

Abstract
Objective: To evaluate the long-term effects of treatment with diclofenac sodium 3% in 2.5% hyaluronic acid gel on clinically diagnosed actinic keratosis lesions in well-defined skin areas. Design: A one-year extension of a Phase 4, single-arm, multicenter, open-label study was conducted. Patients in the original study received diclofenac sodium 3% gel twice daily for 90 days. The extension study consisted of a single evaluation approximately one year post-treatment. Setting: Five US centers. Participants: Patients who had completed the initial treatment phase with no further treatment for actinic keratosis in the designated treatment blocks. Measurements: The primary endpoint was the proportion of patients achieving 75-percent clearance of actinic keratosis lesions at one-year follow up based on percent change from baseline in target lesion number score or cumulative lesion number score. Secondary endpoints were the proportion of patients achieving 100-percent actinic keratosis lesion clearance and change in investigator’s global improvement index scores. Results: Eighty-one percent of patients reported no additional treatment for actinic keratosis lesions for one year after completing treatment with diclofenac sodium 3% gel. The proportion of patients with 75-percent clearance after one year was 91 percent (95% CI, 84–99%) for target lesions and 70 percent (95% CI, 57–83%) for cumulative lesions. The proportion of patients with 100-percent clearance at one year was 79 percent (95% CI, 67–90%) for target lesions and 30 percent (95% CI, 17–43%) for cumulative lesions. Investigator’s global improvement index severity scores showed that the majority (96%) of patients improved from baseline after one year. Conclusion: The efficacy of a single, 90-day course of diclofenac sodium 3% gel persisted in the majority of patients at one year. (J Clin Aesthetic Dermatol. 2009;2(7):20–25.)
A ctinic keratoses (AKs) are intraepidermal lesions that most commonly develop in fair-skinned individuals after prolonged exposure to ultraviolet (UV) light.1 AK lesions develop on a background of field cancerization in which UV exposure damages widespread areas of the dermis that incur molecular changes, but remain clinically and histologically normal for prolonged periods.2,3 Normal-appearing skin surrounding AKs frequently expresses molecular changes in the form of p53 mutations, and the whole area, therefore, has the potential to develop AKs.3 AK is thus a chronic condition in which new or recurrent lesions continue to develop over time on a background of subclinical disease.
There is widening acceptance of AK as the initial lesion in a disease continuum that can progress to invasive squamous cell carcinoma (SCC).4–6 The two conditions share epidemiological, cytological, and molecular features.1,4,7 Epidemiological data indicate that, in patients with multiple lesions, up to 10 percent of AK may progress to SCC within 10 years,8,9 and it has been estimated that 60 percent of SCCs arise from clinically diagnosed AK.10 Because of the substantial risk of the progression of AK to SCC and the inability of current diagnostic techniques to predict the behavior of individual lesions, current management guidelines recommend considering treatment for all AK lesions.9,11–13
The presence of field cancerization suggests that long-term management of AK will require repeated treatment of continually evolving lesions.2 Currently, the two main approaches to treating AK are in-office treatments, such as cryotherapy targeted at single isolated lesions and patientapplied topical therapies directed at a more widespread field of lesions.13 Data on long-term, follow-up post-treatment for AK are limited; however, there is much discussion about possible recurrence of existing lesions versus emergence of new AK lesions in a similar area. With cryotherapy, reported rates of recurrent or new lesions after initial therapy were 12 percent after 1 to 1.5 years and 30 percent after three years.14 Long-term, follow-up studies with imiquimod 5% cream showed the incidence of new lesions increasing from eight percent at one year to 20 percent after two years in one study15 and a 25-percent incidence of AK lesion appearance in the originally treated area after 16 months in another study.16 Approximate recurrence of lesions in a comparative study was 46 percent for 5-fluorouracil (FU) 12 months post-treatment and 27 percent for imiquimod 12 months post-treatment.17 Given the chronic nature of AK, optimal management typically requires frequent retreatment to manage emerging lesions. Tolerability is an important consideration for any long-term therapeutic option.
Diclofenac sodium 3% in 2.5% hyaluronic acid gel (Solaraze© PharmaDerm, a division of Nycomed US Inc., Florham Park, New Jersey) is a topical nonsteroidal antiinflammatory agent that is approved for the treatment of AK. This treatment option has been shown to be both well tolerated and effective. In Phase 3 studies, treatment with diclofenac sodium 3% gel for 90 days led to 100-percent clearance of existing and emerging AK lesions in 47 percent of patients.18 In subsequent studies, treatment of patients with AKs on various body areas with diclofenac sodium 3% gel for 90 days resulted in ≥75-percent target lesion clearance in 85 to 89 percent of patients at 30 days after completion of treatment.19,20 In all studies, diclofenac sodium 3% gel was well tolerated; most adverse events were mild or moderate application-site reactions.19,20
A Phase 4, open-label study previously showed that twice-daily treatment with diclofenac sodium 3% gel for 90 days resulted in a mean reduction in the number of target lesions of 83 percent at the completion of treatment and 90 percent at the 30-day post-treatment follow up.19 The current report describes the long-term follow up (1 year post-treatment) of patients from this study.
Methods
Study design. The objective of the extension study was to evaluate the long-term effects of treatment with diclofenac sodium 3% gel on clinically diagnosed AK lesions in well-defined skin areas. The study design and results of the original Phase 4 study have been previously reported.19 The original study was a single-arm, open-label, clinical trial conducted at five centers in the United States. Eligible patients (with ≥5 AK lesions in 1 to 3 areas on the face, forehead, or scalp) received treatment with diclofenac sodium 3% gel twice daily for 90 days with a follow up at 120 days (30 days post-treatment). In the extension study, patients returned for a single visit for observation and evaluation approximately one year after the last application of diclofenac sodium 3% gel (Figure 1). No treatment was administered during the extension phase.
Figure 1.

Study design; AK = actinic keratosis
Patients were eligible to participate in the extension study if they had completed the 90-day treatment phase and had not received any further treatment for AK lesions within the designated treatment blocks following the last application of diclofenac sodium 3% gel.
Both phases of the study were conducted in accordance with Good Clinical Practice (GCP) and federal and local regulations. Approval from the institutional review board was obtained before initiation of the study, and informed consent was obtained from each patient before screening for the treatment phase and again before screening for the extension phase.
Study endpoints. The primary efficacy endpoint was the proportion of patients achieving 75-percent clearance of AK lesions as measured by the percent change from baseline to one-year follow up in target lesion number score (TLNS) or cumulative lesion number score (CLNS). The TLNS consisted of the total number of lesions in the designated treatment area at baseline and subsequent visits. The CLNS was the number of original and new AK lesions in the same areas at all visits after the baseline visit. Secondary endpoints included the proportion of patients achieving 100-percent AK lesion clearance calculated from the TLNS or CLNS. The proportion of patients with improvement in global AK condition, as measured by the change in the frequency distribution of scores on the investigator’s global improvement index (IGII) at Visit 6 compared with baseline, was also calculated. As defined in Nelson et al,19 IGII is a score of the investigator’s evaluation of the change in lesion status on a seven-point scale ranging from -2 to 4 points (-2=sigificantly worse; -1=slightly worse; 0=no change; 1=slightly improved; 2=moderately improved; 3=significantly improved; 4=completely improved). No safety or tolerability assessments were made during the extension study.
Statistical analyses. Descriptive statistics were used for TLNS and CLNS and change in these scores. The proportion of patients achieving 75-percent and 100-percent clearance of AK lesions and the corresponding 95-percent confidence intervals (CIs) were calculated by site and for all sites. The frequency distribution of IGII scores was tabulated at baseline and after one year. Shifts in the frequency distribution from the baseline severity index to the one-year post-treatment IGII evaluation were tabulated.
Results
Patient disposition. Sixty-seven of 76 patients (88%) who were enrolled in the treatment phase completed all study visits and were eligible for the one-year screening. Of 64 patients screened, 12 had received treatment for AK lesions after completion of the treatment phase and were excluded. Of the 52 patients eligible for the one-year assessment, 90 percent (n=47) completed the assessment.
Baseline characteristics. The study population at baseline (N=76) was predominantly male (87%), averaged 68 years of age, and had a mean of 8.4 target AK lesions.
Efficacy analyses. Primary endpoint (proportion of patients with 75% clearance). Figure 2a shows the proportion of patients at one year who achieved 75-percent clearance of their lesions from baseline. At one year, 75-percent clearance of target lesions was achieved by 43 of 47 patients (91% [95% CI, 83–99%]). For cumulative lesions, 33 of 47 patients (70% [95% CI, 57–83%]) achieved 75-percent clearance.
Figure 2a.

Proportion of patients achieving 75-percent clearance in the original study and at the one-year post-treatment follow up. Adapted with permission from Journal of Drugs in Dermatology. Copyright 2009. Nelson C, Rigel D, Smith S, Swanson M, Wolf J. Phase IV, open-label assessment of the treatment of actinic keratosis with 3.0% diclofenac sodium topical gel (Solaraze™). J Drugs Dermatol. 2004;3(4):401–407.
Secondary endpoints (proportion of patients with 100-percent clearance). The proportion of patients with 100-percent lesion clearance one year post-treatment is shown in Figure 2b. At one year, 37 of 47 patients (79% [95% CI, 67–90%]) achieved 100-percent clearance of target lesions. Complete clearance of cumulative lesions occurred in 14 of 47 patients (30% [95% CI, 17–43%].
Figure 2b.

Proportion of patients achieving 100-percent clearance in the original study and at the one-year post-treatment follow up. Adapted with permission from Journal of Drugs in Dermatology. Copyright 2009. Nelson C, Rigel D, Smith S, Swanson M, Wolf J. Phase IV, open-label assessment of the treatment of actinic keratosis with 3.0% diclofenac sodium topical gel (Solaraze™). J Drugs Dermatol. 2004;3(4):401–407.
Lesion clearance. The mean TLNS in 76 patients at baseline was 8.4.19 One year after the completion of treatment with diclofenac sodium 3% gel, the mean (standard deviation [SD]) TLNS decreased to 0.3 (0.7) and the mean (SD) CLNS decreased to 1.5 (1.5) in the 47 patients eligible for the assessment (Figure 3).
Figure 3.
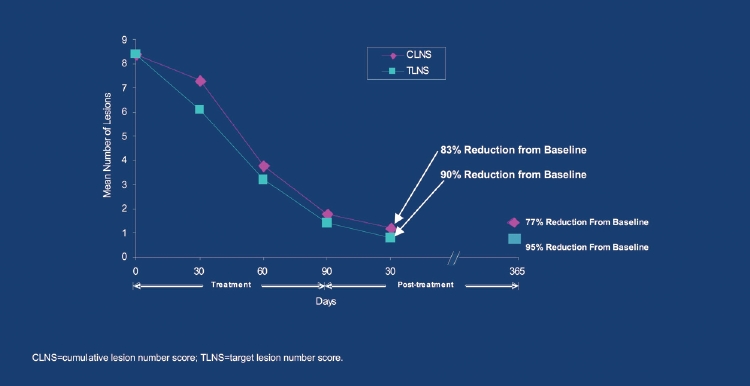
Reduction in actinic keratosis (AK) lesions over time; TLNS = target lesion number score; CLNS = cumulative lesion number score
IGII evaluation. At baseline, most patients (42/47) had an AK severity index of “mild” (n=12) or “moderate” (n=30). At the one-year post-treatment assessment, the majority (96%) of patients were rated as improved based on their baseline disease severity (“completely improved” [n=18], “significantly improved” [n=19], “moderately improved” [n=6], or “slightly improved” [n=2]). Only one patient each was rated as having “no change” or as “slightly worse.”
Discussion
Diclofenac is a nonsteroidal anti-inflammatory drug (NSAID) with preferential activity against the enzyme cyclooxygenase 2 (COX-2). Although the mechanism of action of diclofenac sodium 3% gel in the clearance of AK is unproven, it has been proposed that inhibition of COX-2 may play a role in the persistence of its antitumor effect.21,22 Notably, UV exposure of the skin induces COX-2 expression and prostaglandin production.23 COX-2 not only mediates dermal inflammation, but also promotes tumor growth by enhancing tumor cell proliferation, stimulating angiogenesis, and inhibiting apoptosis.22,24 Significant expression of COX-2 has been observed in AK and SCC, and dermal inflammation is considered a critical component of neoplastic transformation in skin cancer.23,25 The observations that COX-2 inhibitors (including diclofenac sodium 3% gel) have antiangiogenic activity,25 and that, in animal models, COX-2 inhibition can suppress formation of skin tumors26 suggest that the antitumor activity of diclofenac sodium 3% gel in AK may at least in part be ascribed to suppression of COX-2.
This long-term follow-up study of patients with AK treated with a 90-day course of diclofenac sodium 3% gel demonstrated that the efficacy of this agent persisted for at least one year after completion of treatment. Of 64 patients who completed the initial treatment phase, 81 percent (52/64) reported no additional treatment for AK lesions on skin within the designated treatment blocks. One year after receiving no further treatment, 75-percent clearance was noted in 91 percent of patients for target lesions and in 70 percent of patients for cumulative lesions.
When compared with results obtained in the original study at the 30-day post-treatment follow-up,19 the proportion of patients with 75-percent clearance of target lesions was greater after one year than after 30 days (91% vs. 85%; Figure 2a). For cumulative lesions, the proportion of patients with 75-percent clearance was similar after 30 days or one year of follow up (72% vs. 70%).
The rates of complete clearance shortly after treatment and over the longer term provide further insight into the long-term efficacy of diclofenac sodium 3% gel. The proportion of patients with 100-percent clearance of target lesions was considerably higher at one year (79%) than after 30 days post-treatment (58%); whereas, the proportion of patients with 100-percent clearance of cumulative lesions was higher at the 30-day post-treatment follow up (45%) than at the one-year follow up (30%) (Figure 2b). When the 12 patients who had received therapy for AK following completion of the original study were included in the denominator for calculating the proportion of patients achieving 100-percent clearance, the proportions were 63 percent (37/59) for target lesions and 24 percent (14/59) for cumulative lesions. The divergence between complete clearance of target versus cumulative lesions over time among patients included in the current assessment suggests that even in the absence of continued treatment, the effect of diclofenac sodium 3% gel on treated lesions substantially persists over the one-year period. However, new AK lesions can continue to develop after treatment cessation due to previous sun damage to the treatment area. Thus, long-term management of AK may be needed to prevent the emergence of new lesions.
A limitation of the long-term assessment is that not all patients who participated in the initial treatment study were able to be included in the follow-up study. Additional limitations are the challenges of counting AK lesions (e.g., issues such as possible converging of adjacent lesions into one lesion and the appearance of new lesions).
The current study assessed AK clearance in patients who were treatment-free for one year after completing their initial course of diclofenac sodium 3% gel; thus, there was no need for a tolerability assessment. In the original study, the therapy was associated with high compliance and was well tolerated with most application-site reactions being mild or moderate in severity.19 In a directly comparative study, diclofenac sodium 3% gel and 5-FU (5%) were applied to contralateral sides of the face in patients with AK. In this study, 5-FU treatment was associated with markedly greater moderate or severe erythema, scaling, oozing/crusting, and edema.27 Although there is no direct comparison of diclofenac sodium 3% gel with imiquimod, intense local skin reactions with imiquimod have been reported in the majority of patients with AK and include edema, erosion, erythema, flaking/scaling, and scabbing/crusting.28
The current study adds needed information to the literature regarding the long-term follow up of AK treatment. There are few long-term efficacy data available for AK treatments, and methodological differences make direct comparisons between studies difficult. One recent study17 reported results for the 12-month follow up after treatment of AK with either cryosurgery (up to two sessions), 5-FU (twice daily for 4 weeks), or imiquimod (up to two courses). At the 12-month, treatment-free follow up, the proportion of patients with sustained clinical clearance (defined by the investigators as “nonrecurrence” of initially cleared lesions) was 28 percent (7/25) for cryosurgery, 54 percent (13/24) for 5-FU, and 73 percent (19/26) for imiquimod. Another measure of clearance used in this study was sustained clearance of the total treatment field, which was reported in four percent (1/25) of patients for cryosurgery, 33 percent (8/24) for 5-FU, and 73 percent (19/26) for imiquimod. The substantially lower proportion of patients achieving clearance of the total treatment field post-cryosurgery compared with the topical agents may reflect the limitation of a lesion-directed approach and explain the longer-term effectiveness of diclofenac sodium 3% gel in AK therapy.
In conclusion, diclofenac sodium 3% gel in this study produced sustained clearance of the majority of AK lesions for at least one year post-treatment.
Acknowledgments
Editorial support was provided by Meher M. Dustoor, PhD, and Kulvinder K. Singh, PharmD. Both contributors have no financial relationships to disclose. This study was conducted under an educational grant from PharmaDerm, a division of Nycomed US Inc. (formerly Doak Dermatologics).
Contributor Information
Christopher Nelson, University of South Florida, Tampa, Florida.
Darrell Rigel, New York University Medical Center, New York, New York.
References
- 1.Salasche SJ. Epidemiology of actinic keratoses and squamous cell carcinoma. J Am Acad Dermatol. 2000;42:S4–S7. doi: 10.1067/mjd.2000.103342. [DOI] [PubMed] [Google Scholar]
- 2.Vatve M, Ortonne JP, Birch-Machin MA, Gupta G. Management of field change in actinic keratosis. Br J Dermatol. 2007;157(2):21–24. doi: 10.1111/j.1365-2133.2007.08268.x. [DOI] [PubMed] [Google Scholar]
- 3.Quatresooz PC, Pierard-Franchimont C, Pauquet P, et al. Crossroads between actinic keratosis and squamous cell carcinoma, and novel pharmacological issues. Eur J Dermatol. 2008;18(1):6–10. doi: 10.1684/ejd.2008.0303. [DOI] [PubMed] [Google Scholar]
- 4.Oppel T, Korting HC. Actinic keratosis: the key event in the evolution from photoaged skin to squamous cell carcinoma. Therapy based on pathogenetic and clinical aspects. Skin Pharmacol Physiol. 2004;17:67–76. doi: 10.1159/000076016. [DOI] [PubMed] [Google Scholar]
- 5.Patel MJ, Stockfleth E. Does progression from actinic keratosis and Bowen’s disease end with treatment: diclofenac 3% gel, an old drug in a new environment? Br J Dermatol. 2007;156(3):53–56. doi: 10.1111/j.1365-2133.2007.07859.x. [DOI] [PubMed] [Google Scholar]
- 6.Fu W, Cockerell CJ. The actinic (solar) keratosis. A 21st-century perspective. Arch Dermatol. 2003;139:66–70. doi: 10.1001/archderm.139.1.66. [DOI] [PubMed] [Google Scholar]
- 7.Schwartz RA. The actinic keratosis. A perspective and update. Dermatol Surg. 1997;23:1009–1019. doi: 10.1111/j.1524-4725.1997.tb00438.x. quiz 1020–1021. [DOI] [PubMed] [Google Scholar]
- 8.Dodson JM, DeSpain J, Hewett JE, Clark DP. Malignant potential of actinic keratoses and the controversy over treatment. A patient-oriented perspective. Arch Dermatol. 1991;127:1029–1031. [PubMed] [Google Scholar]
- 9.Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000;42:S23–S24. doi: 10.1067/mjd.2000.103339. [DOI] [PubMed] [Google Scholar]
- 10.Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet. 1988;1(8589):795–797. doi: 10.1016/s0140-6736(88)91658-3. [DOI] [PubMed] [Google Scholar]
- 11.Callen JP, Bickers DR, Moy RL. Actinic keratoses. J Am Acad Dermatol. 1997;36(4):650–653. doi: 10.1016/s0190-9622(97)70265-2. [DOI] [PubMed] [Google Scholar]
- 12.Dinehart SM. The treatment of actinic keratoses. J Am Acad Dermatol. 2000;42:S25–S28. doi: 10.1067/mjd.2000.103338. [DOI] [PubMed] [Google Scholar]
- 13.Stockfleth E, Ferrandiz C, Grob JJ, et al. Development of a treatment algorithm for actinic keratoses: a European consensus. Eur J Dermatol. 2008;18(6):651–659. doi: 10.1684/ejd.2008.0514. [DOI] [PubMed] [Google Scholar]
- 14.Chiarello SE. Cryopeeling (extensive cryosurgery) for treatment of actinic keratoses: an update and comparison. Dermatol Surg. 2000;26:728–732. doi: 10.1046/j.1524-4725.2000.99197.x. [DOI] [PubMed] [Google Scholar]
- 15.Stockfleth E, Christophers E, Benninghoff B, Sterry W. Low incidence of new actinic keratoses after topical 5% imiquimod cream treatment: a long-term follow-up study. Arch Dermatol. 2004;140 doi: 10.1001/archderm.140.12.1542-a. [DOI] [PubMed] [Google Scholar]
- 16.Lee PK, Harwell WB, Loven KH, et al. Long-term clinical outcomes following treatment of actinic keratosis with imiquimod 5% cream. Dermatol Surg. 2005;31:659–664. doi: 10.1111/j.1524-4725.2005.31608. [DOI] [PubMed] [Google Scholar]
- 17.Krawtchenko N, Roewert-Huber J, Ulrich M, et al. A randomised study of topical 5% imiquimod vs. topical 5-fluorouracil vs. cryosurgery in immunocompetent patients with actinic keratoses: a comparison of clinical and histological outcomes including 1-year follow-up. Br J Dermatol. 2007;157(2):34–40. doi: 10.1111/j.1365-2133.2007.08271.x. [DOI] [PubMed] [Google Scholar]
- 18.Wolf JE, Jr., Taylor JR, Tschen E, Kang S. Topical 3.0% diclofenac in 2.5% hyaluronan gel in the treatment of actinic keratoses. Int J Dermatol. 2001;40:709–713. doi: 10.1046/j.1365-4362.2001.01324.x. [DOI] [PubMed] [Google Scholar]
- 19.Nelson C, Rigel D, Smith S, Swanson N, Wolf J. Phase IV, open-label assessment of the treatment of actinic keratosis with 3.0% diclofenac sodium topical gel (Solaraze™) J Drugs Dermatol. 2004;3(4):401–407. [PubMed] [Google Scholar]
- 20.Nelson CG, Spencer J, Nelson CG., Jr. A single-arm, open-label efficacy and tolerability study of diclofenac sodium 3% gel for the treatment of actinic keratosis of the upper and lower lip. J Drugs Dermatol. 2007;6(7):712–717. [PubMed] [Google Scholar]
- 21.Eberle J, Fecker LF, Forschner T, Ulrich C, Rowert-Huber J, Stockfleth E. Apoptosis pathways as promising targets for skin cancer therapy. Br J Dermatol. 2007;156(3):18–24. doi: 10.1111/j.1365-2133.2007.07855.x. [DOI] [PubMed] [Google Scholar]
- 22.Fecker LF, Stockfleth E, Nindl I, et al. The role of apoptosis in therapy and prophylaxis of epithelial tumours by nonsteroidal anti-inflammatory drugs (NSAIDs) Br J Dermatol. 2007;156(3):25–33. doi: 10.1111/j.1365-2133.2007.07856.x. [DOI] [PubMed] [Google Scholar]
- 23.Zhan H, Zheng H. The role of topical cyclo-oxygenase-2 inhibitors in skin cancer. Treatment and prevention. Am J Clin Dermatol. 2007;8(4):195–200. doi: 10.2165/00128071-200708040-00002. [DOI] [PubMed] [Google Scholar]
- 24.Masferrer JL, Leahy KM, Koki AT, et al. Antiangiogenic and antitumor activities of cyclooxygenase-2 inhibitors. Cancer Res. 2000;60:1306–1311. [PubMed] [Google Scholar]
- 25.Merk HF. Topical diclofenac in the treatment of actinic keratoses. Int J Dermatol. 2007;46:12–18. doi: 10.1111/j.1365-4632.2007.03060.x. [DOI] [PubMed] [Google Scholar]
- 26.Goldyne ME. Cyclooxygenase isoforms in human skin. Prostaglandins Other Lipid Mediat. 2000;63:15–23. doi: 10.1016/s0090-6980(00)00094-0. [DOI] [PubMed] [Google Scholar]
- 27.Smith SR, Morhenn VB, Piacquadio DJ. Bilateral comparison of the efficacy and tolerability of 3% diclofenac sodium gel and 5% 5-fluorouracil cream in the treatment of actinic keratoses of the face and scalp. J Drugs Dermatol. 2006;5:156–159. [PubMed] [Google Scholar]
- 28.Bristol, Tennessee: Graceway Pharmaceuticals LLC; 2007. Aldara [package insert] [Google Scholar]