

Abstract
Blastomycosis is a fungal infection caused by Blastomyces dermatitidis. Exposure in endemic regions frequently occurs when spores in soil are disturbed and subsequently inhaled. Less commonly, primary cutaneous blastomycosis may follow after traumatic inoculation of the fungus into the skin. Most patients infected with blastomycosis are asymptomatic, but an unfortunate small number present with fulminant disease. Rarely, the infection can affect organs, such as the skin, bone, or genitourinary system. In a small percentage of cases, blastomycosis may cause acute respiratory distress syndrome, which is associated with a very high mortality rate. Increased survival rates have been shown when the clinician has a high index of suspicion and facilitates rapid evaluation and initiation of the appropriate therapy. We present a rare case of a patient presenting with primary cutaneous blastomycosis that progressed to disseminated disease causing acute respiratory distress syndrome. High clinical suspicion, prompt diagnostic testing, and therapy with amphotericin B, confirmed the diagnosis and resulted in a swift recovery.
Blastomycosis is an infection caused by the fungus Blastomyces dermatitidis, which is endemic to areas of the United States and Canada including the Great Lakes Region and the Mississippi and Ohio River Valleys.1,2 Exposure occurs in moist wooded areas during outdoor activities when fungal microhabitats existing in soil are disturbed. Inhaled conidia can result in a primary lung infection, which may then become disseminated.3,4 Pulmonary disease is the most common manifestation of blastomycosis with isolated lung disease occurring in 60 to 75 percent of infected people.5 In the remaining group, dissemination to skin, bone, genitourinary, and other organ systems can be seen.4 In fewer than 10 percent of cases, blastomycosis can progress to acute respiratory distress syndrome (ARDS) with dyspnea, tachypnea, and hypoxemia as systemic manifestations.6–12
Palmer and McFadden reported the first case of disseminated blastomycosis causing ARDS in 1968.13 Since then, few studies have identified disseminated blastomycosis as a cause of ARDS (Table 1). Our review of these reports revealed that out of 33 patients with ARDS secondary to blastomycosis, 21 deaths resulted. Although the exact mechanism is not fully known, systemic stimulation of inflammatory mediators gives a reasonable explanation for the high mortality rate of 40 to 60 percent described in the literature for all causes of ARDS.14 Thus, early suspicion of disseminated disease is especially helpful in endemic areas since rapid institution of therapy can improve morbidity and mortality.
Table 1.
Case reports of blastomycosis causing acute respiratory distress syndrome in the literature
| Author | Year | No. of Patients | Symptoms | Ventilation | Initial Treatment | Ultimate Treatment | Survival |
|---|---|---|---|---|---|---|---|
| Palmer et al13 | 1968 | 1 | fatigue, general malaise, cough with sputum, shortness of breath, fever | 0 of 1 | penicillin | amphotericin B | 0/1 (0%) |
| Griffith et al11 | 1979 | 1 | fever, malaise, dyspnea, cough | 1 of 1 | penicillin + gentamicin + methylprednisolone + digoxin | amphotericin B + hydroxystilbamidine | 1/1 (100%) |
| Lockridge et al8 | 1979 | 1 | pleuritic chest pain, fever, shortness of breath, cough with sputum production | 1 of 1 | aspirin | multiple antibiotics + amphotericin B + high-dose steroids | 0/2 (0%) |
| Evans et al7 | 1982 | 2 | fever, cough, right upper lobe pneumonia, dyspnea | 1 of 2 | 1) isoniazid + ethambutol 2) cephalothin + erythromycin | 1) amphotericin B + hydroxystilbamidine + highdose methylprednisolone 2) cefazolin + tobramycin + erythromycin + isoniazid + sulfamethoxazole + methylprednisolone | 0/2 (0%) |
| Atkinson et al90 | 1983 | 1 | fever, cough, dyspnea | 1 of 1 | cephalothin | multiple antibitoics + isoniazide + highdose methylprednisolone | 0/1 (0%) |
| Thiele et al91 | 1984 | 1 | left ear pain and discharge | 1 of 1 | penicillin + chloramphenicol + tobramycin + nafcillin | isoniazid + rifampin + ethambutol + ketoconazole + amphotericin B | 0/1 (0%) |
| Skillrud et al60 | 1985 | 1 | dyspnea on exertion, fatigue, shaking chills, nearsyncopal episode | 1 of 1 | cefazolin + cefoxitin + erythromycin + tobramycin + clindamycin | amphotericin B | 1/1 (100%) |
| Unger92 | 1986 | 1 | cough, fever, bloody sputum | 1 of 1 | multiple antibiotics | amphotericin B | 1/1 (100%) |
| MacDonald93 | 1990 | 1 | cough, dyspnea | 1 of 1 | amphotericin B | amphotericin B | 1/1 (100%) |
| Renston et al94 | 1992 | 1 | fever, chills, sweats, cough, pain and swelling of right knee | 1 of 1 | multiple antibiotics + antituberculosis drugs | amphotericin B | 1/1 (100%) |
| Meyer et al6 | 1993 | 10 | cough, chills, fever, dyspnea | 9 of 10 | multiple antibiotics | amphotericin B + ketoconazole + rifampin | 5/10 (50%) |
| Craft59 | 1995 | 1 | fever, cough, chills, hemoptysis, rightsided pleuritic chest pain | 1 of 1 | multiple antibiotics | fluconazole + rifampin + pyrazinamide + amikacin + ethambutol + vancomycin + isoniazid + amphotericin B + itraconazole | 1/1 (100%) |
| Mukkamala et al95 | 1997 | 2 | cough with sputum production, night sweats, weight loss, headache, backache, shortness of breath | 2 of 2 | amphotericin B | amphotericin B | 0/2 (0%) |
| Mundey et al10 | 2001 | 1 | fever, chills, cough without sputum, weakness, diarrhea | 1 of 1 | ampicillin/sulbactam + ceftazidime + gentamicin | azithromycin + amphotericin B | 0/1 (0%) |
| Amini96 | 2007 | 1 | fever, cough | 0 of 1 | piperacillin/tazobactum + levofloxacin | amphotericin B | 0/1 (0%) |
| Gauthier et al48 | 2007 | 6 | fever, cough, skin lesions | 0 of 6 | immunosuppressive agents + antibiotics + antiviral agents | amphotericin B, itraconazole, voriconazole | 2/6 (33%) |
| Watts et al97 | 2007 | 1 | suprapubic pain with inability to urinate, fever, pruritic lesions of arms, face, and trunk, right ankle pain | 1 of 1 | gatifloxacin | vancomycin + piperacillin/tazobactum +ciprofloxacin + amphotericin B | 0/1 (0%) |
Blastomycosis may seldom present as a primary cutaneous lesion after traumatic inoculation from laboratory or autopsy exposure, animal bites or scratches, and outdoor trauma.15,16 A total of 22 cases of cutaneous inoculation blastomycosis were compiled for a major article, reviewing literature from 1903 to 2002.17 The clinical presentation of infected patients is variable and symptoms of infection may be absent, chronic, acute, or even fulminant. Primary cutaneous blastomycosis is often mistaken for other cutaneous entities such as keratoacanthoma, squamous cell carcinoma, tuberculosis, tertiary syphilis, leprosy, or bacterial pyoderma.18
We describe a rare case of a patient with an unhealed cutaneous lesion who underwent surgical debridement and postoperatively developed life-threatening disseminated blastomycosis progressing to ARDS. With a high index of clinical suspicion, rapid diagnosis, and prompt therapy with amphotericin B (AmB), the patient recovered.
Case Report
A 49-year-old man with a past medical history of type 2 diabetes mellitus (T2DM) and hypertension presented with a history of right knee pain and swelling. The patient had sustained a small bruise on his right knee following minor trauma eight months previously. The bruise resolved spontaneously; however, approximately three months prior to presentation, he noted onset of pain and swelling over the right knee. The pain and swelling were associated with intermittent bloody and purulent discharge from a cutaneous lesion that had developed. Over the next three months, he had multiple right knee fluid aspirations with fluid analysis that showed no crystals, minimal white blood cells, and no growth on bacterial culture. No mycobacterial or deep fungal cultures of either the aspirated fluid or wound discharge were requested. As an outpatient, he had been treated empirically for gouty arthritis and had two courses of oral antibiotics. The patient’s review of systems was significant only for subjective fevers. He denied chills, shortness of breath, cough, or hemoptysis.
On initial presentation, the patient’s temperature was 100.2°F, heart rate 102 beats per minute (bpm), respiratory rate 14, blood pressure 160/70mmHg, and oxygen saturation 97 percent on room air. The chest auscultatory findings were normal bilaterally. The most pertinent physical examination finding was a dark purple-black eschar over the anterior surface of the right knee, with punctate hemorrhage and purulent drainage (Figure 1). The right knee was exquisitely tender to light palpation, and he experienced severe pain on passive range of motion. Bacterial wound and blood cultures were taken before intravenous (IV) vancomycin and ceftriaxone were started. The wound was then debrided in the operating room. Three days after debridement, the patient was noted to be acutely short of breath with a respiratory rate of 24, febrile with a temperature of 103.3°F, and hypoxemic with an oxygen saturation of 80 percent on room air.
Figure 1.

Dark purpleblack eschar over the anterior surface of the right knee
A chest radiograph revealed diffuse bilateral pulmonary infiltrates (Figure 2). Computed tomography of the chest showed no evidence of pulmonary embolism (Figure 3). A transthoracic echocardiogram revealed no valvular pathology and ejection fraction was 75 percent. Because of high suspicion for blastomycosis, another specimen obtained from the knee was stained with methamine silver, which subsequently revealed broadbased budding yeast (Figures 4a–4c). The patient began AmB at a dose of 1mg/kg/day. The patient required supplemental oxygen by face mask, but not ventilatory support. The patient’s hospital course was complicated by acute renal insufficiency attributed to the AmB therapy. Liposomal AmB was substituted with subsequent stabilization of renal function. Clinical improvement was gradually seen and the patient was discharged on the 17th day of hospitalization with a six-month course of itraconazole therapy (200mg orally twice daily). The patient continued close follow up with the infectious disease service as an outpatient for a duration of nine months and is currently fully recovered.
Figure 2.
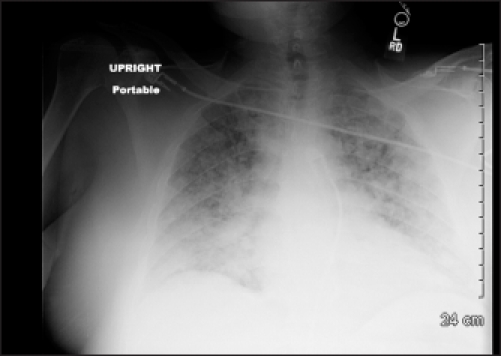
Bilateral pulmonary infiltrates revealed by chest radiograph
Figure 3.
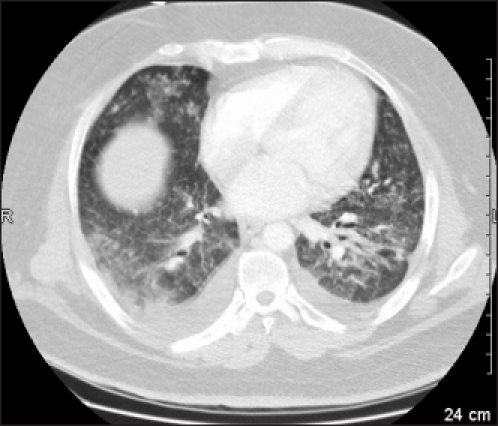
Computed tomography of the chest demonstrating bilateral pulmonary infiltrates without any pulmonary embolism
Figure 4a–4c.
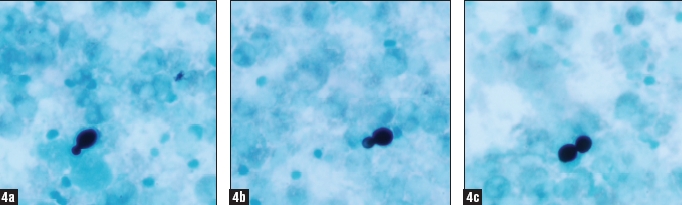
Right-knee aspiration stained with methamine silver demonstrating multiple broad-based budding yeast forms
Discussion
B. dermatitidis is a fungal pathogen that can affect any mammalian host. It is a common pulmonary and cutaneous mycosis encountered in people living in southeastern states near the Mississippi and Ohio River basins and the Midwestern states and Canadian provinces bordering the Great Lakes.1,2 Infection with B. dermatitidis is known as Gilchrist’s disease, named after the Johns Hopkins pathologist who was first to describe the disease in 1894. The disease has also been called Chicago’s disease because of early case reports from that area.15
In 1951, Schwarz and Baum emphasized that the portal of entry in humans is the respiratory tract rather than the skin, as was previously believed.19 It was discovered that infection occurred by inhalation of aerosolized conidial forms of the organism, which grow in warm, moist soils of wooded areas rich in organic debris.4,20 After inhalation, the conidia transform to yeast which, with a thick cell wall, confer resistance to phagocytosis allowing for rapid growth, noncaseating granuloma formation, and progression to an intense inflammatory reaction allowing for dissemination. Extrapulmonary sites of blastomycosis include skin (20–40%), bone (10–25%), prostate and genitourinary organs (5–15%), and the central nervous system (5%).3, 21–29
Since this landmark discovery, it has been widely accepted that most cases of cutaneous blastomycosis occur after hematogenous spread from a primary pulmonary infection, even in the absence of overt pulmonary disease.30 Most cases of secondary cutaneous infection have no associated pulmonary findings on chest radiograph.31–33 Primary cutaneous blastomycosis may result as a traumatic inoculation event, but systemic spread from cutaneous lesions rarely occurs.34
There is no established common link among patients developing blastomycosis infection with respect to underlying disease, immunosuppression, age, sex, occupation, or other factors. However, in multiple epidemiological studies, the majority of patients with blastomycosis were men who were immunocompetent.35 The male prevalence likely reflects occupational exposure in agricultural work and manual labor in endemic 15,23,36 Many reports have been published of patients who lived in endemic areas and often participated in activities in the wooded outdoors. Numerous cases in the literature draw attention to blastomycosis infection in hunters and their hunting dogs simultaneously.37–39
The varied clinical presentation of blastomycosis ranges from a subclinical asymptomatic infection or a more severe disseminated infection presenting with acute respiratory failure.40 A fulminant course may present in both immunocompetent and immunocompromised hosts. Skin lesions are the most common presenting feature of extrapulmonary blastomycosis, but may present after cutaneous trauma, transmitting the fungus into the skin. In a patient with cutaneous disease and no evidence of pulmonary disease, current concepts presume an underlying pulmonary infection or one that may have resolved spontaneously. Cellular immunity is considered to be the major protective factor in preventing progressive disease.41 Unlike other fungi causing systemic mycosis, B. dermatitidis has been reported as significant in only a small number of patients who are immunocompromised, such as those with HIV infection.42,43
Skin manifestations of blastomycosis are often very striking, thus the initial cases were reported as primarily dermatologic.2,3 Lesions are more common on the face, neck, and extremities and begin as papules, pustules, or subcutaneous nodules. Typical lesions are verrucous plaques or cutaneous ulcers, frequently with a distinctive purpleblue halo that may suppurate and spontaneously drain, forming deep cutaneous ulcers. The lesions can easily be mistaken for pyoderma gangrenosum, squamous cell carcinoma, and other chronic cutaneous infections, such as sporotrichosis, nocardiosis, atypical mycobacteriosis, tularemia, anthrax, or leishmaniasis.22–24
Although cutaneous blastomycosis is most often secondary to dissemination, self-inoculation has been documented. In an article by Wilson et al,16 four cases were documented—three by accidental cutaneous puncture wounds while performing autopsies and one in a pathologist who worked with fungi and inadvertently noted an indolent abscess on his left wrist that, after evacuation, persisted as a papule with a central crater. B. dermatitidis was demonstrated by microscopic examination of pus taken from the primary lesion and was later recovered in culture. All cases were treated with local wound care and none resulted in disseminated disease.16,44
Gray and Baddour17 summarized published cases of inoculation and established that the physical examination of lesions cannot differentiate primary cutaneous inoculation from disseminated lesions. Lesions were nonspecific and variably described as: verrucous, nodular, papular, and chancreform.17 Alternatively, Rutland and Horenstein suggested that inoculation blastomycosis is often associated with painful lympadenopathy, induration and chancre formation, and spontaneous resolution— clinical features that can help to differentiate primary inoculation from an asymptomatic dissemination.45
Pulmonary blastomycosis is less commonly recognized than the cutaneous form.46 Patients can present with an acute or chronic pneumonia with fever, cough, weight loss, night sweats, and hemoptysis that does not respond to empiric antibiotics. Chest radiographs often reveal diffuse interstitial infiltrates lacking cardiomegaly, pleural effusions, and vascular redistribution; although it is often difficult to distinguish these features from cardiogenic pulmonary edema.47 In fewer than 10 percent of cases, blastomycosis has a fulminant course manifesting as fevers, chills, and shortness of breath, which can progress to ARDS.6–9 Patients often require ventilator assistance within a few days of admission.
Meyer et al6 reported a 57-year-old man who presented with pain and swelling in his right elbow. On the second day of hospitalization, large numbers of broadbased budding yeast forms were identified on a wet mount of tracheal secretions and treatment ensued with AmB. Severe tachypnea and hypoxemia required the use of mechanical ventilatory support for 50 days. The patient’s recovery was slow and complicated, but he was discharged home after 75 days of hospitalization.6 Many studies highlight the extremely high mortality of ARDS secondary to blastomycosis dissemination.35,48
The most expeditious way to diagnose blastomycosis is to demonstrate the budding yeast on 10% KOH preparation, Gomori’s stain, periodic acid-Schiff stain, or Papanicolaou’s smear of tissue biopsy specimens, tracheal aspirates, bronchoalveolar lavage fluid, or sputum.15,22,49,50 B. dermatitidis appears as single or budding spherical cells, 8 to 15µm in diameter, with thick cell walls and daughter cells that are nearly as large as the mother cell before separation.1,51 KOH preparations should be followed by tissue cytological analysis or fungal culture on Sabouraud dextrose agar at room temperature.34 The latter is the most accurate method of diagnosis, although results can require up to four weeks.46,49,52,53 Multiple authors have demonstrated that high diagnostic yields can be obtained from culture of specimens, regardless of the method of collection.54,55 Although microscopic broadbased budding yeast is often diagnostic, fungal cultures of skin biopsies should always be done, especially when microscopy is negative or inconclusive. Skin testing and serodiagnosis of blastomycosis currently have very limited roles in diagnosis because of poor sensitivity and specificity as a result of cross-reactivity with other fungi.33,56,57 In two large series of cultureproven blastomycosis, 85 to 100 percent of patients had negative blastomycin skin tests.3 Recently developed enzyme immunoassay (EIA) using a yeast phase antigen (A antigen) of B. dermatitidis has been shown to be more sensitive; however, its use is limited due to poor availability.49 Klein et al described antibody detection by complement fixation, immunodiffusion, and EIA to be 9 percent, 28 percent, and 77 percent, respectively.40 Thus, a negative test result should not exclude a diagnosis of blastomycosis and a positive test result requires further examination by microscopy or culture. Klein and Jones have isolated a surface protein of the fungus useful in detection of antibodies in patients in a research setting.58
In cases presenting with cutaneous manifestations, skin biopsy with histological hematoxylin and eosin (H&E) analysis and silver stain may reveal the organism.59–63 Skin biopsy shows histologic evidence of papillomatosis, downward proliferation of the epidermis with intraepidermal microabscesses, and an inflammatory or granulomatous reaction in the dermis.64,65 The hyperplasia and acanthosis may suggest other diagnoses unless fungi are sought with specific stains. The histological changes may prompt an erroneous diagnosis of squamous cell carcinoma or keratoacanthoma.44
Various antifungal drugs are available for the treatment of blastomycosis. Before antifungal therapy was available, the fatality rate among patients with disseminated blastomycosis was 21 to 78 percent.63–65 However, fatality rates dropped significantly after the introduction of AmB in 1956.66–69 Cases of patients with localized blastomycosis who spontaneously recovered without antifungal therapy have been reported.4,70 Nonetheless, oral antifungal agents have become the standard of care for inoculation or pulmonary blastomycosis and AmB the standard of care for disseminated disease.
Important consideration should be given to three factors when deciding upon the appropriate treatment for a patient with blastomycosis: the clinical presentation and the severity of disease, the immune status of the patient, and the toxicity of the antifungal agent.71 In the immunocompetent host, acute blastomycosis may be mild or self-limited requiring treatment only to prevent extrapulmonary dissemination. Patients presenting with severe pneumonia or ARDS, disseminated infection, or those who are immunocompromised, require aggressive antifungal therapy. In 2007, a panel of infectious disease specialists from North America with expertise in blastomycosis met to develop guideline recommendations for the treatment of blastomycosis based on results from several prospective, multicenter treatment trials of individual antifungal agents (Table 2).5
Table 2.
Clinical practice guidelines for the treatment of blastomycosis5
| Manifestation | Preferred Treatment | Comments |
|---|---|---|
| Table adapted from Chapman SW, Dismukes WE, Prioa LA, et al. Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801–1812. | ||
| Mild-to-moderate pulmonary and primary cutaneous | Itraconazole 200mg once or twice per day for 6–12 months | Reports of spontaneous resolution. No recommendation on the use of corticosteroids |
| Moderate-to-severe pulmonary | Lipid AmB 3–5mg/kg/day or deoxycholate AmB 0.7–1mg/kg/day for 1–2 weeks followed by itraconazole 200mg bid for 6–12 months | The entire course of therapy can be given with deoxycholate AmB to a total of 2g; however, most clinicians prefer to use stepdown itraconazole therapy after the patient’s condition improves. The lipid formulations of AmB have fewer adverse effects. Possible use of corticosteroids |
| Mild-to-moderate disseminated | Itraconazole 200mg once or twice per day for 6–12 months | Treat osteoarticular disease for 12 months |
| Moderate-to-severe disseminated | Lipid AmB 3–5mg/kg/day or deoxycholate AmB 0.7–1mg/kg/day for 1–2 weeks followed by itraconazole 200mg bid for 12 months | The entire course of therapy can be given with deoxycholate AmB to a total of 2g; however, most clinicians prefer to use stepdown itraconazole therapy after the patient’s condition improves. The lipid formulations of AmB have fewer adverse effects. Treat osteoarticular disease for 12 months. Possible use of corticosteroids |
| Immunosuppressed patients | Lipid AmB 3–5mg/kg/day or deoxycholate AmB 0.7–1mg/kg/day for 1–2 weeks followed by itraconazole 200mg bid for 12 months | Lifelong suppressive treatment may be required if immunosuppression cannot be reversed |
- AmB
amphotericin
- bid
twice per day
Itraconazole is now considered the agent of choice for non-life-threatening blastomycosis with fluconazole, voriconazole, and posaconazole having a role in selected patients.49 In 1976, a multicentered clinical trial of low-dose (400mg/day) compared to high-dose (800mg/day) ketoconazole for six months reported cure rates of 79 and 100 percent, respectively.72–76 However, relapse rates were more common after ketoconazole (10–14%) as compared to AmB (4%). Thus patients treated with ketoconazole require close clinical follow up of one to two years after discontinuation.52 Compared with ketoconazole, itraconazole has enhanced antifungal activity and is firstline therapy for nondisseminated blastomycosis.41,77 Bradsher et al noted success for a cohort of 42 patients treated with itraconazole at a dosage of 200mg/day.78 Cure rates of up to 90 percent have been reported after a sixmonth treatment regimen of 200–400mg/day of itraconazole.77 The same therapy is effective for primary pulmonary blastomycosis.
For disseminated blastomycosis, a total dosage of AmB >1g has resulted in cure without relapse in 77 to 91 percent of patients, and a total dosage >2g has resulted in cure rates of 97 percent.49,79,80 Although not studied in controlled human trials, clinical experience suggests that lipid formulations of AmB are as effective as the deoxycholate formulation and are associated with less toxicity.81–83 AmB is safe for use and equally effective in immunocompromised and pregnant hosts.
The major limiting factor to the use of these medications for the treatment of blastomycosis is the multiple significant adverse drug effects and serious drug interactions they present. AmB has been associated with decline in renal function leading to renal failure and anemia, and infusion-related toxicities such as fever, rigors, myalgia, headache, and anaphylaxis. Ketoconazole causes hormonal abnormalities, significant drug interactions, life-threatening arrhythmias, nausea and vomiting, and hepatitis.2,84,85 Itraconazole is generally well tolerated, although side effects include pedal edema and congestive heart failure, hypokalemia, elevated liver enzymes, drug interactions, and torsade de pointes.73,86–88
While corticosteroids are recommended for the treatment of severe pulmonary infections with Pneumocystis jirovecii and Histoplasma capsulatum, no consensus exists regarding their role in the treatment of the host inflammatory response seen in pulmonary blastomycosis. Lahm et al89 reported two cases of pulmonary blastomycosis that quickly advanced to ARDS despite treatment with AmB at 1mg/kg/day. In both cases, the addition of methylprednisolone (60mg IV every 6 hours vs. 250mg IV every 6 hours) resulted in marked clinical improvement over the next 5 to 7 days. The authors concluded that although routine use of steroids in 9. ARDS is not recommended, it may be initiated and show a benefit in a subset of patients who present with an exaggerated immune response. It is thought that a blastomycosis-induced hyperinflammation syndrome 10. contributes to the clinical deterioration and respiratory failure despite adequate treatment with antifungal therapy.89 There is currently no recommendation on the 11. use of corticosteroids in primary cutaneous fungal disease.
Summary
Blastomycosis has become an increasingly recognized serious infection that can present in any type of patient and may mimic many other conditions; thus, a high index of suspicion is required when assessing skin and pulmonary infections in areas endemic with B. dermatitidis. A thorough history and physical examination with microbiologic laboratory testing can assist the physician in making correct clinical and diagnostic decisions when presented with pertinent symptoms. We have described a case of a patient who presented with a nonhealing cutaneous lesion despite multiple surgical and medical treatments. Only after progression to ARDS was an accurate and swift diagnosis obtained. Although rare, progression to ARDS can have a strikingly high mortality rate. Prompt therapy with antifungal agents and possibly steroids can result in an improved outcome. Proper diagnosis relies on maintaining a high level of clinical suspicion and subsequent laboratory evaluation and initiation of appropriate therapy.
Acknowledgments
The authors wish to thank Brian Marciniak for his writing and editing assistance.
References
- 1.Fang W, Washington L, Kumar N. Imaging manifestations of blastomycosis: a pulmonary infection with potential dissemination. Radiographics. 2007;27(3):641–655. doi: 10.1148/rg.273065122. [DOI] [PubMed] [Google Scholar]
- 2.Witorsch P, Utz JP. North American blastomycosis: a study of 40 patients. Medicine (Baltimore) 1968;47(3):169–200. doi: 10.1097/00005792-196805000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Sarosi GA, Davies SF. Blastomycosis. Am Rev Respir Dis. 1979;120(4):911–938. doi: 10.1164/arrd.1979.120.4.911. [DOI] [PubMed] [Google Scholar]
- 4.Klein BS, Vergeront JM, Weeks RJ, et al. Isolation of Blastomyces dermatitidis in soil associated with a large outbreak of blastomycosis in Wisconsin. N Engl J Med. 1986;314(9):529–534. doi: 10.1056/NEJM198602273140901. [DOI] [PubMed] [Google Scholar]
- 5.Chapman SW, Dismukes WE, Prioa LA, et al. Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801–1812. doi: 10.1086/588300. [DOI] [PubMed] [Google Scholar]
- 6.Meyer KC, McManus EJ, Maki DG. Overwhelming pulmonary blastomycosis associated with the adult respiratory distress syndrome. N Engl J Med. 1993;329(17):1231–1236. doi: 10.1056/NEJM199310213291704. [DOI] [PubMed] [Google Scholar]
- 7.Evans ME, Haynes JB, Atkinson JB, et al. Blastomyces dermatitidis and the adult respiratory distress syndrome. Case reports and review of the literature. Am Rev Respir Dis. 1982;126(6):1099–1102. doi: 10.1164/arrd.1982.126.6.1099. [DOI] [PubMed] [Google Scholar]
- 8.Lockridge RS, Glauser F. Adult respiratory distress syndrome secondary to diffuse pulmonary blastomycosis. South Med J. 1979;72(2):235–236. doi: 10.1097/00007611-197902000-00031. [DOI] [PubMed] [Google Scholar]
- 9.Lemos LB, Baliga M, Guo M. Acute respiratory distress syndrome and blastomycosis: presentation of nine cases and review of the literature. Ann Diagn Pathol. 2001;5(1):1–9. doi: 10.1053/adpa.2001.21473. [DOI] [PubMed] [Google Scholar]
- 10.Mundey K, Varkey B, VanRuiswyk J, et al. Acute respiratory distress syndrome from blastomycosis: a case report. WMJ. 2001;100(7):40–42. [PubMed] [Google Scholar]
- 11.Griffith JE, Campbell GD. Acute miliary blastomycosis presenting as fulminating respiratory failure. Chest. 1979;75(5):630–632. doi: 10.1378/chest.75.5.630. [DOI] [PubMed] [Google Scholar]
- 12.Arvanitakis C, Sec SK, Magnin GE. Fulminating fatal pneumonia due to blastomycosis. Am Rev Respir Dis. 1972;105(5):827–831. doi: 10.1164/arrd.1972.105.5.827. [DOI] [PubMed] [Google Scholar]
- 13.Palmer PE, McFadden SW. Blastomycosis: report of an unusual case. N Engl J Med. 1968;279(18):979–983. doi: 10.1056/NEJM196810312791806. [DOI] [PubMed] [Google Scholar]
- 14.Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–1349. doi: 10.1056/NEJM200005043421806. [DOI] [PubMed] [Google Scholar]
- 15.Steck WD. Blastomycosis. Dermatol Clin. 1989;7(2):241–250. [PubMed] [Google Scholar]
- 16.Wilson JW, Cawley EP, Weidman FD, Gilmer WS. Primary cutaneous North American blastomycosis. Arch Dermatol. 1955;71(1):39–45. doi: 10.1001/archderm.1955.01540250041008. [DOI] [PubMed] [Google Scholar]
- 17.Gray NA, Baddour LM. Cutaneous inoculation blastomycosis. [Epub 2002 Apr 17];Clin Infect Dis. 2002 34(10):e44–49. doi: 10.1086/339957. [DOI] [PubMed] [Google Scholar]
- 18.Body BA. Cutaneous manifestations of systemic mycoses. Dermatol Clin. 1996;14(1):125–135. doi: 10.1016/s0733-8635(05)70332-6. [DOI] [PubMed] [Google Scholar]
- 19.Schwarz J, Baum GL. Blastomycosis. Am J Clin Pathol. 1951;21(11):999–1029. doi: 10.1093/ajcp/21.11.999. [DOI] [PubMed] [Google Scholar]
- 20.Chapman SW, Lin AC, Hendricks KA, et al. Endemic blastomycosis in Mississippi: epidemiological and clinical studies. Semin Respir Infect. 1997;12(3):219–228. [PubMed] [Google Scholar]
- 21.Furcolow ML, Busey JF, Menges RW, Chick EW. Prevalence and incidence studies of human and canine blastomycosis. (II. Yearly incidence studies in three selected states, 1960-1967).Am J Epidemiol. 1970;92(2):121–131. doi: 10.1093/oxfordjournals.aje.a121184. [DOI] [PubMed] [Google Scholar]
- 22.Chapman SW. In: Blastomycosis dermatitidis. Principles and Practice of Infectious Diseases. Mandell GL, Bennett JE, Dolin R, editors. New York: Churchill Livingstone; 2000. pp. 2733–2746. [Google Scholar]
- 23.Schwarz J, Salfelder K. Blastomycosis: a review of 152 cases. Curr Top Pathol. 1977;65:165–200. [PubMed] [Google Scholar]
- 24.Pappas PG, Dismukes WE. Blastomycosis: Gilchrist’s disease revisited. Curr Clin Top Infect Dis. 2002;22:61–77. [PubMed] [Google Scholar]
- 25.Eikenburg HU, Amin HU, Lich R. Blastomycosis of the genitourinary tract. J Urol. 1975;113:650–652. doi: 10.1016/s0022-5347(17)59545-2. [DOI] [PubMed] [Google Scholar]
- 26.Beuchner HA, Clawson CM. Blastomycosis of the central nervous system. II. A report of nine cases from the Veterans Administration Cooperative Study. Am Rev Respir Dis. 1967;95(5):820–826. doi: 10.1164/arrd.1967.95.5.820. [DOI] [PubMed] [Google Scholar]
- 27.Gonyea EF. The spectrum of primary blastomycosis meningitis: a review of central nervous system blastomycosis. Ann Neurol. 1978;3(1):26–39. doi: 10.1002/ana.410030106. [DOI] [PubMed] [Google Scholar]
- 28.Friedman JA, Wijdicks EF, Fulgham JR, Wright AJ. Meningoencephalitis due to Blastomycosis dermatitidis: case report and literature review. Mayo Clin Proc. 2000;75(4):403–408. doi: 10.4065/75.4.403. [DOI] [PubMed] [Google Scholar]
- 29.Roos KL, Bryan JP, Maggio WW, et al. Intracranial blastomycoma. Medicine (Baltimore) 1987;66(3):224–235. doi: 10.1097/00005792-198705000-00006. [DOI] [PubMed] [Google Scholar]
- 30.Mason AR, Cortes GY, Cook J, et al. Cutaneous blastomycosis: a diagnostic challenge. Int J Dermatol. 2008;47(8):824–830. doi: 10.1111/j.1365-4632.2008.03732.x. [DOI] [PubMed] [Google Scholar]
- 31.Bradsher RW, Rice DC, Abernathy RS. Ketoconazole therapy of endemic blastomycosis. Ann Intern Med. 1985;103(6):872–879. doi: 10.7326/0003-4819-103-6-872. [DOI] [PubMed] [Google Scholar]
- 32.Halvorsen RA, Duncan JD, Merten DF, et al. Pulmonary blastomycosis: radiologic manifestations. Radiology. 1984;150(1):1–5. doi: 10.1148/radiology.150.1.6689749. [DOI] [PubMed] [Google Scholar]
- 33.Sarosi GA, Davies SF. Blastomycosis. Compr Ther. 1986;12(4):31–37. [PubMed] [Google Scholar]
- 34.Koneman EW, Allen SD, Janda WM, et al. Color Atlas and Textbook of Diagnostic Microbiology. Philadelphia, Pa: Lippinicott-Raven; 1997. [Google Scholar]
- 35.Vasquez JE, Mehta JB, Agrawal R, Sarubbi FA. Blastomycosis in northeast Tennessee. Chest. 1998;114(2):436–443. doi: 10.1378/chest.114.2.436. [DOI] [PubMed] [Google Scholar]
- 36.Baum GL, Schwarz J. North American blastomycosis. Am J Med Sci. 1959;238 [Google Scholar]
- 37.Armstrong CW, Jenkins SR, Kaufman L, et al. Common-source outbreak of blastomycosis in hunters and their dogs. J Infect Dis. 1987;155(3):568–570. doi: 10.1093/infdis/155.3.568. [DOI] [PubMed] [Google Scholar]
- 38.McDonough ES, Kuzma JF. Epidemiological studies on blastomycosis in the state of Wisconsin. Sabouraudia. 1980;18(3):173–183. doi: 10.1080/00362178085380321. [DOI] [PubMed] [Google Scholar]
- 39.Sarosi GA, Eckman MR, Davies SF, Laskey WK. Canine blastomycosis as a harbinger of human disease. Ann Intern Med. 1979;91(5):733–735. doi: 10.7326/0003-4819-91-5-733. [DOI] [PubMed] [Google Scholar]
- 40.Klein BS, Vergeront JM, Kaufman L, et al. Serological tests for blastomycosis: assessments during a large point-source outbreak in Wisconsin. J Infect Dis. 1987;155(2):262–268. doi: 10.1093/infdis/155.2.262. [DOI] [PubMed] [Google Scholar]
- 41.Pappas PG, Pottage JC, Powderly WG, et al. Blastomycosis in patients with the acquired immunodeficiency syndrome. Ann Intern Med. 1992;116(10):847–853. doi: 10.7326/0003-4819-116-10-847. [DOI] [PubMed] [Google Scholar]
- 42.Pappas PG. Blastomycosis in the immunocompromised patient. Semin Respir Crit Care Med. 1997;12:243–251. [PubMed] [Google Scholar]
- 43.Herd AM, Greenfield SB, Thompson GW, Brunham RC. Miliary blastomycosis and HIV infection. CMAJ. 1990;143(12):1329–1330. [PMC free article] [PubMed] [Google Scholar]
- 44.Bradsher RW, Martin MR, Wilkes TD, et al. Unusual presentations of blastomycosis: ten case summaries. Infect Med. 1990;7:10–19. [Google Scholar]
- 45.Rutland BM, Horenstein MG. A 53-year-old man with an anterior knee fungating mass. Cutaneous blastomycosis. Arch Pathol Lab Med. 2005;129(5):e132–133. doi: 10.5858/2005-129-e132-AYMWAA. [DOI] [PubMed] [Google Scholar]
- 46.O’Neill RP, Penman RW. Clinical aspects of blastomycosis. Thorax. 1970;25(6):708–715. doi: 10.1136/thx.25.6.708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mortelliti MP, Manning H. Acute Respiratory Distress Syndrome. Am Fam Physician. 2002;65:1823–1830. [PubMed] [Google Scholar]
- 48.Gauthier GM, Safdar N, Klein BS, Andes DR. Blastomycosis in solid organ transplant recipients. Transpl Infect Dis. 2007;9(4):310–317. doi: 10.1111/j.1399-3062.2007.00227.x. [DOI] [PubMed] [Google Scholar]
- 49.Bradhser RW., Jr. Pulmonary blastomycosis. Semin Respir Crit Care Med. 2008;29(2):174–181. doi: 10.1055/s-2008-1063856. [DOI] [PubMed] [Google Scholar]
- 50.Sanders JS, Sarosi GA, Nollet DJ, Thompson JI. Exfoliative cytology in the rapid diagnosis of pulmonary blastomycosis. Chest. 1977;72(2):193–196. doi: 10.1378/chest.72.2.193. [DOI] [PubMed] [Google Scholar]
- 51.Cush R, Light RW, George RB. Clinical and roentgenographic manifestations of acute and chronic blastomycosis. Chest. 1976;69(3):345–349. doi: 10.1378/chest.69.3.345. [DOI] [PubMed] [Google Scholar]
- 52.Bradsher RW, Chapman SW, Pappas PG. Blastomycosis. Infect Dis Clin North Am. 2003;17(1):21–40. doi: 10.1016/s0891-5520(02)00038-7. [DOI] [PubMed] [Google Scholar]
- 53.Blastomycosis Cooperative Study of the Veterans Administration. Blastomycosis. A review of 198 cases. Amer Rev Resp Dis. 1964;89 doi: 10.1164/arrd.1964.89.5.659. [DOI] [PubMed] [Google Scholar]
- 54.Martynowicz MA, Prakash U. Pulmonary blastomycosis: an appraisal of diagnostic techniques. Chest. 2002;121(3):768–773. doi: 10.1378/chest.121.3.768. [DOI] [PubMed] [Google Scholar]
- 55.Trumbull ML, Chesney TM. The cytological diagnosis of pulmonary blastomycosis. JAMA. 1981;245(8):836–838. [PubMed] [Google Scholar]
- 56.Louria DB. Deep-seated mycotic infections, allergy to fungi and mycotoxins. New Engl J Med. 1967;277(21):1126–1134. doi: 10.1056/NEJM196711232772106. [DOI] [PubMed] [Google Scholar]
- 57.Davies SF, Sarosi GA. Serodiagnosis of histoplasmosis and blastomycosis. Am Rev Respir Dis. 1987;136(2):254–255. doi: 10.1164/ajrccm/136.2.254. [DOI] [PubMed] [Google Scholar]
- 58.Klein BS, Jones JM. Isolation, purification, and radiolabeling of a novel 120-kD surface protein on Blastomyces dermatitidis yeasts to detect antibody in infected patients. J Clin Invest. 1990;85(1):152–161. doi: 10.1172/JCI114406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Craft PP. A case report of disseminated blastomycosis and adult respiratory distress syndrome. J Fam Pract. 1995;40(6):597–600. [PubMed] [Google Scholar]
- 60.Skillrud DM, Douglas WW. Survival in adult respiratory distress syndrome caused by blastomycosis infection. Mayo Clin Proc. 1985;60(4):266–269. doi: 10.1016/s0025-6196(12)60320-6. [DOI] [PubMed] [Google Scholar]
- 61.Head AJ, Myers LK, Thomspon JD, et al. Disseminated blastomycosis presenting as oligoarticular septic arthritis in a 12-year-old girl. Arthritis Rheum. 2005;53(1):138–141. doi: 10.1002/art.20916. [DOI] [PubMed] [Google Scholar]
- 62.Stelling CB, Woodring JH, Rehm SR, et al. Miliary pulmonary blastomycosis. Radiology. 1984;150(1):7–13. doi: 10.1148/radiology.150.1.6689789. [DOI] [PubMed] [Google Scholar]
- 63.Smith JG, Jr., Harris JS, Conant NF, Smith DT. An epidemic of North American blastomycosis. JAMA. 1955;158(8):641–646. doi: 10.1001/jama.1955.02960080017005. [DOI] [PubMed] [Google Scholar]
- 64.Martin DS, Smith DT. Blastomycosis: I. A review of the literature. Am Rev Tuberc. 1939;39:275–304. [Google Scholar]
- 65.Abernathy RS. Clinical features of pulmonary blastomycosis. Ann Intern Med. 1959;51:707–727. doi: 10.7326/0003-4819-51-4-707. [DOI] [PubMed] [Google Scholar]
- 66.Lockwood WR, Alison F, Jr., Batson BE, Busey JF. The treatment of North American blastomycosis: ten years’ experience. Am Rev Respir Dis. 1969;100(3):314–320. doi: 10.1164/arrd.1969.100.3.314. [DOI] [PubMed] [Google Scholar]
- 67.Parker JD, Doto IL, Tosh FE. A decade of experience with blastomycosis and its treatment with amphotericin B. A National Communicable Disease Center Cooperative Mycoses Study. Am Rev Respir Dis. 1969;99(6):895–902. doi: 10.1164/arrd.1969.99.6.895. [DOI] [PubMed] [Google Scholar]
- 68.Seaburg JH, Dascomb HE. Results of the treatment of systemic mycosis. JAMA. 1964;188:509–513. doi: 10.1001/jama.1964.03060320031007. [DOI] [PubMed] [Google Scholar]
- 69.Busey JF. Blastomycosis. (III. A comparative study of 2-hydroxystilbamidine and amphotericin B therapy).Am Rev Respir Dis. 1972;105(5):812–818. doi: 10.1164/arrd.1972.105.5.812. [DOI] [PubMed] [Google Scholar]
- 70.Tosh FE, Hammerman KJ, Weeks RJ, Sarosi GA. A common source epidemic of North American blastomycosis. Am Rev Respir Dis. 1974;109(5):525–529. doi: 10.1164/arrd.1974.109.5.525. [DOI] [PubMed] [Google Scholar]
- 71.Bradsher RW. Blastomycosis. Clin Infect Dis. 1992;14(1):S82–90. doi: 10.1093/clinids/14.supplement_1.s82. [DOI] [PubMed] [Google Scholar]
- 72.McManus EJ, Jones JM. The use of ketoconazole in the treatment of blastomycosis. Am Rev Respir Dis. 1986;133(1):141–143. doi: 10.1164/arrd.1986.133.1.141. [DOI] [PubMed] [Google Scholar]
- 73.Centers for Disease Control and Prevention. Blastomycosis—North Carolina. MMWR. 1976;25:205–206. [Google Scholar]
- 74.Drake RG., Jr. North American blastomycosis: a review. J Ky Med Assoc. 1985;83(2):77–82. [PubMed] [Google Scholar]
- 75.Tuthill SW. Disseminated blastomycosis treated with ketoconazole. South Med J. 1986;79(9):1188–1189. doi: 10.1097/00007611-198609000-00044. [DOI] [PubMed] [Google Scholar]
- 76.NIAID. Treatment of blastomycosis and histoplasmosis with ketoconazole: results of a prospective randomized clinical trial. Ann Intern Med. 1985;103(6 Pt 1):861–872. [PubMed] [Google Scholar]
- 77.Dismukes WE, Bradsher RW, Jr., Cloud GC, et al. Itraconazole therapy for blastomycosis and histoplasmosis. NIAID Mycoses Study Group. Am J Med. 1992;93(5):489–497. doi: 10.1016/0002-9343(92)90575-v. [DOI] [PubMed] [Google Scholar]
- 78.Bradsher RW. Histoplasmosis and blastomycosis. Clin Infect Dis. 1996;22(2):S102–111. doi: 10.1093/clinids/22.supplement_2.s102. [DOI] [PubMed] [Google Scholar]
- 79.Bradsher RW, Pappas PG. Detection of specific antibodies in human blastomycosis by enzyme immunoassay. South Med J. 1995;88(12):1256–1259. doi: 10.1097/00007611-199512000-00013. [DOI] [PubMed] [Google Scholar]
- 80.Cook PP. Amphotericin B liquid complex for the treatment of recurrent blastomycosis of the brain in a patient previously treated with itraconazole. South Med J. 2001;94(5):548–549. [PubMed] [Google Scholar]
- 81.Perfect JR. Treatment of non-Aspergillus moulds in immunocompromised patients, with amphotericin B lipid complex. Clin Infect Dis. 2005;40(6):S401–S408. doi: 10.1086/429331. [DOI] [PubMed] [Google Scholar]
- 82.Panicker J, Walsh T, Kamani N. Recurrent central nervous system blastomycosis in an immunocompetent child treated successfully with sequential liposomal amphotericin B and voriconazole. Pediatr Infect Dis J. 2006;25(4):377–379. doi: 10.1097/01.inf.0000207475.89745.51. [DOI] [PubMed] [Google Scholar]
- 83.Chowfin A, Tight R, Mitchell S. Recurrent blastomycosis of the central nervous system: case report and review. Clin Infect Dis. 2000;30(6):969–971. doi: 10.1086/313828. [DOI] [PubMed] [Google Scholar]
- 84.Abernathy RS. Amphotericin therapy of North American blastomycosis. Antimicrob Agents Chemother (Bethesda) 1966;6:208–211. [PubMed] [Google Scholar]
- 85.Heidemann HT, Gerkens JF, Spickard WA, et al. Amphotericin B nephrotoxicity in humans decreased by salt repletion. Am J Med. 1983;75(3):476–481. doi: 10.1016/0002-9343(83)90353-4. [DOI] [PubMed] [Google Scholar]
- 86.Gallis HA, Drew RH, Pickard WW. Amphotericin, B: 30 years of clinical experience. Rev Infect Dis. 1990;12(2):308–329. doi: 10.1093/clinids/12.2.308. [DOI] [PubMed] [Google Scholar]
- 87.Ahman SR, Singer SJ, Leissa BG. Congestive heart failure associated with itraconazole. Lancet. 2001;357(9270):1766–1777. doi: 10.1016/S0140-6736(00)04891-1. [DOI] [PubMed] [Google Scholar]
- 88.Pohjola-Sintonen S, Viitasalo M, Toivonene L, Neuvonen P. Torsades de pointes after terfenadine-itraconazole interaction. BMJ. 1993;306(6871) doi: 10.1136/bmj.306.6871.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Lahm T, Neese S, Ober M, et al. Reversal of refractory blastomycosisinduced acute respiratory distress syndrome with corticosteroids. Chest. 2007;132 [Google Scholar]
- 90.Atkinson JB, McCurley TL. Pulmonary blastomycosis: filamentous forms in an immunocompromised patient with fulminating respiratory failure. Hum Pathol. 1983;14(2):186–188. doi: 10.1016/s0046-8177(83)80250-0. [DOI] [PubMed] [Google Scholar]
- 91.Thiele JS, Buechner HA, Deshotels SJ., Jr. Blastomycosis and the adult respiratory distress syndrome. J La State Med Soc. 1984;136(11):38–40. [PubMed] [Google Scholar]
- 92.Unger JM, Peters ME, Hinke ML. Chest case of the day. AJR Am J Roentgenol. 1986;146(5):1080–1086. doi: 10.2214/ajr.146.5.1080. [DOI] [PubMed] [Google Scholar]
- 93.MacDonald D, Alguire PC. Adult respiratory distress syndrome due to blastomycosis during pregnancy. Chest. 1990;98(6):1527–1528. doi: 10.1378/chest.98.6.1527. [DOI] [PubMed] [Google Scholar]
- 94.Renston JP, Morgan J, Dimarco AF. Disseminated miliary blastomycosis leading to acute respiratory failure in an urban setting. Chest. 1992;101(5):1463–1465. doi: 10.1378/chest.101.5.1463. [DOI] [PubMed] [Google Scholar]
- 95.Mukkamala R, Metha JB, Myers JW, Cole CP. Pulmonary blastomycosis with acute respiratory failure as predominant clinical feature. South Med J. 1997;90(8):847–850. doi: 10.1097/00007611-199708000-00017. [DOI] [PubMed] [Google Scholar]
- 96.Amini M, Shams WE. Barklow, Sarubbi FA. A 45-year-old man with fever and adult respiratory distress syndrome. Clin Infect Dis. 2007;44:566–567. doi: 10.1086/511072. [DOI] [PubMed] [Google Scholar]
- 97.Watts B, Argekar P, Saint S, Kauffman CA. Building a diagnosis from the ground up. New Engl J Med. 2007;356(14):1456–1462. doi: 10.1056/NEJMcps055322. [DOI] [PubMed] [Google Scholar]