

Abstract
Over the past twenty years, a resurgence in vitamin D deficiency and nutritional rickets has been reported throughout the world, including the United States. Inadequate serum vitamin D concentrations have also been associated with complications from other health problems, including tuberculosis, cancer (prostate, breast and colon), multiple sclerosis and diabetes. These findings support the concept of vitamin D possessing important pleiotropic actions outside of calcium homeostasis and bone metabolism. In children, an association between nutritional rickets with respiratory compromise has long been recognized. Recent epidemiological studies clearly demonstrate the link between vitamin D deficiency and the increased incidence of respiratory infections. Further research has also elucidated the contribution of vitamin D in the host defense response to infection. However, the mechanism(s) by which vitamin D levels contribute to pediatric infections and immune function has yet to be determined. This knowledge is particularly relevant and timely, because infants and children appear more susceptible to viral rather than bacterial infections in the face of vitamin D deficiency. The connection between vitamin D, infections and immune function in the pediatric population indicates a possible role for vitamin D supplementation in potential interventions and adjuvant therapies.
After the discovery that vitamin D deficiency is the cause of nutritional rickets, the emphasis on vitamin D status in children was relegated to a discussion primarily focused on prevention and treatment of the disease. A few early clinicians, however, astutely recognized the increased incidence of respiratory infections among infants and children with rickets. Most presumed, however, that the increased incidence of respiratory infections in these children reflected compromised lung compliance from the rib deformities associated with severe rickets as well as an overall poor nutritional status. Now epidemiologic studies have identified a link between inadequate vitamin D concentrations and infectious disease. Furthermore, the contribution of vitamin D in host defense against infection has been elucidated. The goal of this paper is to provide an overview on the current knowledge available regarding the role of vitamin D in immunological function and the manifestations of infectious diseases in the pediatric population.
Delineating Vitamin D Sufficiency, Insufficiency and Deficiency
By definition, vitamin D is not a true vitamin since adequate exposure to sunlight either negates or significantly diminishes the need for dietary supplementation. Instead, this imprecise descriptor refers to a group of steroid molecules also encompassing both vitamin D2 (derived from plants that utilize ergosterol rather than cholesterol) and vitamin D3 molecules (derived from cholesterol). The human body thus procures vitamin D through two independent pathways: the photochemical action of solar UVB light (≈ 295 to 320 nm) in the skin and some limited dietary sources (1).
Given that vitamin D2 is produced by plants, dietary sources (naturally occurring and/or obtained via oral supplementation) are the only means for acquiring it. Vitamin D3, on the other hand, is predominantly procured via the sunlight driven cutaneous reaction described above or from dietary sources. For adults, consumption of fatty fish and/or oral supplementation supplies the most abundant amounts of vitamin D3. In contrast, the major dietary sources of vitamin D in the pediatric population are provided by fortified foods such as cereal, cheese, and milk, none of which are uniformly consumed in large quantities by all age groups. The average adult diet typically provides less than 10-20% of an individual’s vitamin D stores with a child’s diet likely to provide even less vitamin D (2).
In the body, 25D (25-hydroxy vitamin D) is the major circulating vitamin D metabolite. It is generated predominantly through hepatic 25-hydroxylation via many potential catalysts, including CYP2R1 and CYP27A1. The conversion to hormonal 1,25D (1,25-dihydroxyvitamin D) requires the enzyme CYP27B1. The kidneys have long been considered the major site for 1α-hydroxylation of 25D to 1,25D. Unlike the loosely regulated hepatic hydroxylation of 25D, the renal 1α-hydroxylation falls under tight control of PTH (parathyroid hormone) and is primarily involved in calcium regulation and signaling. In sites other than the renal tubule (keratinocytes (3), the trophoblastic layer of the placenta (4), IFN-γ stimulated macrophages (5), and granulomata (6), this type of fastidious regulation is either absent or operates very inefficiently. Compared to adults, strict control of renal 1α-hydroxylation and the normal feedback suppression by 1,25D is also less precise in infants.
Once converted, 1,25D serves as the active form of vitamin D and binds to the VDR (vitamin D receptor), a nuclear receptor and ligand-activated transcription factor (7). VDR is expressed in most tissues and regulates cellular differentiation and function in many cell types. For example, VDR expression is found in monocytes as well as stimulated macrophages, dendritic cells, NK cells, T cells and B cells of the immune system. Activation of the VDR leads to production of downstream gene products. In immune cells, VDR activation elicits potent anti-proliferative, pro-differentiative, and immunomodulatory effects.
Initially, research focused on the role of vitamin D in bone metabolism and calcium homeostasis. Regulation of intestinal calcium transport is still the most significant effect of 1,25D acting through its binding to the VDR. More recently, however, it has become clear that vitamin D has pleiotropic effects, including some VDR transcription-independent actions and plays a key role in immune system regulation. Activation of the VDR by 1,25D, the active form of vitamin D alters cytokine secretion patterns, suppresses effector T cell activation and induces regulatory T cells. In dendritic cells, it has also been demonstrated to affect maturation, differentiation and migration. 1,25D can enhance the phagocytic activity of macrophages and increase the activity of natural killer cells. Therefore, tissue and cell-specific differences in the regulation of 25D are highly relevant to the roles of 25D and 1,25D as immunomodulators.
The effects observed with vitamin D are dependent on the availability of the substrate. Designations for sufficient, toxic, insufficient and deficient states are defined by the serum concentrations of 25D. Normal 25D concentrations associated with a vitamin D sufficient individual are usually greater than 30 to 32 ng/mL (75-80 nM). Hypervitaminosis D is arbitrarily defined as 25D concentrations > 100 ng/mL (250 nmol/L). However, people living and/or working in sun-enriched environments, such as lifeguards and sunbathers, reached 25D concentrations exceeding this value without evidence of deleterious consequences beyond the well characterized solar damage from UVR (ultra violet radiation) (8). Symptoms of vitamin D intoxication typically do not manifest until circulating 25D concentrations rise above 150 ng/mL (375 nM). The most common adverse effect is hypercalcemia, which can lead to the formation of kidney or bladder stones and cause renal failure.
Vitamin D deficiency is typically defined as circulating 25D concentrations less than 20 ng/mL (50 nM) (7, 9). In this state, the subsequently low ionized calcium concentration stimulates PTH secretion, which eventually leads to increased 1,25D synthesis. The elevated PTH concentrations also lead to a decrease in bone mineralization and osteomalacia. In the immature bones of children, the term rickets describes the osteomalacia and the abnormal organization of the cartilaginous growth plate along with the accompanying impairment of cartilage mineralization (10). PTH and 25D concentrations are inversely related until the 25D concentration is greater than 30-40 ng/mL (75-100 nM), after which PTH concentrations fall precipitously.
Individuals with 25D concentrations > 20 ng/mL (50 nM) have been originally classified in the vitamin D sufficient category. With more information emphasizing the important roles vitamin D plays outside of calcium homeostasis and bone metabolism, 25D concentrations that span the range between the loosely defined parameters of vitamin D sufficiency and deficiency are now associated with manifestations of disease. In both the adult and pediatric population, use of the term vitamin D insufficiency is increasingly recommended for ranges that fall between 20 ng/mL (50 nM) and 30 to 32 ng/mL (75-80 nM) to account for these observations.
During the winter solstice period (outside the latitudinal lines, Tropic of Cancer and Tropic of Capricorn), surface solar UVB irradiation is inadequate to trigger sufficient production of vitamin D3. The seasonal variations in temperate climates, related to distance in latitude from the equator and decreased sun exposure, greatly exacerbate the problem of vitamin D insufficiency/deficiency. The melanin content in the epidermis of an individual also affects absorption of UVB with darker pigmented individuals absorbing less UVB due to melanin acting as a natural sunscreen. Any mechanism that prevents UVB absorption (clothing, increased pollution, longer periods spent indoors, etc.) works in a similar fashion to prevent cutaneous production of vitamin D3. Using the definitions from above, estimates suggest that 1 billion people around the world may be vitamin D insufficient/deficient.
In characterizing the global health status of children, recognition of vitamin D insufficiency has increased significantly, particularly over the past 20 years. In the United States, relatively high rates of vitamin D deficiency not necessarily associated with rickets have been reported in healthy infants (11, 12), children (13, 14) and adolescents (15, 16). A high prevalence of vitamin D deficiency has also been reported in infants, children, and adolescents from other countries, including the United Kingdom (17), Greece (18), Lebanon (19), China (20), Finland (21), and Canada (22). Besides the resurgence of rickets, vitamin D insufficiency in children is implicated as a risk factor for the development of chronic diseases later in life, including asthma, diabetes, heart disease and cancer (23). A separate study from the United Kingdom also found that the cost of preventing vitamin D deficiency in a high risk population of Asian children theoretically favored this approach as compared to the financial burden of treating the general health problems associated with chronic vitamin D deficiency (24). Despite the small cohort, the study provides an impetus for considering more aggressive prevention and treatment of widespread vitamin D deficiency.
Vitamin D Insufficiency/Deficiency and Infectious Diseases
Vitamin D insufficiency and deficiency have been associated with various disease states. Below “normal” vitamin D concentrations in adults have been strongly associated with tuberculosis, influenza, autoimmune diseases, cancer (prostate, colon and breast) and myocardial infarction. Expanded studies in infants and children are also exploring the effects of vitamin D insufficiency and type 1 diabetes mellitus (25) as well as investigating the risk of developing of allergies and atopic diseases (26). Still, a significant gap exists in our understanding of the consequences of vitamin D insufficiency/deficiency in the pediatric population.
The prototypical example of a connection between vitamin D insufficiency and susceptibility to infectious disease is TB (tuberculosis). Published studies over the past twenty years ago have strongly connected the association of decreased serum 25D concentrations and increased severity and/or susceptibility to TB infection. Davies et al. demonstrated significantly lower 25D3 concentrations among culture positive TB patients versus their matched controls (27). More recently, a case-control study of the Gujarati Indian population in London found that 25D3 deficiency was more commonly observed in patients with active TB (67%) versus their uninfected household co-inhabitants (26%) who served as the control group (28).
In children, infections remain a major cause of morbidity and mortality around the world (29). Several recent epidemiology studies have observed the association between inadequate vitamin D concentrations and hospitalization and/or respiratory infection among children. Williams et al. determined the vitamin D status of 64 children infected with TB. Eighty-six percent of their patients had inadequate vitamin D stores(30). Although TB is the prototypical association of vitamin D deficiency and infectious disease, other infectious diseases have also been linked to inadequate vitamin D stores in children.
Muhe et al. examined the risk for developing pneumonia among Ethiopian children with nutritional rickets (31). This case-control study found a strong positive correlation between vitamin D deficiency and respiratory compromise. More recently, Najada et al. studied a cohort of hospitalized infants with respiratory diseases and found a higher incidence of nutritional rickets (32). Wayse et al. also investigated ALRIs (acute lower respiratory tract infections) in non-rachitic children admitted to a private hospital in India (33). Their study led to recognition of a link between sub-clinical vitamin D deficiency, nonexclusive breastfeeding and increased risk for severe ALRIs. Karatekin et al. followed up with a report from Turkey on ALRIs and non-rachitic vitamin D deficiency in newborns (34). They found that serum 25D concentrations in the newborns with ALRIs were lower than the healthy control group. The risk for developing an ALRI also increased significantly with 25D concentrations less than 10 ng/mL (25 nM). In their study population, infants with ALRIs spent an average of 8 days in the NICU, again implying the financial and social impact of vitamin D insufficiency/deficiency.
The incidence of viral infections, particularly in the pediatric population, typically peak in the winter months when cutaneous vitamin D synthesis is naturally impaired. In contrast to data available from adult subjects, infections observed in children with inadequate vitamin D stores are more frequently reported as viral in origin. Several of the previously cited studies have pointed to adequate vitamin D concentrations playing a potential role in protecting against upper and lower respiratory tract infections. One of the key points in these studies is the suggestion that susceptibility to infection occurs before many of the overt manifestations of nutritional rickets might appear. More specifically, the risk for acquiring an infection necessitating hospitalization is also reflective of a vitamin D insufficient state, rather than a secondary manifestation of the more severe vitamin D deficiency typically documented in cases of nutritional rickets. For most populations, inadequate concentrations of vitamin D appear to clinically impact the health of children more severely and often prior to the manifestations of rickets and osteomalacia.
CF (cystic fibrosis) is another disease encountered in the pediatric population characterized by recurrent infections and inadequate serum concentrations of vitamin D (35). Patients with CF usually experience problems with malabsorption and are typically placed on oral supplementation of fat-soluble vitamins, including vitamin D. Severe pulmonary infections often require repeated hospitalizations. Treatment for these infections has led to the increasingly problematic issue of antibiotic resistance by the causative pathogens. One promising area of research for improving the efficacy of antibiotic therapy is the use of AMPs (anti-microbial peptides) as therapeutic adjuvants. Cathelicidin is an AMP with multi-functional roles in host defense whose expression is up-regulated by 1,25D. Yim et al. recently investigated the production of cathelicidin in primary cultures of normal and CF bronchial epithelial cells (36). They were able to demonstrate 1,25D-stimulated induction of cathelicidin in this cell type. They also provided evidence for 1,25D treated bronchial epithelial cells exhibiting increased antibacterial activity against common CF airway pathogens such as Pseudomonas aeruginosa and Bordetella bronchiseptica. Based on these results, they speculate on the targeted use of inhaled 1,25D to augment the expression of cathelicidin on the mucosal surface of bronchial epithelia.
HIV is an example of an infection where the clinical and genetic evidence is aggregating together to suggest that vitamin D may play a role in susceptibility to as well as control of the infection. To our knowledge, no studies to date have found a correlation between vitamin D status and risk for death from HIV. In one study, however, HIV-positive patients supplemented with vitamin D demonstrated a positive impact on their CD4+ T-cell counts (37). Further research into the connection between vitamin D and HIV is ongoing and includes studies on the role of vitamin D signaling and the vitamin D receptor (VDR) in HIV infection.
Research into VDR gene polymorphisms also supports the association between vitamin D and other infectious diseases. Janssen et al. reported a significant association between genetic susceptibility to RSV (respiratory syncytial virus) bronchiolitis and several SNPs (single nucleotide polymorphisms) of genes related to innate immune function, including the VDR (38). Roth et al. previously published a report which demonstrated no association between ALRI and vitamin D concentrations in Canadian hospitalized children (39). Most of the children in their study, however, were relatively vitamin D replete. They then undertook a secondary analysis of the subject population used for that study. They identified two SNPs using the TaqI and FokI restriction endonucleases as these had been previously associated with pulmonary TB in several adult populations. The designation of a lowercase t (Taq1) or f (FokI) indicated the presence of a restriction site. Among their study population, children with the ff genotype were at a high risk for developing an ALRI (predominantly RSV bronchiolitis) (40). Their finding remained statistically significant even after attempting to account for potential confounders such as ethnicity.
Vitamin D-related pathways have been studied in terms of their involvement in the host immune response to viral respiratory infections, such as influenza (41). In several pediatric studies, an association with the ff genotype of the VDR increased the risk of acquiring an acute lower respiratory tract infection (predominantly viral bronchiolitis). The ff genotype appears to encode a less active VDR and diminish the ability of immune cells to use vitamin D for its immunomodulatory effects or to generate antimicrobial activity. With estimates of costs exceeding $500 million dollars per year (42), bronchiolitis places a tremendous financial burden on the healthcare system in the United States. A relatively simple intervention such as vitamin D supplementation that might decrease the incidence of this disease would be a highly sought after option for treatment provided by healthcare providers and requested by parents and public health officials.
Effects of Vitamin D on Immune Function
The effects of vitamin D on immune function can be thought of in relation to diseases characterized by autoimmune dysfunction, such as asthma, type 1 diabetes mellitus and multiple sclerosis. Inadequate intake of vitamin D and low serum concentrations of 25D in pregnancy have been associated with higher risk of wheezing illnesses in children (43). A study from Boston, MA suggested that increasing maternal vitamin D intake while pregnant could potentially decrease the risk of recurrent wheeze during early childhood in the offspring of the mothers compliant with the recommendations (44).
In type 1 diabetes, studies of vitamin D supplementation during pregnancy and early childhood demonstrated a potential to reduce the risk of developing the disease (45-47). A population-based birth cohort study of 10,366 Finnish children followed for three decades found that children who regularly ingested 2,000 IU of vitamin D during the first year of life were 80% less likely to develop type 1 diabetes mellitus (47). Some other studies have reported contrasting findings. A Swedish birth cohort study of 11,081 children found that maternal supplementation with > 200 IU of vitamin D during pregnancy reduced islet autoimmunity at 1 year of age, but this effect was not sustained when children were examined at 2 1/2 years of age. Supplementation with a daily dose of 400 IU during infancy was not associated with islet autoimmunity (48). Discrepancies between study designs may partially explain the discrepancy between findings.
Vitamin D deficiency as an infant has been implicated as one risk factor for the development of multiple sclerosis. The season of birth, used as a surrogate marker of vitamin D concentrations during pregnancy, was associated with familial cases of multiple sclerosis in a population based study conducted throughout several different countries (49). Utilizing serum samples stored in the United States Department of Defense Serum Repository, another group of investigators conducted a prospective, nested case-control study and found interesting differences between the ethnically diverse populations represented in the repository. Among white adults, those in the highest quintile of measured vitamin 25D prior to diagnosis had less of a risk for developing multiple sclerosis than those in the lowest quintile (odds ratio 0.59) (50). The inverse relationship between vitamin D and risk of a multiple sclerosis diagnosis was strongest when the 25D concentrations were measured in subjects prior to their reaching 20 years of age. These findings, however, were not duplicated in the samples from African-American and Latino sera contained in the repository.
The effects of vitamin D on the immune system extend beyond manifestations of autoimmune diseases with several studies extensively investigating and summarizing the role of 1,25D on the innate (51-59) and adaptive (59-62) immune responses. In general, 1,25D acts not only to promote the innate immune response to microbial pathogens but to also quell what might be an overzealous adaptive immune response to pathogens that prove difficult for the macrophage to handle effectively. Although 1,25D has direct effects on the adaptive immune system, it also affects the ability of the innate immune system to instruct the adaptive immune response. In this instance 1,25D is a potent suppressor of IL-12 production (63) and dendritic cell (DC) differentiation (64). It is important to note that all of the in vitro studies demonstrating an effect for 1,25D on innate immunity added exogenous 1,25D to cell cultures either at levels above the physiologic serum range or in addition to the 1,25D present in the serum supplemented media. Furthermore, the serum 1,25D levels, as mentioned, are tightly regulated by parathyroid feedback, even in the face of 25D insufficiency. These findings raised questions as to whether there was a role for vitamin D at physiologic concentrations in host immune responses.
The association of 25D insufficiency with various disease states combined with the in vitro studies, prompted researchers to investigate direct effects of 25D on innate immunity. Hewison et al. found that 25D at physiologic levels (100nM) suppressed CD40L-induced IL-12 production in day-7 GM-CSF/IL-4 derived DCs (58). Similarly, there is little data on the effects of altering the 25D status in vivo on the immune status of the host. Yang et al. showed that profound reduction in the serum 25D in mice resulted in significant blunting of the cell-mediated immune response to cutaneous DNFB challenge (65). Administration of 25D to humans with head and neck squamous cell carcinoma increased plasma IL-12 and IFN-γ levels, and improved T-cell blastogenesis (66). One possible resolution of these conflicting data is that the cell-surface makers of a GM-CSF/IL-4 derived DC do not represent a physiologic DC that can be detected in human tissue (67), so this remains an area for new investigation.
In the 1980s, important studies from Rook and Crowle demonstrated the ability of 1,25D to induce anti-microbial activity in Mycobacterium tuberculosis (M. tb.) infected macrophages (68, 69). These studies were carried out before the in situ conversion of 25D to 1,25D in extrarenal tissues was widely recognized and appreciated. As such, the investigators were appropriately cautious to raise concerns regarding their methodology in that they used concentrations of 1,25D far greater than normal serum levels. They questioned whether or not their findings were replicable in the presence of the presumed physiologic serum concentrations of 1,25D available to macrophages. Recent studies in our lab (70) addressed these questions and concerns by providing new insight into the involvement of vitamin D in the toll-like receptor triggering of an anti-microbial response to infection (Figure 1). Using microarray studies, we found that signaling through human macrophage TLR 2/1 heterodimers stimulated with bacterial lipopepties induced expression of both CYP27B1 and the VDR. The exciting aspect of the findings demonstrated that in TRL 2/1-stimulated human macrophages cultured in the presence of human serum, downstream VDR-driven responses were strongly dependent on serum 25D concentrations. VDR-driven responses were either greatly diminished or absent in serum from vitamin D deficient individuals. This response could be “rescued” with 25D supplementation in vitro to a physiologically equivalent serum concentration thereby providing a rationale for considering vitamin D supplementation as prevention and/or as a therapeutic adjuvant.
Figure 1.
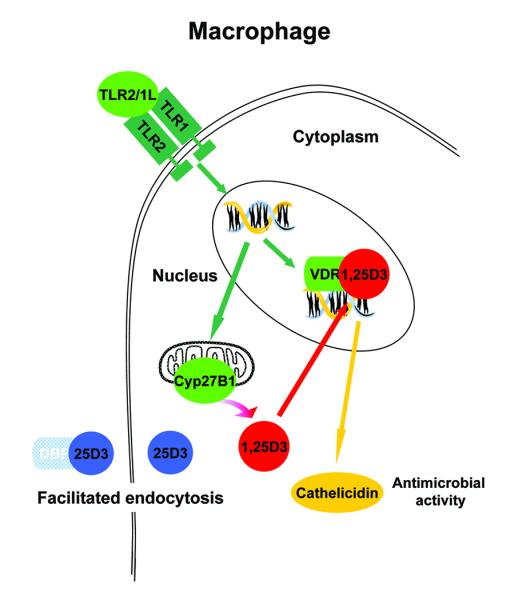
Model of the vitamin D pathway in a macrophage.
Vitamin D Supplementation
As mentioned previously, naturally occurring dietary sources of vitamin D are limited. Foods enriched with vitamin D include fatty fish (e.g. sockeye salmon, raw Atlantic herring, pickled herring, canned pink salmon with bones in oil), fish oils (e.g. cod liver) and sun-dried shitake mushrooms (9, 10). None of these comprise a typical adolescent’s, child’s or infant’s diet. Fortified foods such as infant formulas, cow’s milk, orange juice, breakfast cereals, cheese and butter are more likely to be consumed by children but contain significantly less and often fluctuating amounts of vitamin D. Furthermore, fortification of dairy products in the United States is not mandatory as required in Canada. Fortification of foods is fraught with problems related to lax regulations on compliance with fortification requirements as well as decreasing consumption of vitamin-D fortified foods and beverages.
Sun-avoidant behavior due to concerns for skin cancer leaves many dependent upon inadequate diets for intake of vitamin D. Besides the difficulty in obtaining a sufficient quantity of vitamin D via dietary sources to compensate for the lack of cutaneous D3 synthesis, availability of vitamin D in foods consumed are often further diminished by the methods used in preparation and cooking. Generally speaking, oral supplementation with multivitamins has become a widely accepted means of addressing nutritional deficiencies and inadequacies. With oral supplements, most commercially available multivitamins contain vitamin D2. In terms of potency, plant-derived vitamin D2 is considered less potent than vitamin D3. Poly-Vi-Sol, however, is one pediatric multivitamin that contains vitamin D3. The amount of vitamin D available via oral supplements lacks uniformity or standardized regulation. These discrepancies in food fortification and contradictory recommendations for use of oral supplements directly conflict with the studies supporting the use of vitamin D supplementation in treatment of diseases other than nutritional rickets.
In 1827, the introduction of routine oral cod liver oil administration successfully remedied the manifestations of nutritional rickets. Several decades later, vitamin D3 was identified as the active ingredient in cod liver oil. As early as the 19th century, sanatoria were also popular because of their beneficial effects on patients suffering from a variety of ailments, including cutaneous TB. In 1903, the Nobel Prize in Medicine was awarded to Niels Ryberg Finsen for his use of UV treatment to specifically treat cutaneous TB. However, the past 20 years has seen a resurgence in vitamin D deficiency and rickets. More concerning are the studies linking vitamin D insufficiency/deficiency to a host of other health problems, including asthma, cancer, diabetes, respiratory infections and multiple sclerosis.
Quite a long history exists documenting the use of vitamin D to treat mycobacterial infections with apparent success. In 1946, Dowling et al. reported the treatment of patients with lupus vulgaris (a form of cutaneous TB) with oral vitamin D2 (71). Eighteen of 32 patients appeared to be cured and nine others improved. Morcos et al. treated 24 newly diagnosed cases of TB in children with standard chemotherapy with and without vitamin D (72). They noted clinical and radiological improvement in the group who received treatment plus the vitamin D adjuvant therapy. Nursyam et al. administered vitamin D or placebo to 67 TB patients following the 6th week of standard TB treatment (73). Out of 60 total patients, the group treated with vitamin D had higher sputum conversion and radiological improvement (100%) as compared to the placebo group (76.7%). This difference was statistically significant (p=0.002). In vitro study results published from our lab indicate that the inactive 25D can be converted to the active 1,25D form upon monocyte activation (70). This could be a possible mechanism by which supplementation of patients with inactive vitamin D leads to a positive therapeutic outcome.
In 1997, the Institute of Medicine recommended 200 IU of vitamin D per day for children. The AAP (American Academy of Pediatrics) also adopted this recommendation in their 2003 consensus statement. These recommendations were approved and disseminated despite historical evidence demonstrating one teaspoon of cod liver oil daily for prevention of rickets. (A teaspoon of cod liver oil contains approximately 400 IU of vitamin D.). Administering a daily dose of 200 IU of vitamin D to children also contradicted the FDA recommendations of 400 IU per day for infants, children and adolescents. Recognizing the continued increase in cases of rickets in the United States, the AAP revised their consensus statement in October 2008 (74). The current recommendations outlined several major issues related to vitamin D insufficiency in the United States.
The consensus committee stressed that, despite rickets being a completely preventable disease, exclusively breastfed and/or darkly pigmented infants remain at high risk for vitamin D deficiency and rickets. Additionally, vitamin D insufficiency among pregnant women places newborns at a greater risk for vitamin D deficiency because fetal and newborn concentrations of vitamin D are dependent upon and correlated with maternal serum 25D concentrations (75). In mother-infant pairs, cord blood concentrations of 25D (reflective of the neonate) are typically significantly less than the 25D concentrations measured in the mother. Neonates born to marginally sufficient women, therefore, are still at risk for vitamin D deficiency and those born to vitamin D insufficient women are almost certainly deficient themselves.
To exacerbate the problem for the newborn, the vitamin D content of human milk also correlates with a mother’s serum 25D concentration (74). Due to the multiple factors affecting a person’s vitamin D status, providing supplementation with a daily dose of 400 IU does not guarantee that a mother’s measured 25D serum concentration will rise to a value sufficient for an exclusively breastfeeding infant. Infant formulas in the United States have required minimum (40 IU/100 kcal) and maximum (100 IU/100 kcal) vitamin D concentrations. Based on a typical 20 kcal/oz formula, this is the equivalent of 258 IU/L to 666 IU/L. Fortunately, all U.S. formulas contain at least 400 IU/L of vitamin D3. In the case of exclusively formula fed infants that are expected to consume at least a liter of formula each day, commercially available formula products would provide a minimum of 400 IU/day of vitamin D3. However, the increasing recognition of vitamin D insufficiency among women of childbearing age combined with the increase in exclusive and partial breastfeeding may prevent many infants from receiving an adequate amount of vitamin D from their diets. Studies demonstrating increased cases of rickets, ALRIs and hospitalizations in vitamin D insufficient children appear to bear out these concerns.
Despite vitamin D deficiency rickets being a disease of infants and children, there are also cases of nutritional rickets being reported among adolescents (15). As mentioned previously, the typical adolescent diet lacks an abundant supply of vitamin D fortified foods and drinks. Based on the myriad of concerns, the AAP now recommends 400 IU daily of vitamin D with supplementation to begin in the first few days after birth and continue through childhood and adolescence. The consensus committee also suggests further studies to examine supplementation with higher doses (1,000 – 4,000 IU) similar to some recommendations for adults and, in countries like Canada, pregnant women (76, 77).
The ideal amount of vitamin D intake needed to prevent the adverse health conditions associated with vitamin D insufficiency/deficiency remains unclear. Disagreements on cut-off values for vitamin D sufficiency in the pediatric population likewise complicate interpretation of the recommendations. Furthermore, recommendations for increased sunlight exposure to promote adequate cutaneous vitamin D3 synthesis will need to be balanced with concerns for the risks associated with the increased time spent in the sun exposed to UV radiation. Based on currently available research, however, support for supplementation greater than what prevents the most adverse outcomes (i.e. severe rickets) is strongly advocated.
Summary/Conclusion
Over the past twenty years, clinicians around the world have alerted us to the resurgence of vitamin D associated rickets. Even in the United States, several vulnerable populations have been identified, including premature infants, medically fragile children and exclusively breastfed dark-skinned infants (23). A tremendous amount of historical evidence and epidemiological data support the association between inadequate vitamin D concentrations and infections.
Investigators have demonstrated how appropriate serum concentrations of vitamin D facilitate the ability of immune cells to defend against bacterial and viral infections. Ongoing research in this area has provided new ways of understanding the immune system and how the pleiotropic actions of vitamin D serve an important immunoregulatory role in proper immune function. With the increasing evidence of vitamin D insufficiency’s detrimental effects beyond the classically defined cause of rickets, the full story behind the role of vitamin D insufficiency/deficiency in pediatric infection and immune function awaits full elucidation.
Acknowledgments
Financial Support: NIH/NIAID A147868 (RM), NIH/NIAID A173539 (RM), RWJF 053510 (VW)
ABBREVIATIONS
- 1,25D
1,25-dihydroxyvitamin D
- 25D
25-hydroxy vitamin D
- AAP
American Academy of Pediatrics
- ALRI
acute lower respiratory tract infection
- CF
cystic fibrosis
- DCs
dendritic cells
- PTH
parathyroid hormone
- TB
tuberculosis
- VDR
vitamin D receptor
Footnotes
Publisher's Disclaimer: Pediatric Research Articles Ahead of Print contains articles in unedited manuscript form that have been peer-reviewed and accepted for publication. As a service to our readers, we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting and review of the resulting proof before it is published in its final definitive form. Please note that during the production process errors may be discovered, which could affect the content, and all legal disclaimers that apply to the journal pertain
References
- 1.White JH. Vitamin D signaling, infectious diseases, and regulation of innate immunity. Infect Immun. 2008;76:3837–3843. doi: 10.1128/IAI.00353-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sichert-Hellert W, Wenz G, Kersting M. Vitamin intakes from supplements and fortified food in German children and adolescents: results from the DONALD study. J Nutr. 2006;136:1329–1333. doi: 10.1093/jn/136.5.1329. [DOI] [PubMed] [Google Scholar]
- 3.Lehmann B, Knuschke P, Meurer M. A novel pathway for hormonally active calcitriol. Horm Res. 2000;54:312–315. doi: 10.1159/000053278. [DOI] [PubMed] [Google Scholar]
- 4.Diaz L, Sanchez I, Avila E, Halhali A, Vilchis F, Larrea F. Identification of a 25-hydroxyvitamin D3 1alpha-hydroxylase gene transcription product in cultures of human syncytiotrophoblast cells. J Clin Endocrinol Metab. 2000;85:2543–2549. doi: 10.1210/jcem.85.7.6693. [DOI] [PubMed] [Google Scholar]
- 5.Mawer EB, Hayes ME, Still PE, Davies M, Lumb GA, Palit J, Holt PJ. Evidence for nonrenal synthesis of 1,25-dihydroxyvitamin D in patients with inflammatory arthritis. J Bone Miner Res. 1991;6:733–739. doi: 10.1002/jbmr.5650060711. [DOI] [PubMed] [Google Scholar]
- 6.Zehnder D, Bland R, Williams MC, McNinch RW, Howie AJ, Stewart PM, Hewison M. Extrarenal expression of 25-hydroxyvitamin d(3)-1 alpha-hydroxylase. J Clin Endocrinol Metab. 2001;86:888–894. doi: 10.1210/jcem.86.2.7220. [DOI] [PubMed] [Google Scholar]
- 7.Lin R, White JH. The pleiotropic actions of vitamin D. Bioessays. 2004;26:21–28. doi: 10.1002/bies.10368. [DOI] [PubMed] [Google Scholar]
- 8.Vieth R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am J Clin Nutr. 1999;69:842–856. doi: 10.1093/ajcn/69.5.842. [DOI] [PubMed] [Google Scholar]
- 9.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 10.Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398–417. doi: 10.1542/peds.2007-1894. [DOI] [PubMed] [Google Scholar]
- 11.Lee JM, Smith JR, Philipp BL, Chen TC, Mathieu J, Holick MF. Vitamin D deficiency in a healthy group of mothers and newborn infants. Clin Pediatr (Phila) 2007;46:42–44. doi: 10.1177/0009922806289311. [DOI] [PubMed] [Google Scholar]
- 12.Ziegler EE, Hollis BW, Nelson SE, Jeter JM. Vitamin D deficiency in breastfed infants in Iowa. Pediatrics. 2006;118:603–610. doi: 10.1542/peds.2006-0108. [DOI] [PubMed] [Google Scholar]
- 13.Rajakumar K, Fernstrom JD, Janosky JE, Greenspan SL. Vitamin D insufficiency in preadolescent African-American children. Clin Pediatr (Phila) 2005;44:683–692. doi: 10.1177/000992280504400806. [DOI] [PubMed] [Google Scholar]
- 14.Sullivan SS, Rosen CJ, Halteman WA, Chen TC, Holick MF. Adolescent girls in Maine are at risk for vitamin D insufficiency. J Am Diet Assoc. 2005;105:971–974. doi: 10.1016/j.jada.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 15.Gordon CM, DePeter KC, Feldman HA, Grace E, Emans SJ. Prevalence of vitamin D deficiency among healthy adolescents. Arch Pediatr Adolesc Med. 2004;158:531–537. doi: 10.1001/archpedi.158.6.531. [DOI] [PubMed] [Google Scholar]
- 16.Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahyoun NR. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone. 2002;30:771–777. doi: 10.1016/s8756-3282(02)00692-0. [DOI] [PubMed] [Google Scholar]
- 17.Lawson M, Thomas M. Vitamin D concentrations in Asian children aged 2 years living in England: population survey. BMJ. 1999;318:28. doi: 10.1136/bmj.318.7175.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nicolaidou P, Hatzistamatiou Z, Papadopoulou A, Kaleyias J, Floropoulou E, Lagona E, Tsagris V, Costalos C, Antsaklis A. Low vitamin D status in mother-newborn pairs in Greece. Calcif Tissue Int. 2006;78:337–342. doi: 10.1007/s00223-006-0007-5. [DOI] [PubMed] [Google Scholar]
- 19.Fuleihan G El-Hajj, Nabulsi M, Choucair M, Salamoun M, Shahine C Hajj, Kizirian A, Tannous R. Hypovitaminosis D in healthy schoolchildren. Pediatrics. 2001;107:E53. doi: 10.1542/peds.107.4.e53. [DOI] [PubMed] [Google Scholar]
- 20.Du X, Greenfield H, Fraser DR, Ge K, Trube A, Wang Y. Vitamin D deficiency and associated factors in adolescent girls in Beijing. Am J Clin Nutr. 2001;74:494–500. doi: 10.1093/ajcn/74.4.494. [DOI] [PubMed] [Google Scholar]
- 21.Lehtonen-Veromaa M, Mottonen T, Irjala K, Karkkainen M, Lamberg-Allardt C, Hakola P, Viikari J. Vitamin D intake is low and hypovitaminosis D common in healthy 9- to 15-year-old Finnish girls. Eur J Clin Nutr. 1999;53:746–751. doi: 10.1038/sj.ejcn.1600844. [DOI] [PubMed] [Google Scholar]
- 22.Ward LM, Gaboury I, Ladhani M, Zlotkin S. Vitamin D-deficiency rickets among children in Canada. CMAJ. 2007;177:161–166. doi: 10.1503/cmaj.061377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Huh SY, Gordon CM. Vitamin D deficiency in children and adolescents: epidemiology, impact and treatment. Rev Endocr Metab Disord. 2008;9:161–170. doi: 10.1007/s11154-007-9072-y. [DOI] [PubMed] [Google Scholar]
- 24.Zipitis CS, Markides GA, Swann IL. Vitamin D deficiency: prevention or treatment? Arch Dis Child. 2006;91:1011–1014. doi: 10.1136/adc.2006.098467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bener A, Alsaied A, Al-Ali M, Al-Kubaisi A, Basha B, Abraham A, Guiter G, Mian M. High prevalence of vitamin D deficiency in type 1 diabetes mellitus and healthy children. Acta Diabetol. 2008 doi: 10.1007/s00592-008-0071-6. (in press) [DOI] [PubMed] [Google Scholar]
- 26.Zittermann A, Dembinski J, Stehle P. Low vitamin D status is associated with low cord blood levels of the immunosuppressive cytokine interleukin-10. Pediatr Allergy Immunol. 2004;15:242–246. doi: 10.1111/j.1399-3038.2004.00140.x. [DOI] [PubMed] [Google Scholar]
- 27.Davies PD, Brown RC, Woodhead JS. Serum concentrations of vitamin D metabolites in untreated tuberculosis. Thorax. 1985;40:187–190. doi: 10.1136/thx.40.3.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wilkinson RJ, Llewelyn M, Toossi Z, Patel P, Pasvol G, Lalvani A, Wright D, Latif M, Davidson RN. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: a case-control study. Lancet. 2000;355:618–621. doi: 10.1016/S0140-6736(99)02301-6. [DOI] [PubMed] [Google Scholar]
- 29.Bryce J, Boschi-Pinto C, Shibuya K, Black RE. WHO estimates of the causes of death in children. Lancet. 2005;365:1147–1152. doi: 10.1016/S0140-6736(05)71877-8. [DOI] [PubMed] [Google Scholar]
- 30.Williams B, Williams AJ, Anderson ST. Vitamin D deficiency and insufficiency in children with tuberculosis. Pediatr Infect Dis J. 2008;27:941–942. doi: 10.1097/INF.0b013e31817525df. [DOI] [PubMed] [Google Scholar]
- 31.Muhe L, Lulseged S, Mason KE, Simoes EA. Case-control study of the role of nutritional rickets in the risk of developing pneumonia in Ethiopian children. Lancet. 1997;349:1801–1804. doi: 10.1016/S0140-6736(96)12098-5. [DOI] [PubMed] [Google Scholar]
- 32.Najada AS, Habashneh MS, Khader M. The frequency of nutritional rickets among hospitalized infants and its relation to respiratory diseases. J Trop Pediatr. 2004;50:364–368. doi: 10.1093/tropej/50.6.364. [DOI] [PubMed] [Google Scholar]
- 33.Wayse V, Yousafzai A, Mogale K, Filteau S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 y. Eur J Clin Nutr. 2004;58:563–567. doi: 10.1038/sj.ejcn.1601845. [DOI] [PubMed] [Google Scholar]
- 34.Karatekin G, Kaya A, Salihoglu O, Balci H, Nuhoglu A. Association of subclinical vitamin D deficiency in newborns with acute lower respiratory infection and their mothers. Eur J Clin Nutr. 2007 doi: 10.1038/sj.ejcn.1602960. (in press) [DOI] [PubMed] [Google Scholar]
- 35.Green D, Carson K, Leonard A, Davis JE, Rosenstein B, Zeitlin P, Mogayzel P., Jr Current treatment recommendations for correcting vitamin D deficiency in pediatric patients with cystic fibrosis are inadequate. J Pediatr. 2008;153:554–559. doi: 10.1016/j.jpeds.2008.04.058. [DOI] [PubMed] [Google Scholar]
- 36.Yim S, Dhawan P, Ragunath C, Christakos S, Diamond G. Induction of cathelicidin in normal and CF bronchial epithelial cells by 1,25-dihydroxyvitamin D(3) J Cyst Fibros. 2007;6:403–410. doi: 10.1016/j.jcf.2007.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Villamor E. A potential role for vitamin D on HIV infection? Nutr Rev. 2006;64:226–233. doi: 10.1301/nr.2006.may.226-233. [DOI] [PubMed] [Google Scholar]
- 38.Janssen R, Bont L, Siezen CL, Hodemaekers HM, Ermers MJ, Doornbos G, van ’t Slot R, Wijmenga C, Goeman JJ, Kimpen JL, van Houwelingen HC, Kimman TG, Hoebee B. Genetic susceptibility to respiratory syncytial virus bronchiolitis is predominantly associated with innate immune genes. J Infect Dis. 2007;196:826–834. doi: 10.1086/520886. [DOI] [PubMed] [Google Scholar]
- 39.Roth DE, Jones AB, Prosser C, Robinson JL, Vohra S. Vitamin D status is not associated with the risk of hospitalization for acute bronchiolitis in early childhood. Eur J Clin Nutr. 2007 doi: 10.1038/sj.ejcn.1602946. (in press) [DOI] [PubMed] [Google Scholar]
- 40.Roth DE, Jones AB, Prosser C, Robinson JL, Vohra S. Vitamin D receptor polymorphisms and the risk of acute lower respiratory tract infection in early childhood. J Infect Dis. 2008;197:676–680. doi: 10.1086/527488. [DOI] [PubMed] [Google Scholar]
- 41.Cannell JJ, Vieth R, Umhau JC, Holick MF, Grant WB, Madronich S, Garland CF, Giovannucci E. Epidemic influenza and vitamin D. Epidemiol Infect. 2006;134:1129–1140. doi: 10.1017/S0950268806007175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pelletier AJ, Mansbach JM, Camargo CA., Jr Direct medical costs of bronchiolitis hospitalizations in the United States. Pediatrics. 2006;118:2418–2423. doi: 10.1542/peds.2006-1193. [DOI] [PubMed] [Google Scholar]
- 43.Devereux G, Litonjua AA, Turner SW, Craig LC, McNeill G, Martindale S, Helms PJ, Seaton A, Weiss ST. Maternal vitamin D intake during pregnancy and early childhood wheezing. Am J Clin Nutr. 2007;85:853–859. doi: 10.1093/ajcn/85.3.853. [DOI] [PubMed] [Google Scholar]
- 44.Camargo CA, Jr, Rifas-Shiman SL, Litonjua AA, Rich-Edwards JW, Weiss ST, Gold DR, Kleinman K, Gillman MW. Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of age. Am J Clin Nutr. 2007;85:788–795. doi: 10.1093/ajcn/85.3.788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Arkkola T, Uusitalo U, Kronberg-Kippila C, Mannisto S, Virtanen M, Kenward MG, Veijola R, Knip M, Ovaskainen ML, Virtanen SM. Seven distinct dietary patterns identified among pregnant Finnish women--associations with nutrient intake and sociodemographic factors. Public Health Nutr. 2008;11:176–182. doi: 10.1017/S1368980007000420. [DOI] [PubMed] [Google Scholar]
- 46.Fronczak CM, Baron AE, Chase HP, Ross C, Brady HL, Hoffman M, Eisenbarth GS, Rewers M, Norris JM. In utero dietary exposures and risk of islet autoimmunity in children. Diabetes Care. 2003;26:3237–3242. doi: 10.2337/diacare.26.12.3237. [DOI] [PubMed] [Google Scholar]
- 47.Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM. Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet. 2001;358:1500–1503. doi: 10.1016/S0140-6736(01)06580-1. [DOI] [PubMed] [Google Scholar]
- 48.Brekke HK, Ludvigsson J. Vitamin D supplementation and diabetes-related autoimmunity in the ABIS study. Pediatr Diabetes. 2007;8:11–14. doi: 10.1111/j.1399-5448.2006.00223.x. [DOI] [PubMed] [Google Scholar]
- 49.Willer CJ, Dyment DA, Sadovnick AD, Rothwell PM, Murray TJ, Ebers GC, Canadian Collaborative Study Group Timing of birth and risk of multiple sclerosis: population based study. BMJ. 2005;330:120. doi: 10.1136/bmj.38301.686030.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A. Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA. 2006;296:2832–2838. doi: 10.1001/jama.296.23.2832. [DOI] [PubMed] [Google Scholar]
- 51.Adams JS, Gacad MA, Singer FR, Sharma OP. Production of 1,25-dihydroxyvitamin D3 by pulmonary alveolar macrophages from patients with sarcoidosis. Ann N Y Acad Sci. 1986;465:587–594. doi: 10.1111/j.1749-6632.1986.tb18535.x. [DOI] [PubMed] [Google Scholar]
- 52.Adams JS, Singer FR, Gacad MA, Sharma OP, Hayes MJ, Vouros P, Holick MF. Isolation and structural identification of 1,25-dihydroxyvitamin D3 produced by cultured alveolar macrophages in sarcoidosis. J Clin Endocrinol Metab. 1985;60:960–966. doi: 10.1210/jcem-60-5-960. [DOI] [PubMed] [Google Scholar]
- 53.Adams JS, Gacad MA. Characterization of 1 alpha-hydroxylation of vitamin D3 sterols by cultured alveolar macrophages from patients with sarcoidosis. J Exp Med. 1985;161:755–765. doi: 10.1084/jem.161.4.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Barnes PF, Modlin RL, Bikle DD, Adams JS. Transpleural gradient of 1,25-dihydroxyvitamin D in tuberculous pleuritis. J Clin Invest. 1989;83:1527–1532. doi: 10.1172/JCI114048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Fagan DL, Prehn JL, Adams JS, Jordan SC. The human myelomonocytic cell line U-937 as a model for studying alterations in steroid-induced monokine gene expression: marked enhancement of lipopolysaccharide-stimulated interleukin-1 beta messenger RNA levels by 1,25-dihydroxyvitamin D3. Mol Endocrinol. 1991;5:179–186. doi: 10.1210/mend-5-2-179. [DOI] [PubMed] [Google Scholar]
- 56.Hewison M, Dabrowski M, Faulkner L, Hughson E, Vadher S, Rut A, Brickell PM, O’Riordan JL, Katz DR. Transfection of vitamin D receptor cDNA into the monoblastoid cell line U937. The role of vitamin D3 in homotypic macrophage adhesion. J Immunol. 1994;153:5709–5719. [PubMed] [Google Scholar]
- 57.Hewison M, Dabrowski M, Vadher S, Faulkner L, Cockerill FJ, Brickell PM, O’Riordan JL, Katz DR. Antisense inhibition of vitamin D receptor expression induces apoptosis in monoblastoid U937 cells. J Immunol. 1996;156:4391–4400. [PubMed] [Google Scholar]
- 58.Hewison M, Freeman L, Hughes SV, Evans KN, Bland R, Eliopoulos AG, Kilby MD, Moss PA, Chakraverty R. Differential regulation of vitamin D receptor and its ligand in human monocyte-derived dendritic cells. J Immunol. 2003;170:5382–5390. doi: 10.4049/jimmunol.170.11.5382. [DOI] [PubMed] [Google Scholar]
- 59.Jordan SC, Lemire JM, Sakai RS, Toyoda M, Adams JS. Exogenous interleukin-2 does not reverse the immunoinhibitory effects of 1,25-dihydroxyvitamin D3 on human peripheral blood lymphocyte immunoglobulin production. Mol Immunol. 1990;27:95–100. doi: 10.1016/0161-5890(90)90064-7. [DOI] [PubMed] [Google Scholar]
- 60.Lemire JM, Adams JS, Kermani-Arab V, Bakke AC, Sakai R, Jordan SC. 1,25-Dihydroxyvitamin D3 suppresses human T helper/inducer lymphocyte activity in vitro. J Immunol. 1985;134:3032–3035. [PubMed] [Google Scholar]
- 61.Lemire JM, Adams JS, Sakai R, Jordan SC. 1 alpha,25-dihydroxyvitamin D3 suppresses proliferation and immunoglobulin production by normal human peripheral blood mononuclear cells. J Clin Invest. 1984;74:657–661. doi: 10.1172/JCI111465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Prehn JL, Fagan DL, Jordan SC, Adams JS. Potentiation of lipopolysaccharide-induced tumor necrosis factor-alpha expression by 1,25-dihydroxyvitamin D3. Blood. 1992;80:2811–2816. [PubMed] [Google Scholar]
- 63.D’Ambrosio D, Cippitelli M, Cocciolo MG, Mazzeo D, Di LP, Lang R, Sinigaglia F, Panina-Bordignon P. Inhibition of IL-12 production by 1,25-dihydroxyvitamin D3. Involvement of NF-kappaB downregulation in transcriptional repression of the p40 gene. J Clin Invest. 1998;101:252–262. doi: 10.1172/JCI1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Piemonti L, Monti P, Sironi M, Fraticelli P, Leone BE, Dal Cin E, Allavena P, Di Carlo V. Vitamin D3 affects differentiation, maturation, and function of human monocyte-derived dendritic cells. J Immunol. 2000;164:4443–4451. doi: 10.4049/jimmunol.164.9.4443. [DOI] [PubMed] [Google Scholar]
- 65.Yang S, Smith C, Prahl JM, Luo X, DeLuca HF. Vitamin D deficiency suppresses cell-mediated immunity in vivo. Arch Biochem Biophys. 1993;303:98–106. doi: 10.1006/abbi.1993.1260. [DOI] [PubMed] [Google Scholar]
- 66.Lathers DM, Clark JI, Achille NJ, Young MR. Phase 1B study to improve immune responses in head and neck cancer patients using escalating doses of 25-hydroxyvitamin D3. Cancer Immunol Immunother. 2004;53:422–430. doi: 10.1007/s00262-003-0459-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Krutzik SR, Tan B, Li H, Ochoa MT, Liu PT, Sharfstein SE, Graeber TG, Sieling PA, Liu YJ, Rea TH, Bloom BR, Modlin RL. TLR activation triggers the rapid differentiation of monocytes into macrophages and dendritic cells. Nat Med. 2005;11:653–660. doi: 10.1038/nm1246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Rook GA, Steele J, Fraher L, Barker S, Karmali R, O’Riordan J, Stanford J. Vitamin D3, gamma interferon, and control of proliferation of Mycobacterium tuberculosis by human monocytes. Immunology. 1986;57:159–163. [PMC free article] [PubMed] [Google Scholar]
- 69.Crowle AJ, Ross EJ, May MH. Inhibition by 1,25(OH)2-vitamin D3 of the multiplication of virulent tubercle bacilli in cultured human macrophages. Infect Immun. 1987;55:2945–2950. doi: 10.1128/iai.55.12.2945-2950.1987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, Ochoa MT, Schauber J, Wu K, Meinken C, Kamen DL, Wagner M, Bals R, Steinmeyer A, Zugel U, Gallo RL, Eisenberg D, Hewison M, Hollis BW, Adams JS, Bloom BR, Modlin RL. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science. 2006;311:1770–1773. doi: 10.1126/science.1123933. [DOI] [PubMed] [Google Scholar]
- 71.Dowling GB. The present status of vitamin D2 in the treatment of lupus vulgaris. Dermatologica. 1957;115:491–495. doi: 10.1159/000256074. [DOI] [PubMed] [Google Scholar]
- 72.Morcos MM, Gabr AA, Samuel S, Kamel M, el Baz M, el Beshry M, Michail RR. Vitamin D administration to tuberculous children and its value. Boll Chim Farm. 1998;137:157–164. [PubMed] [Google Scholar]
- 73.Nursyam EW, Amin Z, Rumende CM. The effect of vitamin D as supplementary treatment in patients with moderately advanced pulmonary tuberculous lesion. Acta Med Indones. 2006;38:3–5. [PubMed] [Google Scholar]
- 74.Wagner CL, Greer FR. Prevention of rickets and vitamin d deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142–1152. doi: 10.1542/peds.2008-1862. [DOI] [PubMed] [Google Scholar]
- 75.Hollis BW, Pittard WB., 3rd Evaluation of the total fetomaternal vitamin D relationships at term: evidence for racial differences. J Clin Endocrinol Metab. 1984;59:652–657. doi: 10.1210/jcem-59-4-652. [DOI] [PubMed] [Google Scholar]
- 76.Canadian Paediatric Society Vitamin D supplementation: Recommendations for Canadian mothers and infants. Paediatr Child Health. 2007;12:583–598. [PMC free article] [PubMed] [Google Scholar]
- 77.Kovacs CS. Vitamin D in pregnancy and lactation: maternal, fetal, and neonatal outcomes from human and animal studies. Am J Clin Nutr. 2008;88:520S–528S. doi: 10.1093/ajcn/88.2.520S. [DOI] [PubMed] [Google Scholar]