

Abstract
Background
The objective of this study is to estimate the number of dementia cases expected to occur in France and Europe over the next few decades, until 2050.
Methodology
Our estimates are based on a model using the European incidence data for dementia by age and sex, the relative mortality risks related to dementia stratified by age classes and the projections of mortality coefficients in the French and European general population.
Results
In France, in 2010, the number of dementia cases should reach 754,000, i.e. 1.2% of the general population or 2.8% of the active population. By 2050 this number should be multiplied by 2.4, i.e. 1,813,000 cases, which will be 2.6% of the total population and 6.2% of the active population. In Europe this number could reach more than 6 millions in 2010 and 14 millions in 2050. The sensitivity analysis performed on French data show that our projections are robust to the use of alternative data for incidence and relative mortality risk (variation of 5.5% and 6.5%), but very sensitive to hypotheses of evolution of mortality (variation of −22 to 29%).
Conclusions
The approach used in our study, integrating both the dementia incidence and the mortality in the calculations, allowed us to refine the projections and stress the great sensitivity of the demographic hypotheses forecasts on the evolution of life expectancy. The likely increase is particularly important and confirms that French and European health systems must take this into account when making future plans.
Keywords: dementia, forecast, projection, burden, Europe
Introduction
Dementia mainly affects the elderly and inevitably leads to a loss of autonomy and independence. Currently there is little that can be done to prevent it (management of cardiovascular risk factors, nutrition, physical activity and emotional and social equilibrium) and the symptomatic treatment available is not particularly effective.
The French demographic structure is marked by the history of the twentieth century and the two World Wars. At present the over 65 age group comprises people born in a period with a low birth rate, related to the drop in births during the WWII (1939–45) period and the arrival of the period of fertility of the children born during the 1914–18 war. This low birth rate cohort will soon be replaced by the baby boom generation (increase in births between 1946 and 1973) who also benefited from increased life expectancy. So people over 65 years, who represent about 16% of the population at the moment, will be one quarter of the French population in a little over 20 years time. The evolution of the aging process of the population, does not seem to be linear and will be less marked at the European level. In 1998 an American study forecast that, in the United States, there would be a tripling of the number of new cases and a quadrupling of the prevalence of dementias by 2050 [1]. However, these numbers are probably an overestimation as there was, in particular, an under estimation of mortality in demented subjects. In 2005, a French report[2] presented, for France, projections for the number of dementia cases and their cost for the years 2020 and 2040. According to these calculations the number of cases of dementia should reach 1,150,000 people in 2020 and 2,020,000 in 2040. These estimates were based on the use of dementia prevalence applied to French demographic projections. For the European projections a recently published study[3] estimated the number of dementia cases in 2006 at 7.21 million and forecasts the increase of this number to 16.51 million in 2050. These estimates were produced with American, not European, mortality data. None of these studies evaluated the sensitivity of the projections to changes in the hypothesis on the data used.
The principal objective of our study is to estimate the projections of the number of cases of dementia until 2050 in France and in the 27 EU countries by using a model that takes into account dementia incidence and mortality. We tested the robustness of these estimates with different hypotheses taking into account estimates of alternative incidence and scenarios for life expectancy or using the hypothesis that a preventive intervention that delays the age of onset of the disease is put in place.
Methods
The statistical method used to achieve our projection was based on Brookmeyer’s [4] method published in 2000. The data required for our calculation were: the number of population by age (t) and sex (s) for the year 2000, the incidence (In) of dementia and Alzheimer’s disease (AD), the projections for the mortality ratio (d) by age (t), sex (s) and years (y) until 2050 and the relative mortality risk for demented patients by age group (λ).
The size of the population by age and sex for the year 2000 was obtained through the INSEE site [5]. Applying the prevalence figures [6, 7] to this population gave us both the number of demented patients by age and sex in 2000 and the size of the population free from dementia in 2000 by age and sex. The equation (1) gives the probability Ps,t,y(D̄) that one person of sex (s) born in the year (y−t) free from dementia and aged (a) in 2000 would be alive at age (t) year (y) without having a dementia:
| (1) |
Where In s,j,y and d s,j,y are the incidence of disease and the mortality coefficient for the sex s, at the age j and the year y respectively. The projections for the population free from dementia by sex, age and year are then obtained by multiplying Ps,t,y(D̄) by the size of the population free from dementia in 2000 and by sex (s) and age (t-(y-2000)).
The number of new cases per year is obtained by multiplying, for each age and sex stratum the incidence by age and sex, by the size of the non-demented population by age and sex for the year studied. The survival of these incident cases and prevalent cases in 2000 was calculated using the equation (2). Ps,t,y(D) is the probability that a demented person living in the year ya of sex s would still be alive in year y and at the age t.
| (2) |
Where λj is the relative risk (RR) of death in demented patients at the age j in comparison with the non-demented population of the same age. The total number of dementia cases for each year is obtained by adding the incident cases to the surviving cases from the previous years. All the estimates are presented with ranges, the calculation of which is based on the confidence interval for the incidence of dementia
Data sources and definition of our principal projection scenario
We first chose certain values, that seemed most reasonable to us, to construct a principal projection scenario. The incidence data used came from the EURODEM analysis [8].
The mortality coefficient of the French population by age, sex and year until 2050 were obtained through the INSEE site. In France, over the period 1988–2002, the evolution of the mortality quotients, for each sex/age combination (by 5 year age group) follows an exponential law [9]. So, the logarithms for the quotients have a rectilinear trend. INSEE’s central demographic scenario draws up the hypothesis that the logarithms of the mortality quotients will continue to follow this same rectilinear trend until 2050, and therefore have been estimated by extrapolation of these trends by age, sex and calendar year until 2050 [9]. For the reported proportions of the total population the hypothesis of the fertility used was a constant of 1.9 children/woman.
The RR of death of demented patients were calculated from crude data published in a Canadian study [10]. These were non adjusted rates, estimated in three age groups (RR=3.75 between 65 and 74 years, RR=2.59 between 75 and 84, RR= 1.59 after 85).
Sensitivity analysis, construction of alternative scenarios
We varied the values of the data used one by one, to construct alternative scenarios.
Scenario S1
Variation of the incidence: the EURODEM incidence data were replaced by data from the PAQUID study which was done in a region of south west France[6].
Scenario S2
Variation of the relative mortality risk: we estimated a constant RR (λ =1.8), from several papers presenting RRs adjusted for different death risk factors [11, 12]. This calculation did not take into account interaction with age.
Scenario S3
Demographic projection with a life expectancy in 2050 longer than that used in the central scenario [9]: scenario with a ‘high’ increase in life expectancy in which the projected mortality quotients were calculated using a hypothetical life expectancy in 2050 of 2.5 years above that used for the central scenario.
Scenario S4
Demographic projection with a life expectancy in 2050 below than that used in the central scenario [9]: scenario with a ‘low’ increase in life expectancy in which the projected mortality quotients were calculated using a hypothetical life expectancy in 2050 of 2.5 years lower that used for the central scenario.
Scenario S5
Simulation of therapeutic or preventive intervention in 2010: simulating the impact of an intervention (starting in 2010) which would delay the onset of the dementia by 1, 2 or 5 years. This impact was evaluated on all types of dementia and specifically on AD.
European analyses
The same methodology was applied to the European projections, the demographic data was obtained from the EUROSTAT site [13–15]. The data on the European population sizes and mortality coefficients after the age of 80 years were only available for all the subjects over 80 grouped together. By default we used the French data, for the distribution by age of subjects over 80 years of age in 2000, and for the mortality coefficients after that age.
Calculation of the economic burden in France
These calculations were done from the available French estimations [16, 17] of the direct cost strictly attributable to AD. After correction with the retail price index, this cost was 22,800 Euros per individual (in 2007 Euros). It included the drugs costs, the accommodation costs, and the remunerated and non-remunerated care costs. The projections for the economic burden were first calculated for the overall burden, then divided by the total population and the active population.
Results
Principal scenario: (Table 1, figure 1&2)
Table 1.
projections of number of dementia (in thousand) until 2050: French and European main scenario
| 2005 | 2010 | 2015 | 2020 | 2030 | 2040 | 2050 | |
|---|---|---|---|---|---|---|---|
| France | |||||||
| Prevalent case of dementia (in thousands) N [rangea] | 714 [616–855] | 754 [614–958] | 966 [757–1254] | 1 026 [805–1354] | 1 287 [1005–1709] | 1 579 [1239–2080] | 1 813 [1428–2373] |
| % of population 65 years oldb | 7,1 % | 7,2 % | 8,1% | 7,6 % | 8,0 % | 8,7 % | 9,6 % |
| % of total populationb | 1,2% | 1,2 % | 1,5% | 1,5 % | 1,9 % | 2,2 % | 2,5% |
| Ratio/active population% | 2,8 | 3,4 | 4,4 | 6,2 | |||
| Annual incidental cases of dementia (in thousands) | 138 | 152 | 165 | 174 | 218 | 272 | 298 |
| Prevalent cases of Alzheimer disease (in thousand) N [rangea] | 447 [347–530] | 504 [360–626] | 657 [452–827] | 699 [472–894] | 864 [579–1117] | 1 066 [717–1362] | 1 226 [827–1552] |
| 27 EU countries | |||||||
| Prevalent case of dementia (in thousands) N [range a] | 5 589 [4813–6693] | 6 027 [4909–7654] | 7 698 [6116–9985] | 8 327 [6555–10921] | 10 261 [8047–13528] | 12 081 [9485–15918] | 14 519 [11453–18981] |
| % of population 65 years oldb | 6,95% | 8,16% | 8,11% | 8,44% | 8,77% | 10,13% | |
| % of total populationb | 1,2 % | 1,2% | 1,6% | 1,7% | 2,1% | 2,6% | 3,3% |
| Ratio/population 15–64 years old | 1,81 | 2,36 | 2,63 | 3,48 | 4,52 | 6,00 | |
| Annual incidental cases of dementia (in thousands) | 1 066 | 1 162 | 1 264 | 1 359 | 1 634 | 1 987 | 2 248 |
range: projections built with the 95% confidence interval of the incidence of the dementia provided in the Eurodem Analysis;
These proportions relate to projections of population of the central demographic scenario of INSEE for France (with a constant fecundity of 1,9), and projection made by Eurostat for the 27 EU countries.
Figure 1.
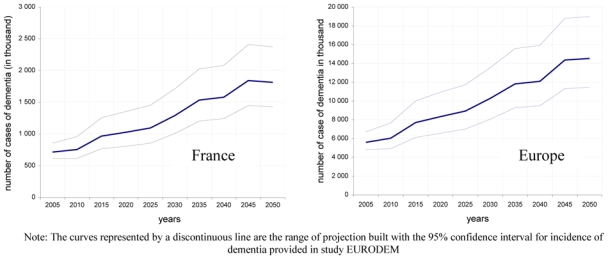
evolution of the number of cases of dementia for the principal scenario in France and Euro Europe pe
Figure 2.
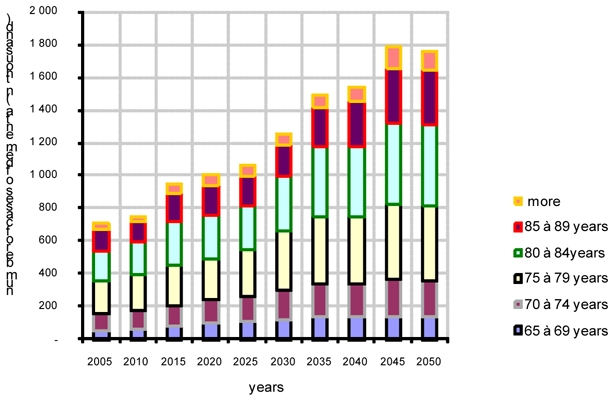
Contribution of each classes of age age, in the projection of the number of dementia cases in France and Europe until 2050 (principal scenario scenario)
In 2010 in France, 754,000 people would be affected by dementia, 72% would be women. This total number of dementia cases would be 1.2% of the total population, 7.9% of the population over 65 years of age, and 2.8% of the active population.
In 2050, 1,813,000 people would be affected by dementia, 68% would be women. This total number of dementia cases would be 2.5% of the total population, 9.6% of the population over 65 years of age, and 6.2% of the active population.
During the period 2010–2050, the number of dementias is multiplied by 2.4, this is an average increase of 2.2% per year over 40 years. This is not a linear change, it would be affected by several periods of acceleration and slowing as various birth cohorts arrive in the age groups with high incidence of dementia. Throughout the period studied the subjects aged between 75 and 85 years represented more than 50% of dementia cases and it is the change in the size of this age group which will mostly affect the change in the number of cases prevalent over time.
Thus a considerable increase in the number of cases between 2010 and 2015 can be seen (increase in the number of cases by 5.3% per year, corresponding to the arrival of cohorts born between 1920 and 1935), a slowing between 2015 and 2025 (increase of 1.0% per year, with the arrival of the age group which were part of the low birth rate during WWII), then a renewed acceleration between 2025 and 2035 (increase of 4.8% per year during this period of baby boom generation aging) to exceed 1,500,000 cases at the end of this period. From 2045, with the arrival of the subjects born after 1970, a period marked by a decline in the birth rate, the number of dementia cases would start to decrease.
In Europe in 2010, more than 6 million people would be affected by dementia, 74.3% would be women. This figure would represent 6.95% of the population aged over 65 years and 1.81% of the population between 15 and 64 years. 1.162 million of new cases would occur every year. In 2050, 14.5 million cases are expected, representing 3.3 % of the total population, 10.1% of the population over 65 years, and 6.2% of the population between 15 and 64 years.
Sensitivity analysis (table 2) (figure 3 supplemental material)
Tableau 2.
Forecast of the number of case of dementia until 2050 (in thousand): result of the different proposed scenario
| 2005 | 2010 | 2015 | 2020 | 2030 | 2040 | 2050 | |
|---|---|---|---|---|---|---|---|
| principal scenario N [range*] | 714 [616–855] | 754 [614–958] | 966 [757–1254] | 1 026 [805–1354] | 1 287 [1005–1709] | 1 579 [1239–2080] | 1 813 [1428–2373] |
| S1= PAQUID incidence ** N | 749 | 793 | 1 020 | 1 083 | 1 366 | 1 668 | 1 920 |
| S2 = relative risk of mortality =1,8 N [range*] | 765 [660–920] | 838 [683–7071] | 1 070 [849–1400] | 1 136 [889–1516] | 1 411 [1098–1895] | 1 717 [1343–2288] | 1 928 [1514–2550] |
| S3 = high increase in life expectancy N [range*] | 714 [616–855] | 769 [626–976] | 1 008 [802–1305] | 1 104 [867–1450] | 1 448 [1132–1909] | 1 876 [1473–2452] | 2 353 [1850–3047] |
| S4 = low increase in life expectancy N [range*] | 714 [616–855] | 745 [606–947] | 932 [740–1212] | 959 [751–1270] | 1 142 [890–1523] | 1 308 [1024–1733] | 1 411 [1109–1860] |
range: projections built with the 95% confidence interval of the incidence of the dementia provided in the Eurodem Analysis;
we did not dispose of the confidence interval of the Incidence value of the study PAQUID, we thus do not have could provide "ranges" for these projections
Figure 3.

Forecast of the num number of case of dementia until 2050 ber : result of the different proposed scenario
The use of alternative hypotheses, involving the disease incidence and relative mortality risk, produced an increase in the number of cases forecast in 2050 of +5.9% (i.e. an additional 107,000 cases) and +6.3% (i.e. an additional 115,000 cases) respectively in comparison with our principal scenario.
The use of alternative hypotheses for the evolution in mortality produced a forecast that the number of cases would be lower by −22.2% (402,000 cases less) for the low demographic scenario, and higher by 29.7% (540,000 additional cases) for the high demographic scenario.
Impact of an intervention (Table 3)
Tableau 3.
Impact of an intervention carried out in 2010 involving an immediate reduction in the incidence of dementia and Alzheimer disease
| Intervention delaying onset of dementia | ||||||
|---|---|---|---|---|---|---|
| 2010 | 2015 | 2020 | 2030 | 2040 | 2050 | |
| Without intervention N | 754 | 966 | 1 026 | 1 287 | 1 579 | 1 813 |
| Onset delaying of 1 year N | 754 | 885 | 914 | 1 131 | 1 397 | 1 615 |
| %* | 8,3 | 10,9 | 12,2 | 11,5 | 10,9 | |
| Onset delaying of 2 year N | 754 | 812 | 813 | 987 | 1 230 | 1 431 |
| %* | 15,9 | 20,8 | 23,3 | 22,1 | 21,1 | |
| Onset delaying of 5 year N | 754 | 635 | 566 | 641 | 812 | 965 |
| %* | 34,2 | 44,8 | 50,2 | 48,6 | 46,8 | |
| Intervention delaying onset of Alzheimer disease | ||||||
| Impact on the number of Alzheimer disease | ||||||
| Without intervention N | 504 | 657 | 699 | 864 | 1 066 | 1 226 |
| Onset delaying of 1 year N | 504 | 600 | 621 | 756 | 940 | 1 089 |
| %* | 8,7 | 11,2 | 12,4 | 11,8 | 11,2 | |
| Onset delaying of 2 years N | 504 | 548 | 550 | 659 | 825 | 961 |
| %* | 16,6 | 21,4 | 23,7 | 22,6 | 21,6 | |
| Onset delaying of 5 years N | 504 | 425 | 379 | 426 | 539 | 641 |
| %* | 35,4 | 45,8 | 50,7 | 49,4 | 47,7 | |
| Impact on the number of Dementia | ||||||
| Without intervention N | 754 | 966 | 1 026 | 1 287 | 1 579 | 1 813 |
| Onset delaying of 1 year N | 754 | 908 | 947 | 1 180 | 1 453 | 1 676 |
| %* | 5,9 | 7,6 | 8,4 | 8,0 | 7,6 | |
| Onset delaying of 2 year N | 754 | 856 | 877 | 1 082 | 1 338 | 1 548 |
| %* | 11,3 | 14,5 | 15,9 | 15,3 | 14,6 | |
| Onset delaying of 5 year N | 754 | 733 | 706 | 849 | 1 052 | 1 228 |
| %* | 24,1 | 31,2 | 34,0 | 33,4 | 32,2 | |
Proportion of reduction in the number of cases compared to projections of the principal scenario without intervention
An intervention, producing a reduction in the incidence of dementias from 2010, would have an impact 5 years after it was started. Delaying the onset of dementias, overall, or specifically AD by 1, 2 or 5 years, would reduce the prevalence of these diseases in the medium and the long term by about 10, 20 and 50% respectively.
Economic burden (Table 4)
Tableau 4.
forecast of the economic burden of the dementia
| Total cost (in billion €) | Cost divided by the total population | Cost divided by the active population | |
|---|---|---|---|
| 2005 | 16 | 267 € | 591 € |
| 2010 | 17 | 277 € | 611 € |
| 2015 | 22 | 347 € | 780 € |
| 2020 | 23 | 361 € | |
| 2030 | 29 | 438 € | 1 043 € |
| 2040 | 36 | 523 € | |
| 2050 | 41 | 592 € | 1 452 € |
Using the hypothesis of a fixed cost over time, the total direct cost strictly attributable to dementia would increase proportional to the number of cases, reaching 41 billion Euros in 2050. This burden could be borne by the active section of the population which is likely to remain stable at around 28 million people between 2010 and 2050[18]. This cost will therefore almost triple during this period, increasing from 611 € in 2010 to 1,452 € per active person in 2050
Discussion
According to our estimates the number of prevalent cases of dementia in 2005 was approximately 710,000 and this would reach 740,000 in 2010. This figure would be multiplied by 2.5 by 2050 to reach a figure of 1,760,000. However, these figures are very dependent on the hypotheses of the evolution of longevity and, in the choice of hypotheses of estimators for the incidence and survival of the dementias.
The key points of our study have been: performing the study with a model using high quality incidence and mortality data from French and European studies, using the relative mortality risk stratified by age, and performing a sensitivity analysis to test the robustness of our projections.
We constructed our principal scenario with data on the incidence of dementia which integrated the results of several European studies, a method which has the advantage of being, in principle, more precise and allowing us to reduce the variance of the estimated population sizes. Nonetheless these data are relatively old (data published in the 90’s with predominantly DSMIII criteria) and it is possible that they may have underestimated the real incidence of the disease. In fact, despite using precise criteria for diagnosing dementia, an important part of the diagnosis is left up to the clinician’s subjective evaluation. This explains why, since 1998 and the introduction of acetylcholinesterase inhibitors, the diagnosis of dementia is made with a higher MMSE score than previously and with less emphasis on the activities of daily living. All the same it is probable that, if an effective treatment is found in the future, the diagnosis will be made even earlier and the number of cases will soar, but not the number of dependent people.
Generally, future parameters, like diagnostic of AD by biomarkers, are likely to lead to earlier diagnosis. Although these parameters will have no impact on disease incidence, they will increase time lived after diagnosis. However, the increase in the resulting prevalence, will not be accompanied by an increase in the number of dependent people, and will probably have little effect on the social burden of the disease. In this context, carrying out of projection of the number of dependent people would have enabled us to produce estimates robust to the shifting diagnosis point. Unfortunately absence of reliable data on the incidence and the survival of this population, prevent us from carrying out this type of projection.
It is also possible that the measurement of the incidence in the large cohorts was underestimated due to the competitive risk of death occurring between the 2 follow up visits [19]. Nevertheless the fact that these subjects had not been diagnosed in the study indicates that the magnitude of their impact on the health system and their care-givers was low. So we chose not to take into account the corrected figures on this effect for our estimates.
Our projections hypothesised that the incidence did not change until 2050. This is a bold hypothesis which requires discussion. We already know that certain dementia protective factors, such as the education level and management of cardiovascular risk factors, is likely to be very different in the coming generations. Besides, a recent American study showed a drop in the prevalence of cognitive impairment between 1993 and 2002[20]. According to this study this drop could partly be due to an increase in the educational level of elderly populations between these two times. Other factors such as life style and the environment for the subsequent generations of elderly people would probably also be very different (diet, activities, exposure to toxic substances, and so on). So it is difficult to anticipate the future evolution of the incidence of dementias.
For the calculations specific to France, projections done for a report drawn up before the 3rd Governmental Plan on Alzheimer’s disease was initiated, estimated the number of cases prevalent in 2004 as 856,000 and as 2,020,000 in 2040 [2]. This report used the prevalence data from the PAQUID study and not the incidence data. It is interesting to note that a similar calculation based on the prevalence data from the EURODEM study [21] also gives a lower estimate with 683,889 cases in 2005. In the end, the sensitivity analysis done with the incidence data from the PAQUID [6] [7] study showed a difference with our results of 100,000 cases in 2050.
The calculations done using the incidence of cases also allowed integration of the case survival parameters. Our choices for these parameters were different to those in Brookmeyer’s paper [1] which introduced a RR adjusted for mortality for demented patients constant with age of 1.4 [22], which is one of the lowest found in the literature [11, 23–25]. However, the use of adjusted rates does not seem adequate to us, in that demented patients are not identical to non-demented patients in their mortality risk factors (for example, the educational level and cardiovascular risk factors affect the risk of developing the disease and also the risk of death). To use an adjusted RR factor leads one to consider demented patients as strictly comparable to the rest of the population and therefore to underestimate the excess mortality in these patients. For example: a study done in 2005 found an adjusted mortality RR of 1.4 and a nonadjusted risk of 2.6 [26]. Also, the use of RR stratified for age is justified by the results of several studies [11, 23, 27], the youngest demented subjects presenting a higher RR than the older individuals. Thus, the sensitivity analysis with the use of a fixed RR of 1.8 modifies, in particular, the estimates which are the highest with this fixed risk. For example, a difference of nearly 50,000 cases is shown from 2020. A recent study from Brookmeyer [3] uses an additive type excess mortality risk. Whatever age the individual was, 6 years after the onset of AD the probability of death was increased by 11%. We did not use this method because of the diversity of the time periods for development of dementias, notably as a function of the age, and the hypothesis of a zero relative mortality risk during the first six years which seems very unlikely due to the very advanced ages. This study anticipated a 2.28 multiplication of the number of cases between 2006 and 2050 in Europe, our work provides for a 2.62 multiplication of cases over the same period.
The main element which would vary our projections is the evolution of mortality (more than 20% difference depending on the population mortality scenario chosen). However it is difficult to decide on the most probable scenario. INSEE asked a panel of experts about this point. They arrived at the conclusion that the central mortality scenario would be rather optimistic for women and rather pessimistic for men (delayed onset), the central hypothesis is currently the most reasonable but the differences depending on the scenarios used are such that the demographic parameters must be updated regularly so that the estimates can be as precise as possible.
References
- 1.Brookmeyer R, Gray S, Kawas C. Projections of Alzheimer’s disease in the United States and the public health impact of delaying disease onset. Am J Public Health. 1998;88:1337–1342. doi: 10.2105/ajph.88.9.1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gallez C. Rapport : La prise en charge de la maladies d’Alzheimer et des maladies apparentées. 2005. pp. 50–58. [Google Scholar]
- 3.Brookmeyer R, Johnson E, Ziegler-Graham K, Michael Arrighi H. Forecasting the global burden of Alzheimer’s disease. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association. 2007;3:186–191. doi: 10.1016/j.jalz.2007.04.381. [DOI] [PubMed] [Google Scholar]
- 4.Brookmeyer R, Gray S. Methods for projecting the incidence and prevalence of chronic diseases in aging populations: application to Alzheimer’s disease. Stat Med. 2000;19:1481–1493. doi: 10.1002/(sici)1097-0258(20000615/30)19:11/12<1481::aid-sim440>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 5.INSEE. http://www.insee.fr/fr/themes/detail.asp?ref_id=irsd2005&page=irweb/sd2005/dd/sd2005_pop.htm.
- 6.Ramaroson H, Helmer C, Barberger-Gateau P, Letenneur L, Dartigues JF. Prevalence of dementia and Alzheimer’s disease among subjects aged 75 years or over: updated results of the PAQUID cohort. Rev Neurol (Paris) 2003;159:405–411. [PubMed] [Google Scholar]
- 7.De Ronchi D, Berardi D, Menchetti M, et al. Occurrence of cognitive impairment and dementia after the age of 60: a population-based study from Northern Italy. Dement Geriatr Cogn Disord. 2005;19:97–105. doi: 10.1159/000082660. [DOI] [PubMed] [Google Scholar]
- 8.Fratiglioni L, Launer LJ, Andersen K, et al. Incidence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S10–15. [PubMed] [Google Scholar]
- 9.INSEE. http://www.insee.fr/fr/themes/detail.asp?ref_id=irprojpop0550&page=irweb/projpop0550/dd/projpop0550_hypotheses_hd.htm.
- 10.Ostbye T, Hill G, Steenhuis R. Mortality in elderly Canadians with and without dementia: a 5-year follow-up. Neurology. 1999;53:521–526. doi: 10.1212/wnl.53.3.521. [DOI] [PubMed] [Google Scholar]
- 11.Helmer C, Joly P, Letenneur L, Commenges D, Dartigues JF. Mortality with dementia: results from a French prospective community-based cohort. Am J Epidemiol. 2001;154:642–648. doi: 10.1093/aje/154.7.642. [DOI] [PubMed] [Google Scholar]
- 12.Jagger C, Andersen K, Breteler MM, et al. Prognosis with dementia in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S16–20. [PubMed] [Google Scholar]
- 13.EUROSTAT. http://epp.eurostat.ec.europa.eu/portal/page?_pageid=0,1136184,0_45572595&_dad=portal& _schema=PORTAL.
- 14.EUROSTAT. http://epp.eurostat.ec.europa.eu/portal/page?_pageid=0,1136184,0_45572595&_dad=portal& _schema=PORTAL.
- 15.EUROSTAT. http://epp.eurostat.ec.europa.eu/portal/page?_pageid=0,1136184,0_45572595&_dad=portal& _schema=PORTAL.
- 16.Gallez C. Rapport : La prise en charge de la maladies d’Alzheimer et des maladies apparentées. 2005. pp. 153–176. [Google Scholar]
- 17.Fagnani F, Everhard F, Buteau L, Detournay B, Sourgen C, Dartigues JF. Coût et retentissement de la maladie d’Alzheimer en France : une extrapolation des données de l’étude Paquid. Revue de Gériatrie. 1999;24:205–211. [Google Scholar]
- 18.INSEE. http://www.insee.fr/fr/themes/document.asp?ref_id=projpopact0650#a2.
- 19.Joly P, Commenges D, Helmer C, Letenneur L. A penalized likelihood approach for an illness-death model with interval-censored data: application to age-specific incidence of dementia. Biostatistics. 2002;3:433–443. doi: 10.1093/biostatistics/3.3.433. [DOI] [PubMed] [Google Scholar]
- 20.Langa KM, Larson EB, Karlawish JH, et al. Trends in the prevalence and mortality of cognitive impairment in the United States: is there evidence of a compression of cognitive morbidity? Alzheimers Dement. 2008;4:134–144. doi: 10.1016/j.jalz.2008.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lobo A, Launer LJ, Fratiglioni L, et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S4–9. [PubMed] [Google Scholar]
- 22.Evans DA, Smith LA, Scherr PA, Albert MS, Funkenstein HH, Hebert LE. Risk of death from Alzheimer’s disease in a community population of older persons. Am J Epidemiol. 1991;134:403–412. doi: 10.1093/oxfordjournals.aje.a116102. [DOI] [PubMed] [Google Scholar]
- 23.Tschanz JT, Corcoran C, Skoog I, et al. Dementia: the leading predictor of death in a defined elderly population: the Cache County Study. Neurology. 2004;62:1156–1162. doi: 10.1212/01.wnl.0000118210.12660.c2. [DOI] [PubMed] [Google Scholar]
- 24.Desmond DW, Moroney JT, Sano M, Stern Y. Mortality in patients with dementia after ischemic stroke. Neurology. 2002;59:537–543. doi: 10.1212/wnl.59.4.537. [DOI] [PubMed] [Google Scholar]
- 25.Baldereschi M, Di Carlo A, Maggi S, et al. Dementia is a major predictor of death among the Italian elderly. ILSA Working Group. Italian Longitudinal Study on Aging. Neurology. 1999;52:709–713. doi: 10.1212/wnl.52.4.709. [DOI] [PubMed] [Google Scholar]
- 26.Ganguli M, Dodge HH, Shen C, Pandav RS, DeKosky ST. Alzheimer disease and mortality: a 15-year epidemiological study. Arch Neurol. 2005;62:779–784. doi: 10.1001/archneur.62.5.779. [DOI] [PubMed] [Google Scholar]
- 27.Wolfson C, Wolfson DB, Asgharian M, et al. A reevaluation of the duration of survival after the onset of dementia. N Engl J Med. 2001;344:1111–1116. doi: 10.1056/NEJM200104123441501. [DOI] [PubMed] [Google Scholar]