from diabetes. During the 1990s the prevalence of type-2 diabetes rose by 46% among AI adolescents aged 15-19 years compared with 14% for the general US population (Acton et al., 2002; IHS, 2003; Liao et al.).
Obesity in adolescence is associated with increased mortality from diabetes in adulthood (Daniels et al., 2005). Forty-four percent of AIs aged 5-13 are overweight (BMI > 85 percentile) and obese (BMI > 95 percentile) (Zephier, Himes, Story, & Zhou, 2006). Curtailing overweight or obesity in AI adolescents can prevent type-2 diabetes and its harmful consequences in adulthood. One avenue to curtailing obesity is through promoting physical activity.
Cognizant of these disparities, a northwest tribal community has made promoting physical activity a priority for preventing obesity, diabetes, and other chronic illness. The tribe offers several programs designed to encourage physical activity among children, adults, and elders. Program success is measured by attendance. The programs have had varying levels of attendance and therefore success. The existing programs, however, have stimulated only minimal interest among tribal youth, generating community concern about youth’s level of physical activity. The purpose of this study was to assess youth’s current level of physical activity and evaluate current programming for youth.
American Indian Experiences with Research
American Indians have been the subject of, and participated in thousands of studies over the past 20 years; however, during that time AI tribal communities experienced little or no improvement in their overall health. In some cases, research projects carried out by academics have resulted in more harm than benefit for tribal communities. For example, in the late 1970s the lay press reporting on results of a research study, which examined the rate of alcohol use among the primarily Inupiaq residents of Barrow Alaska. The reporters portrayed that Inupiaq community as irresponsible alcoholics (Foulks, 1989). Consequently, the Native community was not able to obtain financing to support necessary community projects, ultimately harming the community (Manson, Garroutte, Goins, & Henderson, 2004). In a more recent case, blood samples were drawn from Havasupai tribal members in the early 1990s for research examining a genetic link that might have explained the high prevalence of diabetes among the Havasupai. Over the next decade, the blood samples were shared with researchers at multiple institutions to examine genetic links with schizophrenia, inbreeding, and migratory patterns unbeknownst to the Havasupai (McGregor, 2007). In 2004 the Havasupai became aware of this unauthorized use of data and filed a lawsuit against the involved universities (Dalton, 2004); however the judge overseeing the case dismissed it (Associated Press, 2007).
Community-Based Participatory Research
In response to these and other cases, many tribal communities mistrust university researchers and are reluctant to embark on a research project with universities. Community-based participatory research (CBPR) offers the opportunity to establish trust within tribal communities, which have a history of unfavorable research experiences with academics (Burhansstipanov, Christopher, & Schumacher, 2005; Caldwell et al., 2005; Fisher & Ball, 2003). In CBPR, community members affected by the issues under study are actively involved in all aspects of a research project and share decision-making power about data collection and the development and implementation of interventions designed to address the influences on a particular health issue (Schultz, Krieger, & Galea, 2002). Adopting a CBPR approach in tribal communities involves considering the historical and cultural context for a tribal community, for example, historical trauma (Caldwell et al.; Fisher & Ball). A participatory research approach has been shown to improve data quality and community ownership of research endeavors (Farquhar, Parker, Schultz, & Israel, 2006; Gittelsohn et al., 2006). Although time intensive, CBPR increases the likelihood of addressing issues salient to the community and developing programs that are sustainable and in concert with community values and resources.
Working with Tribal Communities
Tribal communities have begun working in partnership with academic researchers using a CBPR approach so that research is done with them rather than to them. A truly equitable partnership in which tribal values and knowledge are respected and tribal members have equal decision-making power is requisite to conducting research with tribal communities. Tribal communities are exerting control as sovereign nations over research that takes place with their members or in their jurisdiction. The Navajo Nation, for example, established an Institutional Review Board (IRB) responsible for approving and monitoring research conducted with their tribal community (Brugge & Missaghian, 2006). Other nations have followed this precedence by establishing formal research review processes. The tribal review process emphasizes protection of the community as a whole whereas the university IRB process typically addresses risks to individuals. This tribal review is an additional step that involves extra time and needs to be taken into account when planning research projects with tribal communities.
Study Objectives
This CBPR program evaluation and development project was undertaken in two phases. The first phase involved developing community relationships, establishing an academic-community partnership, and determining priorities. The second phase involved conducting a baseline assessment of community needs by understanding level and type of physical activity and motivators associated with youth physical activity in this community. The objectives of this 15-month project were to 1) assess tribal youth’s current level and patterns of physical activity, 2) delineate preferences and determinants for physical activity, and 3) explore beliefs and definitions about physical activity and 4) explore ideas on how to motivate youth to be active. Our goal was to enhance existing physical activity programming aimed at tribal adolescents.
Methods
Design and Sample
Tribal Community
The tribal community has approximately 1,000 members. The rural tribal reservation comprises approximately 7,486 acres. All enrolled tribal members are part of the Tribal General Council. Those who are eligible to vote elect 7 tribal members to 3-year terms on the Tribal Council. The Tribal Council is the governing body for the tribe. The Youth Council is advisory to the Tribal Council and its members are elected by youth eligible to vote. The tribe was interested in learning youth’s current patterns of physical activity and their determinants for physical activity in order to assess current programming and assist in future program development.
The Collaborative Process
Several preliminary steps were undertaken prior to initiating work with the tribal community involved in this project (Table 1). First the investigator met with individual members of the tribal community to discuss issues of concern, ascertain needs of the tribal and academic communities, and to establish goals for the project. The investigator then submitted a grant application for research funding and received grant funding for 12 months. Next, the investigator discussed the project with the Tribal Youth Council, which expressed interest in and a desire to work on the project. Then, the investigator presented the project to the Tribal Council along with members of the Youth Council. The Council members gave input into project goals and voted to approve working with the youth on this project. Finally, documents were submitted for review and approval by the university IRB, which gave approval to work with the community.
Table 1.
Steps in the Collaborative Research Process
| Step in Research Process | Schedule (in months) |
|---|---|
| 1: Discussed project ideas with community health nurse | 1 |
| 2: Discussed project ideas with few tribal members | 1-2 |
| 3: Submitted application for research funding and received funding | 2-4 |
| 4: Discussed project with Youth Council & received endorsement | 5 |
| 5. Presented project to Tribal Council & received approval | 6 |
| 6. IRB submission, review, and approval | 6-8 |
| 7. Established Community Advisory Board (CAB) | 8 |
| 8. CAB finalized study procedures | 8-15 |
| 9. Tribal Council approved poster presentation | 12 |
| 10. Youth Council endorsed study procedures | 15 |
| 11. Preparation and approval Data Sharing Agreement | 15 |
| 12. Tribal Council approved study procedures | 16 |
| 13. No cost extension grant funding requested and approved | 16 |
| 14. IRB submission, review and approval | 17 |
| 15. CAB member administered Exercise Survey | 17 |
| 16. Conducted focus groups | 18-19 |
| 17. Audiotapes transcribed & reviewed, data entry & data analysis | 20-21 |
| 18. CAB member reviewed & commented on data analysis | 21 |
| 19. Preparation final report and manuscript | 22-24 |
| 20. Final report presentation to & discussion with Tribal Council | 23 |
A Community Advisory Board (CAB) was established in which all members were involved in decision-making. Members included the investigator and four members from the community; one was a member of the Tribal Council, one was a member of the Youth Council and two were non-tribal employees. We discussed an idea until consensus was reached. Over the course of eight months the CAB met on average twice a month developing study measures and finalizing study procedures. Final measures and procedures agreed upon by the CAB were presented to the Tribal Youth Council and the Council affirmed its interest in working on the project. Then, final measures and procedures were presented to the Tribal Council for review. At this point the Tribal Council (serving as the Tribal IRB) requested the development and approval of a Data Sharing Agreement in order to protect the interests of the community. Over the next two months we developed a mutually acceptable agreement.
Data sharing agreement
This agreement delineated the type of data that were collected (e.g. exercise patterns), how data were collected (e.g. survey, focus groups), and how data were to be handled to protect confidentiality, including decisions about who has access to the data. A key provision was that the tribe and the university jointly owned and had control over the data generated. Thus, both the tribe and the university needed to provide approval before the data are used for future research or educational purposes. Additionally, the Tribal Council has the right to restrict public dissemination of the data. These provisions protect the tribal community from harm resulting from data being used without their knowledge (as occurred in the aforementioned Havasupai case), from misrepresentation, and from exposure of confidential data (such as occurred with Inupiaq community). Once the terms of the agreement were approved, the Tribal Council chair and the investigator signed the agreement and the Tribal Council approved moving forward with the project.
Once the Tribal Council gave approval for data collection, the study procedures, including the data sharing agreement, were submitted to the university IRB and approved, leading to data collection. Upon completion of data collection and analysis, the investigator prepared a report outlining the findings and offering suggestions for program development and presented it to the Tribal Council. The report was reviewed and approved by one of the CAB members prior to the presentation. The findings generated a great deal of discussion among the Tribal Council and tribal members attending the presentation, particularly regarding how to best proceed with program planning based on the findings.
In compliance with the Data Sharing agreement, the investigator brought the documents intended for public dissemination to the Tribal Council for review and approval. Early in this study, the Tribal Council reviewed and approved a poster presentation for a regional nursing research conference that described the CBPR process and steps undertaken at that time point with the tribe. The Tribal Council added additional information for the presentation strengthening its quality. A draft of this paper was submitted to the Tribal Council. The Tribal Council reviewed, commented on, and approved this paper.
Sample
Study participants were recruited using flyers placed in strategic locations in the community frequented by youth, as well as by word of mouth. Twenty-six youth aged 8-18 were recruited to complete the exercise survey. After surveys were completed and analyzed nine youth were recruited via flyers and word of mouth to participate in one of two focus groups. Participants were compensated for their time: $5 to complete the exercise survey, and $20 for participating in a focus group.
Data Collection
Data were collected from exercise surveys in order to gather general data on physical activity patterns, preferences and determinants from a broad representation of the tribal youth. Focus groups were conducted to gain more detailed data and to clarify information collected from the surveys.
Measures
Exercise survey
Initially the CAB reviewed widely used physical activity recall questionnaires with established validity and reliability; however, these questionnaires did not provide the information that the tribe was interested in exploring. Therefore, we collaborated in developing a questionnaire that met the needs of the tribal community. In concert with the principles of CBPR, our goal was to conduct a survey that would provide meaningful data for tribal community to use in program planning.
The questionnaire was specifically designed for this community and was used in this evaluation to ask about favorite and least favorite types of exercise, barriers and facilitators of exercise, and a limited number of demographic questions. The barriers and facilitators listed on the survey were based on the youth CAB member’s interactions with youth at the Youth Center. Respondents were asked to recall their physical activity participation over the last week and to record the time, intensity, and type of exercise (from a list of 34 types, including cultural activities). Mild exercise was defined as minimal effort, moderate was defined as sweating and breathing deeply and vigorous was defined as heart beating rapidly. Because the key phenomena of interest were the preferences, patterns, and determinants of exercise among the youth, the exercise survey was not designed to calculate weekly energy expenditure, but to provide an approximation of minutes of activity per week. One of the CAB tribal members administered the survey. Identifying information was not asked about or written on the survey.
Focus groups
To expand on findings from the Exercise Survey, two focus groups, one with 8-11 year olds and one with 15-18 year olds were conducted. The CAB developed a separate focus group guide for each age group. In the younger age group youth were asked to draw pictures of physical activities that they enjoyed. Then they were asked to describe a typical weekday and weekend day to ascertain engagement in type and amount of physical activity. In the older age group youth were asked direct questions about preferences, determinants, and patterns of exercise, and their ideas regarding how to encourage youth to become more physically active.
Analytic Strategy
The quantitative survey data were entered into SPSS (Version 15, Chicago, IL). Descriptive statistics were calculated. Differences by age group were explored using cross tabulations and chi square tests, p < .05.
Qualitative data collected from the focus groups were analyzed using qualitative descriptive analysis. This analytic approach typically stays closer to the data than other interpretive qualitative methods and does not require highly abstract analysis of data (Sandelowski, 2000). Data were coded inductively based on concepts that reflect participant’s ideas and experiences (e.g. description sports, motivation), and categorized into main themes. Two verification procedures were used to establish credibility of the qualitative analysis and reduce potential biases (Denzin & Lincoln, 2000). First, a qualitative researcher, who was not involved in the data collection or analysis, reviewed the focus groups transcripts, inductively coded the data and sorted the codes into themes. Then, this researcher and the investigator met to review codes and themes, to discuss the meaning of the themes, and to determine that the themes were an accurate representation of the participants’ ideas. Differences in coding were resolved by reading the text of the transcript together and discussing the meaning of the text until consensus was reached. Second qualitative data were triangulated with the quantitative data. We examined information reported on the exercise surveys, for example favorite types of physical activity, and determined that the information in the surveys corroborated the themes from the focus groups.
Results
Table 2 reports the characteristics for the 26 youth who completed the exercise survey. Data on preferences and determinants of physical activity were from the exercise survey completed by 26 youth and from five youth aged 8-11 and four youth aged 15-18 who participated in a focus group. Data on physical activity definition, beliefs, and opinions on how to motivate youth to be active were from four youth aged 15-18 who participated in a focus group. These later data are reported based upon the key themes of exercise and sports are different, exercise for health, and motivate for sports not exercise.
Table 2.
Exercise Survey Respondent Characteristics (N=26)
| Characteristic | Number |
|---|---|
| Age: mean, (SD) | 13.5 (3) |
| Gender | |
| Male | 16 |
| Female | 10 |
| Age Group | |
| Elementary School (ages 8-11) | 8 |
| Middle School (ages 12-14) | 5 |
| High School (ages 15-18) | 9 |
| Live on Reservation | 24 |
| Live in tribal housing | 18 |
| Tribal members | 18 |
| Members of other tribes | 5 |
| Non tribal members | 3 |
Physical Activity Levels and Patterns
There was considerable variation in the number of minutes spent in physical activity per week. On average youth spent 77 minutes (SD = 65, median 60) in strenuous and 146 minutes (SD = 85, median 120) in moderate exercise per week. The tribal youth did not meet the recommended amount of 60 minutes of moderate to strenuous physical activity per day, which is 420 minutes per week. Elementary school youth were more active than middle school and high school youth (Table 3). The majority of time the youth spent in strenuous exercise was not spent in a favorite exercise (Table 3).
Table 3.
Mean, Standard Deviation, and Range of Minutes per Week of Physical Activity by Intensity per Gender and Age Group
| Intensity of Activity | Females, N=10 M (SD) Range | Males, N=16 M (SD), Range | Elementary, N=8 M (SD), Range | Middle, N=5 M (SD) Range | High, N=9 M (SD), Range |
|---|---|---|---|---|---|
| Strenuous | 73 (64), 4-180 | 80 (68), 10-240 | 101 (53), 60-180 | 32 (16), 20-60 | 71 (79), 10-240 |
| Favorite strenuous | 84 (90), 0-240 | 49 (69), 0-240 | 90 (72). 0-180 | 88 (96), 0-240 | 25 (41), 0-120 |
| Moderate | 134 (91), 30-300 | 155 (86), 20-270 | 135 (75), 60-240 | 127 (99), 30-240 | 197 (73), 120-300 |
| Favorite moderate | 24 (50), 0-120 | 2 (7), 0-30 | 15 (42), 0-120 | 6 (13), 0-240 | 13 (40), 0-120 |
Note: when the sample size within a sub group is small and the range within a subgroup is large then the standard deviation could likely be greater than the mean.
Physical Activity Preferences and Determinants
Preferences
Thirteen youth identified running, nine identified basketball and six identified weight lifting as a favorite exercise. In both focus groups, youth confirmed that running was the most common form of exercise and reported that running was most often done alone rather than with a friend or a group. The top two favorite sports identified by elementary aged youth were running (n=4) and basketball (n=4); by middle school youth the favorites were running (n=3) and basketball (=2); and by high school favorites included running (n=4) and weight lifting (n=3). The least favorite form of exercise reported by elementary aged youth were strengthening exercises (n=3) and running (n=2); by middle school aged were baseball (n=1), jogging (n=1), and strengthening (n=1); and by high school aged was running (n=2).
Determinants
The most frequently cited motivators for exercise were friends, a coach, and school or team; the most frequently cited barriers included age, work or school, lack of programs, and lack of time (Figures 1 and 2). Structured physical activity programs in the tribal community targeted certain age groups, such as preschoolers, but not all age groups. Among elementary school aged youth lack of time was the predominant barrier. All participants in the focus group of youth aged 8-11 described a typical day in which most of their time was scheduled and involved sedentary activities without any planned physical activities. They reported little free time in the day and they spent their free time in sedentary rather than physical activities. For instance, one elementary aged youth described a typical day beginning with waking up, having breakfast, going to school, going to homework club, going home and watching television or playing computer games, having diner, watching television or playing video games, and then going to bed.
Figure 1.
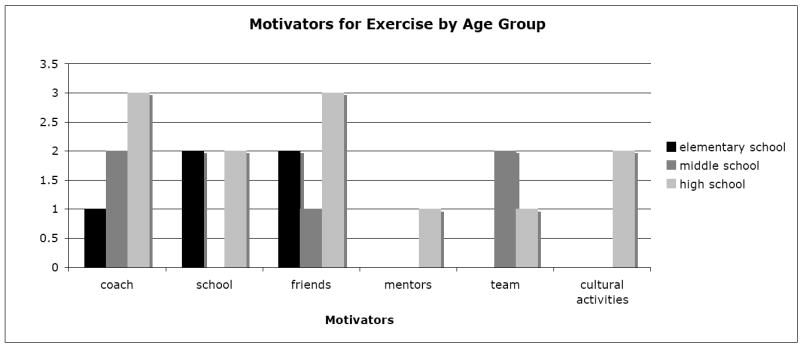
Motivators to Physical Activity by Age Group
Figure 2.
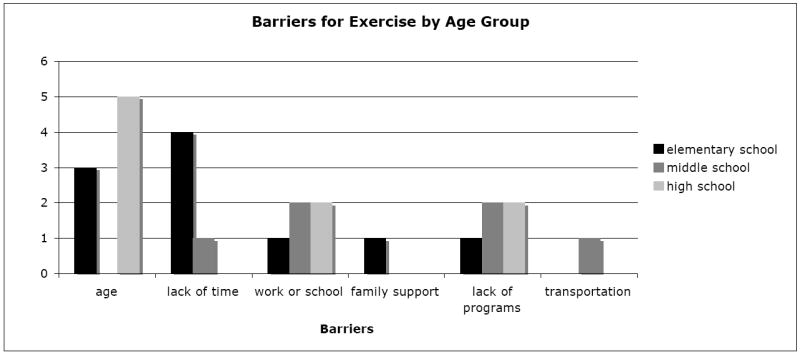
Barriers to Physical Activity by Age Group
Definitions and Beliefs about Physical Activity
Exercise and Sports are Different
Youth differentiated between the terms ‘exercise’ and ‘sports.’ All of the youth defined exercise as moving and working the body. They described exercise as work, which results in feeling tired and out of breath yet energized. Typical exercises identified included jumping rope, running, and strengthening exercise (e.g. crunches, push-ups). Participant A stated, “when I think of exercise, it’s kind of like push-ups and all that crap.” All the youth identified running as the most common form of exercise. Three of the youth described exercisers as those individuals who have made a personal choice to exercise and motivate themselves because they want to realize the benefits from exercising.
All the youth described sports as fun and sociable. They identified basketball, baseball, canoe pulling, and dancing as the most common sports. They reported perceptions that most youth participate in a team sport, such as basketball, because they want to support and be part of a team. They noted their observations that youth who do not exercise typically walk rather than run during a team sport, because they are in poor condition. Participant B summed it up, “Youth do sports; they just don’t exercise.”
Exercise for Health
The four older youth (15-18 years) were aware of the importance of establishing a habit of exercising regularly and the consequences of not exercising regularly, such as increased risk of obesity and diabetes. All expressed the understanding that if one does not exercise, then one is more likely to become “out of shape” and overweight, making it much more difficult to start exercising. Participant C stated,
Exercising makes a lot of things easier. And when you get older you won’t feel so physically [weak]-if you’re lazy when you’re younger and you just sit down, you’ll probably be like that when you get older too. But if you run when you’re younger and stay in shape, you’ll stay in shape when you’re older too.
They identified other benefits of exercise including improved mood and maintaining health, weight, and fitness.
How to Motivate Youth
Motivate for Sports not Exercise
Youth agreed that encouraging team involvement and interaction could motivate youth to play on a sports team. Being a team member provides a reason to gather, socialize and “hang out together.” Playing the sport is necessary to be a team member. They acknowledged that participating in a team sport involved exercise, such as running, and that sports participation made exercise fun. Participant D commented,
Like playing basketball makes exercise fun, because you’re running and its fun.
Like football makes exercise fun, sports makes it fun if you’re playing sports you have to run.
The youth discussed at length the issue of how to motivate other youth to exercise. They offered a variety of strategies. One suggested posting flyers with messages about health and exercise; another suggested mailing information to each family with children; and another suggested giving a class that describes the benefits of exercise and what happens when you do not exercise. They acknowledged that motivating youth to exercise is complex and this complexity stems from the diversity in beliefs and behaviors among individuals. Ultimately they concluded that each individual must decide whether or not to exercise. Participant C summed up the group’s conclusion:
I don’t know that you can make youth exercise. Everybody has their own perspective on how they see exercise and how they would get in shape or what they do to stay in shape or what they do to sit and be lazy. It’s up to you; what motivates you; what pushes you to do it.
Programming Changes as Result of Assessment
Since the results of this assessment were reported to the tribe, tribal members and staff have moved programs from the development to implementation stage in a relatively short time. Results were presented during an open session of a Tribal Council meeting in which any tribal member could attend and participate in a discussion regarding the findings. There was a lively discussion after the assessment findings were presented regarding programming and supporting youth to be physically active. A written report of the evaluation with recommendations was provided to the Tribal Council. The staff and youth working at the youth center had considered implementing structured physical activity groups for 8 to 11 years old boys and girls to be held at the youth center. In response to the evaluation a boys’ and girls’ basketball group was initiated and is well attended. Other recreational team activities such as baseball and wrestling are being planned. Two years ago the tribe launched the evidenced-based Sports, Play and Active Recreation for Kids (SPARK) program developed by Sallis and colleagues (1997) with preschool children. This program has recently been incorporated into after school club programming for elementary aged youth and held at the early learning center. Funding was secured to purchase equipment and train staff through an Indian Health Service (IHS) Child and Youth Program grant. The tribal community is also planning to integrate the SPARK program into activities held at the youth center. The tribe has decide to make funds available to tribal youth in order to cover the cost of fees and uniforms required for tribal youth to participate in non-tribal recreation league teams. There are recreational leagues available in the nearby town for boys and girls aged 6-12 in baseball, soccer, and basketball. Other non-tribal opportunities for physical activity include daily 20-minute recess for elementary students and twice weekly physical education class for high school students. The tribe is exploring other way to promote physical activity within the tribal community including building walking trails that connect with the county trail system, family field days to teach traditional games, and integrating playing traditional games during community events (e.g. annual General Council meeting).
Discussion
This study used a CBPR approach to identify patterns of physical activity and barriers and motivators for physical activity in tribal youth. In concert with CBPR, a culturally specific instrument was developed by the researcher-community team to collect data. In this tribal community youth differentiated exercise and sports and identified different motivators and barriers for both exercise and sports. Some of these differed from barriers and motivators in other populations of youth. They defined exercise as work that resulted in multiple benefits such as improved mood, health, stable weight, conditioning, and strength. They defined sports as fun, team oriented and sociable. They realized that by participating in sports one is actually exercising and receiving the benefits of exercise. The tribal community is using the findings from this assessment to develop physical activity programs that are tailored to and salient for this community’s youth. Using a CBPR approach for the program evaluation promises to enhance the likelihood that these and similar programs will increase physical activity among tribal youth.
In this tribal community none of the 26 youth reported meeting the recommended amount of physical activity, 60 minutes of moderate to vigorous physical activity every day. A recent national study used accelerometers to measure physical activity and found that 42% of youth aged 6-11 and 8% youth aged 12-19 met the physical activity recommendations (Troiano et al., 2008). Nationally 34% of high school aged youth reported meeting the recommended amount of physical activity (Eaton et al., 2008). The youth in this tribal community reported being much less active than the national average. A lower level of physical activity among youth in various AI communities compared with youth in the general population has been a consistent finding (Gordon-Larsen, McMurray, & Popkin, 1999). This observed lower level of physical activity might be due to differences in the measures used to assess the amount and patterns of physical activity and/or to the small sample size. Younger youth were more active than older youth, consistent with findings on the national level (Nader, Bradley, Houts, McRitchie, & O’Brien, 2008).
A recent examination of accelerometer data from National Health and Nutritional Survey 2003 and 2004 data found that youth spent over 50% of their waking hours in sedentary activities (Matthews et al., 2008). These tribal youth reported spending over 50% of their day in sedentary activities. It appeared that youth spend most of their time in sedentary behavior in part because a majority of their time was typically scheduled with sedentary activities, such as sitting in a classroom or doing homework. Additionally, elementary aged youth reported choosing to watch television or play video games rather than to be physically active. Elementary aged youth in other tribal communities have reported spending time watching television or playing video games every day (Thompson et al., 2001).
The most commonly cited motivators for engagement in physical included a coach, friends, school, and team. Other adolescent populations have identified perceived physical competence, prior positive physical activity, spending time with peers, experiencing positive social interaction, support from peers, and having fun and enjoyment as motivators (Allender, Cowburn, & Foster, 2006; Brooks & Magnusson, 2006; Sallis, Prochaska, & Taylor, 2000). Common barriers reported by the tribal youth included age (too old or young), lack of time, school and/or work responsibilities, and lack of programs. In other adolescent populations, lack of perceived competence in sports, prior negative physical activity experiences, poor body image, concern regarding appearance, negative interactions with peers (e.g., as being last to be picked for a team) have been identified as barriers to engaging in physical activity (Allender et al.; Brooks & Magnusson; Sallis, et al.). In a study with American Indians, elementary aged youth reported homework, fatigue, weather, chores, and lack of a safe place to play as barriers and peer support and participation in physical activity and parental support as motivators (Thompson et al., 2001). Some of the barriers and motivators reported by these tribal youth differ from those reported with other youth populations, including other tribal communities, suggesting that we might have been successful in developing salient instruments and data collection procedures for this community of youth. In response to the evaluation, this tribal community has expanded the structured recreational sport opportunities available for tribal youth so that there are programs targeting all age groups rather than just selected age groups, such as preschoolers. Identification of this unique constellation of determinants for physical activity will increase the likelihood of developing programs that meet the needs of youth in this community.
Implications for Research and Practice
This study incorporated a CBPR approach in working with a tribal community to explore physical activity beliefs, preferences, and patterns among tribal youth. We stressed the collaboration between both partners in the research process and recognized the unique strengths of each partner. Using a CBPR approach increased the amount of time we devoted to the preparatory steps in the research process. Initially, time was spent developing relationships, understanding each other’s perspective, and developing mutually agreeable goals. We engaged in obtaining tribal approval, creating a data sharing agreement, and designing a tribal relevant exercise survey. Later, we followed through in the tribal review process for publications and presentations. This investment created culturally relevant results that facilitated developing germane programs for the tribal youth. Other researchers have described similar time commitments and challenges when incorporating a CBPR approach in working with tribal communities (Burhansstipanov, et al., 2005; Fisher & Ball, 2003; Strickland, 1999).
For this project we prepared a written Data Sharing Agreement that was signed by the investigator and the Tribal Council Chair. We recommend developing a Memorandum of Understanding (MOU), which is signed by a representative from the tribe and university. Unlike the Data Sharing Agreement, the MOU clarifies the nature of the relationship and responsibilities of each organization involved in the research project in addition to outlining issues of data ownership, control and use. Similar to the Data Sharing Agreement the MOU is really a good-faith agreement because an MOU is not legally binding. The MOU delineates the roles of individuals or organization, boundaries for confidentiality, and procedure to resolve conflict. Negotiated items to include are roles and responsibilities of each member of the research team, ownership and control of data, required tribal approval of manuscripts or presentations, restrictions on the use of tribal data collected for research studies, and an outline of acceptable community-responsive dissemination plan for research results. An alternative to the MOU is a written contract, which is legally binding. This approach typically is more bureaucratic and involves considerable time investment.
Youth participation in planning the study was important in developing instruments and procedures that resonated with youth and encouraged youth to voice their opinions. In this tribal community there was a formal structure, Tribal Youth Council, for youth to engage in pertinent issues and have a voice in tribal governance. The investigator worked with the Youth Council in each phase of the research process and a member of the Youth Council was on the CAB for the project. The youth member had equal voice and the other CAB members relied on her as a cultural broker between the adult and youth perspective. If there is not a youth-led organization or formal structure for youth to give voice, we recommend establishing a youth advisory board and have representation from the youth board serve on the CAB. Key aspects to working with youth include: understanding their position in their community, being aware of how this position influences their participation, and creating a safe environment for youth to voice their concerns and ideas (Nygreen, Kwon, & Sánchez, 2006). We recommend initiating working with youth very early in a project’s development.
Conclusions
The principles of CBPR are in concert with tribal values and with the principles of community health nursing. The Institute of Medicine has identified CBPR as a priority approach in chronic disease prevention research (Institute of Medicine, 2001). We recommend using a CBPR approach when working with and conducting research with tribal communities. Respecting tribal knowledge, traditions and beliefs is inherent in CBPR. The CBPR approach enhances the likelihood of establishing trust, building capacity in the community, conducting salient research, and creating sustainable programs (Christopher, 2005; Cochran et al., 2008; Fisher & Ball, 2003). Although this approach requires more time than a traditional academic driven community-placed approach, it is more likely to bring about a change in the community that will foster improved health behaviors.
Contributor Information
Cynthia Perry, Family and Child Nursing, University of Washington, Bo 357262, Seattle, WA 98195-7262, Phone: 206-685-0843, perryc@u.washington.edu.
Barbara Hoffman, Community Health Nurse, Suquamish Tribe.
References
- Acton K, Burrows N, Moore K, Querec L, Geiss L, Engelgau M. Trends in diabetes prevalence among American Indian and Alaska Native children, adolescents, and young adults. American Journal of Public Health. 2002;92(9):1485–1490. doi: 10.2105/ajph.92.9.1485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allender S, Cowburn G, Foster C. Understanding participation in sport and physical activity among children and adults: a review of qualitative studies. Health Education Research. 2006;21(6):826–835. doi: 10.1093/her/cyl063. [DOI] [PubMed] [Google Scholar]
- Associated Press. Arizona lawsuit over misuse of Havasupai blood samples dismissed 5-4-07. News from Indian Country. 2007 Retrieved November 20, 2007 from http://indiancountrynews.net/index.php?option=com_content&task=view&id=393&Itemid=109.
- Brooks F, Magnusson J. Taking part counts: adolescents’ experience of the transition from inactivity to active participation in school-based physical education. Health Education Research. 2006;21(6):872–883. doi: 10.1093/her/cyl006. [DOI] [PubMed] [Google Scholar]
- Brugge D, Missaghian M. Protecting the Navajo people through tribal regulation of research. Science and Engineering Ethics. 2006;12(3):491–507. doi: 10.1007/s11948-006-0047-2. [DOI] [PubMed] [Google Scholar]
- Burhansstipanov L, Christopher S, Schumacher A. Lessons learned from community-based participatory research in Indian country. Cancer Control. 2005;12(S):70–76. doi: 10.1177/1073274805012004s10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldwell J, Davis J, DuBois B, Echo-Hawk H, Erickson J, Goins T, et al. Culturally competent research with American Indians and Alaska Natives: Findings and recommendations of the first symposium of the Work Group on American Indian Research and Program Evaluation Methodology. American Indian and Alaska Native Mental Health Research. 2005;12(1):1–21. doi: 10.5820/aian.1201.2005.1. [DOI] [PubMed] [Google Scholar]
- Christopher S. Recommendations for conducting successful research with Native Americans. Journal Cancer Education. 2005;20(Suppl):47–51. doi: 10.1207/s15430154jce2001s_11. [DOI] [PubMed] [Google Scholar]
- Cochran P, Marshall C, Garcis-Downing C, Kendall E, Cook D, McCubin L, et al. Indigenous ways of knowing: Implications for participatory research and community. American Journal of Public Health. 2008;98(1):8–13. doi: 10.2105/AJPH.2006.093641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dalton R. When two tribes go to war. Nature. 2004;430:500–502. doi: 10.1038/430500a. [DOI] [PubMed] [Google Scholar]
- Daniels S, Arnett D, Eckel R, Gidding S, Hayman L, Kumanyika S, et al. Overweight in children and adolescents: Pathophysiology, consequences, prevention, and treatment. Circulation. 2005;111:199–2012. doi: 10.1161/01.CIR.0000161369.71722.10. [DOI] [PubMed] [Google Scholar]
- Denny C, Holtzman D, Cobb N. Prevalence of diagnosed diabetes among American Indians/Alaska Natives. Morbidity and Mortality Weekly Report. 1998;47(42):901–904. [PubMed] [Google Scholar]
- Denzin N, Lincoln Y. Handbook of qualitative research. 2. Thousand Oaks, CA: Sage Publications; 2000. [Google Scholar]
- Eaton D, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, et al. Youth Risk Behavior Surveillance--United States, 2007. Morbidity and Mortality Weekly Report. 2008;57(SS04):1–131. [PubMed] [Google Scholar]
- Farquhar J, Parker E, Schultz A, Israel B. Application of qualitative methods in program planning for health promotion interventions. Health Promotion Practice. 2006;7:234–242. doi: 10.1177/1524839905278915. [DOI] [PubMed] [Google Scholar]
- Fisher P, Ball T. Tribal participatory research: Mechanisms of a collaborative model. American Journal of Community Psychology. 2003;32(3/4):207–216. doi: 10.1023/b:ajcp.0000004742.39858.c5. [DOI] [PubMed] [Google Scholar]
- Foulks E. Misalliances in the Barrow Alcohol Study. American Indian and Alaska Native Mental Health Research. 1989;2(3):2–17. doi: 10.5820/aian.0203.1989.7. [DOI] [PubMed] [Google Scholar]
- Gittelsohn J, Steeckler A, Johnson C, Pratt C, Grieser M, Pickrel J, et al. Formative research in school and community-based health programs and studies: “State of the art” and the TAAG approach. Health Education and Behavior. 2006;33:25–39. doi: 10.1177/1090198105282412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon-Larsen P, McMurray R, Popkin B. Adolescent physical activity and inactivity vary by ethnicity: The National Longitudinal Study of Adolescent Health. Journal of Pediatrics. 1999;135:301–306. doi: 10.1016/s0022-3476(99)70124-1. [DOI] [PubMed] [Google Scholar]
- Indian Health Service. Final report of the Restructuring Initiative Workgroup. Rockville, MD: 2002. [Google Scholar]
- Indian Health Service. Trends in Indian Health 200-2001. Rockville, MD: Indian Health Service; 2003. [Google Scholar]
- Institute of Medicine Committee on Health and Behavior Research and Practice and Policy Board on Neuroscience and Behavioral Health. Health and behavior: the Interplay of biological, behavioral, and social influences: Executive summary. Washington DC: National Academy Press; 2001. [Google Scholar]
- Liao Y, Tucker P, Okoro C, Giles W, Mokdad A, Harris V. REACH 2010 Surveillance for health. Status in minority communities-United States, 2001-2002. Morbidity and Mortality Weekly Report. 2004;532(SS06):1–36. [PubMed] [Google Scholar]
- Manson S, Garroutte E, Goins R, Henderson P. Access, relevance, and control in the research process: Lessons from Indian Country. Journal of Aging and Health. 2004;16(5S):58S–77S. doi: 10.1177/0898264304268149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews C, Chen K, Freedson P, Buchowski M, Beech B, Pate R, et al. Amount of time spent in sedentary behaviors in the United States, 2003-2004. American Journal of Epidemiology. 2008;167:875–881. doi: 10.1093/aje/kwm390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGregor J. Population genomics and research ethics with socially identifiable groups. Journal of Law Medicine & Ethics. 2007;35(3):356–370. doi: 10.1111/j.1748-720X.2007.00160.x. [DOI] [PubMed] [Google Scholar]
- Nader P, Bradley R, Houts R, McRitchie S, O’Brien M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA. 2008;300(3):295–305. doi: 10.1001/jama.300.3.295. [DOI] [PubMed] [Google Scholar]
- Nygreen K, Kwon S, Sánchez P. Urban youth building community: Social change and participatory research in schools, homes, and community-based organizations. Journal of Community Practice. 2006;14(1/2):107–123. [Google Scholar]
- Sallis J, McKenzie T, Alcaraz J, Kolody B, Faucette N, Hovell M. The effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. American Journal of Public Health. 1997;87:1328–1334. doi: 10.2105/ajph.87.8.1328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallis J, Prochaska J, Taylor W. A review of correlates of physical activity of children and adolescents. Medicine &Science in Sports & Exercise. 2000;32(5):963–975. doi: 10.1097/00005768-200005000-00014. [DOI] [PubMed] [Google Scholar]
- Sandelowski M. Whatever happened to qualitative description? Research in Nursing & Health. 2000;23:224–340. doi: 10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- Schultz A, Krieger J, Galea S. Addressing social determinants of health: Community-based participatory approaches to research and practice. Health Education and Behavior. 2002;29:287–295. doi: 10.1177/109019810202900302. [DOI] [PubMed] [Google Scholar]
- Strickland C. Conducting focus groups cross-culturally: Experiences with Pacific Northwest Indian people. Public Health Nursing. 1999;16(3):190–197. doi: 10.1046/j.1525-1446.1999.00190.x. [DOI] [PubMed] [Google Scholar]
- Thompson J, Davis S, Gittelsohn J, Stone E, Harnack L, Ring K. Patterns of physical activity among American Indian children: An assessment of barriers and support. Journal of Community Health. 2001;26(6):423–445. doi: 10.1023/a:1012507323784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troiano R, Berrigan D, Dodd K, Masse L, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Medicine & Science in Sports & Exercise. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- Zephier E, Himes J, Story M, Zhou X. Increasing prevalence of overweight and obesity in Northern Plains American Indian children. Archives of Pediatrics and Adolescent Medicine. 2006;160:34–39. doi: 10.1001/archpedi.160.1.34. [DOI] [PubMed] [Google Scholar]