

Abstract
The study was conducted to evaluate if balance or weight training could alter gait characteristics of older adults contributing to a reduction in the likelihood of slip-induced falls. A total of 18 older adults were evaluated for the study. The results indicated decreases in heel contact velocities and the friction demand characteristics after eight weeks of training although fundamental gait characteristics such as walking velocity and step length were not changed. The results also indicated an increase in transitional acceleration of the whole body center of mass. The number of falls after eight weeks was reduced in training groups. These findings were found in conjunction with the improvements in knee flexor muscle and plantarflexor muscle strength. In conclusion, after training, older adults were less likely to initiate slips and more likely to recover from slips.
Keywords: Slip, Fall, Exercise, Older Adults, RCOF, Gait, Strength
INTRODUCTION
Slip-induced falls were most likely to occur when the required coefficient of friction (RCOF) at the shoe-floor interface exceeded the available coefficient of friction (ACOF) of the floor (Hanson et al., 1999; Irvine, 1986). RCOF was determined by a ratio of Fh (vertical force) over Fv (horizontal force) (Hanson et al., 1999). Modifications in either Fh or Fv could result in higher or lower RCOF. The RCOF was suggested to increase as heel contact velocity (HCV) increased or transitional acceleration of the whole body center of mass (TA COM) decreased because of their effects on the variation in horizontal ground reaction force while walking (Lockhart et al., 2003; Soames and Richardson, 1985). Therefore, inability to reduce heel contact velocity during the heel contact phase of the gait cycle could result in higher horizontal foot force leading to higher RCOF, contributing to the risk of slip-induced falls. Activation of hamstring muscles, tibialis anterior muscles and gluteus maximas and minimus muscles were functionally important indicators for horizontal heel contact velocity since one major role of these muscles was to decelerate the forward leg momentum during the heel contact phase of the gait cycle (Hashimoto et al., 2000).
Two other main factors that could influence RCOF were step length and transitional acceleration of the whole body center of mass (TA COM). RCOF (Fh / Fv) increased if resistance (horizontal) force (Fh) increases or normal (vertical) force decreases. Ankle strength during the push-off (i.e. plantarflexion) phase and hamstring strength during heel contact phase of gait cycle were important indicators for TA COM and heel contact velocity since roles of the muscles were to either accelerate forward body momentum after the heel contact or to decelerate forward leg momentum before the heel contact (Chen et al., 1997; Devita et al., 2000; Khuvasanont and Lockhart, 2002).
Previous studies (Aagaard et al., 2003; Barnett et al., 2003; Gardner et al., 2002; Jones et al., 1989; Mador et al., 2004; Woo et al., 2007) suggested that strength or balance training program could have a profound effect on reducing risk for falls, which could result in fewer injuries or even death. However, previous studies have not measured if training, in deed, would transform gait characteristics, resulting in a reduction in the likelihood of slip-induced falls. The present study evaluated if training would benefit particular aging gait characteristics that would contribute to the likelihood of slips and falls among older adults. Particularly, it was hypothesized that strengthening lower extremity muscles among older adults had an influence on speeding the forward progression of COM resulting in a decreased RCOF and on decelerating the forward leg momentum resulting in a decreased heel contact velocity. In other words, strength training would improve gait characteristics such that older adults’ risks for dangerous slips would be lessened.
METHOD
Subjects
Six individuals for each group totaling 18 individuals were examined: weight, balance, and control groups. The volunteers were recruited from Montgomery County, Virginia. Department of Park and Recreation for Montgomery County contacted all individuals (65 years or older) from their directory and asked if they volunteered to participate for the study. Each volunteer was randomly assigned to one of three groups. Each participant completed a written consent form approved by the Virginia Tech Internal Review Board (IRB) as well as listened to verbal explanations from graduate students. Participants were excluded from the study if they indicated any physical problems (i.e. hip, knee, ankle problems); a written questionnaire and a verbal interview were used as an initial screening tool. See Kim et al., (2009) for more details.
Balance and Weight Training
During the first week, exercises were performed on a hard surface floor in order for all the participants to be familiar with the balance exercise routines, which is provided in the instructional manual of Stability Trainer (Thera-Band®, 1245 Home Avenue, Akron, OH 44310). During 2nd week, all volunteers were tested to see if they could perform the exercises on green stability trainer (intermediate challenge level) with no assistance. If an individual could not perform the exercises safely on the stability trainer, his/her exercise routines continued on firm surface until she/he was able to perform the exercises safely on the green stability trainer. In addition, blue stability trainers (advanced challenge level) were introduced if an individual performed exercises perfectly and confidently on the green stability trainer. Among 6 volunteers, only 2 progressed to perform the exercises on blue stability trainer. They met three times a week.
Periodized strength training was implemented as it was proven to be more effective in gaining strength than non-periodized strength training (Baker et al., 1994; Fleck, 1999). Two different hypertrophy phases was introduced for 5 weeks; 3 sets of 10 repetitions with 50% of maximum exertion for 2 weeks and 3 sets of 10 repetitions for 70% of maximum exertion for 3 week. Strength phase lasted for the last 3 weeks; 3 sets of 7 repetitions with 85% of maximum exertion. See Kim et al. (2009) for details in exercise regimen.
Procedure and Gait Analysis
Peak isokinetic ankle and knee strengths at 30°, 90°, and 120° were evaluated using Biodex System 3. For ankle strength test, participants were seated with their right foot on a footplate attached to Biodex System 3 (Biodex Medical Systems, Inc., Shirley, New York 11967). For knee strength test, participants were seated with their right ankle strapped to a knee attachment fixed to Biodex System 3. The ankle and knee strength tests were performed as recommended in Biodex 3 Instructional Manual (Biodex Medical Systems, Inc., Shirley, New York 11967). Three trials for each measurement were collected and averaged to be used for statistical analysis.
Walking trials including the slipping and falling trials were conducted on a walking track (20m), which was elevated 15cm above the floor surface (Kim and Lockhart, 2008; Lockhart and Kim, 2006). Kinematic and kinetic data (see table 1 for variable definitions) were evaluated using 6 cameras and 2 force platforms (Kim et al., 2005). The entire walking track was covered with the vinyl tile. For slippery conditions, the vinyl tile surface was covered with a soap and water mixture (2:3) to reduce COF of the floor surface. The dynamic coefficient of friction of the soapy and dry vinyl floors was 0.07 and 1.80, respectively (Lockhart and Kim, 2006). The camera was calibrated before every experiment and the force plates were calibrated and zeroed before every trial.
Table 1. Variable Definitions.
| Variables | Definitions |
|---|---|
| Required Coefficient of Friction (RCOF) |
Peak 3 (vertical GRF/horizontal GRF) as defined by Perkins (1978) (see Fig. 1) |
| Right Heel contact velocity (HCV) |
The instantaneous horizontal heel contact velocity (HCV) was calculated utilizing the heel position in horizontal direction at the foot displacement of 1/120 second before and after the heel contact phase of the gait cycle using the instantaneous heel velocity formula: HV = [X (i+1) – X (i−1)]/ 2Δt. Heel contact was defined when the vertical force exceeded more than 7 N after the heel contacted the ground. |
| The whole body Center-of- Mass (COM) velocity (i.e., walking velocity) |
The Center of Mass was calculated by averaging all the centers of mass from the 14 segments (left and right feet, left and right shanks, left and right thighs, trunk, left and right hands, left and right lower arms, left and right upper arms, head). The COM velocity of all the participants was calculated using the formula: COM velocity = [X (i+1) – X (i-1)]/ 2Δt, where X = COM, Then, all COG velocities from left heel contact to right heel contact were averaged. |
| Step Length (SL) | The linear distance was measured in the direction of progression between successive points of foot-to-floor contact of left foot (X1, Y1) and right foot (X2,Y2). Step length was calculated from the distance between consecutive positions of the heel contacting the floor. |
| Initial Slip Distance (SDI) | Slip distance was divided into slip distance I (SDI) and slip distance II (SDII). SDI was measured to provide information concerning the severity of slip initiation. Slip-start point was defined as the point where non-rearward positive acceleration of the heel after heel contact, equivalently where the first minimum of the horizontal heel velocity after the heel contact (Figure 2). The slip-stop point for SDI was defined as the point where peak horizontal heel acceleration occurred after the slip-start point (mid slip on Figure 2). SDI was obtained using the heel coordinates between slip-start and slip-end point on the vinyl floor surface (Figure 2). |
| Slip Distance II (SDII) | Slip distance II provided information concerning the slip behavior after the initiation of slips. The start point for the slip distance II was defined from SDI slip-stop point (peak heel acceleration “mid slip” in Figure 2) to the end of slip (Lockhart et al., 2002 and 2003). The end of the slip was estimated as the time where the first maximum of the horizontal heel velocity after slip start point occurred (Figure 2). SDII was calculated from the heel coordinates using the distance between the two points as with SDI (Figure 2). |
| Peak Sliding Heel Velocity | The peak sliding heel velocity after slip-start point (see figure 2) was measured while slipping. This measure was used to predict slip severity in addition to slip distances. |
| Frequency of Actual Falls | A fall was identified via visual inspections of video recordings of the actual fall trials. A slipping event was identified as a fall if participants was aided by the fall arresting rig when attempting to recover from the slipping. |
Descriptive and inferential statistical analyses were performed by utilizing the JMP statistical packages (SAS Institute Inc. Cary, NC, USA). 2 × 3 (time; pre and post, group; weight, balance, control) repeated measure ANOVA was performed to evaluate the effects of training on the risk of slip-induced falls. In addition, 2 × 2 (floor; slippery and non-slippery, time; pre and post) within-subject ANOVA was performed on right HCV and step length to evaluate consistent gait patterns between normal walking trials and slippery walking trials to see if there were an order effect; data during dry surface condition was collected before wet surface since people’s gait characteristics changed after they walked over the slippery surface. The results were considered statistically significant when p≤0.05. To keep consistencies in the coefficient of friction between the wet floor surface and the experimental shoes, the available coefficient of the wet floor surface was tested daily and the same brand experimental shoes were used for every trial.
RESULTS
Gait characteristics (Floor × Time)
Table 2 suggested that there was no difference in HCV and step length while walking on the difference floor surface. These results suggested that participants did not notice slippery surface while approaching to the slippery area.
Table 2.
ANOVA summary of Right HCV and Step Length (Floor × Time)
| Right HCV | Step Length | |||
|---|---|---|---|---|
| Source | F | Prob >F | F | Prob >F |
| Floor | 1.66 | 0.20 | 0.24 | 0.62 |
| Time | 0.16 | 0.68 | 0.60 | 0.43 |
| Floor*Time | 0.02 | 0.88 | 0.006 | 0.93 |
Slip Vulnerability (Time × Group)
The data was collected during walking on the slippery surface. The results indicated that the risk of slips for all groups did not change after 8 weeks.
HCV
Table 3 (Time, p = 0.004) indicated that HCV was decreased at post-training stage. In addition, table 3 (Time*Group, p = 0.004), and student’s t-test (not provided) revealed that HCV was decreased only in training group.
Table 3.
ANOVA summary of HCV, COM Velocity, TA COM (transitional acceleration of center of mass), and Step Length (Time × Group)
| HCV | COM Velocity | TA COM | Step Length | |||||
|---|---|---|---|---|---|---|---|---|
| Source | F Ratio | Prob > F | F Ratio | Prob > F | F Ratio | Prob > F | F Ratio | Prob > F |
| Group | 9.41 | 0.002 | 6.69 | 0.008 | 11.64 | 0.0009 | 7.01 | 0.007 |
| Time | 11.45 | 0.004 | 2.09 | 0.168 | 12.57 | 0.002 | 2.17 | 0.16 |
| Time*Group | 7.96 | 0.004 | 0.15 | 0.857 | 4.82 | 0.02 | 0.34 | 0.71 |
COM Velocity (WV)
Table 3 indicated that there was no significant main or interaction effect.
TA COM
Table 3 and figure 3 indicated that, after 8 weeks, individuals in training groups walked with faster TA COM during heel contact phase of gait cycle, whereas, individuals in control group showed no change in TA COM (Time*Group, p = 0.02).
Fig. (3).
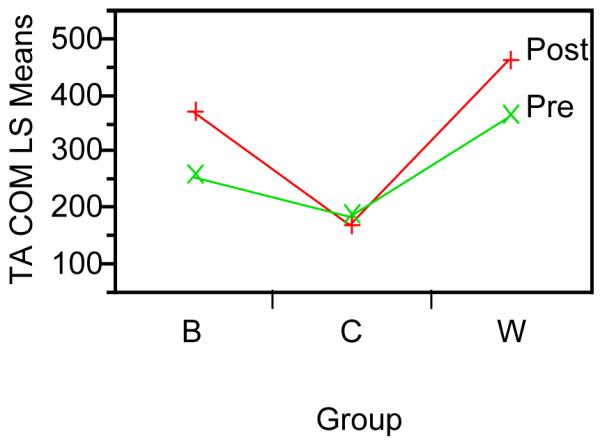
Interaction of Time × Group for TA COM (Post: post-training, Pre: pre-training, LS means: least square means, B: balance group, C: control group, W: weight group).
Step Length
Table 3 indicated that there was no significant main or interaction effect.
RCOF (friction demand)
Table 4 (Time, p = 0.03) indicated that the RCOF was reduced after training. Furthermore, student’s t-test suggested that the reduction in RCOF was seen only in training groups.
Table 4.
ANOVA summary of RCOF, SD1, SD2, and PSHV (Time × Group)
| RCOF | SD 1 | SD 2 | PSHV | |||||
|---|---|---|---|---|---|---|---|---|
| Source | F Ratio | Prob > F | F Ratio | Prob > F | F Ratio | Prob > F | F Ratio | Prob > F |
| Group | 0.96 | 0.40 | 0.004 | 0.99 | 1.53 | 0.24 | 3.55 | 0.05 |
| Time | 5.75 | 0.03 | 0.035 | 0.85 | 5.95 | 0.02 | 0.96 | 0.34 |
| Time*Group | 13.41 | 0.0005 | 0.593 | 0.56 | 11.19 | 0.001 | 0.37 | 0.69 |
Slip Severity
Table 4 indicated that that there was no significant main or interaction effect in SD 1 and PSHV. But, Table 4 and figure 4 indicated that, after 8 weeks, training groups showed a reduction in SD 2, whereas, control group showed no change in SD 2 (Time*Group, p = 0.001).
Fig. (4).
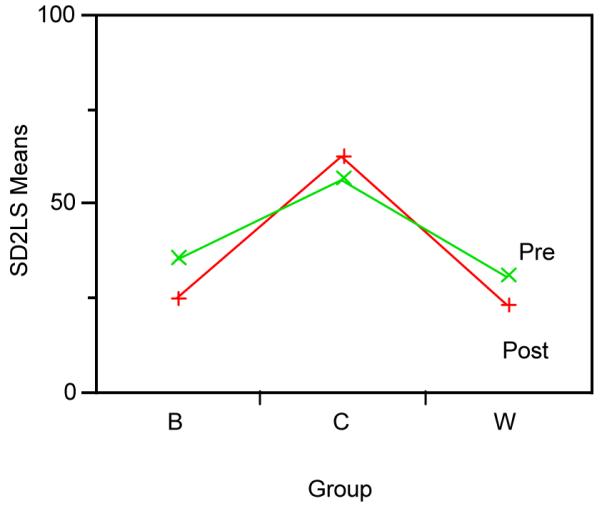
Interaction of Time × Group for SD 2 (Post: post-training, Pre: pre-training, LS means: least square means, B: balance group, C: control group, W: weight group)
Isokinetic Ankle and Knee Strength
Table 5 indicated that ankle plantarflexion and knee extension strengths improved only in the two exercise groups.
Table 5.
ANOVA of isokinetic ankle plantarflexion and knee extension strengths at various speeds
| Weight (N = 6) |
Balance (N = 6) |
Control (N = 6) |
P (Time) |
P (Group× Time) |
||
|---|---|---|---|---|---|---|
| A 30 Px | Pre | 38.3 ± 17.5 | 34.5 ± 8.5 | 22.7 ± 7.6 | 0.003 | 0.003 |
| Post | 48.0 ± 9.2 | 45.7 ± 12.1 | 23.7 ± 6.0 | |||
| A 90 Px | Pre | 27.3 ± 17.3 | 30 ± 9.2 | 17.5 ± 6.9 | 0.01 | 0.05 |
| Post | 40.2 ± 8.1 | 35.5 ± 11.8 | 17.0 ± 4.3 | |||
| A 120 Px | Pre | 25.7 ± 16.0 | 29.0 ± 10.0 | 16.7 ±6.6 | 0.001 | 0.02 |
| Post | 35.0 ± 8.0 | 33.3 ± 9.8 | 16.7 ± 5.2 | |||
| K 30 Ex | Pre | 68 ± 5.9 | 63.7 ± 12.7 | 53.5 ± 9.9 | 0.0001 | 0.001 |
| Post | 79.3 ± 13.9 | 73.3 ± 18.8 | 52.5 ± 10.3 | |||
| K 90 Ex | Pre | 52.3 ± 7.0 | 48.3 ± 14.5 | 40.7 ± 8.7 | 0.001 | 0.006 |
| Post | 59.5 ± 7.6 | 56.0 ± 13.7 | 38.8 ± 10.8 | |||
| K 120 Ex | Pre | 47 ± 7.6 | 45.2 ± 16.2 | 36.2 ± 6.9 | 0.0001 | 0.0004 |
| Post | 53.5 ± 8.1 | 48.2 ± 12.2 | 34.3 ± 7.2 |
* A = right ankle, K = right knee, Px = ankle plantarflexion, Ex = knee extension
Fall frequency
In balance training group or weight training group, 4 individuals in each group who fell in the pre-training stage recovered from slips and 2 individuals in each group who recovered from slips in the pre-training stage recovered from slips. In control group, 5 individuals who fell in the pre-training stage fell again and 1 individual who recovered from a slip again recovered. These results with consistent gait characteristics suggested that older individuals with training showed more chance to recover from slips.
DISCUSSION
After 8 weeks of training, older adults’ HCV and TA COM besides walking velocity and step length were altered in training groups. These results were similar to previous literatures (Schlicht et al., 2001; Sipila et al., 1996) although some studies indicated unclear relationship between strength gain and gait characteristics (Buchner et al., 1997; Singh, 1997). On the other hand, these previous studies did not attempt to see if changes in gait characteristics influenced the likelihood of slips or falls (i.e. RCOF).
As a result of neuro-musculo-skeletal degradation, older adults could not develop rapid torque at knee (Ferri et al., 2002) or ankle joints (Schultz et al., 1998; Connelly and Vandervoort, 2000), or could not generate explosive forces (Hook et al. 1999; Lexell, 1995). Lockhart and Kim (2006) reported that ability to generate adequate neural response in hamstring muscle could be a factor for a reduction in heel contact forces (i.e. horizontal shear force). In the present study, strength improvements in knee flexors could play a role in reducing the forward leg momentum in agreement with Lockhart and Kim (2006), and strength improvements in ankle plantar-flexor muscles played a role in pushing off the whole body center-of-mass in forward direction after the heel contact in agreement with Khuvasanont and Lockhart (2002). Reducing forward leg momentum and accelerating the whole body in forward direction were critical components in avoiding dangerous slips (Gronqvist et al. 1989; Lockhart et al., 2003). Individuals in training groups were capable of reducing HCV and of increasing TA COM and, thus, lessening the RCOF. Moreover, it was noteworthy to see improvements in slip propensity (i.e. slower HCV and faster TA COM) among older adults in training groups without exhibiting alterations in fundamental gait characteristics such as walking velocity and step length. In addition, WV and SL (Lockhart and Kim, 2006) were suggested to influence the likelihood of slips due to its mechanical effects on an increase in horizontal shear force component at the heel contact phase of gait cycle. It was generally suggested that older adults exhibited slower gait and shorter SL because they wanted to maintain safer gait characteristics. However, older adults fell more (Lockhart et al., 2002; Lockhart and Kim, 2006) than their younger counterparts. These findings maybe indicated that slower gait and shorter SL should not be referred as a safer gait. It could be more proper to refer slower gait and shorter SL as an aging gait or a pathological gait. The present study suggested that older adults with neuromusculoskeletal training were able to walk normally, but were able to reduce the likelihood of slip by altering only HCV and TA COM.
In the present study, slip severity evaluated by SD 2 were decreased after 8 weeks in only training groups although SD 1 and PSHV were not different after 8 weeks among all three groups. These results suggested that participants in training group were able to recover from the initial slip (e.g. no difference in SD 1, but, significant reductions in SD 2) suggesting that exercise training would influence recovery mechanisms (e.g. they attempted to retract their foot earlier to recover from the initial slip). This could result in small SD 2 in training groups. Also, TA COM difference seen in the present study further supported the effect of training on recovery mechanism. Previous studies (Lockhart et al., 2002; Lockhart and Kim, 2006) reported that younger adults exhibited severe slips than older adults; however, younger adults fell less frequently than older adults. Those studies suggested that fewer falls in younger adults were because they exhibited faster TA COM than older adults. Faster TA COM may have helped individuals to retract their slipping foot or to progress their center of mass forward closer to their slipping foot; two main techniques to recover from the slips was to retract their foot closer to their center of body or to progress their center of mass forward closer to the slipping foot. The present study also found a similar result which participants in training groups recovered more frequently and exhibited enhancements in TA COM. These results suggested that training played a role in improving mechanisms contributing to the forward progression of the whole body COM during double stance phase. Authors in the present study found that all fallers at the pre-training stage fell backward: upper body (i.e. head, trunk, and arms) twisting backward while lower body (i.e. slipping foot) continuously moving forward as slipping. However, non-faller who fell at the pre-training stage exhibited their upper body in forward progressing motion while slipping when they recovered from slipping. These video analyses further emphasized the impacts of faster TA COM in recovering from slipping.
There were some limitations in the present study. The number of each group was 6. The experimenter had no choice but to start the program, immediately with available participants since the experimenter could not postpone the program to wait for the preferred number of participants to join. In fact, most participants would have dropped out if training was postponed for additional participants. Gender was not balanced out across the groups due to the circumstance explained already. Therefore, it was not possible to evaluate the gender effect. This could cause problems when generalizing the results of the present study to all female and male adults over 65 years old. In addition, the experimenter assumed that all individuals were comparable to each other and that all individuals may respond similarly to the programs. Descriptive statistics (i.e. mean and standard deviation) suggested that that height, weight, and age across the three groups were not significantly different. These similarities in physical figures minimized the threat to internal validity. Still, their education level, attitude, personality, motor ability, and mental ability were not statistically evaluated to indicate if those groups were comparable. These factors may influence measures while walking or slipping and responding to questionnaires. Ideally, in the future, more comparable individuals should be tested to minimize the selection bias. The experimenters challenged to monitor each individual’s activities throughout eight weeks. However, it was not possible to monitor their every minute lives which may have consisted of performing heavy housework, gardening, or home improvement projects.
The present study concluded that in order for the elderly to recover effectively or efficiently from dangerous slipping, it was far advantageous to have the whole body center of mass progressed forward enough after heel contact was made. Additionally, improvements in the ankle plantarflexor and knee flexor strengths accounted for improvements in transitional acceleration of COM and for the reduction in HCV, respectively. As a result, training played a critical role in reducing slip-propensity among older adults.
Fig. (1).

Composite view of the Fx (horizontal force), Fz (vertical force), and RCOF (friction demand, the ration of Fx to Fz) during a typical normal walking on dry surface.
Fig. (2).

Composite view of the heel dynamics (kinetics and kinematics) during a typical normal walking on dry surface. Heel dynamics during the first 0.16 s of stance phase. (Lockhart and Kim 2006)
ACKNOWLEDGEMENT
We would like to thank Kemvia Adams-Bush, the recreation supervisor at the Department of Park and Recreation at Montgomery County, for recruiting and monitoring participants, and planning social activities.
Footnotes
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Aagaard P, Simonsen Erik B., Andersen Jesper L., Magnusson Peter, Dyhre-Poulsen Poul. Increased rate of force development and neural drive of human skeletal muscle following resistance training. Journal of Applied Physiology. 2003;93(4):1318–1326. doi: 10.1152/japplphysiol.00283.2002. [DOI] [PubMed] [Google Scholar]
- Barnett A, Ben S, Stephen R, Mandy W, Adrian B. Community-based group exercise improves balance and reduces falls in at-risk older people: a randomized controlled trial. Age and Ageing. 2003;32:407–414. doi: 10.1093/ageing/32.4.407. [DOI] [PubMed] [Google Scholar]
- Buchner D, Elaine C, Barbara L, Esselman P, Margherita A, Price R, Wagner E. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol Med Sci. 1997;52A:M218–M224. doi: 10.1093/gerona/52a.4.m218. [DOI] [PubMed] [Google Scholar]
- Chen IH, Kuo KN, Andriacchi TP. The influence of walking speed on mechanical joint power during gait. Gait and Posture. 1997;6:171–176. [Google Scholar]
- Connelly D, Vandervoort A. Effects of isokinetic strength training on concentric and eccentric torque development in the ankle dorsiflexors of older adults. The Journal of Gerontology Series: Biol Sciences and Med Sciences. 2000;55:B465–B472. doi: 10.1093/gerona/55.10.b465. [DOI] [PubMed] [Google Scholar]
- DeVita P, Hortobagyi T. Age causes a redistribution of joint torques and powers during gait. J Appl Physiol. 2000;88:1804–1811. doi: 10.1152/jappl.2000.88.5.1804. [DOI] [PubMed] [Google Scholar]
- Ferri A, Scaglioni G, Pousson M, Capodaglio P, Van Hoecke J, Narici MV. Strength and power changes of the human plantar flexors and knee extensors in response to resistance training in old age. Acta Physiologica Scandinavica. 2002;177(1):69–78. doi: 10.1046/j.1365-201X.2003.01050.x. [DOI] [PubMed] [Google Scholar]
- Gardner MM, Phty M, Robertson MC, McGee R, Campbell AJ. Application of a fall-prevention program for older people to primary health care practice. Prev Med. 2002;34:546–53. doi: 10.1006/pmed.2002.1017. [DOI] [PubMed] [Google Scholar]
- Hanson J, Redfern M, Mazumdar M. Predicting slips and falls considering required and available friction. Ergonomics. 1999;42(12):1619–1633. doi: 10.1080/001401399184712. [DOI] [PubMed] [Google Scholar]
- Hashimoto F, Ogawa R, Kameyama O. Control engineering and electomyographic kinesiology analyses of normal human gait. J Orthop Sci. 2000;5:139–49. doi: 10.1007/s007760050141. [DOI] [PubMed] [Google Scholar]
- Hook P, Li SP, Sleed J, Hughes S, Larsson L. In vitro motility speed of slow myosin extracted from single soleus fibres from young and old rats. J Physiol (London) 1999;520:463–471. doi: 10.1111/j.1469-7793.1999.00463.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irvine CH. Evaluation of the effect of contact-time when measuring floor slip resistance. Journal of Testing and Evaluation. 1986;1:19–22. [Google Scholar]
- Jones D, Rutherford O, Parker D. Physiological changes in skeletral muscle as a result of strength training. Q J Exp Physiol. 1989;74:233–256. doi: 10.1113/expphysiol.1989.sp003268. [DOI] [PubMed] [Google Scholar]
- Kim Sukwon, Lockhart TE. 10% front load carriage on the likelihood of slips and falls. Industrial Health. 2008;46:32–39. doi: 10.2486/indhealth.46.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Sukwon, Lockhart TE, Roberto K. The effects of 8-week balance training or weight training for the elderly on fear of falling measures and social activity levels. Quality in Ageing. doi: 10.1108/14717794200900030. Accepted for publication on January 20, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Sukwon, Lockhart TE, Yoon H. Relationship between age-related gait adaptations and required coefficient of friction. Safety Science. 2005;43:425–436. doi: 10.1016/j.ssci.2005.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khuvasanont T, Lockhart TE. Age-related ankle strength and the effects on the slip-induced falls; The Proceeding of the XVI Annual International Society of Occupational Ergonomics and Safety (ISOES); Toronto, Canada. June, 9, 2002; 2002. pp. 1–5. Slips, Trips & Falls III. Session 5-4. [Google Scholar]
- Lexell J. Human aging, muscle mass, and fiber type composition. J Gerontol Series A. 1995;50A:11–16. doi: 10.1093/gerona/50a.special_issue.11. Special Issue. [DOI] [PubMed] [Google Scholar]
- Lockhart TE, Woldstad JC, Smith JL, Ramsey JD. Effects of age related sensory degradation on perception of floor slipperiness and associated slip parameters. Safety Science. 2002;40:689–703. doi: 10.1016/S0925-7535(01)00067-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lockhart TE, Woldstad JC, Smith JL. Effects of age-related gait changes on biomechanics of slips and falls. Ergonomics. 2003;46(12):1136–1160. doi: 10.1080/0014013031000139491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lockhart TE, Kim S. Relationship between Hamstring Activation Rate and Heel Contact Velocity: Factors Influencing Age-Related Slip-Induced Falls. Gait and Posture. 2006;24:23–34. doi: 10.1016/j.gaitpost.2005.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mador MJ, Erkan B, Ajay A, Mary S, Thomas K. Endurance and strength training in patients with COPD. Chest. 2004;125:2036–2045. doi: 10.1378/chest.125.6.2036. [DOI] [PubMed] [Google Scholar]
- Rantanen T. Muscle strength, disability, and mortality. Scandinavian Journal of Medicine and Science in Sports. 2003;13:3–8. doi: 10.1034/j.1600-0838.2003.00298.x. [DOI] [PubMed] [Google Scholar]
- Schlicht J, Camaionea David N., Owen Steven V. Effect of Intense Strength Training on Standing Balance, Walking Speed, and Sit-to-Stand Performance in Older Adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2001;56:M281–M286. doi: 10.1093/gerona/56.5.m281. [DOI] [PubMed] [Google Scholar]
- Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. J Gerontol Med Sci. 1997;52A:M27–M35. doi: 10.1093/gerona/52a.1.m27. [DOI] [PubMed] [Google Scholar]
- Sipila S, Multanen J, Kallinen M, Era P, Suominen H. Effects of strength and endurance training on isometric muscle strength and walking speed in elderly women. Acta Physiol Scand. 1996;156:457–464. doi: 10.1046/j.1365-201X.1996.461177000.x. [DOI] [PubMed] [Google Scholar]
- Thelen DG, Brockmiller C, Ashton-Miller JA, Schultz AB, Alexander NB. Thresholds for sensing foot dorsi- and plantar-flexion during upright stance: effects of age and velocity. J Gerontol A Biol Sci Med Sci. 1998;53:33–38. doi: 10.1093/gerona/53a.1.m33. [DOI] [PubMed] [Google Scholar]
- Woo J, Hong Athena, Lau Edith, Lynn Henry. A randomised controlled trial of Tai Chi and resistance exercise on bone health, muscle strength and balance in community-living elderly people. Age and Ageing. 2007;36(3):262–268. doi: 10.1093/ageing/afm005. [DOI] [PubMed] [Google Scholar]