

INTRODUCTION
Flexibility in myocardial substrate metabolism for energy production is fundamental to cardiac health. This loss in plasticity or flexibility leads to an over dependence on the metabolism of an individual category of substrates with the predominance in fatty acid metabolism characteristic of diabetic heart disease and the accelerated glucose use associated with pressure-overload left ventricular hypertrophy being prime examples. Important unresolved questions include the extent to which these metabolic patterns are adaptive and have the propensity to become maladaptive, what are the key determinants of these metabolic perturbations, do they alter prognosis, and do they represent robust targets for novel therapeutics. Accelerating our understanding of the role of alterations in myocardial substrate metabolism cardiac disease is the development of transgenic models targeting key aspects of myocardial substrate use. However, the relevance of the metabolic phenotype of these models to the corresponding human condition is frequently unclear. In addition, applied genomics have identified numerous gene variants intimately involved in the regulation of myocardial substrate use. Yet, identifying the clinically significant genetic variants remains elusive. For all these reasons, there is a strong demand for accurate non-invasive imaging approaches of myocardial substrate metabolism that can facilitate the crosstalk between the bench and the bedside leading to improved patient management paradigms. Currently the most successful example is the detection of ischemic but viable myocardium with PET and 18F-fluorodexoglucose (FDG) for the management of patients with ischemic cardiomyopathy. In this review potential future applications of metabolic imaging, particularly radionuclide approaches, for assessment of cardiovascular disease are discussed.
Overview of Myocardial Metabolism-The Need for Flexibility
The heart is an omnivore capable of switching between one substrate to another for energy production. This flexibility in substrate use occurs in response to numerous stimuli including substrate availability, the hormonal environment, the level of tissue perfusion, and the level of workload by the heart (Figure 1).1, 2 The control of substrate switching can either represent an acute or chronic adaptation in response to either short or prolonged alterations in the physiological environment. Examples of acute or short term adaptations would include inhibitory effects of fatty acid oxidation on glucose oxidation as well as the converse, in addition of the oxidation of fatty acids by glucose oxidation as well as the increasing oxidation of glycogen, lactate and glucose in response to increasing workload. Regulating these rapid changes are a host enzymes such as pyruvate dehydrogenase complex and enzyme carnitine palmitoyl transferase 1 which is regulated by the concentration of malonyl-CoA.3–7
Figure 1.

Summary of myocardial substrate metabolism demonstrating the need for flexibility in myocardial substrate use to maintain myocardial health. DCM, Dilated cardiomyopathy; IR, insulin resistance; DM, diabetes mellitus. Reproduced with permission from Herrero P, Gropler RJ. Imaging of myocardial metabolism. J Nucl Cardiol 2005;12(3):345–358.
In contrast, chronic metabolic adaptations reflect alterations in the metabolic machinery of the heart. These changes occur primarily at the transcriptional level through the coordinated up-regulation of enzymes and proteins in key metabolic pathways. A prominent example in this case is the nuclear receptor peroxisome proliferator-activated receptor alpha (PPARα), which is a key regulator of myocardial fatty acid uptake, oxidation and storage.8 For example, in diabetes mellitus, PPARα activity is increased leading to an up-regulation in genes controlling fatty acid uptake and oxidation.9 In contrast, pressure-overload hypertrophy PPARα activity is reduced leading to a down-regulation of genes controlling fat metabolism and in turn leading to an up-regulation of glucose use.10 These chronic adaptations can induce numerous detrimental effects that extend beyond alterations in energy production and may include increases in oxygen free radical production, impaired energetics, increases in apoptosis, and the induction of left ventricular dysfunction. Discussed in the subsequent sections is how metabolic imaging has helped characterize this loss of metabolic flexibility due to these chronic adaptations in various disease processes.
Methods to Image Myocardial Metabolism
There are currently three methods to image myocardial metabolism noninvasively, magnetic resonance spectroscopy (MRS), single photon emission computed tomography (SPECT) and positron emission tomography (PET). A summary of each technique is listed below:
MRS
This technology offers numerous advantages for the measurement of myocardial metabolism. They include the ability to measure multiple metabolic pathways simultaneously, relative ease in performing serial measurements, and the lack of ionizing radiation. When combined with MRI, near simultaneous measurements of myocardial perfusion and mechanical function are possible. MRS allows direct measurement of biochemical information about in vivo processes. This biochemical data can be acquired repeatedly with minimal interference to tissue function. A number of biologically important nuclei can be measured including phosphorous (31P), hydrogen (1H), carbon (13C), sodium (23Na), nitrogen (15N) and fluorine (19F). The basic principle of MRS relies on the fact that the chemical environment of a nuclei induces local magnetic fields that shifts its resonance frequency. The different frequency shift for different metabolites results in an NMR signal consisting of one or more discrete resonance frequencies. The Fourier transform of the acquired signal produces a spectrum with peaks at distinct frequencies. The MRS spectrum displays the signal intensity as a function of frequency measured in parts per million (ppm) relative to the frequency of a reference compound. The signal intensity at a given frequency is proportional to the amount of the respective metabolite and can be used to determine the absolute concentration of the metabolite using appropriate calibrating reference signal.11, 12
MRS is limited by inherent low signal-to-noise, concomitant limited spatial resolution, intravoxel signal contamination and long acquisition times. Compared with nuclear imaging methods, MRS has a much lower sensitivity (detecting millimolar as opposed to nanomolar concentrations). Thus, although recent studies suggest imaging of cardiac metabolism using C-13 labeled agents is possible in intact animals, studies in humans are still not possible.13 Of note, cardiac applications for MRS become more limited as one moves from rodent to man as opposed to nuclear methods where the reverse occurs. This appears to be a function of both the higher field strength in the small bore systems and the use of radiofrequency coils that are in closer proximity to the entire heart used in small animal imaging. These advantages overcome the need for markedly improved spatial resolution. Indeed, as opposed to rodent hearts where the measurements of the left ventricular myocardium is obtained, measurements in human myocardium are typically limited to the anterior myocardium. Currently, only 31P and 1H have been widely used for in vivo clinical cardiac examinations focusing on myocardial energetics (31P) and lipid accumulation (1H).11, 13, 14
Single Photon Emission Computed Tomography (SPECT)
An advantage of SPECT is the inherent high sensitivity of the radionuclide method to measure metabolic processes. The technology is widely available in both the clinical and research setting. With ECG-gating, measurements of myocardial function can be obtained simultaneously. Because of the long-physical half-life of SPECT radionuclides radiopharmecutical delivery to multiple sites is possible, facilitating the performance of multi-center studies that incorporate measurements of myocardial substrate metabolism. Theoretically, assessing more than one metabolic process simultaneously is possible if the heart is imaged after the administration of radiopharmaceuticals labeled with radionuclides with different primary photon energies. Finally, small animal SPECT and SPECT/CT systems are rapidly advancing, facilitating the performance of myocardial metabolic studies in rodent models of cardiac disease. The major disadvantage of SPECT is the inability to quantify cellular metabolic processes primarily because of the technical limitations of SPECT (relatively poor temporal and spatial resolution and inaccurate correction for photon attenuation).
Metabolic processes that can be measure by SPECT include:
Glucose Metabolism: No specific SPECT radiotracers are currently available to measure myocardial glucose metabolism. However, when combined with the appropriate detection scheme or collimator design, myocardial glucose metabolism can be measured with SPECT and FDG15.
Fatty Acid Metabolism: Over the past 20 years numerous radiotracers have been developed to assess myocardial fatty acid metabolsim with SPECT. On the earliest and most promising was 15-(p-iodophenyl)-pentadecanoic acid (IPPA).16–18 This radiotacer demonstrated rapid accumulation in the heart and exhibited clearance kinetics that followed a biexponential function characteristic for 11C-palmitate. Moreover, the clearance rates correlated directly with β-oxidation. Initial studies in humans with coronary atherosclerosis demonstrated reduced uptake and washout and in regions subtended by occlude arteries19. Thus, the kinetics of IPPA made it quite attractive as a radiotracer of fatty acid metabolism. Unfortunately, SPECT systems did not have the temporal resolution to take advantage of the rapid turnover of IPPA. As a consequence quantification of myocardial fatty acid metabolism was not possible and image quality was reduced. This led to the development of branched-chain analogs of IPPA, such as 123I-beta-methyl-P-iodophenylpentadecanoic acid (BMIPP) (Figure 2).18–21 Alkyl branching inhibits β-oxidation and shunting radiolabel to the triglyceride pool thereby increasing radiotracer retention. The metabolic stability of BMIPP affords retention of radioactivity in the heart long enough to allow sufficient blood clearance such that high-quality SPECT imaging can be performed.
Figure 2.

Summary of the various PET and SPECT radiopharmaceuticals to assess myocardial substrate metabolism. FTHA, F-18 fluoro-6-thia-heptadecanoic acid. FCPHA, trans-9(RS)-18F-fluoro-3,4(RS,RS) methyleneheptadecanoic acid, BMIPP. 123I-beta-methyl-P iodophenylpentadecanoic acid HK, Hexokinase; PFK, phosphorfructokinase; ADP, adenosine diphosphate; TCA; tricarboxcylic acid cycle; PDH, pyruvate dehydrogenase; TG, triglyceride; G3PDH, glyceraldehyde 3-phosphate dehydrogenase;αGP, alpha-glycerol phosphate. Reproduced with permission from Herrero P, Gropler RJ. Imaging of myocardial metabolism. J Nucl Cardiol 2005;12(3):345–358.
PET
The two major advantages of PET are its intrinsic quantitative capability and the use of radiopharmaceuticals labeled with the positron-emitting radionuclides. The PET detection scheme permits accurate quantification of activity in the field of view. The positron-emitting radionuclides of the biologically ubiquitous elements oxygen (15O), carbon (11C), and nitrogen (13N), as well as fluorine (18F) substituting for hydrogen, can be incorporated into a wide variety of substrates or substrate analogues that participate in diverse biochemical pathways without altering the biochemical properties of the substrate of interest (Figure 2). By combining the knowledge of the metabolic pathways of interest with kinetic models that faithfully describe the fate of the tracer in tissue, an accurate interpretation of the tracer kinetics as they relate to the metabolic process of interest can be achieved. The major disadvantages of PET are its complexity in both radiotracer design and image quantification schemes and expense. Metabolic processes that are typically measured with PET are:
-
Myocardial Oxygen Consumption (MVO2):
15O-oxygen: Because oxygen is the final electron acceptor in all pathways of aerobic myocardial metabolism, PET with 15O-oxygen has also been used to measure MVO2. The major advantage of the approach is that it provides a measure of myocardial oxygen extraction and measures MVO2 directly. Due to the short half-life of this tracer, 15O-oxygen is readily applicable in studies requiring repetitive assessments, such as those with an acute pharmacologic intervention. Its major disadvantages are the need for a multiple-tracer study (to account for myocardial blood flow and blood volume) and fairly complex compartmental modeling to obtain the measurements. 22–24
11C-acetate: PET using 11C-acetate is the preferred method of measuring MVO2 noninvasively. Once taken up by the heart, acetate, a two-carbon chain free fatty acid, is rapidly converted to acetyl–CoA. The primary metabolic fate of acetyl-CoA is metabolism through the tricarboxylic acid cycle. Because of the tight coupling of the tricarboxylic acid cycle and oxidative phosphorylation, the myocardial turnover of 11C-acetate reflects overall flux in the tricarboxylic acid cycle and, thus, overall oxidative metabolism or MVO2. Either exponential curve fitting or compartmental modeling is used to calculate MVO2. The latter is typically preferable in situations of low cardiac output where marked splaying of the input function and spill-over of activity from the lungs to the myocardium can decrease the accuracy of the curve-fitting method.25–29
-
Carbohydrate metabolism:
FDG: Most studies of myocardial glucose metabolism with PET have used FDG. This radiotracer competes with glucose for facilitated transport into the sarcolemma then for hexokinase-mediated phosphorylation. The resultant F-FDG-6-phosphate is trapped in the cytosol and the myocardial uptake of FDG is thought to reflect overall anaerobic and aerobic myocardial glycolytic flux.30–33 Regional myocardial glucose utilization can be assessed in either relative or in absolute terms (i.e., in nmol·g−1·min−1). In the latter case, a mathematical correction for the kinetic differences between FDG and glucose called the lumped constant” must be used calculate rates of glucose. However, this value may vary depending upon the prevailing plasma substrate and hormonal conditions decreasing the accuracy of the measurement.32, 34–36 Other disadvantages of FDG include the limited metabolic fate of FDG in tissue, precluding determination of the metabolic fate (i.e., glycogen formation vs. glycolysis) of the extracted tracer and glucose, and limitations on the performance of serial measurements of myocardial glucose utilization because of the relatively long physical half-life of 18F. On the other hand, the myocardial kinetics of 18F-FDG have been well characterized, the acquisition scheme is relatively straightforward, and its production has become routine owing in part to the rapid growth of its clinical use in oncology; as such, it remains the most widely used tracer for determination of myocardial glucose metabolism.
Carbon-11 glucose: More recently, quantification of myocardial glucose utilization has been performed with PET using glucose radiolabeled in the 1-carbon position with 11C (11C-glucose). Because 11C-glucose is chemically identical to unlabeled glucose it has the same metabolic fate as glucose thus, obviating the need for the lumped constant correction. It has been demonstrated that measurements of myocardial glucose utilization based on compartmental modeling of tracer kinetics are more accurate with 11C-glucose than with FDG.37, 38 Moreover, it has been recently demonstrated that PET with 11C-glucose permits the estimation of glycogen synthesis, glycolysis and glucose oxidation (Figures 3 and 4).39 Disadvantages of this method include, compartmental modeling that is more demanding with 11C-glucose than it is with FDG, the need to correct the arterial input function for the production of 11CO2 and 11C-lactate, a fairly complex synthesis of the tracer, and short physical half-life of 11C requires an on-site cyclotron.
11C-lactate Lactate metabolism in the heart correlates with serum lactate level at rest but this relationship may vary with exercise or ischemia. Recently, a multi-compartment model was developed for the assessment of myocardial lactate metabolism using PET and L-3[11C] lactic acid. Under a wide variety of conditions, PET derived extraction of lactate correlated well with lactate oxidation measured by arterial and coronary sinus sampling (Figure 5).40 This model may help delineate the clinical role of lactate metabolism in a variety of pathological conditions such as diabetes mellitus and myocardial ischemia. Moreover, when combined with either FDG or 11C-glucose it permits a more comprehensive measurement of myocardial carbohydrate metabolism.
-
Fatty acid metabolism:
11C-palmitate: The major advantage of 11C-palmitate is that its myocardial kinetics is identical to labeled palmitate. With appropriate mathematical modeling techniques its use permits the assessment of various aspects of myocardial fatty acid metabolism such as uptake, oxidation and storage.41–44 This is an important attribute because exactly which component of myocardial fatty acid metabolism is the contributor(s) to a pathologic process is frequently not fully elucidated. However, this approach does suffer from several disadvantages including, reduced image quality and specificity, a more complex analysis, and the need for an on-site cyclotron and radiopharmaceutical production capability.
Fatty acid tracers that are trapped: Most of the PET tracers in this category have been designed to reflect myocardial β-oxidation. 14-(R,S)-18F-fluoro-6-thiaheptadecanoic acid (FTHA) was one of the first radiotracers developed using this approach. Initial results were promising with uptake and retention in the myocardium accordingly with changes in substrate delivery, blood flow and workload in animal models.45, 46 As a consequence, PET with FTHA was used to evaluate the effects of various diseases such as coronary artery disease and cardiomyopathy on myocardial fatty acid metabolism.47, 48 However, enthusiasm for FTHA has waned somewhat primarily because its uptake and retention has been shown to be insensitive to the inhibition of β-oxidation by hypoxia.49 Subsequently, 16-18F-fluoro-4-thia-palmitate (FTP) has been developed. This modification retains the metabolic trapping function of the tracer which is proportional to fatty acid oxidaion under normal oxygenation and hypoxic conditions.49, 50 However, the lumped constant for FTP relatively independent of the substrate environment but is very sensitive to the presence of ischemia. Thus, the ability quantify fatty acid oxidation with this radiotracer is still unclear. Currently, FTP is undergoing commercialization as entering early phase-1 evaluation. Recently, a new F-18–labeled fatty acid radiotracer, trans-9(RS)-18F-fluoro-3,4(RS,RS) methyleneheptadecanoic acid (FCPHA), has been developed.51 Results of initial studies show that uptake of FCPHA into rat myocardium was approximately 1.5% injected dose per gram tissue at 5 minutes with little change over a period of 60 minutes and low blood activity over the same period. However, the impact of alterations in plasma substrates, work load and blood flow on myocardial kinetics is unknown. This radiotracer is also undergoing commercialization.
FIGURE 3.

Correlation between PET and arterial and coronary sinus (ART/CS) measurement of fractional glycolysis (A) and glucose oxidation (B). Reproduced with permission from Herrero P, Kisrieva-Ware Z, Dence CS, et al. PET measurements of myocardial glucose metabolism with 1-11C-glucose and kinetic modeling. J Nucl Med. Jun 2007;48(6):955–964.
FIGURE 4.

Correlation between glycogen formation expressed as fraction of myocardial glucose obtained from ART/CS 11C measurements (y-axis) and heart 13C-glycogen content (x-axis) (A). Corresponding correlation between PET 11C and heart 13C-glycogen measurements (B). Fasted group was excluded from analysis because of negligible glucose extraction. Reproduced with permission from Herrero P, Kisrieva-Ware Z, Dence CS, et al. PET measurements of myocardial glucose metabolism with 1-11C-glucose and kinetic modeling. J Nucl Med. Jun 2007;48(6):955–964.
FIGURE 5.

Representative PET time–activity curves of L-3-11C-lactate obtained from intralipid (IL), insulin clamp (CLAMP), lactate infusion (LACTATE), or lactate and phenylepherine (LAC/PHEN) studies and corresponding myocardial images obtained 5–10 min after tracer injection and depicting primarily early tracer uptake. Images are displayed on horizontal long axis. Blood 11C = 11C time–activity curves obtained from region of interest (ROI) placed on left atrium; blood 11C-lactate = blood 11C time–activity curves after removing 11CO2, 11C-neutral, and 11C-basic metabolites; myocardial 11C = 11C time–activity curves obtained from ROI placed on lateral wall. A = apical wall; S = septal wall; L = lateral wall; LV = left ventricle. Reproduced with permission from Herrero P, Dence CS, Coggan AR, Kisrieva-Ware Z, Eisenbeis P, Gropler RJ. L-3-11C-lactate as a PET tracer of myocardial lactate metabolism: a feasibility study. J Nucl Med. Dec 2007;48(12):2046–2055.
Gender and Aging
Both gender and aging impact the myocardial metabolic phenotype. Results of studies in animal models show that there are sex differences in myocardial substrate metabolism, with female rats exhibiting less myocardial glucose and more fatty acid metabolism.52, 53 Recently, using PET with 11C-glucose and 11C-plamitate, these observations were confirmed in young healthy volunteers.54 Women exhibited lower levels of glucose metabolism compared with men (Figure 6). Although, no differences in myocardial fatty acid metabolism were noted, women also exhibited higher MVO2 compared with men as measured by PET with 11C-acetate. These gender differences in substrate metabolism become more pronounced as one transition to more pathologic conditions. For example in addition to the changes in glucose metabolism and MVO2, obese women exhibited higher fatty acid uptake and oxidation compared with obese men.55 Of note, in both these studies, the differences in myocardial metabolism could not be explained by differences in myocardial blood flow, insulin sensitivity, hemodynamics, myocardial work, or the plasma substrate environment.
Figure 6.

Sex-related differences in myocardial glucose extraction fraction (MGEF) and myocardial glucose utilization (MGU). Reproduced with permission from Peterson LR, Soto PF, Herrero P, Schechtman KB, Dence C, Gropler RJ. Sex differences in myocardial oxygen and glucose metabolism. J Nucl Cardiol. Jul 2007;14(4):573–581.
In various experimental models aging, the contribution of fatty acid oxidation to overall myocardial substrate metabolism declines with age.56, 57 It appears the cause for the decrease in fatty acid oxidation is multifactorial including changes in mitochondrial lipid content, lipid composition and protein interactions as well as oxygen free radical injury, a decline in carnitine palmitoyltransferase-1 activity, and a age-related decline in myocardial PPARα activity.58–60 Using the PET approaches described above, it has been shown that a similar metabolic shift occurs in healthy older humans.61 Moreover, older individuals are not able to increase glucose utilization in response to β-adrenergic stimulation with dobutamine to the same extent as younger individuals. This impaired metabolic response may represent a stress-related energy deprivation state in the aging heart or potentially indicate that the heart is more susceptible to injury during periods of ischemia.62 Recently it has been shown that this impairment in metabolic reserve can be ameliorated by endurance exercise training in older subjects.63 In keeping with the discussion above, it appears the myocardial metabolic response to dobutmaine following endurance exercise training is gender specific with men demonstrating an increase in myocardial metabolism whereas women exhibited increase in both glucose and fatty acid metabolism. Although, requiring further study, these gender and age differences in metabolism may provide a partial explanation for the gender- and age-related outcome differences for various cardiovascular diseases where altered myocardial metabolism plays a role.
Ischemia
Under conditions of mild to moderate myocardial ischemia, fatty acid oxidation ceases and anaerobic metabolism supervenes. Glucose becomes the primary substrate for both increased anaerobic glycolysis and for continued, albeit, diminished oxidative metabolism.64 This metabolic switch is prerequisite for continued a energy production and cell survival. When the ischemic insult is reversed, oxygen availability increases and oxidative metabolism resumes. However it appears that, these abnormalities myocardial substrate metabolism may persist well after the resolution of ischemia, so called “ischemic memory”. Demonstration of either accelerated myocardial glucose metabolism or reduced fatty acid metabolism using FDG and BMIPP, respectively, has been used to document this phenomena. For example, over twenty years ago it was shown that PET myocardial FDG uptake was increased in patients with unstable angina during pain-free episodes.65 Moreover, in patients with stable angina increased FDG uptake was demonstrated following exercise-induced ischemia-in the absence of either perfusion deficits or ECG abnormalities66. Similar observations have been made with SPECT using BMIPP. Results of numerous studies have demonstrated in patients with acute chest pain that abnormalities in myocardial BMIPP uptake may persist 24–36 hrs following the resolution of symptoms (Figure 7).67, 68 Moreover, this “metabolic fingerprint” is superior to perfusion imaging for either identifying coronary artery disease as the cause of the chest pain or assigning prognosis.67 The persistence of the metabolic defect increases the flexibility of radiotracer administration as it allows for delivery of a unit dose after the patient has already been evaluated. This is in contrast to the use of perfusion radiotracers which frequently must be available on-site due to the narrow time window from the resolution of symptoms and normalization of the flow deficit. Based on these observations, BMIPP is currently undergoing Phase 3 evaluation for acute chest pain imaging. Metabolic imaging with either FDG or BMIPP has also been for direct ischemia detection during stress testing. The thought process being that abnormalities in vasodilator reserve with perfusion tracers will underestimate ischemia if oxygen and supply remain balanced. Results of initial studies where FDG were injected during appears to support this contention with a greater detection rate for moderately severe coronary artery stenoses compared with perfusion imaging.15 Despite the promising results with these radiotracers, numerous questions still remain as the optimal imaging protocols, the impact of alterations in the plasma substrate environment on diagnostic accuracy, whether added diagnostic and prognostic information is provided over perfusion imaging, and whether this information alters clinical management.
Figure 7.
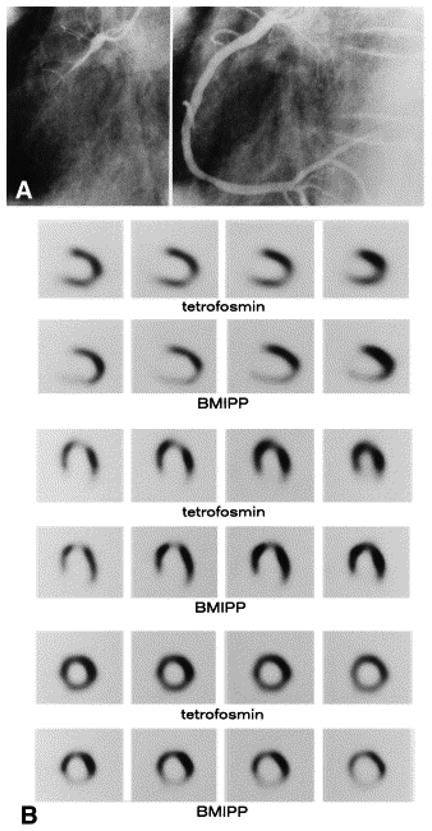
(A) Coronary angiogram of a 48-year-old woman with rest angina in the early morning. Seven days later, coronary angiography shows no significant stenosis in either coronary artery. After injection of ergonovine maleate into the right coronary artery, total spasm was provoked (left), with severe chest pain and electrocardiographic changes. After isosorbide dinitrate was injected, the spasm was completely resolved (right). (B) Series of rest tetrofosmin perfusion and BMIPP single-photon emission computed tomography images. No significant abnormal perfusion is observed on the rest tetrofosmin images at the time of hospital admission. However, the BMIPP images show reduced uptake in the inferior region on the next day. Reproduced with permission from Kawai Y, Tsukamoto E, Nozaki Y, Morita K, Sakurai M, Tamaki N. Significance of reduced uptake of iodinated fatty acid analogue for the evaluation of patients with acute chest pain. J Am Coll Cardiol. Dec 2001;38(7):1888–1894.
Hypertension/Left Ventricular Hypertrophy
There is well-established linkage between abnormalities in myocardial substrate metabolism and left ventricular hypertrophy. In animal models of pressure-overload left ventricular hypertrophy there is a reduction in the expression of of β-oxidation enzymes, leading to a fall in myocardial fatty acid oxidation and an increase in glucose use.69, 70 Moreover, interventions in animals that involve inhibition of mitochondrial fatty acid β-oxidation result in cardiac hypertrophy.70 In humans, variants in genes regulating key aspects of myocardial fatty acid metabolism ranging from PPARa to various key β-oxidative enzymes are associated with left ventricular hypertrophy.71, 72
This metabolic shift has been confirmed in-vivo in an animal model of hypertrophy.73 PET with FDG demonstrated myocardial glucose uptake tracked directly with increasing hypertrophy. Similar results have been found in man. PET with 11C-palmitate in humans has shown the reduction in myocardial fatty acid oxidation is an independent predictor of left ventricular mass in hypertension.74 Combining measurements of left ventricular myocardial external work (either by echocardiography or MRI) with measurements of MVO2 performed by PET with 11C-acetate or 15O-oxygen, it is possible to estimate cardiac efficiency23, 75. Using this approach in patients with hypertension-induced left ventricular hypertrophy has shown that the decline in myocardial fatty acid metabolism is associated with a decline in efficiency, a condition that may increase the potential for the development of heart failure. PET has also been used to phenotype patients with hypertrophic cardiomyopathy attributable to a known specific variant in the α-tropomyosin gene.76 It was observed that increased myocardial perfusion, fatty acid metabolism, and efficiency characterize patients with mild hypertrophy whereas these metabolic alterations decrease as hypertrophy becomes more advanced. The results may represent differential penetrance of the gene variant or the effect of modifier gene(s), potentially helping in their identification. Although, requiring further study in larger patient populations, this study suggests that metabolic imaging may identify relevant gene variants without waiting for more end-stage manifestations such as left ventricular remodeling and dysfunction to occur.
Nonischemic Dilated Cardiomyopathy
In addition to left ventricular hypertrophy, alterations in myocardial substrate metabolism have been implicated in the pathogenesis of contractile dysfunction and heart failure. Animal models of heart failure have shown that in the progression from cardiac hypertrophy to ventricular dysfunction, the expression of genes encoding for enzymes regulating β-oxidation is coordinately decreased, resulting in a shift in myocardial substrate metabolism to primarily glucose use, similar to that seen in the fetal heart.69, 77, 78 These metabolic changes are paralleled by re-expression of fetal isoforms of a variety of contractile and calcium regulatory proteins program. The reactivation of the metabolic fetal gene program may have numerous detrimental consequences on myocardial contractile function ranging from energy deprivation to the inability to process fatty acids leading to accumulation of nonoxidized toxic fatty acid derivatives, resulting in lipotoxicity. It should be noted that alterations in myocardial substrate use are now becoming attractive targets for novel treatments for heart failure with prime examples being the partial fatty acid oxidation antagonists and the insulin sensitizer glucagon-like peptide-1.79
The down-regulation in myocardial fatty acid metabolism leading to an over-dependence on glucose use in heart failure has been well documented using both PET and SPECT techniques. For example, PET using 11C-palmitate and 11C-glucose demonstrated that, myocardial fatty acid uptake and oxidation are lower in patients with nonischemic dilated cardiomyopathy when compared with aged matched controls. In contrast myocardial glucose utilization was higher in the cardiomyopathic patients.42 The metabolic findings cannot be explained by differences in plasma substrates or insulin, blood flow or MVO2. Similarly, SPECT with BMIPP demonstrated reduced myocardial uptake and increased clearance radiotracer in patients with dilated cardiomyopathy compared with controls.80 Moreover, the magnitude of the perturbations correlated with other measurements of heart failure severity such as left ventricular size and plasma b-natruietic peptide levels. PET has also been used provide mechanistic insights into the myocardial metabolic perturbations associated with heart failure. For example, abrupt lowering of fatty acid delivery with acipimox results in reduced fatty acid uptake, MVO2, and cardiac work and no change cardiac efficiency in normal volunteers.81 In contrast, patients with nonischemic dilated cardiomyopathy exhibited a decrease in myocardial fatty acid uptake and cardiac work, no change in MVO2 and a decline in efficiency. Although limited by a small sample size, these results appear to reinforce to the central role of loss flexibility in myocardial substrate metabolism in the pathogenesis of heart failure with even minor changes in substrate delivery having detrimental consequences on cardiac energy transduction.
Metabolic imaging can also been used to study the mechanisms responsible for the effectiveness of treatment in cardiomyopathy. For example, the efficacy of β-blocker therapy in treatment of heart failure patients is well established. Treatment with the selective β-blocker metoprolol results in a reduction in oxidative metabolism and an improvement in cardiac efficiency as measured by PET in patients with left ventricular dysfunction.82 With similar PET techniques, myocardial efficiency has been shown to be improved in patients with heart failure who undergo either exercise training or cardiac resynchronization therapy, implicating improved myocardial energetics as a potential mechanism.83, 84 Moreover, treatment with cardiac resynchronization therapy resulted in homogenization of initially heterogeneously distributed glucose metabolism.85 There is significant interest in the partial fatty acid oxidation inhibitors for the treatment of heart failure. Theoretically, decreasing myocardial fatty acid oxidation should increase the oxidation of glucose leading to a more favorable energetic state and improved left ventricular function. In a recent study, the administration of trimetizidine to patients with dilated cardiomyopathy resulted in a significant improvement in left ventricular ejection fraction.86 However, the improvement in left ventricular function appeared to reflect the complex interplay between a mild decrease in myocardial fatty acid oxidation, improved whole-body insulin resistance and synergestic effects with β-blockade. Metabolic imaging can also be used to predict the response to specific therapies in heart failure patients. For example, in patients with dilated cardiomyopathy, the percent of glucose uptake, as measured by PET with FDG can be used as a predictor for the effectiveness of β-blocker therapy.87 Moreover, in patients with ischemic cardiomyopathy the extent of viable myocardium as measured with PET and FDG correlated with the hemodynamic response after cardiac resynchronization therapy suggesting a role for PET in discriminating responders from non-responders.88
Diabetes Mellitus
Cardiovascular disease is the leading cause of morbidity and mortality in patients with diabetes mellitus.89 The mechanisms by which diabetes mellitus confers this increased cardiovascular risk are multifactorial and complex with possibilities including an increased prevalence of hyperlipidemia and hypertension, impaired fibrinolysis, abnormal myocardial endothelial function and reduced sympathetic neuronal function. There is a burgeoning body of evidence to suggest that abnormalities in myocardial substrate metabolism contribute to the cardiovascular abnormalities observed in diabetic patients.90, 91 As mentioned previously the metabolic phenotype in diabetes is an overdependence on fatty acid metabolism and a decrease in glucose use. Multiple mechanisms contribute to this phenotype. These include increased plasma delivery of fatty acids due peripheral insulin resistance, decreased insulin signaling, and activation of key transcriptional pathways such as the PPARα/PGC-1 signaling network.92–94 Both insulin-mediated glucose transport and glucose transporter expression decline in diabetes mellitus. However, rates of myocardial glucose uptake are frequently normal due to the presence of hyperglycemia. Further metabolism of extracted glucose declines. The increase in myocardial fatty acid utilization results in increased citrate levels which inhibit phosphofructokinase. Glucose oxidation is inhibited at the level of pyruvate dehydrogenase complex due to increased mitochondrial acetyl-CoA levels and the phosphorylation of pyruvate dehydrogenase kinase 4 by PPARα activation. Consequently, the maintenance of myocardial glucose uptake but a decrease in downstream metabolism results in an accumulation of glucose metabolites. Potential detrimental effects associated with this shift in metabolism include: impaired mechanical function due to the inability to increase glucose metabolism in response to increase myocardial work, depletion of tricarboxylic acid cycle intermediates due to reduced anapleurosis, electrical instability and apoptosis, a greater sensitivity to myocardial ischemia and myocardial lipid accumulation or lipotoxicity leading increased apoptosis.
Small animal imaging has helped clarify the mechanisms responsible for the metabolic alterations that occur in diabetes mellitus. Potential mechanisms underlying diabetic cardiomyopathy have been studied in transgenic mice. For example, mice with cardiac-restricted overexpression of PPARα demonstrate a metabolic phenotype that is similar to diabetic hearts.95 Small animal PET studies with 11C-palmitate and FDG in these mice demonstrate an increase in fatty acid uptake and oxidation and an abnormal suppression of glucose uptake. In contrast, in mice with cardiac-restricted overexpression of PPARβ/σ small animal PET measurements demonstrated an increase glucose uptake and reduced fatty acid uptake and oxidation.96 Taken is sum these observations demonstrate that PPARα and PPARβ/σ drive different metabolic regulatory programs in the heart and that imaging can help characterize genetic manipulations in mouse heart. However, from an imaging perspective, these studies also demonstrate the challenges in imaging the mouse heart due to its small size as only semi-quantitative measurements of tracer uptake were performed. However, quantitative measures of myocardial substrate metabolism are now possible with small animal PET in rat heart. For example, rates of myocardial glucose uptake correlate directly and closely and GLUT 4 gene expression in the Zucker-Diabetic-Fat (ZDF) rat, a model of type-2 diabetes mellitus.97 Moreover, rates of myocardial glucose uptake and fatty acid uptake and oxidation measured with PET in the same disease model demonstrated the importance of increased fatty acid delivery to defining the metabolic phenotype in diabetes (Figure 8).98
Figure 8.

Fatty acid metabolism measurements obtained in ZDF and lean rats by compartmental modeling of 11C-palmitate PET data. MFAUP = myocardial fatty acid uptake; MFAU = myocardial fatty acid utilization; MFAO = myocardial fatty acid oxidation; MFAO/MFAU myocardial FFA that was oxidized. *P < 0.001; **P < 0.01 Reproduced with permission from Welch MJ, Lewis JS, Kim J, Sharp TL, Dence CS, Gropler RJ, Herrero P. Assessment of myocardial metabolism in diabetic rats using small-animal PET: a feasibility study. J Nucl Med. Apr 2006;47(4):689–697.
Numerous imaging studies have been performed in humans to assess the impact of diabetes mellitus on myocardial glucose metabolism. These studies have been primarily limited to PET using FDG.99–101 In general, rates myocardial glucose uptake are reduced in patients either type 1 or type 2 diabetes mellitus compared with non-diabetics except in under conditions of marked hyperglycemia or supraphysiological levels in plasma insulin (such as occurs with a hyperinsulinemic-euglycemic clamp. Increased myocardial fatty acid uptake measured by arterial-coronary sinus balance studies has been reported in humans with type-1 diabetes mellitus without coronary artery disease.102 Although, the impact of plasma levels of free fatty acids on the level of myocardial fatty acid uptake was not determined, a negative correlation between myocardial glucose uptake and plasma fatty acid levels was observed. Recently studies using PET and 11C-plamitate and 11C-glucose in patients with type-1 diabetes mellitus have helped clarify the myocardial metabolic phenotype in this disease. For example, diabetic patients exhibited higher levels of fatty acid uptake and oxidation compared with non-diabetics primarily due to increased plasma fatty acid levels. In contrast, glucose uptake was reduced in these patients primarily due to decreased glucose transport mechanisms.43 Moreover, the metabolic fate of extracted glucose is impaired in diabetes with reduced rates of glycolysis and glucose oxidation which become more pronounced with increases in cardiac work induced by dobutamine (Figure 9).103 However, the diabetic myocardium is responsive to changes in plasma insulin and fatty acid levels but at a cost. Higher insulin levels are needed to achieve the same level of glucose uptake and glucose oxidation compared with non-diabetics consistent with myocardial insulin resistance (both). Similarly, in response to higher fatty acid plasma levels, myocardial fatty acid uptake is increased however at a cost of a greater esterification rate.103, 104
Figure 9.

Measurements of overall myocardial glucose uptake (MGU), glycolysis, glucose oxidation and glycogen synthesis for normal volunteers (NV), type-1 diabetic patients studied under baseline metabolic conditions (DM1) and diabetic patients studied during hyperinsulinemic-euglycemic clamp (DM1-C) both at rest (open bars) and during dobutamine (closed bars). Reproduced with permission from Herrero P, McGill JB, Lesniak D, et al. PET detection of the impact of dobutamine on myocardial glucose metabolism in women with type 1 diabetes mellitus. J Nucl Cardiol. November-December 2008;15(6):598–604.
The increase in plasma fatty acids are an attractive target to reduce the over dependence of the myocardium on fatty acid metabolism and perhaps improve energetics and function of the left ventricle. For example, the use of the insulin sensitizing agent troglitazone in ZDF rats results in reduced plasma fatty acid levels, decreased myocardial lipid accumulation, reduced apoptosis and improved left ventricular function.105 In PET with FDG studies in patients with type-2 diabetes mellitus, before and 26 weeks after treatment with rosiglitazone, demonstrated nearly a 40% increase in insulin-stimulated myocardial glucose uptake, implying reduced fatty acid uptake, which was attributed in large part to suppression in plasma fatty acid levels.106 Of note, similar metabolic changes were not seen with the biguanide, metformin whose mechanism of action is designed to reduce hepatic glucose production. The metabolic response could not be predicted by changes in the plasma glucose or HgBA1C levels. Thus, metabolic imaging can be used to follow the effects of therapies designed to alter myocardial substrate metabolism in patients with diseases such as diabetes mellitus where more readily available clinical parameters are not predictive of a therapeutic response.
Obesity and Insulin Resistance
It is now apparent that a significant increase in body mass index (BMI) induces marked increases in myocardial fatty acid metabolism. For example, in either dietary-induced or transgenic models of obesity myocardial fatty acid uptake and oxidation are significantly increased.105, 107 This increase at least initially, reflects the increase in fatty acid delivery to the heart due to increased lipolysis from both visceral/abdominal and subcutaneous fat stores secondary to insulin resistance. Similar to diabetes mellitus, the increased delivery of fatty acids likely initiates a cascade of events that lead to increased fatty acid metabolism. Ultimately, fatty acid uptake may exceed oxidation leading to extracted fatty acids entering non-oxidative pathways most likely initially forming triglycerides. As mentioned above, the accumulation of the neutral fats or triglycerides may ultimately become detrimental.105
Imaging of obese young women with PET and 11C-acetate and 11C-palmitate has demonstrated that an increase in BMI is associated with a shift in myocardial substrate metabolism toward greater fatty acid use. Moreover, this dependence on myocardial fatty acid metabolism increased with worsening insulin resistance.44 Of note, little change in myocardial glucose metabolism was observed. Paralleling the preferential use of fatty acids was an increase in MVO2 and a decrease in energy transduction. These findings suggest that metabolic changes in obesity may play a role in the pathogenesis of cardiac dysfunction. Of note, the myocardial metabolic response to obesity appears to gender dependent.55 For example, using similar PET techniques it has been recently demonstrated that in contrast to obese women, obese men had a greater impairment in myocardial glucose metabolism per level plasma insulin, suggesting greater myocardial insulin resistance. In addition, obesity had less effect on myocardial fatty acid metabolism in men. In contrast, MVO2 was higher in the obese women compared with obese men. Thus it appears there appears to be a complex interplay between gender and obesity in influencing myocardial substrate metabolism.
Beyond the Myocardium - Vascular Imaging
Atherosclerosis is a dynamic immune inflammatory process. It is characterized by cycles of intense activity and progression followed by intervals of stabilization. A common result of this process is coronary artery luminal stenosis that compromises myocardial blood flow and induces ischemia during stress. However, the most devastating event is acute plaque rupture with thrombosis leading to myocardial infarction and frequently, sudden cardiac death. Moreover, for many patients acute plaque rupture is the initial clinical event. Despite the plethora of currently available imaging tools to detect and characterize the extent and severity coronary atherosclerosis, none of them identify patients with active disease and who are at risk of plaque rupture. To this end, FDG is being evaluated for the detection of “biologically active” atherosclerosis based on the premise that the tracer accumulates in activated macrophages which are a key component atherosclerotic plaque. Several groups have established that inflamed arterial vessels have increased uptake of FDG as measured by PET. The increased uptake has been noted in animal models of atherosclerosis, and demonstrated in verified in humans with atherosclerosis of the carotid artery and aorta.108–111 Moreover, a significant correlation between FDG uptake and macrophage staining and CD68 staining has recently been established. Of interest a decrease in carotid artery FDG uptake is correlative with an increase in plasma high-density lipoprotein levels following statin therapy (Figure 10).110 However many questions remain such as the site of localization of radiotracer (e.g., plaque or smooth muscle), the suitability of the method for evaluating the coronary arteries, and whether the information provides more refined risk stratification compared with other more widely applicable methods or if it alters therapy.
Figure 10.
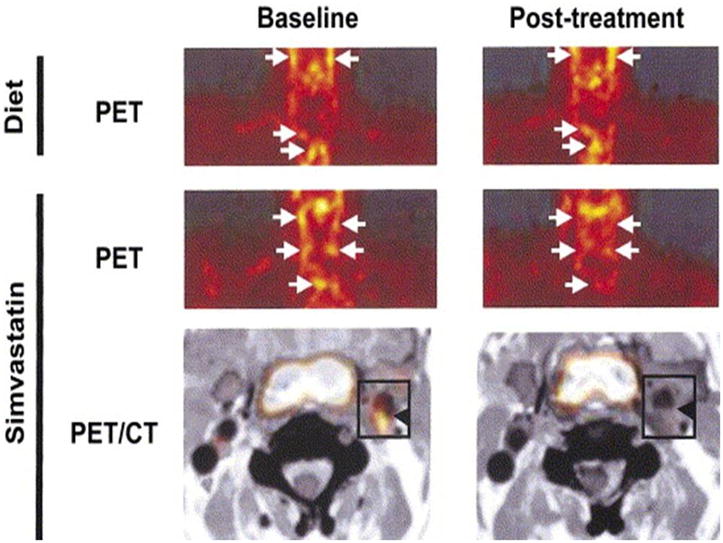

A. Effects of simvastatin on 18FDG uptake in atherosclerotic plaque inflammation. Representative 18FDG-PET images at baseline and after 3 months of treatment (post-treatment) with dietary management alone (diet) or simvastatin. (Top) Dietary management alone had no effect on 18FDG uptakes (arrows) in the aortic arch and the carotid arteries. (Middle) 18F-fluorodeoxyglucose uptakes were attenuated by simvastatin treatment. (Bottom) The co-registered images of 18FDG-PET and CT clearly show that the plaque 18FDG uptakes (arrowheads) disappeared after 3-month treatment with simvastatin. 10B. Correlations of changes in plaque 18F-fluorodeoxyglucose uptakes (ΔSUV) with alterations in HDL cholesterol (ΔHDL, mg/dl) and LDL cholesterol (ΔLDL, mg/dl) after 3-month treatment with dietary management alone (diet) or simvastatin. ΔSUV had a significant correlation only with ΔHDL in the statin group (LDL) cholesterol (A) and high-density lipoprotein (HDL) cholesterol. Reproduced with permission from Tahara N, Kai H, Ishibashi M, et al. Simvastatin attenuates plaque inflammation: evaluation by fluorodeoxyglucose positron emission tomography. J Am Coll Cardiol. Nov 7 2006;48(9):1825–1831.
Future Needs
The continued growth of metabolic imaging will require advances in several areas. First will be the continued improvement in instrumentation design, both at the human level as well as at the level of imaging of small animals. For example, accurate tracer quantification may be possible with new SPECT/CT systems where accurate attenuation correction can be performed. Advances in PET detector design and post-detector electronics will result in improved counting statistics which should improve the ability to perform more complex compartmental modeling permitting more complete characterization of the metabolism of a given substrate. Second, there is a key need for the development of new radiopharmaceuticals that permit characterization of key metabolic pathways such as uptake, storage or oxidation that are linked to disease manifestations. Moreover, new radiopharmaceuticals are needed to provide insights into the pleiotropic aspects of metabolism such as the relationships between substrate metabolism and cell growth, cell survival and energy transduction. Third, the availability of radiopharmaceuticals radiolabeled with either F-18 or I-123 will be needed for the performance of appropriately powered clinical trials designed to answer key questions about metabolic imaging regarding diagnostic accuracy, risk stratification and monitoring of therapy in specific patient populations. Taken together, these advances will facilitate the translation of metabolic imaging to the clinic.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Bing RJ. The metabolism of the heart. Harvey Lect. 1955;50:27–70. [PubMed] [Google Scholar]
- 2.Neely JR, Morgan HE. Relationship between carbohydrate and lipid metabolism and the energy balance of heart muscle. Ann Rev Physiol. 1974;36:413–459. doi: 10.1146/annurev.ph.36.030174.002213. [DOI] [PubMed] [Google Scholar]
- 3.Goodwin GW, Taegtmeyer H. Regulation of fatty acid oxidation of the heart by MCD and ACC during contractile stimulation. Am J Physiol. 1999 Oct;277(4 Pt 1):E772–777. doi: 10.1152/ajpendo.1999.277.4.E772. [DOI] [PubMed] [Google Scholar]
- 4.McGarry JD, Brown NF. The mitochondrial carnitine palmitoyltransferase system. From concept to molecular analysis. Eur J Biochem. 1997 Feb 15;244(1):1–14. doi: 10.1111/j.1432-1033.1997.00001.x. [DOI] [PubMed] [Google Scholar]
- 5.McGarry JD, Mannaerts GP, Foster DW. A possible role for malonyl-CoA in the regulation of hepatic fatty acid oxidation and ketogenesis. J Clin Invest. 1977 Jul;60(1):265–270. doi: 10.1172/JCI108764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sugden MC, Holness MJ. Recent advances in mechanisms regulating glucose oxidation at the level of the pyruvate dehydrogenase complex by PDKs. Am J Physiol Endocrinol Metab. 2003 May;284(5):E855–862. doi: 10.1152/ajpendo.00526.2002. [DOI] [PubMed] [Google Scholar]
- 7.Young ME, Goodwin GW, Ying J, Guthrie P, Wilson CR, Laws FA, Taegtmeyer H. Regulation of cardiac and skeletal muscle malonyl-CoA decarboxylase by fatty acids. Am J Physiol Endocrinol Metab. 2001 Mar;280(3):E471–479. doi: 10.1152/ajpendo.2001.280.3.E471. [DOI] [PubMed] [Google Scholar]
- 8.Kelly DP. PPARs of the heart: three is a crowd. Circ Res. 2003 Mar 21;92(5):482–484. doi: 10.1161/01.RES.0000064382.46274.95. [DOI] [PubMed] [Google Scholar]
- 9.Finck BN, Han X, Courtois M, Aimond F, Nerbonne JM, Kovacs A, Gross RW, Kelly DP. A critical role for PPARalpha-mediated lipotoxicity in the pathogenesis of diabetic cardiomyopathy: modulation by dietary fat content. Proc Natl Acad Sci U S A. 2003 Feb 4;100(3):1226–1231. doi: 10.1073/pnas.0336724100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Depre C, Shipley GL, Chen W, Han Q, Doenst T, Moore ML, Stepkowski S, Davies PJ, Taegtmeyer H. Unloaded heart in vivo replicates fetal gene expression of cardiac hypertrophy. Nat Med. 1998 Nov;4(11):1269–1275. doi: 10.1038/3253. [DOI] [PubMed] [Google Scholar]
- 11.Szczepaniak LS, Babcock EE, Schick F, Dobbins RL, Garg A, Burns DK, McGarry JD, Stein DT. Measurement of intracellular triglyceride stores by H spectroscopy: validation in vivo. Am J Physiol. 1999 May;276(5 Pt 1):E977–989. doi: 10.1152/ajpendo.1999.276.5.E977. [DOI] [PubMed] [Google Scholar]
- 12.Yoshida T. The rate of phosphocreatine hydrolysis and resynthesis in exercising muscle in humans using 31P-MRS. J Physiol Anthropol Appl Human Sci. 2002 Sep;21(5):247–255. doi: 10.2114/jpa.21.247. [DOI] [PubMed] [Google Scholar]
- 13.Lewandowski ED. Cardiac carbon 13 magnetic resonance spectroscopy: on the horizon or over the rainbow? J Nucl Cardiol. 2002 Jul–Aug;9(4):419–428. doi: 10.1067/mnc.2002.125811. [DOI] [PubMed] [Google Scholar]
- 14.Bottomley PA, Weiss RG. Non-invasive magnetic-resonance detection of creatine depletion in non-viable infarcted myocardium. Lancet. 1998 Mar 7;351(9104):714–718. doi: 10.1016/S0140-6736(97)06402-7. [DOI] [PubMed] [Google Scholar]
- 15.He ZX, Shi RF, Wu YJ, Tian YQ, Liu XJ, Wang SW, Shen R, Qin XW, Gao RL, Narula J, Jain D. Direct imaging of exercise-induced myocardial ischemia with fluorine-18-labeled deoxyglucose and Tc-99m-sestamibi in coronary artery disease. Circulation. 2003 Sep 9;108(10):1208–1213. doi: 10.1161/01.CIR.0000088784.25089.D9. [DOI] [PubMed] [Google Scholar]
- 16.DeGrado TR, Holden JE, Ng CK, Raffel DM, Gatley SJ. Quantitative analysis of myocardial kinetics of 15-p-[iodine-125] iodophenylpentadecanoic acid. J Nucl Med. 1989 Jul;30(7):1211–1218. [PubMed] [Google Scholar]
- 17.Dormehl IC, Hugo N, Rossouw D, White A, Feinendegen LE. Planar myocardial imaging in the baboon model with iodine-123-15-(iodophenyl)pentadecanoic acid (IPPA) and iodine-123-15-(P-iodophenyl)-3-R,S-methylpentadecanoic acid (BMIPP), using time-activity curves for evaluation of metabolism. Nucl Med Biol. 1995 Oct;22(7):837–847. doi: 10.1016/0969-8051(95)00015-p. [DOI] [PubMed] [Google Scholar]
- 18.Eckelman WC, Babich JW. Synthesis and validation of fatty acid analogs radiolabeled by nonisotopic substitution. J Nucl Cardiol. 2007 May–Jun;14(3 Suppl):S100–109. doi: 10.1016/j.nuclcard.2007.02.014. [DOI] [PubMed] [Google Scholar]
- 19.Reske SN, Sauer W, Machulla HJ, Knust J, Winkler C. Metabolism of 15 (p 123I iodophenyl-)pentadecanoic acid in heart muscle and noncardiac tissues. Eur J Nucl Med. 1985;10(5–6):228–234. doi: 10.1007/BF00254466. [DOI] [PubMed] [Google Scholar]
- 20.Ambrose KR, Owen BA, Goodman MM, Knapp FF., Jr Evaluation of the metabolism in rat hearts of two new radioiodinated 3-methyl-branched fatty acid myocardial imaging agents. Eur J Nucl Med. 1987;12(10):486–491. doi: 10.1007/BF00620471. [DOI] [PubMed] [Google Scholar]
- 21.Goodman MM, Kirsch G, Knapp FF., Jr Synthesis and evaluation of radioiodinated terminal p-iodophenyl-substituted alpha- and beta-methyl-branched fatty acids. J Med Chem. 1984 Mar;27(3):390–397. doi: 10.1021/jm00369a027. [DOI] [PubMed] [Google Scholar]
- 22.Iida H, Rhodes CG, Araujo LI, Yamamoto Y, de Silva R, Maseri A, Jones T. Noninvasive quantification of regional myocardial metabolic rate for oxygen by use of 15O2 inhalation and positron emission tomography. Theory, error analysis, and application in humans. Circulation. 1996 Aug 15;94(4):792–807. doi: 10.1161/01.cir.94.4.792. [DOI] [PubMed] [Google Scholar]
- 23.Laine H, Katoh C, Luotolahti M, Yki-Jarvinen H, Kantola I, Jula A, Takala TO, Ruotsalainen U, Iida H, Haaparanta M, Nuutila P, Knuuti J. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999 Dec 14;100(24):2425–2430. doi: 10.1161/01.cir.100.24.2425. [DOI] [PubMed] [Google Scholar]
- 24.Yamamoto Y, de Silva R, Rhodes CG, Iida H, Lammertsma AA, Jones T, Maseri A. Noninvasive quantification of regional myocardial metabolic rate of oxygen by 15O2 inhalation and positron emission tomography. Experimental validation. Circulation. 1996 Aug 15;94(4):808–816. doi: 10.1161/01.cir.94.4.808. [DOI] [PubMed] [Google Scholar]
- 25.Armbrecht JJ, Buxton DB, Schelbert HR. Validation of [1-11C]acetate as a tracer for noninvasive assessment of oxidative metabolism with positron emission tomography in normal, ischemic, postischemic, and hyperemic canine myocardium. Circulation. 1990 May;81(5):1594–1605. doi: 10.1161/01.cir.81.5.1594. [DOI] [PubMed] [Google Scholar]
- 26.Brown M, Marshall DR, Sobel BE, Bergmann SR. Delineation of myocardial oxygen utilization with carbon-11-labeled acetate. Circulation. 1987 Sep;76(3):687–696. doi: 10.1161/01.cir.76.3.687. [DOI] [PubMed] [Google Scholar]
- 27.Brown MA, Myears DW, Bergmann SR. Noninvasive assessment of canine myocardial oxidative metabolism with carbon-11 acetate and positron emission tomography. J Am Coll Cardiol. 1988 Oct;12(4):1054–1063. doi: 10.1016/0735-1097(88)90476-7. [DOI] [PubMed] [Google Scholar]
- 28.Buck A, Wolpers HG, Hutchins GD, Savas V, Mangner TJ, Nguyen N, Schwaiger M. Effect of carbon-11-acetate recirculation on estimates of myocardial oxygen consumption by PET. J Nucl Med. 1991 Oct;32(10):1950–1957. [PubMed] [Google Scholar]
- 29.Sun KT, Yeatman LA, Buxton DB, Chen K, Johnson JA, Huang SC, Kofoed KF, Weismueller S, Czernin J, Phelps ME, Schelbert HR. Simultaneous measurement of myocardial oxygen consumption and blood flow using [1-carbon-11]acetate. J Nucl Med. 1998 Feb;39(2):272–280. [PubMed] [Google Scholar]
- 30.Choi Y, Hawkins RA, Huang SC, Gambhir SS, Brunken RC, Phelps ME, Schelbert HR. Parametric images of myocardial metabolic rate of glucose generated from dynamic cardiac PET and 2-[18F]fluoro-2-deoxy-d-glucose studies. J Nucl Med. 1991 Apr;32(4):733–738. [PubMed] [Google Scholar]
- 31.Gambert S, Vergely C, Filomenko R, Moreau D, Bettaieb A, Opie LH, Rochette L. Adverse effects of free fatty acid associated with increased oxidative stress in postischemic isolated rat hearts. Mol Cell Biochem. 2006 Feb;283(1–2):147–152. doi: 10.1007/s11010-006-2518-9. [DOI] [PubMed] [Google Scholar]
- 32.Iozzo P, Chareonthaitawee P, Di Terlizzi M, Betteridge DJ, Ferrannini E, Camici PG. Regional myocardial blood flow and glucose utilization during fasting and physiological hyperinsulinemia in humans. Am J Physiol Endocrinol Metab. 2002 May;282(5):E1163–1171. doi: 10.1152/ajpendo.00386.2001. [DOI] [PubMed] [Google Scholar]
- 33.Krivokapich J, Huang SC, Selin CE, Phelps ME. Fluorodeoxyglucose rate constants, lumped constant, and glucose metabolic rate in rabbit heart. Am J Physiol. 1987 Apr;252(4 Pt 2):H777–787. doi: 10.1152/ajpheart.1987.252.4.H777. [DOI] [PubMed] [Google Scholar]
- 34.Botker HE, Bottcher M, Schmitz O, Gee A, Hansen SB, Cold GE, Nielsen TT, Gjedde A. Glucose uptake and lumped constant variability in normal human hearts determined with [18F]fluorodeoxyglucose. J Nucl Cardiol. 1997 Mar–Apr;4(2 Pt 1):125–132. doi: 10.1016/s1071-3581(97)90061-1. [DOI] [PubMed] [Google Scholar]
- 35.Hariharan R, Bray M, Ganim R, Doenst T, Goodwin GW, Taegtmeyer H. Fundamental limitations of [18F]2-deoxy-2-fluoro-D-glucose for assessing myocardial glucose uptake. Circulation. 1995 May 1;91(9):2435–2444. doi: 10.1161/01.cir.91.9.2435. [DOI] [PubMed] [Google Scholar]
- 36.Hashimoto K, Nishimura T, Imahashi KI, Yamaguchi H, Hori M, Kusuoka H. Lumped constant for deoxyglucose is decreased when myocardial glucose uptake is enhanced. Am J Physiol. 1999 Jan;276(1 Pt 2):H129–133. doi: 10.1152/ajpheart.1999.276.1.H129. [DOI] [PubMed] [Google Scholar]
- 37.Herrero P, Sharp TL, Dence C, Haraden BM, Gropler RJ. Comparison of 1-(11)C-glucose and (18)F-FDG for quantifying myocardial glucose use with PET. J Nucl Med. 2002 Nov;43(11):1530–1541. [PubMed] [Google Scholar]
- 38.Herrero P, Weinheimer CJ, Dence C, Oellerich WF, Gropler RJ. Quantification of myocardial glucose utilization by PET and 1-carbon-11-glucose. J Nucl Cardiol. 2002 Jan–Feb;9(1):5–14. doi: 10.1067/mnc.2001.120635. [DOI] [PubMed] [Google Scholar]
- 39.Herrero P, Kisrieva-Ware Z, Dence CS, Patterson B, Coggan AR, Han DH, Ishii Y, Eisenbeis P, Gropler RJ. PET measurements of myocardial glucose metabolism with 1-11C-glucose and kinetic modeling. J Nucl Med. 2007 Jun;48(6):955–964. doi: 10.2967/jnumed.106.037598. [DOI] [PubMed] [Google Scholar]
- 40.Herrero P, Dence CS, Coggan AR, Kisrieva-Ware Z, Eisenbeis P, Gropler RJ. L-3-11C-lactate as a PET tracer of myocardial lactate metabolism: a feasibility study. J Nucl Med. 2007 Dec;48(12):2046–2055. doi: 10.2967/jnumed.107.044503. [DOI] [PubMed] [Google Scholar]
- 41.Bergmann SR, Weinheimer CJ, Markham J, Herrero P. Quantitation of myocardial fatty acid metabolism using PET. J Nucl Med. 1996 Oct;37(10):1723–1730. [PubMed] [Google Scholar]
- 42.Davila-Roman VG, Vedala G, Herrero P, de las Fuentes L, Rogers JG, Kelly DP, Gropler RJ. Altered myocardial fatty acid and glucose metabolism in idiopathic dilated cardiomyopathy. J Am Coll Cardiol. 2002 Jul 17;40(2):271–277. doi: 10.1016/s0735-1097(02)01967-8. [DOI] [PubMed] [Google Scholar]
- 43.Herrero P, Peterson LR, McGill JB, Matthew S, Lesniak D, Dence C, Gropler RJ. Increased myocardial fatty acid metabolism in patients with type 1 diabetes mellitus. J Am Coll Cardiol. 2006 Feb 7;47(3):598–604. doi: 10.1016/j.jacc.2005.09.030. [DOI] [PubMed] [Google Scholar]
- 44.Peterson LR, Herrero P, Schechtman KB, Racette SB, Waggoner AD, Kisrieva-Ware Z, Dence C, Klein S, Marsala J, Meyer T, Gropler RJ. Effect of obesity and insulin resistance on myocardial substrate metabolism and efficiency in young women. Circulation. 2004 May 11;109(18):2191–2196. doi: 10.1161/01.CIR.0000127959.28627.F8. [DOI] [PubMed] [Google Scholar]
- 45.DeGrado TR. Synthesis of 14(R,S)-[18F]fluoro-6-thia-heptadecanoic acid (FTHA) J Label Comp Radiopharm. 1991;29:989–995. [Google Scholar]
- 46.DeGrado TR, Coenen HH, Stocklin G. 14(R,S)-[18F]fluoro-6-thia-heptadecanoic acid (FTHA): evaluation in mouse of a new probe of myocardial utilization of long chain fatty acids. J Nucl Med. 1991 Oct;32(10):1888–1896. [PubMed] [Google Scholar]
- 47.Schulz G, von Dahl J, Kaiser HJ, Koch KC, Sabri O, Banneitz L, Cremerius U, Buell U. Imaging of beta-oxidation by static PET with 14(R,S)-[18F]-fluoro-6-thiaheptadecanoic acid (FTHA) in patients with advanced coronary heart disease: a comparison with 18FDG-PET and 99Tcm-MIBI SPET. Nucl Med Commun. 1996 Dec;17(12):1057–1064. doi: 10.1097/00006231-199612000-00010. [DOI] [PubMed] [Google Scholar]
- 48.Taylor M, Wallhaus TR, Degrado TR, Russell DC, Stanko P, Nickles RJ, Stone CK. An evaluation of myocardial fatty acid and glucose uptake using PET with [18F]fluoro-6-thia-heptadecanoic acid and [18F]FDG in Patients with Congestive Heart Failure. J Nucl Med. 2001 Jan;42(1):55–62. [PubMed] [Google Scholar]
- 49.DeGrado TR, Wang S, Holden JE, Nickles RJ, Taylor M, Stone CK. Synthesis and preliminary evaluation of (18)F-labeled 4-thia palmitate as a PET tracer of myocardial fatty acid oxidation. Nucl Med Biol. 2000 Apr;27(3):221–231. doi: 10.1016/s0969-8051(99)00101-8. [DOI] [PubMed] [Google Scholar]
- 50.DeGrado TR, Kitapci MT, Wang S, Ying J, Lopaschuk GD. Validation of 18F-fluoro-4-thia-palmitate as a PET probe for myocardial fatty acid oxidation: effects of hypoxia and composition of exogenous fatty acids. J Nucl Med. 2006 Jan;47(1):173–181. [PubMed] [Google Scholar]
- 51.Shoup TM, Elmaleh DR, Bonab AA, Fischman AJ. Evaluation of trans-9-18F-fluoro-3,4-Methyleneheptadecanoic acid as a PET tracer for myocardial fatty acid imaging. J Nucl Med. 2005 Feb;46(2):297–304. [PubMed] [Google Scholar]
- 52.Desrois M, Sidell RJ, Gauguier D, Davey CL, Radda GK, Clarke K. Gender differences in hypertrophy, insulin resistance and ischemic injury in the aging type 2 diabetic rat heart. J Mol Cell Cardiol. 2004 Aug;37(2):547–555. doi: 10.1016/j.yjmcc.2004.05.014. [DOI] [PubMed] [Google Scholar]
- 53.Dyck JR, Lopaschuk GD. Glucose metabolism, H+ production and Na+/H+-exchanger mRNA levels in ischemic hearts from diabetic rats. Mol Cell Biochem. 1998 Mar;180(1–2):85–93. [PubMed] [Google Scholar]
- 54.Peterson LR, Soto PF, Herrero P, Schechtman KB, Dence C, Gropler RJ. Sex differences in myocardial oxygen and glucose metabolism. J Nucl Cardiol. 2007 Jul;14(4):573–581. doi: 10.1016/j.nuclcard.2007.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Peterson LR, Soto PM, Herrero P, Mohammed S, Avidan MS, Schechtman KB, Dence C, Gropler RJ. Impact of gender on the myocardial metabolic response to Obesity. J Am Coll Cardiol Imaging. 2008;1:424–433. doi: 10.1016/j.jcmg.2008.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Abu-Erreish GM, Neely JR, Whitmer JT, Whitman V, Sanadi DR. Fatty acid oxidation by isolated perfused working hearts of aged rats. Am J Physiol. 1977 Mar;232(3):E258–262. doi: 10.1152/ajpendo.1977.232.3.E258. [DOI] [PubMed] [Google Scholar]
- 57.McMillin JB, Taffet GE, Taegtmeyer H, Hudson EK, Tate CA. Mitochondrial metabolism and substrate competition in the aging Fischer rat heart. Cardiovasc Res. 1993 Dec;27(12):2222–2228. doi: 10.1093/cvr/27.12.2222. [DOI] [PubMed] [Google Scholar]
- 58.Iemitsu M, Miyauchi T, Maeda S, Tanabe T, Takanashi M, Irukayama-Tomobe Y, Sakai S, Ohmori H, Matsuda M, Yamaguchi I. Aging-induced decrease in the PPAR-alpha level in hearts is improved by exercise training. Am J Physiol Heart Circ Physiol. 2002 Nov;283(5):H1750–1760. doi: 10.1152/ajpheart.01051.2001. [DOI] [PubMed] [Google Scholar]
- 59.Odiet JA, Boerrigter ME, Wei JY. Carnitine palmitoyl transferase-I activity in the aging mouse heart. Mech Ageing Dev. 1995 Apr 14;79(2–3):127–136. doi: 10.1016/0047-6374(94)01552-w. [DOI] [PubMed] [Google Scholar]
- 60.Paradies G, Ruggiero FM, Gadaleta MN, Quagliariello E. The effect of aging and acetyl-L-carnitine on the activity of the phosphate carrier and on the phospholipid composition in rat heart mitochondria. Biochim Biophys Acta. 1992 Jan 31;1103(2):324–326. doi: 10.1016/0005-2736(92)90103-s. [DOI] [PubMed] [Google Scholar]
- 61.Kates AM, Herrero P, Dence C, Soto P, Srinivasan M, Delano DG, Ehsani A, Gropler RJ. Impact of aging on substrate metabolism by the human heart. J Am Coll Cardiol. 2003;41:293–299. doi: 10.1016/s0735-1097(02)02714-6. [DOI] [PubMed] [Google Scholar]
- 62.Soto PF, Herrero P, Kates AM, Dence CS, Ehsani AA, Davila-Roman VG, Schechtman KB, Gropler RJ. Impact of aging on myocardial metabolic response to dobutamine. Am J Physiol Heart Circ Physiol. 2003;285:2158–2164. doi: 10.1152/ajpheart.00086.2003. [DOI] [PubMed] [Google Scholar]
- 63.Soto PF, Herrero P, Schechtman KB, Waggoner AD, Baumstark JM, Ehsani AA, Gropler RJ. Exercise training impacts the myocardial metabolism of older individuals in a gender-specific manner. Am J Physiol Heart Circ Physiol. 2008 Aug;295(2):H842–850. doi: 10.1152/ajpheart.91426.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Lopaschuk G. Regulation of carbohydrate metabolism in ischemia and reperfusion. Am Heart J. 2000 Feb;139(2 Pt 3):S115–119. doi: 10.1067/mhj.2000.103919. [DOI] [PubMed] [Google Scholar]
- 65.Araujo LI, Camici P, Spinks TJ, Jones T, Maseri A. Abnormalities in myocardial metabolism in patients with unstable angina as assessed by positron emission tomography. Cardiovasc Drugs Ther. 1988 May;2(1):41–46. doi: 10.1007/BF00054251. [DOI] [PubMed] [Google Scholar]
- 66.Camici P, Araujo LI, Spinks T, Lammertsma AA, Kaski JC, Shea MJ, Selwyn AP, Jones T, Maseri A. Increased uptake of 18F-fluorodeoxyglucose in postischemic myocardium of patients with exercise-induced angina. Circulation. 1986 Jul;74(1):81–88. doi: 10.1161/01.cir.74.1.81. [DOI] [PubMed] [Google Scholar]
- 67.Kawai Y, Tsukamoto E, Nozaki Y, Morita K, Sakurai M, Tamaki N. Significance of reduced uptake of iodinated fatty acid analogue for the evaluation of patients with acute chest pain. J Am Coll Cardiol. 2001 Dec;38(7):1888–1894. doi: 10.1016/s0735-1097(01)01634-5. [DOI] [PubMed] [Google Scholar]
- 68.Tamaki N. Role of BMIPP imaging for risk stratification in patients with coronary artery disease. J Nucl Cardiol. 2005 Mar–Apr;12(2):148–150. doi: 10.1016/j.nuclcard.2005.01.007. [DOI] [PubMed] [Google Scholar]
- 69.Barger PM, Kelly DP. Fatty acid utilization in the hypertrophied and failing heart: molecular regulatory mechanisms. Am J Med Sci. 1999 Jul;318(1):36–42. doi: 10.1097/00000441-199907000-00006. [DOI] [PubMed] [Google Scholar]
- 70.Rupp H, Jacob R. Metabolically-modulated growth and phenotype of the rat heart. Eur Heart J. 1992 Sep;13( Suppl D):56–61. doi: 10.1093/eurheartj/13.suppl_d.56. [DOI] [PubMed] [Google Scholar]
- 71.Blair E, Redwood C, Ashrafian H, Oliveira M, Broxholme J, Kerr B, Salmon A, Ostman-Smith I, Watkins H. Mutations in the gamma(2) subunit of AMP-activated protein kinase cause familial hypertrophic cardiomyopathy: evidence for the central role of energy compromise in disease pathogenesis. Hum Mol Genet. 2001 May 15;10(11):1215–1220. doi: 10.1093/hmg/10.11.1215. [DOI] [PubMed] [Google Scholar]
- 72.Jamshidi Y, Montgomery HE, Hense HW, Myerson SG, Torra IP, Staels B, World MJ, Doering A, Erdmann J, Hengstenberg C, Humphries SE, Schunkert H, Flavell DM. Peroxisome proliferator--activated receptor alpha gene regulates left ventricular growth in response to exercise and hypertension. Circulation. 2002 Feb 26;105(8):950–955. doi: 10.1161/hc0802.104535. [DOI] [PubMed] [Google Scholar]
- 73.Handa N, Magata Y, Mukai T, Nishina T, Konishi J, Komeda M. Quantitative FDG-uptake by positron emission tomography in progressive hypertrophy of rat hearts in vivo. Ann Nucl Med. 2007 Dec;21(10):569–576. doi: 10.1007/s12149-007-0067-2. [DOI] [PubMed] [Google Scholar]
- 74.de las Fuentes L, Herrero P, Peterson LR, Kelly DP, Gropler RJ, Davila-Roman VG. Myocardial fatty acid metabolism: independent predictor of left ventricular mass in hypertensive heart disease. Hypertension. 2003 Jan;41(1):83–87. doi: 10.1161/01.hyp.0000047668.48494.39. [DOI] [PubMed] [Google Scholar]
- 75.de las Fuentes L, Soto PF, Cupps BP, Pasque MK, Herrero P, Gropler RJ, Waggoner AD, Davila-Roman VG. Hypertensive left ventricular hypertrophy is associated with abnormal myocardial fatty acid metabolism and myocardial efficiency. J Nucl Cardiol. 2006 May–Jun;13(3):369–377. doi: 10.1016/j.nuclcard.2006.01.021. [DOI] [PubMed] [Google Scholar]
- 76.Tuunanen H, Kuusisto J, Toikka J, Jaaskelainen P, Marjamaki P, Peuhkurinen K, Viljanen T, Sipola P, Stolen KQ, Hannukainen J, Nuutila P, Laakso M, Knuuti J. Myocardial perfusion, oxidative metabolism, and free fatty acid uptake in patients with hypertrophic cardiomyopathy attributable to the Asp175Asn mutation in the alpha-tropomyosin gene: a positron emission tomography study. J Nucl Cardiol. 2007 May–Jun;14(3):354–365. doi: 10.1016/j.nuclcard.2006.12.329. [DOI] [PubMed] [Google Scholar]
- 77.Buttrick PM, Kaplan M, Leinwand LA, Scheuer J. Alterations in gene expression in the rat heart after chronic pathological and physiological loads. J Mol Cell Cardiol. 1994 Jan;26(1):61–67. doi: 10.1006/jmcc.1994.1008. [DOI] [PubMed] [Google Scholar]
- 78.Sack MN, Kelly DP. The energy substrate switch during development of heart failure: gene regulatory mechanisms (Review) Int J Mol Med. 1998 Jan;1(1):17–24. doi: 10.3892/ijmm.1.1.17. [DOI] [PubMed] [Google Scholar]
- 79.Taegtmeyer H. Cardiac metabolism as a target for the treatment of heart failure. Circulation. 2004 Aug 24;110(8):894–896. doi: 10.1161/01.CIR.0000139340.88769.D5. [DOI] [PubMed] [Google Scholar]
- 80.Nakae I, Matsuo S, Koh T, Mitsunami K, Horie M. Iodine-123 BMIPP scintigraphy in the evaluation of patients with heart failure. Acta Radiol. 2006 Oct;47(8):810–816. doi: 10.1080/02841850600855354. [DOI] [PubMed] [Google Scholar]
- 81.Tuunanen H, Engblom E, Naum A, Scheinin M, Nagren K, Airaksinen J, Nuutila P, Iozzo P, Ukkonen H, Knuuti J. Decreased myocardial free fatty acid uptake in patients with idiopathic dilated cardiomyopathy: evidence of relationship with insulin resistance and left ventricular dysfunction. J Card Fail. 2006 Oct;12(8):644–652. doi: 10.1016/j.cardfail.2006.06.005. [DOI] [PubMed] [Google Scholar]
- 82.Beanlands RSB, Nahmias C, Gordon E, Coates G, deKemp R, Firnau G, Fallen E. The effects of β1-blockade on oxidative metabolism and the metabolic cost of ventricular work in patients with left ventricular dysfunction: a double-blind, placebo-controlled, positron-emission tomography study. Circ. 2000;102:2070–2075. doi: 10.1161/01.cir.102.17.2070. [DOI] [PubMed] [Google Scholar]
- 83.Stolen KQ, Kemppainen J, Ukkonen H, Kalliokoski KK, Luotolahti M, Lehikoinen P, Hamalainen H, Salo T, Airaksinen KEJ, Nuutila P, Knuuti J. Exercise training improves biventricular oxidative metabolism and left ventricular efficiency in patients with dilated cardiomyopathy. J Am Coll Cardiol. 2003;41(3):460–467. doi: 10.1016/s0735-1097(02)02772-9. [DOI] [PubMed] [Google Scholar]
- 84.Sundell J, Engblom E, Koistinen J, Ylitalo A, Naum A, Stolen KQ, Kalliokoski R, Nekolla SG, Airaksinen KEJ, Bax JJ, Knuuti J. The effects of cardiac resynchronization therapy on left ventricular function, myocardial energetics, and metabolic reserve in patients with dilated cardiomyopathy and heart failure. J Am Coll Cardiol. 2004;43(6):1027–1033. doi: 10.1016/j.jacc.2003.10.044. [DOI] [PubMed] [Google Scholar]
- 85.Nowak B, Sinha AM, Schaefer WM, Koch KC, Kaiser HJ, Hanrath P, Buell U, Stellbrink C. Cardiac resynchronization therapyhomogenizes myocardial glucosemetabolism and perfusion in dilatedcardiomyopathy and left bundle branch block. J Am Coll Cardiol. 2003;41(9):1523–1528. doi: 10.1016/s0735-1097(03)00257-2. [DOI] [PubMed] [Google Scholar]
- 86.Tuunanen H, Engblom E, Naum A, Nagren K, Scheinin M, Hesse B, Juhani Airaksinen KE, Nuutila P, Iozzo P, Ukkonen H, Opie LH, Knuuti J. Trimetazidine, a metabolic modulator, has cardiac and extracardiac benefits in idiopathic dilated cardiomyopathy. Circulation. 2008 Sep 16;118(12):1250–1258. doi: 10.1161/CIRCULATIONAHA.108.778019. [DOI] [PubMed] [Google Scholar]
- 87.Hasegawa S, Kusuoka H, Maruyama K, Nishimura T, Hori M, Hatazawa J. Myocardial positron emission computed tomographic images obtained with fluorine-18 fluoro-2-deoxyglucose predict the response of idiopathic dilated cardiomyopathy patients to beta-blockers. J Am Coll Cardiol. 2004;43(2):224–233. doi: 10.1016/j.jacc.2003.09.025. [DOI] [PubMed] [Google Scholar]
- 88.van Campen CM, Visser FC, van der Weerdt AP, Knaapen P, Comans EF, Lammertsma AA, de Cock CC, Visser CA. FDG PET as a predictor of response to resynchronisation therapy in patients with ischaemic cardiomyopathy. Eur J Nucl Med Mol Imaging. 2007 Mar;34(3):309–315. doi: 10.1007/s00259-006-0235-y. [DOI] [PubMed] [Google Scholar]
- 89.Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34:29–34. doi: 10.1016/0002-9149(74)90089-7. [DOI] [PubMed] [Google Scholar]
- 90.Stanley WC, Lopaschuck GD, McCormack JG. Regulation of energy substrate metabolism in the diabetic heart. Cardiovasc Res. 1997;34(1):25–33. doi: 10.1016/s0008-6363(97)00047-3. [DOI] [PubMed] [Google Scholar]
- 91.Rodrigues B, Cam MC, McNeill JH. Myocardial substrate metabolism: implications for diabetic cardiomyopathy. J Mol Cell Cardiol. 1995;27:169–179. doi: 10.1016/s0022-2828(08)80016-8. [DOI] [PubMed] [Google Scholar]
- 92.Stanley WC, Lopaschuk GD, McCormack JG. Regulation of energy substrate metabolism in the diabetic heart. Cardiovasc Res. 1997 Apr;34(1):25–33. doi: 10.1016/s0008-6363(97)00047-3. [DOI] [PubMed] [Google Scholar]
- 93.Taegtmeyer H, McNulty P, Young ME. Adaptation and maladaptation of the heart in diabetes: Part I: general concepts. Circulation. 2002 Apr 9;105(14):1727–1733. doi: 10.1161/01.cir.0000012466.50373.e8. [DOI] [PubMed] [Google Scholar]
- 94.Young ME, McNulty P, Taegtmeyer H. Adaptation and maladaptation of the heart in diabetes: Part II: potential mechanisms. Circulation. 2002 Apr 16;105(15):1861–1870. doi: 10.1161/01.cir.0000012467.61045.87. [DOI] [PubMed] [Google Scholar]
- 95.Finck BN, Lehman JJ, Leone TC, Welch MJ, Bennett MJ, Kovacs A, Han X, Gross RW, Kozak R, Lopaschuk GD, Kelly DP. The cardiac phenotype induced by PPARalpha overexpression mimics that caused by diabetes mellitus. J Clin Invest. 2002 Jan;109(1):121–130. doi: 10.1172/JCI14080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Burkart EM, Sambandam N, Han X, Gross RW, Courtois M, Gierasch CM, Shoghi K, Welch MJ, Kelly DP. Nuclear receptors PPARbeta/delta and PPARalpha direct distinct metabolic regulatory programs in the mouse heart. J Clin Invest. 2007 Dec;117(12):3930–3939. doi: 10.1172/JCI32578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Shoghi KI, Gropler RJ, Sharp T, Herrero P, Fettig N, Su Y, Mitra MS, Kovacs A, Finck BN, Welch MJ. Time course of alterations in myocardial glucose utilization in the Zucker diabetic fatty rat with correlation to gene expression of glucose transporters: a small-animal PET investigation. J Nucl Med. 2008 Aug;49(8):1320–1327. doi: 10.2967/jnumed.108.051672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Welch MJ, Lewis JS, Kim J, Sharp TL, Dence CS, Gropler RJ, Herrero P. Assessment of myocardial metabolism in diabetic rats using small-animal PET: a feasibility study. J Nucl Med. 2006 Apr;47(4):689–697. [PubMed] [Google Scholar]
- 99.Monti LD, Landoni C, Setola E, Galluccio E, Lucotti P, Sandoli EP, Origgi A, Lucignani G, Piatti P, Fazio F. Myocardial insulin resistance associated with chronic hypertriglyceridemia and increased FFA levels in Type 2 diabetic patients. Am J Physiol Heart Circ Physiol. 2004 Sep;287(3):H1225–1231. doi: 10.1152/ajpheart.00629.2003. [DOI] [PubMed] [Google Scholar]
- 100.Monti LD, Lucignani G, Landoni C, Moresco RM, Piatti P, Stefani I, Pozza G, Fazio F. Myocardial glucose uptake evaluated by positron emission tomography and fluorodeoxyglucose during hyperglycemic clamp in IDDM patients. Role of free fatty acid and insulin levels. Diabetes. 1995 May;44(5):537–542. doi: 10.2337/diab.44.5.537. [DOI] [PubMed] [Google Scholar]
- 101.vom Dahl J, Herman WH, Hicks RJ, Ortiz-Alonso FJ, Lee KS, Allman KC, Wolfe ER, Jr, Kalff V, Schwaiger M. Myocardial glucose uptake in patients with insulin-dependent diabetes mellitus assessed quantitatively by dynamic positron emission tomography. Circulation. 1993 Aug;88(2):395–404. doi: 10.1161/01.cir.88.2.395. [DOI] [PubMed] [Google Scholar]
- 102.Avogaro A, Nosadini R, Doria A, Fioretto P, Velussi M, Vigorito C, Sacca L, Toffolo G, Cobelli C, Trevisan R, et al. Myocardial metabolism in insulin-deficient diabetic humans without coronary artery disease. Am J Physiol. 1990 Apr;258(4 Pt 1):E606–618. doi: 10.1152/ajpendo.1990.258.4.E606. [DOI] [PubMed] [Google Scholar]
- 103.Herrero P, McGill JB, Lesniak D, Matthew S, Dence C, Scott S, Kisrieve-Ware Z, Gropler RJ. PET detection of the impact of dobutamine on myocardial glucose metabolism in women with type 1 diabetes mellitus. J Nucl Cardiol. 2008 November-December;15(6):598–604. doi: 10.1007/BF03007360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Peterson LR, Herrero P, McGill J, Schechtman KB, Kisrieva-Ware Z, Lesniak D, Gropler RJ. Fatty acids and insulin modulate myocardial substrate metabolism in humans with type 1 diabetes. Diabetes. 2008 Jan;57(1):32–40. doi: 10.2337/db07-1199. [DOI] [PubMed] [Google Scholar]
- 105.Zhou YT, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, Orci L, Unger RH. Lipotoxic heart disease in obese rats: implications for human obesity. Proc Natl Acad Sci U S A. 2000 Feb 15;97(4):1784–1789. doi: 10.1073/pnas.97.4.1784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Hallsten K, Virtanen KA, Lonnqvist F, Janatuinen T, Turiceanu M, Ronnemaa T, Viikari J, Lehtimaki T, Knuuti J, Nuutila P. Enhancement of insulin-stimulated myocardial glucose uptake in patients with Type 2 diabetes treated with rosiglitazone. Diabet Med. 2004 Dec;21(12):1280–1287. doi: 10.1111/j.1464-5491.2004.01332.x. [DOI] [PubMed] [Google Scholar]
- 107.Commerford SR, Pagliassotti MJ, Melby CL, Wei Y, Gayles EC, Hill JO. Fat oxidation, lipolysis, and free fatty acid cycling in obesity-prone and obesity-resistant rats. Am J Physiol Endocrinol Metab. 2000 Oct;279(4):E875–885. doi: 10.1152/ajpendo.2000.279.4.E875. [DOI] [PubMed] [Google Scholar]
- 108.Ogawa M, Ishino S, Mukai T, Asano D, Teramoto N, Watabe H, Kudomi N, Shiomi M, Magata Y, Iida H, Saji H. (18)F-FDG accumulation in atherosclerotic plaques: immunohistochemical and PET imaging study. J Nucl Med. 2004 Jul;45(7):1245–1250. [PubMed] [Google Scholar]
- 109.Rudd JH, Warburton EA, Fryer TD, Jones HA, Clark JC, Antoun N, Johnstrom P, Davenport AP, Kirkpatrick PJ, Arch BN, Pickard JD, Weissberg PL. Imaging atherosclerotic plaque inflammation with [18F]-fluorodeoxyglucose positron emission tomography. Circulation. 2002 Jun 11;105(23):2708–2711. doi: 10.1161/01.cir.0000020548.60110.76. [DOI] [PubMed] [Google Scholar]
- 110.Tahara N, Kai H, Ishibashi M, Nakaura H, Kaida H, Baba K, Hayabuchi N, Imaizumi T. Simvastatin attenuates plaque inflammation: evaluation by fluorodeoxyglucose positron emission tomography. J Am Coll Cardiol. 2006 Nov 7;48(9):1825–1831. doi: 10.1016/j.jacc.2006.03.069. [DOI] [PubMed] [Google Scholar]
- 111.Tawakol A, Migrino RQ, Bashian GG, Bedri S, Vermylen D, Cury RC, Yates D, LaMuraglia GM, Furie K, Houser S, Gewirtz H, Muller JE, Brady TJ, Fischman AJ. In vivo 18F-fluorodeoxyglucose positron emission tomography imaging provides a noninvasive measure of carotid plaque inflammation in patients. J Am Coll Cardiol. 2006 Nov 7;48(9):1818–1824. doi: 10.1016/j.jacc.2006.05.076. [DOI] [PubMed] [Google Scholar]