

Abstract
The aim of this study was to identify whether there was a relationship between the distance that people have to carry water home and ill health. We conducted a systematic review for papers that reported on the association between diarrheal risk and distance. Six papers were identified for inclusion in the meta-analysis. These were all observational studies, and only two reported effect sizes that adjusted for possible confounding. Multiple different types of water sources supplied the study communities. The combined odds ratio (OR) showed a significant increase in illness risk in people living farther away from their water source (OR = 1.45; 95% confidence interval [CI] = 1.04–1.68). There is a need for better designed studies to further elucidate the health impacts on having to carry water home.
Water is widely accepted as being one of the most important natural resources for human health and development. However, despite this general consensus, the evidence of public-health benefit from water interventions, especially community interventions in low-income countries, remains unclear. In a recent systematic review, the authors were unable to identify a strong impact of community interventions on reducing diarrheal disease.1 Other authors have also cast doubt on the value of prioritizing communal water-infrastructure development.2 However, as discussed by Waddington and others,1 the vast majority of the community water interventions included in their review were of poor quality. One of the key problems is that, among the community-intervention studies included in this review, there were ones that were not likely to be able to show an effect. In this paper, we report an attempt to investigate the value of community water interventions in more detail by looking at one aspect of many community water systems in low-income countries, namely the distance that people have to walk to carry their water home. Globally, many people do not have a piped supply into their home. Hutton and others3 reported that many people, mainly women and girls, regularly spend 60 minutes or more per day in collecting and carrying home water. This short paper is a systematic review designed to investigate whether there is any relationship between the distance that people have to walk to carry water home and diarrheal disease
Several computerized literature databases were searched from 1950 to November 2009 without language restrictions. Databases searched were Pubmed (http://www.ncbi.nlm.nih.gov/pubmed/), Scopus (http://www.scopus.com/home.url), ScienceDirect (http://www.sciencedirect.com/), and SpringerLink (http://www.springerlink.com/home/main.mpx). The primary search strategy was “diarrh” AND “water” AND (“Distance” OR “time” OR “minutes”). In addition, the references of any included papers were also searched by hand. The full papers that looked relevant based on the title or abstract were retrieved and read in further detail.
The titles and abstracts of articles retrieved through the search were checked, read, and selected for inclusion if they fulfilled the following criteria: studies whose participants were households, children, or adults from developing countries; studies of populations that predominantly did not have a tap within the home but had to carry water from a tap or other source some distance from their home; studies where the health outcome was diarrhea; studies that attempted to determine whether there was a relationship between diarrheal disease and either distance from home to tap or time per trip to collect water. Studies that reported only distance or time to collect water, without linking these to reported illness rates, were excluded. Data were extracted from each paper to include effect size (relative risk [RR] or odds ratio [OR]) in relation to some distance comparison. Where neither RR or OR was given in the original paper, these were calculated from data in the paper. In the paper that presented only median incidence in the two groups and P value, the RRs were determined directly from the median values, and confidence intervals (CIs) were back-calculated from the P value presented in the paper.4 Where there was more than one possible breakpoint of distance given, the points closest to 150 m or 5–10 minutes walking time were chosen. Meta-analysis was performed with StatsDirect (http://www.statsdirect.com/).
From initial searches, 1,947 potentially relevant studies were identified. Of these, 1,803 studies were excluded after reviewing the titles, and another 119 were excluded after review of the abstract. The full text of the remaining 25 studies was obtained. Six studies met the inclusion criteria.5–9
Table 1 summarizes the characteristics of the included studies. In total, 7,208 people in five countries were examined; 5,625 were children under 5 years of age. Four studies analyzed the relationship between distance to water source and diarrhea incidence, and the remaining two studied the relationship between time and diarrhea incidence. Four studies were prospective follow-up studies, and two were case-control studies; only two studies reported effects sizes that adjusted for possible confounding variables. There was also marked heterogeneity in the sources of water that people accessed, even within studies.
Table 1.
Studies included in the analysis
| Study | Comparison point | Location | Population | No. of people in study | Study type and temporal setting | Water source | Adjusted for confounding |
|---|---|---|---|---|---|---|---|
| Gascon and others5 | 10 minutes | Tanzania | Children < 5 years | 309 | Case-control study in rainy season (March to May) | Not stated | No |
| Tonglet and others4 | 5 minutes | Zaire | Children < 4 years on registration | 1,096 | 1-year prospective follow-up study | Standpipes | No |
| Gorter and others6 | 150 m | Nicaragua | Children < 5 years | 2,458 | Case-control study | Mixed surface water, wells, and standpipes | Yes |
| Gorter and others7 | 128 m | Nicaragua | Children < 2 years | 172 | Prospective follow-up study over 5 months | Not stated | No |
| Semenza and others8 | 200 m | Uzbekistan | All ages | 1,583 | Prospective follow-up study over 9.5 weeks | Mixed surface water, wells, and standpipes | No |
| Zeitlin and others9 | Mean of distances | Bangladesh | Children < 2 years | 185 | Prospective follow-up study over 6 months | Tube well in 98% of households | Yes |
Figure 1 shows the summary meta-analysis plot. It can be seen that pooled OR in the random-effects mode is 1.45 (95% CI = 1.04–1.68). There was evidence of marked heterogeneity in the effect sizes (Cochran's Q = 26.6; degrees of freedom [df] = 6; P = 0.0002). Insufficient studies were included to give sufficient power to test for possible publication bias.
Figure 1.
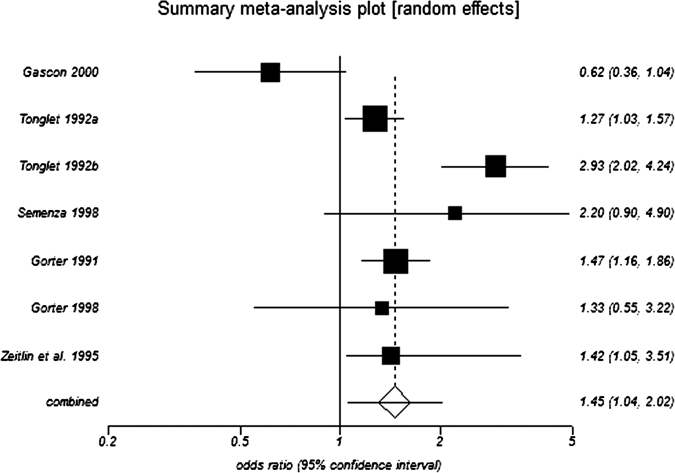
Forrest plot of diarrheal disease relative risk with increased distance from water source. The two effect sizes attributed to Tonglet and others4 relate to different subgroups defined by high- and low-diarrheal illness rates.
From the information available, it was not possible to fully identify any impact of seasonality. However, the one study that was clearly restricted to the rainy season actually found illness rates to be greater in those living closer to the water source.5 All other studies were either sufficiently long to have spanned both wet and dry seasons or did not give timings to say in which seasons they were conducted. It is certainly plausible that effect size and direction could be different in the wet and dry seasons if people close to the source have good-quality water most of the year but very poor water quality in the rainy season. By contrast, people who are at increased risk of disease throughout the year because they live a long way from their source may not experience much increased risk with further increase in exposure during the wet season because of higher levels of prior immunity from earlier infections.10 At least for the prospective studies, there does not seem to be any association between effect size and duration of the study.
Care must be exercised in not giving too much weight to this observation. All of the studies were completed more than 10 years ago, there is marked heterogeneity in effect size between studies, the authors often used statistical methods that would not be considered appropriate these days and they are all observational studies but only two studies adjusted for possible confounding variables. Furthermore, there were a range of different water sources used by the communities within and between the different studies.
Nevertheless, the meta-analysis presented here does suggest that distance from water source may be an important risk factor for diarrheal disease in children. However, given the use of a single breakpoint for each study and the different distance/time breakpoints used in different studies, it is not possible to give an indication of the nature of this relationship and how it may vary with context. The reason why there seems to be an association between distance and diarrheal risk is not clear, although it is plausible that one factor may be that lower availability of water leads to reduced personal hygiene.
There is a pressing need for some well-designed studies to test the hypothesis that distance from water source is indeed correlated with incidence of diarrhea. There is also a need to try to understand the reasons for any such association. Only with the availability of data from such studies would it be possible to better model the cost-effectiveness relationship between standpipe/water-source density and health and then, develop policy for appropriate density of water provision where it is not feasible to place taps in people's homes.
Acknowledgments
This work was supported by funds from the European Commission for the Healthy Water Project (FOOD-CT-2006-036306). The authors are solely responsible for the content of this publication. It does not represent the opinion of the European Commission. The European Commission is not responsible for any use that might be made of data appearing therein.
Footnotes
Disclosure: P.R.H. is Chair of the Board of Directors of the Institute of Public Health and Water Research and Chair of the Science Advisory Council to Suez Environment plc. This statement is made in the interest of full disclosure and not because the author considers this to be a conflict of interest.
Authors' addresses: Xia Wang and Paul R. Hunter, School of Medicine, Health Policy, and Practice, University of East Anglia, Norwich, UK, E-mails: X.Wang@uea.ac.uk and Paul.Hunter@uea.ac.uk.
References
- 1.Waddington H, Snilstveit B, White H, Fewtrell L. Water, Sanitation and Hygiene Interventions to Combat Childhood Diarrhoea in Developing Countries. International Initiative for Impact Evaluation, 3ie Synthetic Review 001. 2009. http://www.3ieimpact.org/admin/pdfs_synthetic2/1.pdf Available at. Accessed December 12, 2009.
- 2.Zwane AP, Kremer M. What Works in Fighting Diarrheal Diseases in Developing Countries? A Critical Review. World Bank Res Observer. 2007;22:1–24. [Google Scholar]
- 3.Hutton G, Haller L, Bartram J. Global cost-benefit analysis of water supply and sanitation interventions. J Water Health. 2007;5:481–502. doi: 10.2166/wh.2007.009. [DOI] [PubMed] [Google Scholar]
- 4.Tonglet R, Isu K, Mpese M, Dramaix M, Hennart P. Can improvements in water supply reduce childhood diarrhoea? Health Policy Plan. 1992;7:260–268. [Google Scholar]
- 5.Gascón J, Vargas M, Schellenberg D, Urassa H, Casals C, Kahigwa E, Aponte JJ, Mshinda H, Vila J. Diarrhea in children under 5 years of age from Ifakara, Tanzania: a case-control study. J Clin Microbiol. 2000;38:4459–4462. doi: 10.1128/jcm.38.12.4459-4462.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gorter AC, Sandiford P, Smith GD, Pauw JP. Water supply, sanitation and diarrhoeal disease in Nicaragua: results from a case-control study. Int J Epidemiol. 1991;20:527–533. doi: 10.1093/ije/20.2.527. [DOI] [PubMed] [Google Scholar]
- 7.Gorter AC, Sandiford P, Pauw J, Morales P, Pérez RM, Alberts H. Hygiene behaviour in rural Nicaragua in relation to diarrhoea. Int J Epidemiol. 1998;27:1090–1100. doi: 10.1093/ije/27.6.1090. [DOI] [PubMed] [Google Scholar]
- 8.Semenza JC, Roberts L, Henderson A, Bogan J, Rubin CH. Water distribution system and diarrheal disease transmission: a case study in Uzebekistan. Am J Trop Med Hyg. 1998;59:941–946. doi: 10.4269/ajtmh.1998.59.941. [DOI] [PubMed] [Google Scholar]
- 9.Zeitlin MF, Ahmed NU, Beiser AS, Zeitlin JA, Super CM, Guldan GS. Developmental, behavioural, and environmental risk factors for diarrhoea among rural Bangladeshi children of less than two years. J Diarrhoeal Dis Res. 1995;13:99–105. [PubMed] [Google Scholar]
- 10.Hunter PR, Zmirou-Navier D, Hartemann P. Estimating the impact on health of poor reliability of drinking water interventions in developing countries. Sci Total Environ. 2009;407:2621–2624. doi: 10.1016/j.scitotenv.2009.01.018. [DOI] [PubMed] [Google Scholar]