

Introduction
Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA), first recognized in the early 1980s, was noted to occur in patients with MRSA infections who had no identifiable, predisposing risk factors.1–5 Over time, the prevalence of CA-MRSA infection has increased across the United States in both the pediatric and adult populations with CA-MRSA infections commonly encountered in ambulatory dermatology practices. Some have theorized that CA-MRSA was at first a hospital-acquired pathogen with strains traceable to specific healthcare facilities, while others developed de novo within the community.6–10 With the passing of time, CA-MRSA has become more distinct, both genetically and epidemiologically, from nosocomial MRSA, leading many to believe that CA-MRSA isolates did not emerge from local nosocomial MRSA strains.1 Molecular, genetic, and microbiologic studies have revealed that CA-MRSA is associated with a unique genetic profile and phenotype.11 It has been observed that many CA-MRSA strains have become endemic in a given geographic region, progressively replacing other strains due to selective genetic advantages.12–15 According to a 15-year study performed in San Diego, there has been a dramatic increase in CA-MRSA infections since 2002, with an increasing proportion of cases related to intrafamilial spread.1 An estimated 85 percent of CA-MRSA infections present in the skin as abscesses or as folliculitis.16 Outbreaks are usually in the younger populations and in small clusters in localized geographic regions in both rural and urban areas. In its most severe form, CA-MRSA has also been shown to cause septic arthritis, osteomyelitis, pyomyositis, necrotizing fasciitis, and necrotizing pneumonia, especially in young children.11 The incidence of infection increases with close physical contact, loss of skin integrity, and sharing of contaminated personal use articles or equipment.1 Other factors, such as hygiene and physical crowding, also play a large role in spreading CA-MRSA infections. With regard to carriage, the estimated prevalence of S. aureus and MRSA nasal colonization in the United States was reported to be 32.4 percent and 0.8 percent, respectively, based on a large population-based evaluation.17 A high rate of S. aureus colonization also involves the perineum, which like the anterior nares, demonstrates high organism density and a greater propensity for consistent carriage over time.18–21
What is the role of oral antibiotic therapy in the treatment of cutaneous CA-MRSA infections seen in outpatient dermatology practices?
Oral antibiotic therapy is an important component of therapy for uncomplicated cutaneous CA-MRSA infections.11,18 In office-based dermatology practices, most CA-MRSA infections present as folliculitis or furunculosis, with many patients presenting with at least a few abscess-like lesions.11,16 Incision and drainage represents the primary therapy for treatment of lesions presenting as abscesses.11,18,20 Because many patients present with multiple lesions, oral antibiotic therapy is indicated to assist in eradicating the infection.11,16,18 In cases confounded by multiple recurrences over time, it is often necessary to address decolonization of foci of staphylococcal carriage, such as the anterior nares, perineum, and hands.17–21
What antibiotic therapy options are available for treatment of cutaneous CA-MRSA infections?
Several antibiotic options, such as trimethoprim-sulfamethoxazole, fluoroquinolones, lincosamides (i.e., clindamycin), rifampin, daptomycin, carbapenems, and linezolid, are available to treat skin and soft-tissue infections (SSTIs) caused by CA-MRSA.11,16,18,22,23 Oral antibiotics belonging to the tetracycline family, including minocycline and doxycycline, provide an effective means of treating CA-MRSA infections.11,16,18,22,23 As stated above, incision and drainage remains the single most important intervention against CA-MRSA infections, which present as abscess-like lesions. However, when oral antibiotic therapy is indicated based on the judgement of the clinician, tetracycline agents and trimethoprim-sulfamethoxazole are effective in the majority of patients presenting with uncomplicated SSTIs caused by CA-MRSA, and are commonly recommended.1,2,11,16,18,22,23 Tetracyclines are effective against many strains of CA-MRSA.1,2,24–26
What information is available on the use of oral doxycycline for treatment of cutaneous CA-MRSA infections?
Multiple reports support the use of doxycycline in patients with suspected or confirmed cutaneous CA-MRSA infection.24–26 A retrospective cohort study investigated the therapeutic outcomes of patients with CA-MRSA infection treated with extended-spectrum tetracyclines.24 This study evaluated results from 276 patients who presented with 282 episodes of cutaneous MRSA between 2002 and 2007. Ninety episodes (32%) were treated with extended-spectrum tetracyclines (doxycycline or minocycline); whereas, 192 episodes (68%) were treated with a β-lactam agent. The rate of susceptibility of MRSA strains to tetracyclines remained stable at 95 percent during the study. Doxycycline monotherapy was administered in 87 of 90 episodes (97%) treated with tetracyclines. Ninety-six percent of patients (86/90) treated with an extended-spectrum tetracycline achieved success with resolution of their CA-MRSA infection, as compared to 88 percent (168/192) of patients treated with β-lactam monotherapy. Treatment failure was higher in the β-lactam group than in the extended-spectrum tetracycline group (12.5% vs. 4.4%). Four patients who were treatment failures in the tetracycline group exhibited improvement on continued tetracycline therapy after a repeat incision and drainage procedure.
In another study of adult patients with CA-MRSA infections, 54 percent (13/24) were treated with doxycycline and 46 percent (11/24) were treated with minocycline.25 Doxycycline achieved a 92-percent success rate as compared to a 73-percent success rate with minocycline. Based on microbiologic testing in vitro, doxycycline has also been shown to be a very potent agent against CA-MRSA strains with a minimum inhibitory concentration (MIC50 ) value of 0.25μg/mL.26
When used to treat cutaneous CA-MRSA infections, a daily doxycycline dose of 200mg per day is generally used. The duration of therapy varies based on clinical response, with an average duration of treatment ranging from 10 to 21 days.22,23 Interestingly, when utilized in combination with rifampin, doxycycline may prevent the emergence of CA-MRSA strains that become resistant to rifampin.27
What concerns exist regarding CA-MRSA resistance to non-β-lactam oral antibiotics, including extended-spectrum tetracycline agents?
Antibiotic resistance to CA-MRSA is emerging with resistance reported to many antibiotics including fluoroquinolones, macrolides, and lincosamides.22,23,28,29 Resistance of S. aureus to tetracyclines has been reported and is achieved by two potential mechanisms: active reflux and ribosomal protection.24,25,30 Active reflux is mediated by plasmid-located tetK and tetL genes; whereas, chromosome-located tetM or tetO genes mediate ribosomal protection.18,24,25,30 Presence of the tetM gene confers resistance to all antibiotics within the tetracycline family including doxycycline and minocycline; however, presence of tetK gene confers resistance to tetracycline, but the isolates can still be inhibited by minocycline.30 There exists potential for cross-resistance between tetracycline and the extended-spectrum tetracycline derivatives. Therefore, tetracycline-resistant S. aureus should also be considered resistant to doxycycline and minocycline unless sensitivity testing is performed against each individual tetracycline agent that demonstrates otherwise.25,30 In most reference microbiology laboratories used by dermatologists in clinical practice across the United States, sensitivity to tetracycline is all that is reported routinely.
May the formulation of oral doxycycline be clinically significant in the treatment of cutaneous CA-MRSA infections?
Doxycycline is available as either the monohydrate or hyclate salt, with most formulations being immediate release and nonenteric coated. An enteric-coated formulation of doxycycline hyclate is also available (75mg, 100mg, and 150mg tablets). This enteric-coating technology allows for a delay in degradation of the enteric-coated pellets, which are embedded within the body of the tablet matrix. Thus, release of doxycycline bypasses the stomach and occurs within the upper small intestine where the active drug is absorbed.31
Abdominal pain, esophageal pain, nausea, and vomiting are common gastrointestinal (GI) side effects associated with immediate-release, nonenteric coated formulations of doxycycline hyclate and monohydrate.32,33 In one study, a three-fold higher incidence of nausea and vomiting was noted in subjects receiving nonenteric-coated doxycycline as compared to those treated with either penicillin, ampicillin, or tetracycline.32 Nonenteric-coated doxycycline has also proven to be more poorly tolerated in terms of GI side effects as compared to roxithromycin and ciprofloxacin.34,35 Although it has been suggested that nonenteric-coated doxycycline monohydrate produces fewer GI side effects than nonenteric-coated doxycycline hyclate, due to the lower pH of the former, definitive clinical evidence supporting this theoretical suggestion is lacking.31,36
In a randomized, prospective, double-blind, multiple-dose, placebo-controlled, three-way crossover study, healthy adult subjects (N=98; mean age 29 years) were treated for four consecutive days with either enteric-coated doxycycline hyclate 100mg, nonenteric-coated doxycycline hyclate 100mg, or placebo capsules, after treatment on Day 1 with 100mg twice daily.37 All subjects received all three treatments, with a three-day washout between the four-day courses of active treatment. The order of drug administration was balanced and randomized, and a double-dummy technique was used to preserve the study blind. Medication was administered with 180mL of water and at least one hour before food intake. Study diaries were used to capture the incidence and severity of GI complaints, with recordings completed at 0.5, 1, 1.5, 2, 4, 6, 12, and 24 hours post dose. Symptom scores were computed by summing the individual complaints within each treatment period. Figure 1 depicts the mean symptom scores for all three treatment periods, indicating that reports of GI side effects were greatest with nonenteric-coated doxycycline hyclate capsules.
In another randomized, double-blind, multiple-dose, prospective, three-way cross-over, placebo-controlled trial completed in healthy adults (N=111; mean age 26 years), enteric-coated doxycycline hyclate 150mg, nonenteric-coated doxycycline monohydrate 150mg, and placebo tablets were compared regarding the incidence of adverse events, especially GI side effects.31 All subjects received each treatment over three consecutive days with a washout period of 4 to 10 days between active study periods. Medication was administered in the morning after an overnight 10-hour fast with 200mL of water, with no food intake allowed for at least two hours post dose. Subject diaries were used each day to capture the timing, frequency, severity, and cessation of any side effects. Figure 2 demonstrates the results reported by subjects during the study. The incidence of adverse events was highest during treatment with nonenteric-coated doxycycline monohydrate 150mg tablets. The number of subjects experiencing GI side effects, especially nausea and abdominal pain, was markedly higher during administration of nonenteric-coated doxycycline monohydrate 150mg tablets.
Effective oral antibiotic treatment of cutaneous CA-MRSA infections requires adherence with the treatment regimen, which in some cases may be 1 to 2 weeks longer than a conventional duration of treatment.22,23 Therefore, decreasing the potential for subjective GI complaints that often lead to voluntary discontinuation of therapy by the patient is clinically relevant. The marked reduction in GI side effects associated with enteric-coated doxycycline hyclate tablets favors greater overall adherence with the recommended treatment course.
What can be concluded from the available information on the use of oral doxycycline for the treatment of cutaneous CA-MRSA infections?
Based on available data, doxycycline should be considered among the group of first-line oral antibiotic agents used to treat uncomplicated cutaneous CA-MRSA infections. Both in-vitro and clinical studies support its use.24–26 Doxycycline exhibits a more favorable safety profile as compared to trimethoprim-sulfamethoxazole and immediate-release minocycline formulations used to treat CA-MRSA infections.38,39 Unlike rifampin and fluoroquinolones, there is no evidence of rapid emergence of bacterial resistance when doxycycline is used as monotherapy to treat cutaneous CA-MRSA infections.16,23–27 Additionally, the availability of an enteric-coated doxycycline formulation, which is associated with a lower incidence of GI side effects, provides an option that is likely to optimize adherence.31,37
Figure 1.
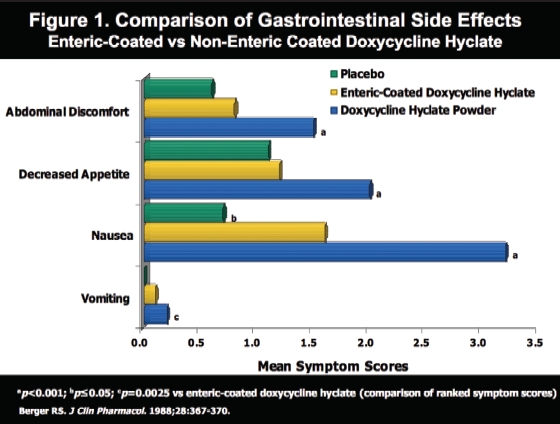
Comparison of Gastrointestinal Side Effects Enteric-Coated vs Non-Enteric Coated Doxycycline Hyclate
Figure 2.
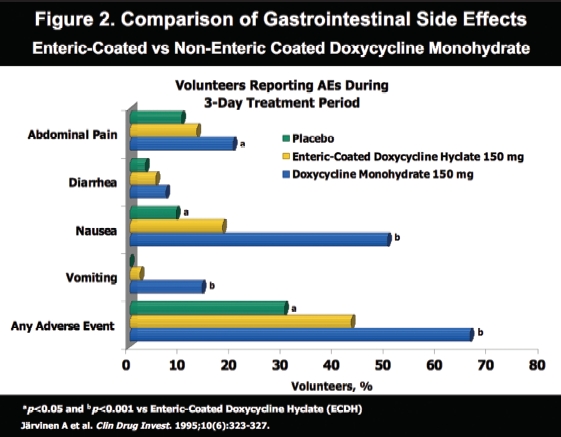
Comparison of Gastrointestinal Side Effects Enteric-Coated vs Non-Enteric Coated Doxycycline Monohydrate
Contributor Information
Sanjay Bhambri, Dr. Bhambri is Chief Dermatology Resident, Valley Hospital Medical Center, Las Vegas, Nevada..
Grace Kim, Dr. Kim is a dermatologist at Valley Hospital Medical Center, Las Vegas, Nevada. The authors report no conflicts of interest in relationship to the content of this article..
James Q. Del Rosso, Dr. Del Rosso is Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada, Touro University College of Osteopathic Medicine, Henderson, Nevada; Clinical Associate Professor, Dermatology, University of Nevada School of Medicine, Las Vegas, Nevada; Las Vegas Skin & Cancer Clinics, Las Vegas and Henderson, Nevada..
References
- 1.Crum NF, Lee RU, Thornton MS, et al. Fifteen-year study of the changing epidemiology of methicillin-resistant Staphylococcus aureus. Am J Med. 2006;119:943–951. doi: 10.1016/j.amjmed.2006.01.004. [DOI] [PubMed] [Google Scholar]
- 2.Hryniewicz W. Epidemiology of MRSA. Infection. 1999;27:S13–S16. doi: 10.1007/BF02561663. [DOI] [PubMed] [Google Scholar]
- 3.Salgado CS, Far BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131–139. doi: 10.1086/345436. [DOI] [PubMed] [Google Scholar]
- 4.Gorak EJ, Yamada SM, Brown JD. Community-aquired methicillin-resistant Staphylococcus aureus in hospitalized adults and children without known risk factors. Clin Infect Dis. 1999;29:797–800. doi: 10.1086/520437. [DOI] [PubMed] [Google Scholar]
- 5.Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279(8):593–598. doi: 10.1001/jama.279.8.593. [DOI] [PubMed] [Google Scholar]
- 6.Charlebois ED, Perdreau-Remingon F, Kreiswirth B, et al. Origins of community strains of methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2004;15:47–54. doi: 10.1086/421090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Eady EA, Cove JH. Staphylococcal resistance revisited: Community-acquired methicillin-resistant Staphylococcus aureus—an emerging problem for the management of skin and soft tissue infections. Curr Opin Infect Dis. 2003;16:103–124. doi: 10.1097/00001432-200304000-00007. [DOI] [PubMed] [Google Scholar]
- 8.Fey PD, Said-Salim B, Rupp ME, et al. Comparative molecular analysis of community- or hospital-acquired methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2003;47:196–203. doi: 10.1128/AAC.47.1.196-203.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Deresinski S. Methicillin-resistant Staphylococcus aureus: an evolutionary, epidemiologic, and therapeutic odyssey. Clin Infect Dis. 2005;40:562–573. doi: 10.1086/427701. [DOI] [PubMed] [Google Scholar]
- 10.Chambers HF. The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis. 2001;7(2):178–182. doi: 10.3201/eid0702.010204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Elston DM. Community-aquired methicillin-resistant Staphylococcus aureus. J Am Acad Dermatol. 2007;56:1–16. doi: 10.1016/j.jaad.2006.04.018. [DOI] [PubMed] [Google Scholar]
- 12.Wang C-C, Lo W-T, Chu M-L, Sui LK. Epidemiological typing of community-acquired methicillin-resistant Staphylococcus aureus isolates from children in Taiwan. Clin Infect Dis. 2004;39:481–487. doi: 10.1086/422642. [DOI] [PubMed] [Google Scholar]
- 13.Holmes A, Ganner M, Mcauane S, et al. Staphylococcus aureus isolates carrying Panton-Valentine Leucocidin genes in England and Wales: frequency, characterization, and association with clinical disease. J Clin Microbiol. 2005;43:2384–2390. doi: 10.1128/JCM.43.5.2384-2390.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Faria NA, Oliveira DC, Westh H, et al. Epidemiology of emerging methicillin-resistant Staphylococcus aureus (MRSA) in Denmark: a nationwide study in a country with low prevalence of MRSA infection. J Clin Microbiol. 2005;43:1836–1842. doi: 10.1128/JCM.43.4.1836-1842.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mishaan AMA, Mason EO, Jr, Martinez-Aguilar G, et al. Emergence of a predominant clone of community-acquired Staphylococcus aureus among children in Houston, Texas. Pediatr Infect Dis J. 2005;24:201–206. doi: 10.1097/01.inf.0000151107.29132.70. [DOI] [PubMed] [Google Scholar]
- 16.Kim G, Del Rosso JQ. Pharmacotherapy update: community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) infections: evaluation and management strategies. Skin & Aging. 2008;16:36–38. [Google Scholar]
- 17.Kuehnert MJ, Kruszon-Moran D, Hill HA, et al. Prevalence of Staphylococcus aureus nasal colonization in the United States, 2001–2002. J Infect Dis. 2006;193:172–179. doi: 10.1086/499632. [DOI] [PubMed] [Google Scholar]
- 18.Elston DM. Methicillin-sensitive and methicillin-resistant Staphylococcus aureus: management principles and selection of antibiotic therapy. Dermatol Clin. 2007;25:157–164. doi: 10.1016/j.det.2007.01.007. [DOI] [PubMed] [Google Scholar]
- 19.Del Rosso JQ, Elston DM. Tackling the anterior nares and other sites of colonization: implications for the dermatologist. Cutis. 2007;79(6):52–59. [PubMed] [Google Scholar]
- 20.Elston DM. How to handle a CA-MRSA outbreak. Dermatol Clin. 2009;27:43–48. doi: 10.1016/j.det.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 21.Wertheim HF, Melles DC, Vos MC, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis. 2005;5:751–762. doi: 10.1016/S1473-3099(05)70295-4. [DOI] [PubMed] [Google Scholar]
- 22.Cohen PR. Community-acquired methicillin-resistant Staphylococcus aureus skin infections: implications for patients and practitioners. Am J Clin Dermatol. 2007;8:259–270. doi: 10.2165/00128071-200708050-00001. [DOI] [PubMed] [Google Scholar]
- 23.Cohen PR, Grossman ME. Management of cutaneous lesions associated with an emerging epidemic: community-acquired methicillin-resistant Staphylococcus aureus infections. J Am Acad Dermatol. 2004;51:132–135. doi: 10.1016/j.jaad.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 24.Ruhe JJ, Menon A. Tetracyclines as an oral treatment option for patients with community onset skin and soft tissue infections caused by methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2007;51:3298–3303. doi: 10.1128/AAC.00262-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ruhe JJ, Monson T, Bradsher RW, et al. Use of long-acting tetracyclines for methicillin-resistant Staphylococcus aureus infections: case series and review of the literature. Clin Infect Dis. 2005;40:1429–1434. doi: 10.1086/429628. [DOI] [PubMed] [Google Scholar]
- 26.Tsuji BT, Rybak MJ, Cheung CM, et al. Community- and healthcare-associated methicillin-resistant Staphylococcus aureus: a comparison of molecular epidemiology and antimicrobial activities of various agents. Diagn Microbiol Infect Dis. 2007;58:41–47. doi: 10.1016/j.diagmicrobio.2006.10.021. [DOI] [PubMed] [Google Scholar]
- 27.Kirkland EB, Adams BB. Methicillin-resistant Staphylococcus aureus and athletes. J Am Acad Dermatol. 2008;59:494–502. doi: 10.1016/j.jaad.2008.04.016. [DOI] [PubMed] [Google Scholar]
- 28.Del Rosso JQ, Leyden JJ. Status report on antibiotic resistance: implications for the dermatologist. Dermatol Clin. 2007;25:127–132. doi: 10.1016/j.det.2007.01.001. [DOI] [PubMed] [Google Scholar]
- 29.Guay DRP. Treatment of bacterial skin and structure infections. Expert Opin Pharmacother. 2003;4:1259–1275. doi: 10.1517/14656566.4.8.1259. [DOI] [PubMed] [Google Scholar]
- 30.Trzcinski K, Cooper BS, Hryniewicz W, et al. Expression of resistance to tetracyclines in strains of methicillin-resistant Staphylococcus aureus. J Antimicrob Chemother. 2000;45:763–770. doi: 10.1093/jac/45.6.763. [DOI] [PubMed] [Google Scholar]
- 31.Järvinen A, Nykanen S, Paasiniemi L, et al. Enteric coating reduces upper gastrointestinal adverse reactions to doxycycline. Clin Drug Investig. 1995;10(6):323–327. doi: 10.2165/00044011-199510060-00002. [DOI] [PubMed] [Google Scholar]
- 32.Bryant SG, Fisher S, Kluge RM. Increased frequency of doxycycline side-effects. Pharmacotherapy. 1987;7:125–129. doi: 10.1002/j.1875-9114.1987.tb04037.x. [DOI] [PubMed] [Google Scholar]
- 33.Del Rosso JQ, Schlessinger J, Werschler P. Comparison of anti-inflammatory dose doxycycline versus doxycycline 100 mg in the treatment of rosacea. J Drugs Dermatol. 2008;7:573–576. [PubMed] [Google Scholar]
- 34.De Vlieger A, Druart M, Puttemans M. Roxithromycin versus doxycycline in the treatment of acute exacerbations of chronic bronchitis. Diagn Microbiol Infect Dis. 1992;15:1235–1237. doi: 10.1016/0732-8893(92)90139-k. [DOI] [PubMed] [Google Scholar]
- 35.Beltran RR, Herrero JIH. Evaluation of ciprofloxacin and doxycycline in the treatment of Mediterranean spotted fever. Eur J Clin Microbiol Infect Dis. 1992;11:427–431. doi: 10.1007/BF01961857. [DOI] [PubMed] [Google Scholar]
- 36.Carlborg B, Farmer JC. Esophageal corrosion tests with doxycycline monohydrate tablets. Curr Ther Res. 1983;34:110–116. [Google Scholar]
- 37.Berger RS. A double-blind, multiple-dose, placebo-controlled, cross-over study to compare the incidence of gastrointestinal complaints in healthy subjects given Doryx R and Vibramycin R. J Clin Pharmacol. 1988;28:367–370. doi: 10.1002/j.1552-4604.1988.tb03160.x. [DOI] [PubMed] [Google Scholar]
- 38.Del Rosso JQ. Systemic therapy for rosacea: focus on oral antibiotic therapy and safety. Cutis. 2000;66:7–13. [PubMed] [Google Scholar]
- 39.Bhambri S, Del Rosso JQ, Desai A. Oral trimethoprim-sulfamethoxazole in the treatment of acne vulgaris. Cutis. 2007;79:430–434. [PubMed] [Google Scholar]