

Abstract
Hyperhidrosis is a common dermatological condition that has a tremendous impact on the quality of life of affected patients. Aluminum chloride hexahydrate is considered first-line therapy for patients with mild-to-moderate hyperhidrosis. This treatment has been proven to be effective in the treatment of hyperhidrosis; however, its use has been limited by significant irritation. In many patients, the irritant dermatitis is so severe that, despite clinical efficacy, this therapy must be discontinued. There are many topical aluminum chloride therapies available. Observations from a busy hyperhidrosis practice revealed decreased irritation and increased efficacy with a novel therapy that combines 15% aluminum chloride hexahydrate with 2% salicylic acid in a gel base. This combination of 15% aluminum chloride hexahydrate with 2% salicylic acid offers patients who have failed aluminum chloride hexahydrate in the past excellent efficacy with minimal irritation. We report seven cases of patients with a history of severe irritation from aluminum chloride who maintained excellent results with this new topical without any significant irritation.
Hyperhidrosis, or excessive sweating beyond physiological needs, is a common dermatological condition with a prevalence of one percent.1 Treatment options include topical aluminum chloride hexahydrate (AC), iontophoresis, botulinum toxin A, oral anticholinergics, local resection of sweat glands, and endoscopic sympathectomy.1,2,3 Topical AC is a well-established therapy for hyperhidrosis and is first-line therapy for mild-to-moderate disease. The mechanism of action is via aluminum salt blockage of the distal acrosyringium, which leads to functional and structural degeneration of the eccrine acini.4,5 Although many studies have demonstrated significant efficacy with topical AC, formulations of AC in an alcohol solution have been limited by patient tolerance.6–9 In one study, up to 26 percent of patients found the associated pain and pruritus unacceptable.7 In clinical practice, an even greater percentage of patients discontinue due to poor tolerability.
Case Reports
The authors present a series of seven patients with hyperhidrosis with a history of severe irritation from topical AC solution. All of the patients in this series had failed topical AC solution due to severe irritation. Fifteen percent AC in a 2% salicylic acid gel was offered as an alternative treatment regimen. The patients were instructed to use the topical AC nightly for 4 to 7 nights and then as needed. With the addition of 15% AC in a 2% salicylic acid gel, all seven of the patients achieved control of their hyperhidrosis without significant irritation. The results are summarized in Table 1.
Table 1.
Summary of cases
| CASE | AGE | SKIN TYPE | LOCATION OF HYPERHIDROSIS | FAILED THERAPIES | REASON FOR FAILURE | CONTROLLED WITH 15% AC IN SALICYLIC ACID GEL (HYDROSAL®) | RESIDUAL FINDINGS |
|---|---|---|---|---|---|---|---|
| 1 | 16 | V | Axillae | 20% AC solution (Drysol®) | Irritation Hyperpigmentation | Monotherapy | None |
| 2 | 35 | V | Axillae | 20% AC solution (Hypercare®) | Irritation Hyperpigmentation Tender papules | Monotherapy | None |
| 3 | 37 | III | Hands | 20% AC solution Drysol (®) | Irritation Web space fissures Scale | Combination therapy with botulinum toxin A (Botox®) | Mild xerosis |
| 4 | 48 | V | Axillae | 20% AC solution (Drysol®) | Pruritus | Combination therapy with botulinum toxin A (Botox®) | None |
| 5 | 27 | V | Axillae | 12% AC solution (Certain Dri®) | Irritation Pustules | Combination therapy with botulinum toxin A (Botox®) | None |
| 6 | 29 | V | Axillae | 20% AC solution (Drysol®) | Burning | Combination therapy with botulinum toxin A and gly- copyrrolate (Robinul®) | None |
| 7 | 40 | III | Axillae | 20% AC solution (Drysol®) | Burning | Monotherapy | None |
Case 1. A 16-year-old girl with Fitzpatrick Skin Type V presented to the dermatology clinic with a chief complaint of excessive sweating in the axillae. She was prescribed 20% AC solution (Drysol®, Person and Covey, Inc., Glendale, California) and instructed to use it nightly for seven days and then as needed. The patient called one week later complaining of significant irritation and hyperpigmentation in the axilla due to the medication. She was instructed to discontinue the medication for 1 to 2 weeks and to restart the medication with less frequency. She returned to the clinic one month later with complaints of severe irritation despite intermittent use and persistent hyperpigmentation of the axillae. The 20% AC solution was discontinued. At a follow-up visit one year later, 15% AC in a 2% salicylic acid gel (Hydrosal®, Valeo Pharma Corp., Kirkland, Quebec, Canada) was offered as an alternative treatment option. She was instructed to apply the gel nightly for seven nights and then as needed. At a six-month follow-up visit, the patient reported that her hyperhidrosis was well controlled without irritation or hyperpigmentation.
Case 2. A 35-year-old woman with Fitzpatrick Skin Type VI presented to the clinic with a history of severe hyperhidrosis of the axillae. She presented with a chief complaint of severe irritation of the axillae due to 20% AC solution (Hypercare®, Stratus Pharmaceuticals, Inc., Miami, Florida). On physical examination, she had tender hyperpigmented scaly papules in the axilla (Figure 1). The patient was offered botulinum toxin type A (Botox®, Allergan, Irvine, California) as a treatment for her hyperhidrosis; however, she declined due to a severe needle phobia. The patient was prescribed alclometasone diproprionate for the irritant dermatitis and was instructed to stop all other topicals. At a follow-up visit, the patient was offered 15% AC in a 2% salicylic acid gel. Due to her history of severe dermatitis, the patient was instructed to apply the gel for four consecutive nights and then as needed. At her six-month follow up, the patient reported excellent control of her hyperhidrosis with application every other day. She denied any further irritation on this regimen. Physical exam revealed minimal residual hyperpigmentation (Figure 2).
Figure 1.

As described in Case 2, the patient presented with tender hyperpigmented scaly papules in the axilla
Figure 2.
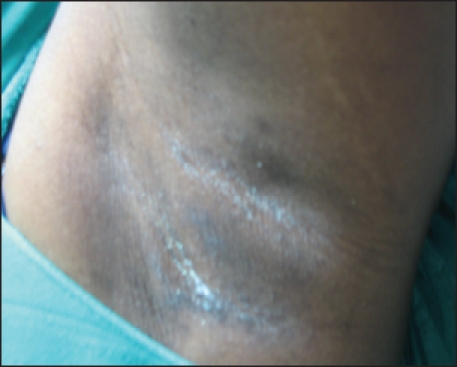
Follow-up physical exam revealed minimal residual hyperpigmentation
Case 3. A 37-year-old man with Fitzpatrick Skin Type III presented to the clinic with a history of severe palmar hyperhidrosis. He required botulinum toxin A every three months for the hands in addition to regular use of 20% AC solution to control his hyperhidrosis. His chief complaint was severe irritation from the regular use of 20% AC solution resulting in chronic hand dermatitis. Due to the severe irritation, he only used the 20% AC solution on the right hand, which was his dominant hand. On physical exam of the right dorsal hand, there were scaly pink lichenified plaques (Figure 3). Small fissures were noted in the web spaces. The patient was treated with botulinum toxin A at that visit. He continued the 20% AC solution; however, he returned one week later with concerns about his chronic severe irritant dermatitis. The patient was switched to 15% AC in a 2% salicylic acid gel. At a two-week follow-up visit, the patient reported continued efficacy, which was confirmed with a starch iodine test. At a three-month follow-up visit, the patient reported complete resolution of his symptoms of burning and stinging. Physical exam revealed only mild residual xerosis.
Case 4. A 48-year-old woman with Fitzpatrick skin type V presented to the clinic with a history of hyperhidrosis in the axillae. The patient was prescribed 20% AC solution, which partially controlled her sweating, but caused significant pruritus. The patient was offered treatment with botulinum toxin A, which also provided some relief, but did not entirely stop her sweating. At this point, 15% AC in a 2% salicylic acid gel was added and she reported complete elimination of sweating with minimal irritation.
Case 5. A 27-year-old woman with Fitzpatrick skin type V presented to the clinic with a history of hyperhidrosis of the axillae and the hands. The patient had failed 12% AC solution (Certain Dri®, DSE Healthcare Solutions, Edison, New Jersey) due to significant irritation associated with pustules in the axillae. She was advised to stop the treatment and was offered botulinum toxin A to treat her hyperhidrosis. Botulinum toxin A significantly improved her hyperhidrosis, but did not completely control it. Fifteen percent AC in a 2% salicylic acid gel was added to her regimen and she reported elimination of sweating with no resulting irritation.
Case 6. A 29-year-old woman with Fitzpatrick skin type V presented to the clinic with a history of severe hyperhidrosis of the axillae. The patient was treated with 20% AC solution. Although the patient experienced a reduction in sweating, the treatment caused her axillae to burn. She was later started on glycopyrrolate (Robinul®, First Horizon Pharmaceutical Corporation, Alpharetta, Georgia) as well as botulinum toxin A and responded well. At a follow-up visit, the patient expressed concern about breakthrough sweating as the effects of the botulinum toxin A diminished. She was given 15% AC in a 2% salicylic acid gel to use in conjunction with the botulinum toxin A and reported elimination of breakthrough sweating with no resulting irritation.
Case 7. A 40-year-old woman with Fitzpatrick skin type III presented to the clinic with a history of severe hyperhidrosis of the axillae and groin. The patient had failed 20% AC solution due to significant irritation. The patient reported control of her inguinal hyperhidrosis with botulinum toxin A and tolerated 15% AC in a 2% salicylic acid gel in the axillae without irritation. The results are summarized in Table 1.
Discussion
Hyperhidrosis, or excessive sweating beyond physiological needs, is a common dermatological condition with a prevalence of one percent.1 Treatment options include topical AC, iontophoresis, botulinum toxin A, oral anticholinergics, local resection of sweat glands, and endoscopic sympathectomy.1,2,3
Topical AC is a well-established therapy for hyperhidrosis. The mechanism of action is via aluminum salt blockage of the distal acrosyringium, which leads to functional and structural degeneration of the eccrine acini.4,5 Although many studies have demonstrated significant efficacy with topical AC, formulations of AC in an alcohol solution have been limited by patient tolerance.6–9 In one study, up to 26 percent of patients found the associated pain and pruritus unacceptable.7 In clinical practice, an even greater percentage of patients discontinue due to poor tolerability.
Many topical AC formulations are available to treat hyperhidrosis (Table 2). Most commercially available formulations are alcohol solutions with concentrations ranging from 6 to 20 percent. Lower concentrations are better tolerated, but less effective. Compounded formulations of up to 50 percent have been utilized to improve efficacy at the expense of patient tolerability.3 The anhydrous alcohol vehicle of the solution appears to significantly contribute to irritation of topical AC.
Table 2.
Available aluminum chloride hexahydrate formulations
| NAME | ACTIVE INGREDIENTS | VEHICLE | OTHER INGREDIENTS |
|---|---|---|---|
| Xerac AC | Aluminum chloride hexahydrate 6.25% | Solution | Anhydrous ethyl alcohol |
| Drysol Mild | Aluminum chloride hexahydrate 6.25% | Solution | Anhydrous ethyl alcohol |
| Certain Dri | Aluminum chloride hexahydrate 12% | Solution | Sodium bicarbonate, water |
| Hydrosal | Aluminum chloride hexahydrate 15% | Gel | EDTA, ethyl alcohol, polyquarternium-10. purified water, salicylic acid |
| Drysol | Aluminum chloride hexahydrate 20% | Solution | Anhydrous ethyl alcohol |
| Hypercare | Aluminum chloride hexahydrate 20% | Solution | Anhydrous ethyl alcohol |
AC in a salicylic acid gel appears to offer improved tolerability without compromising efficacy. There is one study that evaluates efficacy of AC in 4% salicylic acid gel in treating hyperhidrosis of the hands, feet, axilla, and groin. In this large study, 238 patients were treated on 332 anatomic sites. All products were compounded by a pharmacist and concentrations ranged from 10 to 40 percent based on the treated sites. Good to excellent results were achieved in 93 percent of subjects in the axilla (n=139), 60 percent of subjects on the hands (n=46), 84 percent of subjects on the feet (n=139), and 100 percent of subjects in the groin (n=6). Twenty-nine of the 238 subjects had failed AC alcohol solution in the past. This group was evaluated separately and also achieved similar results.10
There are many possible reasons for improved efficacy with the combination formula. These include enhanced absorption of AC due to the keratolytic properties of salicylic acid and a possible synergistic effect with AC due to the astringent and antiperspirant properties of salicylic acid.10–12 Finally, the gel formulation may improve hydration and mitigate the drying effect when compared to an alcohol solution.10 Case 5 originally used a 12% AC solution with significant irritation. Interestingly, in this patient, a higher concentration of AC (15% gel) was well tolerated and effective. This observation suggests that the anhydrous alcohol vehicle may also significantly contribute to the irritation observed in patients using topical AC.
One additional benefit of this formulation is the gel-based vehicle. The patients noted that the gel was easier to apply than a liquid because it stayed on the desired site and did not drip or run. This was especially useful for hand application where web spaces are particularly vulnerable to irritation.
In this case series, clinical improvement in irritation and sweating were subjective. In Case 3, a starch iodine test confirmed sustained reduction in sweating with 15% AC in a 2% salicylic acid gel. However, in all of the cases, more objective measures to assess improvement in irritation and sweating would be useful to confirm these findings.
In conclusion, 15% AC in a 2% salicylic acid gel offers patients a new topical option to treat hyperhidrosis. Additionally, this unique hyperhidrosis therapy demonstrates minimal to no irritation, which is frequently observed with conventional AC solutions. Fifteen percent AC in a 2% salicylic acid gel may be an deal monotherapy for mild hyperhidrosis and adjunctiv i e therapy for those with severe disease. Further studies will be helpful to clarify the role of 15% AC in a 2% salicylic acid gel as a novel addition to our current hyperhidrosis armamentarium.
References
- 1.Stolman LP. Treatment of hyperhidrosis. J Drugs Dermatol. 2003;2:521–527. [PubMed] [Google Scholar]
- 2.Bushara KO. Botulinum toxin—a possible new treatment for axillary hyperhidrosis. Clin Exp Dermatol. 1996;21 doi: 10.1111/j.1365-2230.1996.tb00093.x. [DOI] [PubMed] [Google Scholar]
- 3.Solish N, Bertucci V, Dansereau A, et al. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol Surg. 2007;33(8):908–923. doi: 10.1111/j.1524-4725.2007.33192.x. and the Canadian Hyperhidrosis Advisory Committee. [DOI] [PubMed] [Google Scholar]
- 4.Hölzle E, Braun-Falco O. Structural changes in axillary eccrine glands following long-term treatment with aluminium chloride hexahydrate solution. Br J Dermatol. 1984;110(4):399–403. doi: 10.1111/j.1365-2133.1984.tb04653.x. [DOI] [PubMed] [Google Scholar]
- 5.Hölzle E, Kligman AM. Mechanism of antiperspirant action of aluminum salts. J Soc Cosmetic Chemists. 1979;30 [Google Scholar]
- 6.Scholes KT, Crow KD, Ellis JP, Harman RR, Saihan EM. Axillary hyperhidrosis treated with alcoholic solution of aluminium chloride hexahydrate. BMJ. 1978;2(6130):84–85. doi: 10.1136/bmj.2.6130.84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rayner CR, Ritchie ID, Stark GP. Axillary hyperhidrosis, 20% aluminum chloride hexahydrate, and surgery. BMJ. 1980;280(6224) doi: 10.1136/bmj.280.6224.1168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Glent-Madsen L, Dahl JC. Axillary hyperhidrosis. Local treatment with aluminium-chloride hexahydrate 25% in absolute ethanol with and without supplementary treatment with triethanolamine. Acta Derm Venereol. 1988;68(1):87–89. [PubMed] [Google Scholar]
- 9.Ellis H, Scurr JH. Axillary hyperhidrosis - topical treatment with aluminium chloride hexahydrate. Postgrad Med J. 1979;55(654):868–869. doi: 10.1136/pgmj.55.650.868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Benohanian A, Dansereau A, Bolduc C, et al. Localized hyperhidrosis treated with aluminum chloride in a salicylic acid gel base. Int J Dermatol. 1998;37:701–703. doi: 10.1046/j.1365-4362.1998.00543.x. [DOI] [PubMed] [Google Scholar]
- 11.Peleg H, Noble AC. Perceptual properties of benzoic acid derivatives. Chem Senses. 1995;20(4):393–400. doi: 10.1093/chemse/20.4.393. [DOI] [PubMed] [Google Scholar]
- 12.Benohanian A. Antipersperants and deodorants. Clin Dermatol. 2001;19(4):398–405. doi: 10.1016/s0738-081x(01)00192-4. [DOI] [PubMed] [Google Scholar]