

Abstract
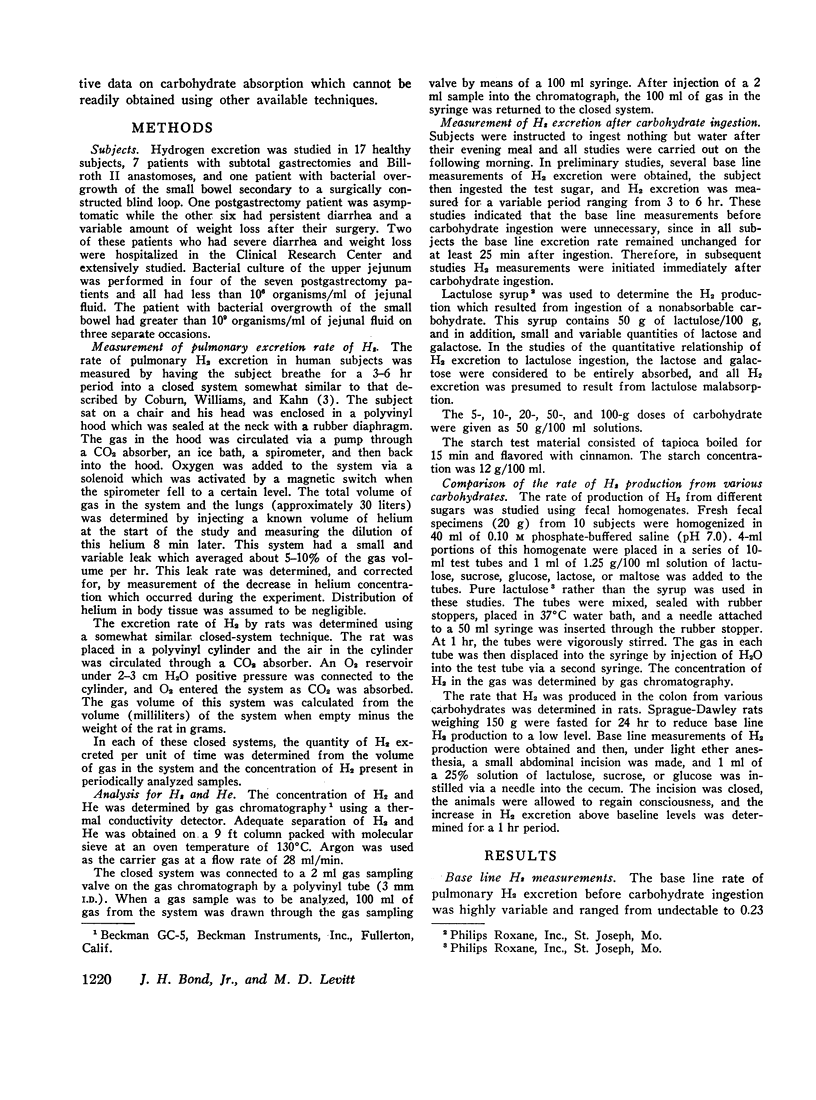
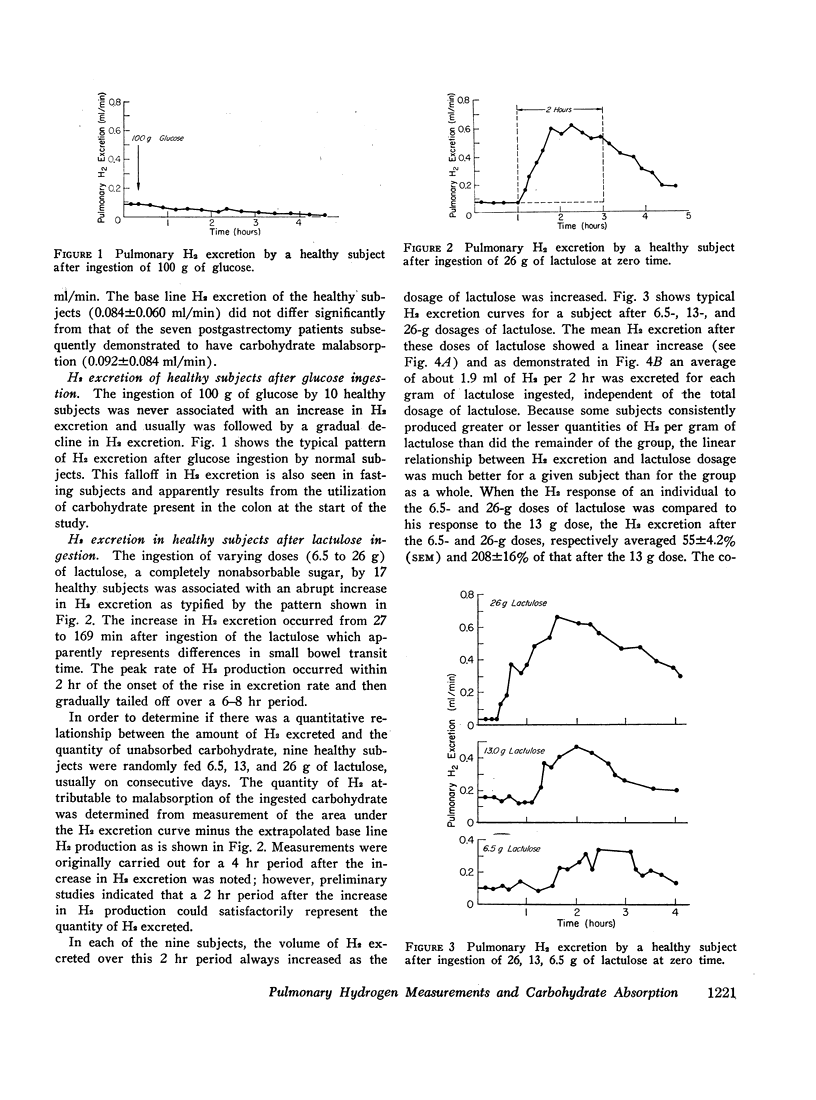
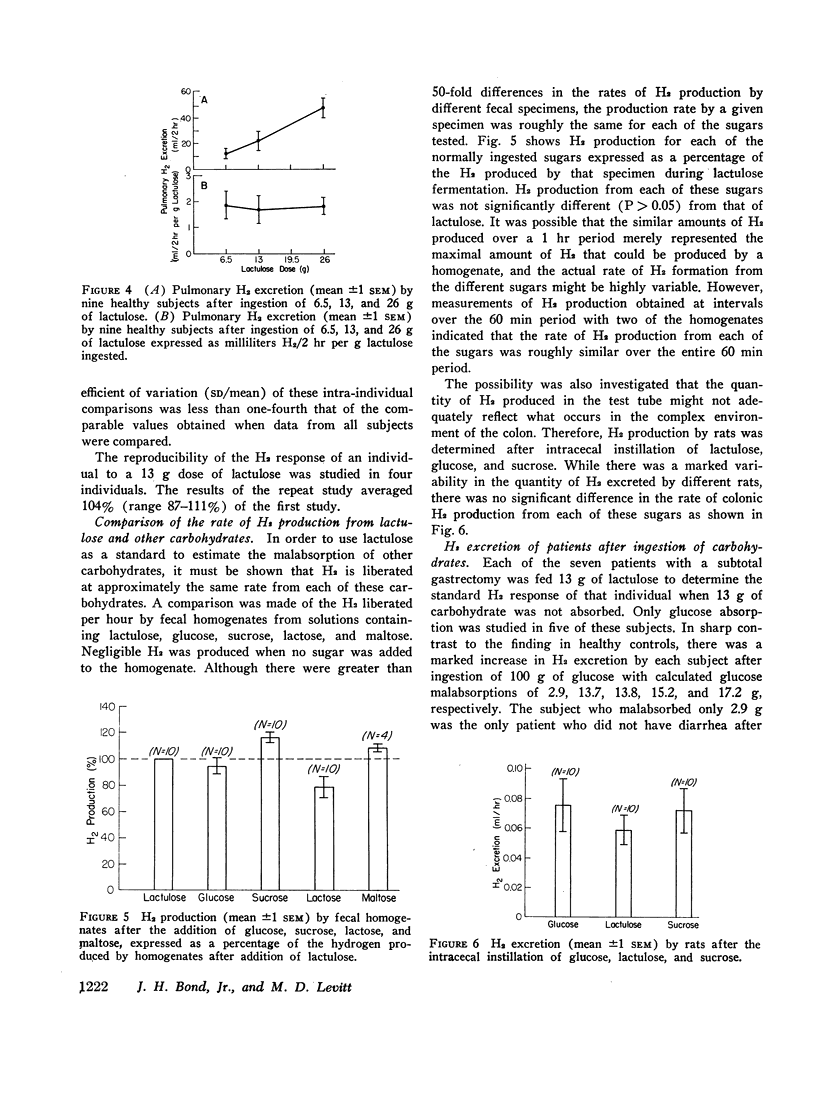
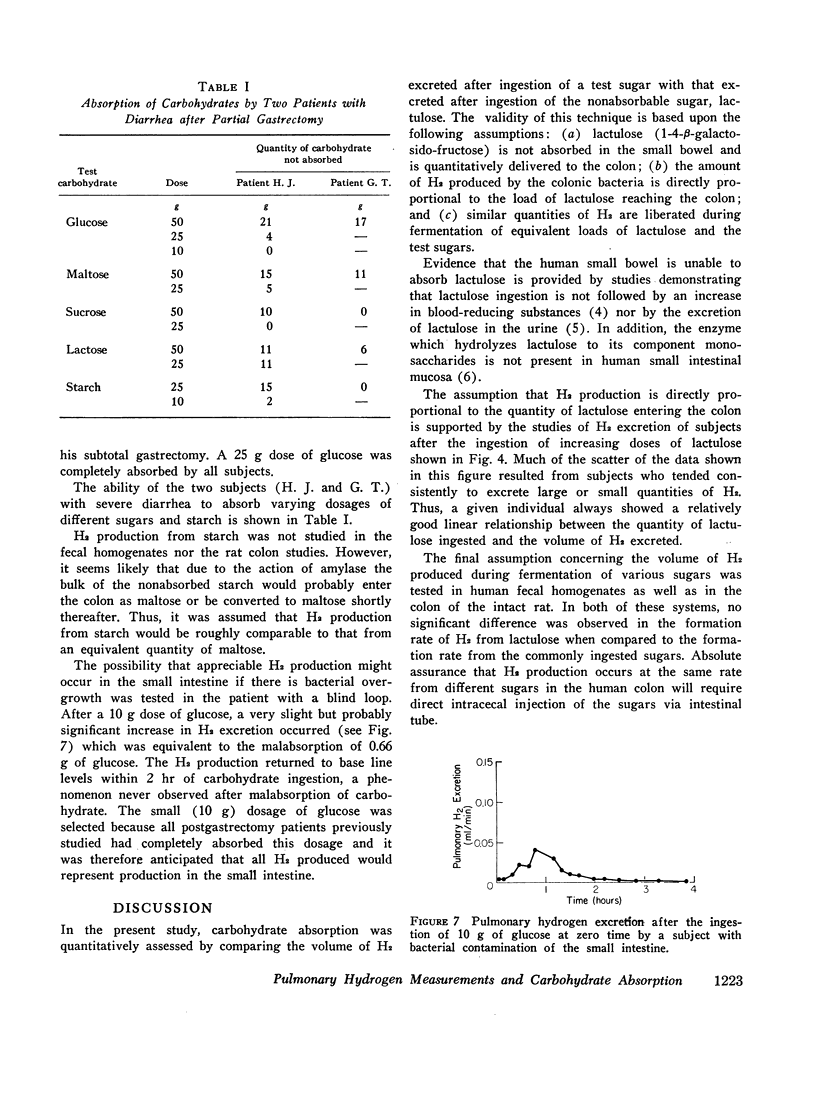
A technique was developed to quantitate the absorption of ingested carbohydrate by means of continuous measurements of pulmonary H2 excretion. This technique is based on the observation that H2 is produced in the colon when carbohydrate is fermented by colonic bacteria, and this H2 is then excreted by the lungs. The quantitative relationship of pulmonary H2 excretion to unabsorbed carbohydrate was studied in nine subjects. After ingestion of 6.5, 13, and 26 g of lactulose (a nonabsorbable disaccharide), H2 excretion increased linearly, averaging (±1 SEM) 13±3.5, 23±7.2, and 49±7 ml per 2 hr. Because of consistent individual differences in H2 excretion per gram of lactulose, the variability of this linear response was less in a given subject, with the H2 excretion after 6.5 g and 26 g lactulose dosages averaging 55±4.2% and 214±16% of that observed after the 13 g dose. It was further demonstrated with fecal homogenates, as well as in rats after direct intracecal instillation of carbohydrate, that there was no significant difference in the rate of H2 formation from lactulose as compared with the normally ingested sugars. Thus, a subject's H2 excretion after a 13 g dose of lactulose can be used as a standard to convert H2 excretion after ingestion of other carbohydrates into grams of carbohydrate not absorbed. Application of this technique to seven partially gastrectomized patients indicated all subjects malabsorbed a portion of a 100 g dose of glucose whereas six of seven completely absorbed a 25 g dose. Malabsorption of physiologic quantities of various carbohydrates was clearly demonstrated in one subject. This technique appears to provide quantitative information on carbohydrate malabsorption not readily obtained by presently available techniques.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BORGSTROM B., DAHLQVIST A., LUNDH G., SJOVALL J. Studies of intestinal digestion and absorption in the human. J Clin Invest. 1957 Oct;36(10):1521–1536. doi: 10.1172/JCI103549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coburn R. F., Williams W. J., Kahn S. B. Endogenous carbon monoxide production in patients with hemolytic anemia. J Clin Invest. 1966 Apr;45(4):460–468. doi: 10.1172/JCI105360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HOFFMANN K., MOSSEL D. A., KORUS W., VAN DE KAMER J. H. UNTERSUCHUNGEN UEBER DIE WIRKUNGSWEISE DER LACTULOSE (BETA-GALACTOSIDO-FRUCTOSE) IM DARM. Klin Wochenschr. 1964 Feb 1;42:126–130. doi: 10.1007/BF01479054. [DOI] [PubMed] [Google Scholar]
- Kasper H. Faecal fat excretion, diarrhea, and subjective complaints with highly dosed oral fat intake. Digestion. 1970;3(6):321–330. doi: 10.1159/000197052. [DOI] [PubMed] [Google Scholar]
- Levitt M. D., Donaldson R. M. Use of respiratory hydrogen (H2) excretion to detect carbohydrate malabsorption. J Lab Clin Med. 1970 Jun;75(6):937–945. [PubMed] [Google Scholar]
- Levitt M. D. Production and excretion of hydrogen gas in man. N Engl J Med. 1969 Jul 17;281(3):122–127. doi: 10.1056/NEJM196907172810303. [DOI] [PubMed] [Google Scholar]
- Soergel K. H. Inert markers. Gastroenterology. 1968 Mar;54(3):449–452. [PubMed] [Google Scholar]