

Abstract
Background: As tattoos have become increasingly popular in the Western world, tattoo-removal requests have also increased, as patients’ personal identities advance. Laser tattoo removal is the current treatment of choice given its safety and efficacy. However, due to varying types of tattoos, it has been difficult to quantify the number of laser treatments required with certainty when discussing laser tattoo removal with our patients. Objective: To propose a practical numerical scale to assess the number of laser tattoo-removal treatments necessary to achieve satisfactory results. Methods and materials: A retrospective chart review was performed on 100 clinic patients who presented for laser tattoo removal. An algorithm was proposed to assign a numerical score to each tattoo across six different categories (skin type, location, color, amount of ink, scarring, and layering). The cumulative score (Kirby-Desai score) is proposed to correlate with the number of treatment sessions required for satisfactory tattoo removal. Results: A correlation coefficient of 0.757 was achieved, with satisfactory tattoo removal in all subjects (N=100, p<0.001). Conclusion: We propose the Kirby-Desai scale as a practical tool to assess the number of laser tattoo-removal sessions required, which will translate into a more certain cost calculation for the patient.
The art of tattooing has a long-dated history in civilization with origins dating back to 12,000 BC.1 From ancient times to modern day, tattoos have gained increasing popularity among many demographic populations with current estimates of more than 20 million people (3–5% of the population) having at least one tattoo.2,3 However, tattoos often become a personal regret, as up to 50 percent of adults older than 40 seek tattoo removal as a means to fix their tattoo quest.4 Lasers have been used to remove tattoos since the late 1970s and have in recent years become the mainstay for removal due to their high efficacy and low incidence of deleterious side effects. Although a patient’s decision to remove a tattoo is definitive, the logistical uncertainty remains—such as the number of treatments and whether laser tattoo removal will be successful—adding unwanted burdens on the patient.
In this paper, we propose the Kirby-Desai scale to assess the potential success and number of treatments necessary for laser tattoo removal, assuming the medical practitioner is using a quality-switched Nd:YAG (neodymium-doped yttrium aluminum garnet) or Alexandrite laser incorporating selective photothermolysis with 6 to 8 weeks between treatments. This scale can be used by the physician during preconsultation to determine the number of treatments required for tattoo removal, decreasing the uncertainty of the laser-removal process. Currently, patients receive a poorly defined assessment of the number of treatments and often engage in the process without full awareness of the potential success. In the Kirby-Desai scale, numerical values are assigned to six parameters: skin type, location, color, amount of ink, scarring or tissue change, and layering. Parameter scores are then added to yield a combined score that will show the estimated number of treatments needed for successful tattoo removal. Tattoos scoring greater than 15 points may be difficult to remove and should be assessed by the physician to decide whether laser removal is the method of choice for the patient. The Kirby-Desai scale is the first proposed scale, to our knowledge, that enables physicians to have a thorough laser-removal assessment and hopefully aids in defining a more accurate treatment plan and improve patient satisfaction.
Materials and Methods
One hundred patients who had been seen in the authors’ clinic (WK, Dr. Tattoff Inc., Beverly Hills, California) from July 2004 through August 2008 for laser tattoo-removal treatments were chosen for retrospective chart review by the authors and were included in our study. Exclusion criteria included patients younger than 18 years of age and patients who did not complete the expected tattoo-removal treatment sessions to achieve a satisfactory outcome due to personal reasons (pain, unable to keep appointments, lost to follow up).
Scale parameters for the Kirby-Desai score were applied as follows: skin type = 1 to 6 based on the Fitzpatrick skin type; location = 1 to 5; color = 1 to 4; amount of ink = 1 to 4; scarring = 0 to 5; layering = 0 to 2 (Tables 1–6).
Table 1.
Fitzpatrick skin type and Kirby-Desai score
| FITZPATRICK TYPE | SKIN COLOR | CHARACTERISTICS | POINTS IN THE KIRBY-DESAI SCALE |
|---|---|---|---|
| I | White; very fair; red or blond hair; blue eyes; freckles | Always burns, never tans | 1 |
| II | White; fair; red or blond hair; blue, hazel, or green eyes | Usually burns, tans with difficulty | 2 |
| III | White or olive skin tone; fair with any eye or hair color; very common | Sometimes mild burn, gradually tans | 3 |
| IV | Brown; common in people of Mediterranean descent | Rarely burns, tans with ease | 4 |
| V | Dark Brown; common in people of Middle-Eastern descent | Very rarely burns, tans very easily | 5 |
| VI | Black | Never burns, tans very easily | 6 |
Table 6.
Tattoo layering and Kirby-Desai score
| TATTOO LAYERING | POINTS IN THE KIRBY-DESAI SCALE |
|---|---|
| No | 0 |
| Yes | 2 |
A Kirby-Desai score was recorded by one investigator for each tattoo based on the patient’s history and photographs taken prior to the initiation of laser tattoo-removal treatments. A Pearson correlation coefficient between Kirby-Desai scores and the number of actual tattoo treatments performed in the subject group was calculated using SPSS 16.0.1 (SPSS Inc., Chicago, Illinois).
Results
Results of the study revealed that complete removal of all the tattoos in 100 patients was achieved in our subject group. The average number of treatments required was 10 treatments (9.91±3.18), with a range of 3 to 20 treatments. This correlated well with the average Kirby-Desai score of 9.87 with a standard deviation of ±2.45. A normal distribution was plotted for both data groups as seen in Figures 1a and 1b. A good correlation coefficient (r= 0.757) was found between the Kirby-Desai score and the number of laser tattoo-removal treatments (Figure 2). Using a t-ratio calculation, we can conclude that the number of patients (N=100) was sufficient to provide a statistically significant association between the Kirby-Desai score and the number of required tattoo-removal treatments (p<0.001).
Figures 1a and 1b.
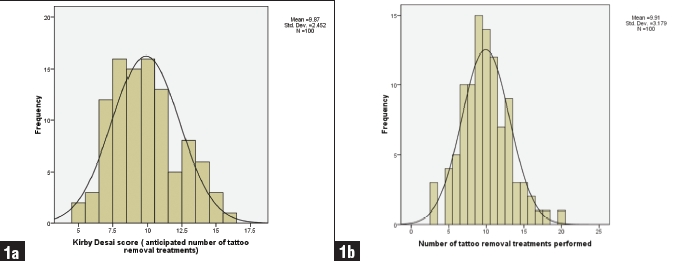
Histogram showing the distribution of (a) the calculated Kirby-Desai scores and (b) the actual laser treatments required to achieve satisfactory tattoo removal.
Figure 2.
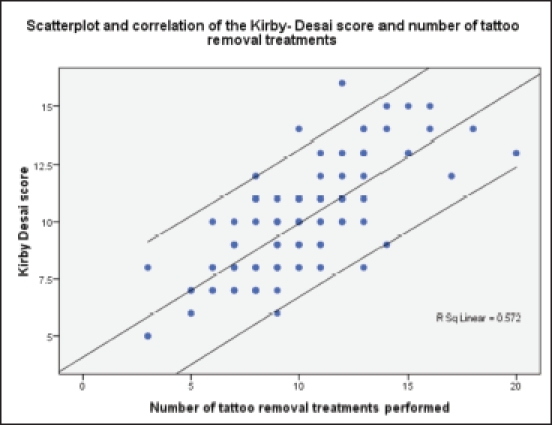
Scatter plot of the Kirby-Desai scores and number of tattoo-removal treatments
Discussion
It is well established in the medical literature that multiple laser treatments are required to remove a tattoo via selective photothermolysis. What has not been elucidated however is the number of treatments that are actually required for a given patient. Using the proposed scale, we were able to provide a good assessment of the anticipated number of treatments required to achieve complete tattoo removal. Further reasoning behind the breakdown of the scale is discussed as follows.
Skin type. Regardless of whether a tattoo is placed unintentionally due to trauma or from a professional artist, the ink must effectively penetrate the dermis of the skin to successfully become a permanent tattoo. Consequently, removal requires laser penetration into the dermal layer while traversing the epidermal layer without causing significant damage. The basal layer of the epidermis contains melanocytes that absorb laser photon energy with decreasing absorption seen from shorter to longer wavelengths.5 Thus one of the considerations in laser tattoo removal is skin type. The Fitzpatrick scale is the current gold standard for clinically categorizing skin types into six classes based on the reaction to ultraviolet radiation, denoting the degree of skin pigmentation and thus melanin deposition. Melanin, like tattoo pigment, is a light-absorbing compound of similar size. Therefore, melanin and tattoo pigments share similar thermal relaxation times; the time needed to dissipate heat absorbed during laser-pulse administration, which relates to the energy level needed to disrupt the granules of both melanin and tattoo pigment.5 That said, because melanin and tattoo ink have very different absorption spectrums, successful laser tattoo outcomes can be achieved on darker skin types although the rate of adverse effects, specifically hypopigmentation, is understandably higher. The decreased efficacy of laser tattoo removal in patients with higher Fitzpatrick scores occurs because the laser operators use lower laser settings and wait longer between treatment sessions to hopefully minimize unwanted side effects. The Kirby-Desai scale incorporates this variable scoring each Fitzpatrick skin type with its corresponding number of 1 to 6 (Table 1).
Location. As the tattoo pigment granules come in contact with blood and lymphatic vessels in the dermal layer, they are immediately engulfed by keratinocytes, fibroblasts, and phagocytic macrophages, which line up under the dermal layers. As time progresses, as is seen in a series of biopsies done at 2 to 3 months and 40 years, ink granules are only seen in the dermal fibroblasts lying in a perivascular location beneath a layer of fibrosis.4 It is this molecular arrangement that allows laser tattoo removal to work. During the laser tattoo-removal process, photons penetrate the molecules of pigment, which try to absorb the energy, but fail to and thus break the bonds of the pigment molecules reducing them to smaller-sized molecules. The macrophages then absorb the smaller molecules and return them to the lymphatic circulation.
Blood and lymphatic supply vary by anatomic region,6 as does the efficacy of laser tattoo removal in such corresponding anatomic areas. The head and neck maintain the largest amount of regional lymph nodes and have a large vascular supply; thus, they are able to mount an increased immune response to phagocytose the ink particles. The upper and lower trunks also have a vast vascular and lymphatic supply, trailing behind the head and neck regions. The proximal extremities have more lymphatic supply than the distal extremities. The Kirby-Desai scale adjusts for such regional variation in blood and lymphatic supply (Table 2).
Table 2.
Tattoo location and Kirby-Desai score
| LOCATION | POINTS IN THE KIRBY–DESAI SCALE |
|---|---|
Head and Neck

|
1 |
Upper Trunk

|
2 |
Lower Trunk

|
3 |
Proximal Extremity
|
4 |
Distal Extremity
|
5 |
Colors. Tattoo artists use a variety of compounds to create tattoo pigment, with an inability to specifically identify the exact makeup of the ink.7 As such, professional and amateur tattoos differ in their physical and chemical composition of ink. Amateur tattoos tend to use elemental carbon particles compiled from cigarette ash, pencil particles, graphite, or inks, such as India ink. Professional artists use organic dyes mixed with metallic elements and have a propensity to mix pigments to achieve a desired color.8,9 Colors most often used by tattoo artists are black, red, blue, green, yellow, and orange. Black pigment granules in tattoos vary in size from 0.5µm to 4.0µm, and are typically composed of carbon- and iron-containing granules. Colors other than black have been noted to be up to twice the size of the black pigment. These differences in pigment size and composition lead to the difference in amount of treatments needed.9 Black pigments are the easiest to remove due to their relative small size, lack of metallic elements, and ability to absorb every wavelength of light. Red pigments are also considered easily removable in comparison to other colors, such as green and yellow based on their composition as well. Red pigments are known to contain a mixture of metallic and carbon elements with a smaller percentage of titanium dioxide, leading to its ease in removal.10 Other colors, such as green, yellow, and orange are more difficult to remove and warrant a higher amount of points on the Kirby-Desai scale (Table 3).
Table 3.
Tattoo pigment color and Kirby-Desai score
| COLOR OF PIGMENT(S) | POINTS IN THE KIRBY-DESAI SCALE |
|---|---|
| Black only | 1 |
| Mostly black with some red | 2 |
| Mostly black and red with other colors | 3 |
| Multiple colors | 4 |
Amount of ink. The amount of ink within a tattoo is another parameter that affects laser tattoo removal. The difference in the amount of ink lies within the type of tattoo the patient has—professional or amateur. Amateur tattoos are usually placed unevenly in the superficial dermis and tend to contain less ink than professional artists. Thus, amateur tattoos tend to respond quicker to laser treatment. Professional tattoos on the other hand tend to lie deeper in the dermis and have a greater density of pigment.7,11 In a paper by Alster, amateur tattoos on average were seen to be smaller in size in comparison to professional tattoos (16cm2 vs. 66cm2). Average amateur tattoos range from 2 to 48cm2, while professional tattoos range from 4 to 200cm2.12–14 In the Kirby-Desai scale, amount of ink is divided into four categories: amateur (letters, words, or small symbols), minimal (one color, simple design), moderate (one color, complex design), and significant (multicolored, complex design), with each category receiving from 1 to 4 points, respectively (Table 4).
Table 4.
Amount of ink and Kirby-Desai score
| AMOUNT OF INK | POINTS IN THE KIRBY-DESAI SCALE |
|---|---|
Amateur

|
1 |
Minimal
|
2 |
Moderate

|
3 |
Significant

|
4 |
Scarring and tissue change. Tattoo placement can sometimes lead to complications that include granulomas, lichen planus, keloids, and psoriasis.15,16 Tattoo placement may result in increased collagen deposition in the superficial dermis, with potential for scar formation. Although the propensity to form scars is highly variable among patients in general, patients with Fitzpatrick skin types 5 and 6 have higher incidences of scar formation. During the normal healing process, following tattoo placement or other trauma, extravasation of immune cells leads to the proliferation of fibroblasts, macrophages, and neovascular tissue. This early formation of neovascularized granulation tissue is a crucial step in redeveloping normal histological structure following injury. However, if excessive fibroblast activity ensues, which leads to overproduction of collagen, permanent scar formation will result. Tattoo pigment within this fibrosed superficial dermis is much more difficult to remove due to the congestion of cells. If cells of the immune system cannot penetrate the area of tattoo ink, removal becomes difficult.17 In the Kirby-Desai scale, scarring and tissue change are incorporated (Table 5).
Table 5.
Scarring and tissue change amount and Kirby-Desai score
| SCARRING AND TISSUE CHANGE AMOUNT | POINTS IN THE KIRBY-DESAI SCALE |
|---|---|
| No Scar | 0 |
| Minimal amount of scarring | 1 |
| Moderate amount of scarring | 3 |
| Significant amount of scarring | 5 |
Layering tattoos. Patients sometimes seek to “remove” an undesirable tattoo by layering it with another tattoo. The new tattoo is usually larger than the tattoo it is replacing, incorporating and hiding the previous tattoo in new contours and colors. Since tattoo ink is translucent, layering or covering up a previous tattoo necessitates darker tones in the new tattoo to effectively hide the older one. Since the new layered tattoo is larger and darker, it will require more treatments for tattoo removal. As such, layering is given 2 points in the Kirby-Desai scale. Those without layering receive 0 points (Table 6).
Results of our retrospective chart review revealed a good correlation between the Kirby-Desai scores and the number of laser tattoo-removal treatments required (r=0.757, p<0.0001). Further studies with more subjects are still needed to confirm the reproducibility of this scale, as our chosen subject group and clinic population may not include sufficient difficult-to-treat tattoos (scarring, layering tattoos), as seen with a completely successful tattoo-removal rate in our subject group. Furthermore, a multivariate linear regression analysis of future larger studies may further elucidate the relationship between our Kirby-Desai parameters.
It is well established in the medical literature that multiple laser treatments are required to remove a tattoo via selective photothermolysis. What has not been elucidated however is the number of treatments that are actually required for a given patient. It is our contention that by incorporating the Kirby-Desai scale into the art of laser tattoo removal, medical professionals will be able to better estimate the required number of patient treatments.
Acknowledgments
The authors would like to thank Sarah Brice, Ian Kirby, Emily Holmes, Marielle Bernstein, Corrie Wahl, and Corey Ordoyne for their contributions to this paper.
References
- 1.Tope W. State and territorial regulation of tattooing in the United States. J Am Acad Dermatol. 1995;32:791–799. doi: 10.1016/0190-9622(95)91477-3. [DOI] [PubMed] [Google Scholar]
- 2.Armstrong M. Career-oriented women with tattoos. Image J Nurs Sch. 1991;23:215–220. doi: 10.1111/j.1547-5069.1991.tb00674.x. [DOI] [PubMed] [Google Scholar]
- 3.Anderson R. Tattooing should be regulated. N Engl J Med. 1992;326 doi: 10.1056/NEJM199201163260318. [DOI] [PubMed] [Google Scholar]
- 4.Kilmer S, Fitzpatrick R, Goldman M. Tattoo lasers. [March 2009]. http://www.emedicine.com/derm/topic563.htm.
- 5.Bernstein E. Laser treatment of tattoos. Clin Dermatol. 2006;24:43–55. doi: 10.1016/j.clindermatol.2005.10.025. [DOI] [PubMed] [Google Scholar]
- 6.Modi S, Stanton AWB, Mortimer PS, Levick JR. Clinical assessment of human lymph flow using removal rate constants of interstitial macromolecules: a critical review of lymphoscintigraphy. Lymphat Res Biol. 2007;5:183–202. doi: 10.1089/lrb.2007.5306. [DOI] [PubMed] [Google Scholar]
- 7.Kuperman-Beade M, Levine V, Ashinoff R. Laser removal of tattoos. Am J Clin Dermatol. 2001;2:21–25. doi: 10.2165/00128071-200102010-00004. [DOI] [PubMed] [Google Scholar]
- 8.Sweeney S. Tattoos: a review of tattoo practices and potential treatment options for removal. Curr Opin Pediatr. 2006;19:391–395. doi: 10.1097/01.mop.0000236388.64333.cd. [DOI] [PubMed] [Google Scholar]
- 9.Taylor C, Anderson R, Gange R, et al. Light and electron microscopic analysis of tattoos treated by Q-switched ruby laser. J Invest Dermatol. 1991;97:131–136. doi: 10.1111/1523-1747.ep12478570. [DOI] [PubMed] [Google Scholar]
- 10.Ross E, Yashar S, Michaud N, et al. Tattoo darkening and nonresponse after laser treatment: a possible role for titanium dioxide. Arch Dermatol. 2001;137:33–37. doi: 10.1001/archderm.137.1.33. [DOI] [PubMed] [Google Scholar]
- 11.Watanabe S. Basics of laser application to dermatology. Arch Dermatol Res. 2008;300:21–30. doi: 10.1007/s00403-007-0801-6. [DOI] [PubMed] [Google Scholar]
- 12.Alster T. Q-switched alexandrite laser treatment (755nm) of professional and amateur tattoos. J Am Acad Dermatol. 1995;33:69s–73s. doi: 10.1016/0190-9622(95)90013-6. [DOI] [PubMed] [Google Scholar]
- 13.Mcburney E. Carbon dioxide laser treatment of dermatologic lesions. South Med J. 1978;71:795–797. doi: 10.1097/00007611-197807000-00017. [DOI] [PubMed] [Google Scholar]
- 14.Brady S, Blokmanis A, Jewett L. Tattoo removal with the carbon dioxide laser. Ann Plast Surg. 1978;2:482–490. doi: 10.1097/00000637-197906000-00006. [DOI] [PubMed] [Google Scholar]
- 15.Tanzi E, Michael E. Tattoo reactions. [March 2009]. http://www.emedicine.com/derm/topic512.htm.
- 16.Kazandjieva J, Tsankov N. Tattoos: dermatological complications. Clin Dermatol. 2007;25:375–382. doi: 10.1016/j.clindermatol.2007.05.012. [DOI] [PubMed] [Google Scholar]
- 17.Urioste S, Arndt K, Dover J. Keloids and hypertrophic scars: review and treatment strategies. Semin Cutan Med Surg. 1999;18:159–171. doi: 10.1016/s1085-5629(99)80040-6. [DOI] [PubMed] [Google Scholar]