

Abstract
Medication error is a major cause of morbidity and mortality in medical profession, and anaesthesia and critical care are no exception to it. Man, medicine, machine and modus operandi are the main contributory factors to it. In this review, incidence, types, risk factors and preventive measures of the medication errors are discussed in detail.
Keywords: Adverse drug event, drug error, medication error
INTRODUCTION
“The error of one moment becomes the sorrow of whole life”
- A Chinese proverb
The management of anaesthesia and critical patients has become safe with the advent of newer safe anaesthesia drugs, good quality equipments and high standards of monitoring, but the practice of poly-pharmacy, complex working conditions and involvement of multilevel medical and paramedical staff expose these areas to potentially life threatening medication error at some point of the treatment process.
Although majority of these errors are without any serious adverse outcome but some of them are associated with increased morbidity and mortality leading to prolonged hospital stay, high cost of treatment and potential for litigation.[1,2] The Institute of Medicine (IOM) report highlights that 44000 - 98000 patients die each year as a result of medical errors, a large portion of these being medication related.[3]
INCIDENCE
Medication errors are common in health care system and reported to be the seventh most common cause of death overall.[4] A total of 2266 members of the Canadian Society of Anaesthesiologists were approached to find out the incidence of medication errors. Surprisingly 30% of them admitted to experience at least more than one error in their lifetime.[5] Japanese Society of Anaesthesiologists (JSA) investigated 27454 anaesthesia procedures over a period of 8 years (1999 – 2007). Out of total 233 incidences of medication error, 6.2% were clerical errors, hence they were not included in the study. Rest were either over-dose (25%), substitution error (23%) or omission error (21%).[6] A total of 89% of respondents in a survey of anaesthesiologists in New Zealand have admitted to made a drug administration error at some stage of their carrier.[7] In a retrospective review of 2000 anaesthetic procedures in Australia, 144 were found to be involved in wrong drug administration.[8] In an another study of 55426 cases in Norway, 63 (0.11%) cases of a drug error were found, out of which 3 cases were classified as serious.[9]
Among critically ill patients, the rate of medical error ranges from 1.2 to 947 errors per 1000 ICU days with a median of 106 errors per 1000 ICU days.[10,11] In intensive care although majority (40%) were of wrong infusion rate.[12] In another study, the incidence of adverse drug event (ADE) was found to be similar in medical ICU and coronary care unit of a tertiary care hospital (127.8 and 131.5 errors per 1000 patient days, respectively).[13]
All these reports are the tip of the iceberg as many cases are not reported due to various reasons like different population variation, clinical practice variation, lack of uniformity in definition, method of reporting and collection of data, fear of blaming and defamation among colleagues etc.[14]
TYPES OF MEDICATION ERRORS
A medication error is any error in the medication process, whether there are adverse consequences or not [Table 1]. Errors can be divided into two groups according to the working system:[15] active failure and latent conditions. Active failure are unsafe acts committed by people who are in direct contact with the patient, slip and lapse are skill behaviour errors whereas mistakes are knowledge-based errors due to perception, judgement, inference or interpretation. Latent conditions are due to the reasons within the system and occurs when individuals make decisions that have unintended consequences in the future.[15,16]
Table 1.
Definition of medication errors[16]
| Medical error | The failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim |
| Medication error | Any error in the medication process, whether there are any adverse consequences or not |
| Adverse drug event | Any injury related to the use of a drug. Not all adverse drug events are caused by medical error or vice versa |
| Preventable ADE | Harm that could have been avoided through reasonable planning or proper execution of an action |
| Near miss | The occurrence of an error that did not result in harm |
| Slip | A failure to execute an action due to routine behaviour being misdirected |
| Lapse | A failure to execute an action due to lapse in memory and a routine behaviour being omitted |
Alternatively, errors can be classified as error of omission or error of commission. Errors of omission are defined as failure to perform an appropriate action whereas errors of commission are defined as performing an inappropriate action.[17]
The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) realised the need for a standardised categorisation of error. On 16 July 1996, this council adopted a medication error index that classified the error according to the severity of the out come[18] [Figure 1]. This is required for categorising medication errors. The ISMP has already implemented this index for use in the database.
Figure 1.
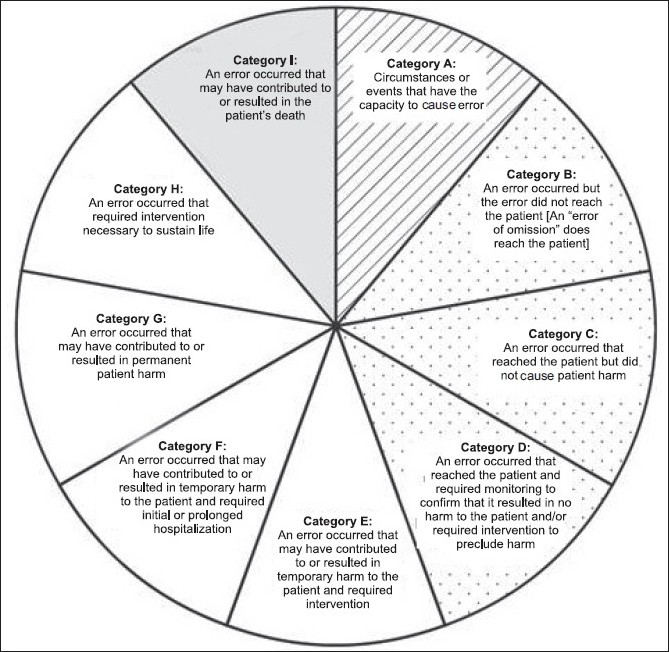
NCC MERP medical error index 18. No error: category A; error, no harm: category B, C, D; error, harm: category E, F, G, H; error, death : category I
TIME OF THE MEDICATION ERROR
Critical incidents occurred most commonly during middle of the anaesthesia (42%), frequently during induction (28%) and at the beginning of the procedure (17%).[19] Against the popular belief that most of the medication errors occur in late night shifts, Fasting et al[9] found that out of 63 drug errors only 1 occurred at night, whereas 56 incidences occurred in day shifts.
The administration of a single dose of any drug to the patient in critical care requires at least 80 - 200 individual steps at different stages namely prescription, transcription, preparation, dispersion, and administration.[20] Most errors occurs during the administration stage (53%), followed by prescription (17%), preparation (14%), and transcription (11%).[21]
RISK FACTORS
Previous reviewers had concentrated primarily on quantitating the overall anaesthesia risk using mortality as the measure of negative outcomes. Human errors were believed to be a factor ranging from 65-87% for deaths during anaesthesia in several studies.[22–25]
Attempts to identify the risk factors have been limited to variables related to either surgical procedures or patients. Factors associated with anaesthesia and/or factors that may have predisposed to an anaesthesia error were not analysed. Furthermore, no study has focused on the process of error, devices, etc, regardless of the outcome. Cooper and colleagues[26] have identified several risk factors in a critical incident analysis to study preventable mistakes. Maximum errors were due to either inadequate experience (16%) or due to inadequate familiarity to equipment or device (9.3%) whereas haste and inattention or carelessness each amounted to 5.6% errors during anaesthesia [Table 2].
Table 2.
Risk factors for errors during anaesthesia[26]
| Inadequate total experience | 77 |
| Inadequate familiarity with equipment/device | 45 |
| Poor communication with team | 27 |
| Haste | 26 |
| Inattention/carelessness | 26 |
| Fatigue | 24 |
| Excessive dependency on other personnel | 24 |
| Failure to perform normal check | 22 |
| Training or experience | 22 |
| Lack of enough supervision | 18 |
| Environment or colleagues | 18 |
| Visual field restricted | 17 |
| Mental and physical factors | 16 |
| Inadequate familiarity with surgery | 14 |
| Distraction | 13 |
| Poor labelling of controls, drug | 12 |
| Supervision-related factors | 12 |
| Situation precluded normal precautions | 10 |
| Inadequate familiarity with the anaesthetic technique | 10 |
| Teaching activity underway | 09 |
| Apprehension | 08 |
| Emergency case | 06 |
| Demanding or difficult case | 06 |
| Boredom | 05 |
| Nature of activity related | 05 |
| Insufficient preparation | 03 |
| Slow procedure | 03 |
| Others | 03 |
| Total | 481 |
Various other factors exist in operating rooms giving rise to a high incidence of medication errors during the conduction of anaesthesia. Lack of staff, overtime and odd working hours, inattention, poor communication, carelessness, haste and fatigue are the common factors related to medical and paramedical personnel.[8,19,27–29] Look-alike, sound-alike drugs,[30,31] confusing, inaccurate or incomplete drug labels and packaging,[31] swapping of syringe labels,[9,32] swapping of syringes and ampoules,[33] unlabelled syringe,[34] and failure of drug dose calculation,[5] have been reported in the literature from time to time.
In critical care, apart from those mentioned above, some other factors also exist which complicate the matter further. Severity of illness,[35] lack of usual medication list,[36] need of sedation and artificial ventilation,[37] calculation and programming of infusion pumps,[38] inexperience, lack of drug knowledge, sleep deprivation of provider,[11,39,40] high stress and fast pace of medication[10] and frequent changes in drugs and doses[41] have been listed by different authors.
DRUGS INVOLVED IN MEDICATION ERRORS
Various group of drugs involved in medication errors during practice of anaesthesia have been reported by different authors. Induction agents like pentothal sodium, ketamine, depolarizing and non-depolarizing muscle relaxants, narcotic and sedatives, anticholinergics, and local anaesthetics have been given wrongly either due to misidentification, wrong labelling, syringe swap, or exchange with another drugs because of inattention or haste. However, in majority of the cases these errors did not result in any serious harm to the patients.[5,9,42]
In critical care units, the involvement of inotropes, narcotics, sedatives, analgesics, potassium chloride, magnesium sulphate, and anticoagulants like heparin or anti-infective agents have been identified in different studies.[12,13,43,44]
CONSEQUENCES OF MEDICATION ERRORS
There is an increasing recognition that medication errors are causing a substantial global problem as many results in harm to patients and increased cost to health care providers, and anaesthesia and critical care are no exception to this.[45]
Medical errors are the leading cause of death in USA. A total of 44000 - 98000 Americans die every year. IOM has estimated that each year medical errors injured at least 1.5 million Americans and cost the health system more than 3.5 billion U.S. dollars. In another study approximately 7000 deaths in USA have cost more than 2 billion dollars.[3]
Medical errors erode not only a patient’s but also a family’s confidence in health care organisations, public confidence also suffers due to these errors.[46] The memory of errors can haunt the provider for years.[47] Anaesthesiologists have been charged for manslaughter, homicide, etc.[7,30,48]
PREVENTION OF MEDICATION ERRORS IN ANAESTHESIA AND CRITICAL CARE
Very often anaesthesia professionals have been compared with commercial pilots because both face a high incidence of accidents either in take-off (induction of anaesthesia) and landing (emergence from anaesthesia) but this is not always true. Working in an operating room is much more complex than being in a commercial aviation set-up.[49] The aviation industry has adopted a definitive safety culture whereas anaesthesia professionals have a attitudinal barrier to safety. Both accidents and incidents in the aviation industry are taken as an opportunity to redesign the faulty system hence having a well developed feed-back and information system whereas an accident during the period of anaesthesia is often not reported due to fear of being blamed for carelessness, forgetfulness and sometimes character weakness.[50]
Most often, the number of people involved in single airline accident is much higher than that related to anaesthesia, hence airline accidents grab quick attention and response. Although deaths due to anaesthesia errors are much higher in number but they are sporadic, spread over a large span of time and invisible; therefore, they do not get immediate attention.[51]
Anaesthesiologists are one of the few groups of physicians who are personally responsible for drug administration. During anaesthesia most drug errors are totally or partially attributed to human error which is an inherent part of human psychology and activity; hence the occurrence of error can only be reduced and not eliminated.[52,53]
In general, following things should be kept in mind while working in the operation room to minimise the incidence of medication errors:
Reducing the complexity of the system to simple and linear to enhance the safety.[15,54]
Redundancy and standardisation are the basic principles in the design of a safe system.[15,54]
Double checking of ampoules, syringes and equipment before starting the procedure.[9]
Simple vigilance during the handling and administration of drugs is of utmost importance.
After a systemic review, Jenson and colleagues[55] recommended a 12-point strategy to prevent medication errors during anaesthesia and critical care:
The label on any drug ampoule or syringe should be read carefully before the drug is drawn up or injected.
Legibility and contents of labels on ampoules and syringes should be optimized according to agreed standards with respect to font, size, colour and information.
Syringes should always be labelled.
Formal organisation of drug drawers and work space should be used with attention to tidiness, position of ampoules and syringes, separation of look-alike drugs and removal of dangerous drugs from the operation room.
Labels should be checked specifically with the help of a second person or a device like bar code reader before administration.
Error during administration should be reported and reviewed.
Management of inventory should focus on minimising the risk of drug error.
Look-alike packaging and presentation of the drug should be avoided where possible.
Drug should be presented in prefilled syringes rather than ampoules.
Drug should be drawn up and labelled by the anaesthesia provider himself/herself.
Colour coding by class of drugs should be according to an agreed national or international standard.
Coding of syringe according to position or size should be done.
Several other measures to promote safe drug administration during anaesthesia and critical care have been suggested:-[33,56–58]
The provision of all labels in a standardised format emphasising the class and generic name of each drug incorporating the bar code and class-specific colour code as per international standard.
The use of a bar code reader to scan the drug at the point of administration immediately before it is given linked to an auditory prompt to facilitate checking of the drug identity.
Integration of scanned information into an automated anaesthesia record and reducing the cognitive load on the anaesthetist.
The use of devices at the point of care to automatically measure the dose of the administered drug.
A dosing nomograph on the infusion syringe label to avoid the need of look-up tables or dose calculations.
The automated medication dispensing system with features such as single issue drawers and bar code scanners to facilitate safer dispensing of drugs.
Camire et al[14] in a review article have suggested seven strategies to prevent errors in ICU. These are as follows:
Eliminating extended physician work schedules.
Computerised physician order entry.
Implement support system for clinical decisions.
Computerised intravenous devices.
Active participation of pharmacists in ICU.
Medication reconciliation.
Merali et al[59] made several recommendations to reduce medication errors at different stages of the system [Table 3].
Table 3.
Recommendations to reduce medication errors[59]
| Patient information | • Consistent documentation and complete operative medication history |
| • Add prompts to pre admission card | |
| Drug information | • Provide enhanced pharmacist support |
| Communication of drug orders and information | • Eliminate use of dangerous abbreviations and dose expressions |
| • Incorporate computerised physician order entry into strategic planning | |
| Drug labelling, packaging and nomenclature | • Enhance communication mechanism |
| • Standardised anaesthetic cart trays and consider usage pattern | |
| • Labelling of all medication and solutions | |
| • Standardise labelling procedures | |
| Drug standardisation, storage and distribution | • Evaluate the need and then clearly identify and segregate hazardous products |
| • Increased provision of premixed solutions | |
| • Segregate and label, storage areas for neuromuscular blockers | |
| • Acquisition of prefilled automated dispensing cabinet | |
| • Incorporate bar coding system | |
| Environment and workflow | • Minimize advance preparation of drug syringe |
| • Return or remove unused medication from work cart | |
| Staff competency and education | • Investigate, evaluate and educate staff about the dangers associated with workaround practices |
| Patient education | • Provide enhanced education material for preoperative patients |
| • Consider pharmacy involvement in same day assessment | |
| Quality processes and risk management | • Encourage reporting (including nearmisses) by all practitioners |
| • Consider monitoring use of all trigger drugs | |
| • Consistently employ independent double checks for hospital selected ‘“high alert”’ drugs |
Many organisations are now dedicated to patient safety, including IOM, Institute for Safe Medical Practice (ISMP), Emergency Care Research Institute (ECRI), Joint Commission for Food and Drug Administration (FDA), Centre for Medicated and Medicare Services (CMS), National Patient Safety Foundation (NPSF), United States Pharmacopeia (USP), Agency for Healthcare Research and Quality, National Quality Forum and many more.[60]
CONCLUSION
Despite the best efforts, the increased use of technology and high standards of both invasive and non-invasive monitoring in anaesthesia and critical care, medication errors continue to occur even at the best centres worldwide. Simple vigilance, standardised protocol, and ‘think before act’ are the key factors to avoid occurrence of medication errors.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Schneider PJ, Gift MG, Lee YP, Rothermich EA, Sill BE. Cost of medication-related problems at a university hospital. Am J Health Syst Pharm. 1995;52:2415–8. doi: 10.1093/ajhp/52.21.2415. [DOI] [PubMed] [Google Scholar]
- 2.Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, et al. The nature of adverse events in hospitalized patients results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324:377–84. doi: 10.1056/NEJM199102073240605. [DOI] [PubMed] [Google Scholar]
- 3.Kohn LT, Corrigan JM, Donaldson M. Washington DC: National Academy Press; 1999. To err is human: Building a safer health system. [PubMed] [Google Scholar]
- 4.Stelfox HT, Palmisani S, Scurlock C, Orav EJ, Bates DW. The “To Err is Human” report and the patient safety literature. Qual Saf Health Care. 2006;15:1748. doi: 10.1136/qshc.2006.017947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Orser BA, Chen RJ, Yee DA. Medication errors in anaesthetic practice, a survey of 687 practitioners. Can J Anesth. 2001;48:139–46. doi: 10.1007/BF03019726. [DOI] [PubMed] [Google Scholar]
- 6.Yamamoto M, Ishikawa S, Makita K. Medication errors in anesthesia: An 8-years retrospective-analysis at an urban university hospital. J Anesth. 2008;22:248–52. doi: 10.1007/s00540-008-0624-4. [DOI] [PubMed] [Google Scholar]
- 7.Merry AF, Peck DJ. Anaesthetists, errors in drug administration and the law. N Z Med J. 1995;108:185–7. [PubMed] [Google Scholar]
- 8.Currie M, Mackay P, Morgan C, Runciman WB, Russell WJ. The Australian Incident monitoring study. The “Wrong drug” problem in anaesthesia: An analysis of 2000 incident reports. Anaesth Intensive Care. 1993;21:596–601. doi: 10.1177/0310057X9302100517. [DOI] [PubMed] [Google Scholar]
- 9.Fasting S, Gisvold SE. Adverse drug errors in anaesthesia, and the impact of coloured syringe labels. Can J Anesth. 2000;47:1060–7. doi: 10.1007/BF03027956. [DOI] [PubMed] [Google Scholar]
- 10.Kane Gill S, Weber RJ. Principles and practices of medication safety in the ICU. Crit Care Clin. 2006;22:273–90. doi: 10.1016/j.ccc.2006.02.005. [DOI] [PubMed] [Google Scholar]
- 11.Donchin Y, Gopher D, Olin M, Badihi Y, Biesky M, Sprung CL, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med. 1995;23:294–300. doi: 10.1097/00003246-199502000-00015. [DOI] [PubMed] [Google Scholar]
- 12.Calabrese AD, Erstad BL, Brandl K, Barletta JF, Kane SL, Sherman DS. Medication administration errors in adult patient in the ICU. Intensive Care Med. 2001;27:1592–8. doi: 10.1007/s001340101065. [DOI] [PubMed] [Google Scholar]
- 13.Rothschild JM, Landrigan CP, Cronin JW, Kaushal R, Lockley SW, Burdick E, et al. The critical care safety study: The incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med. 2005;33:1694–700. doi: 10.1097/01.ccm.0000171609.91035.bd. [DOI] [PubMed] [Google Scholar]
- 14.Camire E, Moyen E, Stelfox HT. Medication errors in critical care: Risk factors, prevention and disclosure. CMAJ. 2009;180:936–43. doi: 10.1503/cmaj.080869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Reason J. New York: Cambridge University Press; 1990. Human error. [Google Scholar]
- 16.Moyen E, Camire E, Stelfox HT. Clinical review: Medication errors in critical care. Crit Care. 2008;12:208. doi: 10.1186/cc6813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pronovost PJ, Thompson DA, Holzmueller CG, Lubomski LH, Morlock LL. Defining and measuring patient safety. Crit Care Clin. 2005;21:1–19. doi: 10.1016/j.ccc.2004.07.006. [DOI] [PubMed] [Google Scholar]
- 18.NCC MERP index categorizing medication error. Available from http://www.nccmerp.org/pdf [last cited on 2010 Jan 25] [Google Scholar]
- 19.Cooper JB, Newbower RS, Long CD, McPeek B. Preventable anaesthesia mishaps: A study of human factors. Anesthesiology. 1978;49:399–406. doi: 10.1097/00000542-197812000-00004. [DOI] [PubMed] [Google Scholar]
- 20.Pharmacy-nursing shared vision for safe medication use in hospitals: Executive summary session. Am J Health Syst Pharm. 2003;60:1046–52. doi: 10.1093/ajhp/60.10.1046. [DOI] [PubMed] [Google Scholar]
- 21.Krahenbuhl MA, Schlienger R, Lampert M, Haschke M, Drewe J, Krahenbuhl S. Drug related problems in hospitals: A review of the recent literature. Drug Saf. 2007;30:379–407. doi: 10.2165/00002018-200730050-00003. [DOI] [PubMed] [Google Scholar]
- 22.Dripps RD, Lamont A, Eckenhoff JE. The role of anaesthesia in surgical mortality. JAMA. 1961;178:261–6. doi: 10.1001/jama.1961.03040420001001. [DOI] [PubMed] [Google Scholar]
- 23.Clifton BS, Hotten W. Deaths associated with anaesthesia. Br J Anaesth. 1963;35:200–59. doi: 10.1093/bja/35.4.250. [DOI] [PubMed] [Google Scholar]
- 24.Edwards G, Morton HJ, Pask EA, Wylie WD. Deaths associated with anaesthesia, report of 1000 cases. Anaesthesia. 1956;11:194–220. doi: 10.1111/j.1365-2044.1956.tb07975.x. [DOI] [PubMed] [Google Scholar]
- 25.Howell S, Driver RP., Jr Unintentional intracerebroventicular administration of etomidate and rocuronium. Anesth Analg. 2008;106:520–2. doi: 10.1213/ane.0b013e3181606ae5. [DOI] [PubMed] [Google Scholar]
- 26.Cooper L, DiGiovanni N, Schultz L, Taylor RN, Nossaman B. Human factors contributing to medication errors in anaesthesia practice. ASA. 2009:A614. [Google Scholar]
- 27.Abeyasekhra A, Bergman IJ, Kluger MT, Short TG. Drug error in anaesthesia practice: A review of 896 reports from the Australian incident monitoring study database. Anaesthesia. 2005;6:220–7. doi: 10.1111/j.1365-2044.2005.04123.x. [DOI] [PubMed] [Google Scholar]
- 28.Merry AF, Webster CS, Mathew DJ. A new, safety oriented, integrated drug administration and automated anaesthesia record system. Anesth Analg. 2001;93:385–90. doi: 10.1097/00000539-200108000-00030. [DOI] [PubMed] [Google Scholar]
- 29.Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failure in anaesthesia management. Considerations for prevention and detection. Anaesthesiology. 1984;60:34–42. doi: 10.1097/00000542-198401000-00008. [DOI] [PubMed] [Google Scholar]
- 30.Orser B. Reducing medication error. CMAJ. 2000;162:1150–1. [PMC free article] [PubMed] [Google Scholar]
- 31.Skegg PD. Criminal prosecutions of negligent health professionals the New Zealand experience. Med Law Rev. 1998;6:220–46. [Google Scholar]
- 32.Perri M, Morris S. Critical incident involving syringe labels. Anaesthesia. 2007;62:95–6. doi: 10.1111/j.1365-2044.2006.04924_1.x. [DOI] [PubMed] [Google Scholar]
- 33.Sakaguchi Y, Tokuda K, Yamaguchi K, Irita K. Incidence of anaesthesia-related medication errors over a 15-year period in a university hospital. Fukuoka Igaku Zasshi. 2008;99:58–66. [PubMed] [Google Scholar]
- 34.Stabile M, Webster CS, Merry AF. Medication administration in anaesthesia. Time for a paradigm shift. APSF Newsletter. 2007;22:44–7. [Google Scholar]
- 35.Valentine A, Capuzzo M, Guidet B, Moreno RP, Dolanski L, Bave P, et al. Patient safety in intensive care: Results from the multinational Sentinel Events Evaluation (SEE) study. Intensive Care Med. 2006;32:1591–8. doi: 10.1007/s00134-006-0290-7. [DOI] [PubMed] [Google Scholar]
- 36.Pronovost PJ, Weast B, Schwarz M, Wyskiel RM, Prow D, Milanovich SN, et al. Medication reconsciliation: A practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201–5. doi: 10.1016/j.jcrc.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 37.Hussain E, Kao E. Medication safety and transfusion errors in ICU and beyond. Crit Care Clin. 2005;21:91–110. doi: 10.1016/j.ccc.2004.08.003. [DOI] [PubMed] [Google Scholar]
- 38.Williams CK, Maddox RR. Implementation of an I.V. medication safety system. Am J Health Syst Pharm. 2005;62:530–6. doi: 10.1093/ajhp/62.5.530. [DOI] [PubMed] [Google Scholar]
- 39.Leape LL, Bates DW, Cullen DJ, Cooper J, Demonaco HJ, Gallivan T, et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA. 1995;274:35–43. [PubMed] [Google Scholar]
- 40.Gaba DM, Howard SK. Patient safety: Fatigue among clinicians and the safety of the patients. N Engl J Med. 2002;347:1249–55. doi: 10.1056/NEJMsa020846. [DOI] [PubMed] [Google Scholar]
- 41.Weingart SN, Wilson RM, Gibberd RW, Harrison B. Epidemiology of medical error. BMJ. 2000;320:774–7. doi: 10.1136/bmj.320.7237.774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bowdle TA. Drug administration errors from the ASA closed claims project. ASA Newsl. 2003;67:113. [Google Scholar]
- 43.Ridley SA, Booth SA, Thompson CM, Clayton T, Eddleston J, Mackenzie S, et al. Prescription errors in UK critical care units. Anaesthesia. 2004;59:1193–200. doi: 10.1111/j.1365-2044.2004.03969.x. [DOI] [PubMed] [Google Scholar]
- 44.Calabrase AD, Erstad BL, Brandl K, Barletta JF, Kana SL, Sherna DS. Medication administration errors in adult patients in ICU. Intensive Care Med. 2001;27:1592–8. doi: 10.1007/s001340101065. [DOI] [PubMed] [Google Scholar]
- 45.Wheeler SJ, Wheeler DW. Medication error in anaesthesia and critical care. Anaesthesia. 2005;60:257–73. doi: 10.1111/j.1365-2044.2004.04062.x. [DOI] [PubMed] [Google Scholar]
- 46.Cohen H, Mandrack MM. Application of the 80/20 rule in the safeguarding the use of high alert medications. Crit Care Nurs Clin North Am. 2002;14:369–74. doi: 10.1016/s0899-5885(02)00018-7. [DOI] [PubMed] [Google Scholar]
- 47.Christensen JF, Levinson W, Dunn PM. The heart of darkness: The impact of perceived mistakes on physicians. J Gen Intern Med. 1992;7:424–31. doi: 10.1007/BF02599161. [DOI] [PubMed] [Google Scholar]
- 48.Recommendation of coroner’s jury from the inquest into the death of Trevor Laundry, Jan 4- Feb 17,(Mississauga, Ont) 1999 [Google Scholar]
- 49.Gaba DM, Singer SJ, Sinaiko AD, Bowen JD, Ciavarelli AP. Differences in safety climate between hospital personnel and naval aviators. Hum Factors. 2003;45:173–85. doi: 10.1518/hfes.45.2.175.27238. [DOI] [PubMed] [Google Scholar]
- 50.Webster CS. The iatrogenic-harm cost equation and new technology. Anaesthesia. 2005;60:843–6. doi: 10.1111/j.1365-2044.2005.04331.x. [DOI] [PubMed] [Google Scholar]
- 51.Preventing and Managing the impact of anaesthesia awareness. Issue 2 October 6, 2004, Sentinel Event Alert, The Joint Commission. Available from: http://www.jointcommission.org/ [Last cited on 2010 Jan 25] [PubMed]
- 52.Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events nd potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA. 1995;274:29–34. [PubMed] [Google Scholar]
- 53.Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10:199–205. doi: 10.1007/BF02600255. [DOI] [PubMed] [Google Scholar]
- 54.Reason J. England: Ashgate Publishing Limited; 1997. Managing the risks of organizational accidents. [Google Scholar]
- 55.Jenson LS, Merry AF, Webster CS, Weller J, Larson L. Evidence based strategies for preventing drug administration errors during anaesthesia. Anaesthesia. 2004;59:493–504. doi: 10.1111/j.1365-2044.2004.03670.x. [DOI] [PubMed] [Google Scholar]
- 56.DocuSys: Digital Medical Solutions. Available from: http://www.docusys.net/ [Last cited on 2010 Jan 25] [Google Scholar]
- 57.Merry AF, Webster CS, Connell H. A new infusion syringe label system designed to reduce task complexity during drug preparation. Anaesthesia. 2006;62:486–91. doi: 10.1111/j.1365-2044.2007.04993.x. [DOI] [PubMed] [Google Scholar]
- 58.Merry AF, Webster CS, Larsson L, Weller J, Frampton CM. Prospective assessment of a new anaesthetic drug administration system designed to improve safety. Anesthesiology. 2006;105:A 138. [Google Scholar]
- 59.Merali R, Orser BA, Leeksma A, Lingard S, Belo S, Hyland S. Medication safety in the operating room: Teaming up to improve patient safety. Healthc Q. 2008;11:54–7. doi: 10.12927/hcq.2008.19650. [DOI] [PubMed] [Google Scholar]
- 60.Martin DE. Medication error persist: Summit addresses intravenous safety. APSF Newsletter. 2008;23:37–9. [Google Scholar]