

Abstract
Data from 18,437 children enrolled in the national evaluation of the Children's Mental Health Initiative between 1994 and 2005 were used to examine the evolution of patterns of risk among boys and girls across funding phases using multi-group latent class analysis. Consistent with previous research, this study identified four sub-groups of children with similar patterns of child risk. Membership to these risk sub-groups varied as a function of age and was associated with differences in impairment levels. Changes in the distribution of boys and girls in the risk classes suggest that, over time, an increasing proportion of boys have entered the system of care program with complex histories of risk. Information on children's exposure to child risk factors can aid policy makers, service providers and clinicians in identifying children who may need more intensive services and tailoring services to their needs.
While a variety of service delivery approaches exist to meet the needs of children with mental health challenges, systems of care is one of the prevailing approaches. Rooted in the Child and Adolescent Service System Program (CASSP) and federally supported by the Substance Abuse and Mental Health Services Administration (SAMHSA) through the Children's Mental Health Initiative, the system of care approach recognizes the complexity of need for children with serious emotional disturbance and advocates for an interagency, community-based, culturally appropriate, child-centered framework around the provision of treatment and delivery of services.1 Funded from 1993 to present, the CMHI stands as the nation's largest and longest continually funded children's mental health services demonstration program and has served over 89,000 children across the United States, its territories, and tribal areas.
In parallel with the continual funding of the CMHI has been funding its national evaluation, which has resulted in a wealth of data gathered about the children served through the CMHI.2, 3 Given the longevity and reach of the CMHI and the implication that it will continue to be a dominant influence in children's mental health service delivery, developing a better understanding of gender differences as a function of psychosocial history, clinical indicators, and pathways to service among those who enter systems of care has become of increasing importance in data driven program and policy decision making.
Gender differences have been documented along a temporal spectrum from risk exposure to clinical indicators, throughout entry into and receipt of services. For example, boys and girls respond differently to certain risks and traumatic events. Boys who have been sexually abused or assaulted4 have higher symptoms of depression than girls, while girls who have problems with their friends and siblings have higher symptoms of depression than boys.5 Boys who have been physically assaulted or witness inter-parental violence are also at greater risk for antisocial behavior4 and oppositional defiant disorder5 than girls exposed to those types of violence.
In addition to differences in responses to risk exposure, there are gender differences in whether and how children enter into mental health services. Overall, girls are less likely to receive any mental health services,6 especially for behavioral problems, than boys; 7 however, when they do enter services they are more likely to enter from child welfare and the court system.8
Once children enter mental health treatment, gender differences continue. Boys are more likely than girls to receive school based services9, 10 and specialty outpatient services.10, 11 Boys are also more likely to be placed in residential treatment centers;8 however, girls tend to have longer stays.12, 13 Among children served in residential treatment centers, girls are more likely to have drug and alcohol use, eating disorders, depression, a history of running away, self-injury, and sexual abuse.12 Boys are more likely to have school problems, aggressive behavior, ADHD, and a history of vandalism, theft, arson, and weapons violations.12
Adding to the growing literature on gender differences among children entering community-based mental health treatment, and directly relevant to the current investigation, a prior study used latent class analysis to identify four risk classes (low-risk, status-offense, abuse, and high-risk) for boys and girls entering into the CMHI between 1994 and 1999.14 While there were some similarities in the patterns of risk, the distribution of boys and girls in the risk classes varied. For example, there were far fewer girls than boys in the low-risk class, roughly equivalent numbers in the status-offense class, and far more girls in both the abuse and high-risk classes.14 Furthermore, this study indicated that both boys and girls in the high-risk class exhibited the highest level of functional impairment, followed by those in the status-offense class, the abuse class, and finally the low-risk class; the overall level of impairment was lower for girls as compared to boys.
While the treatment and service planning implications associated with these findings were articulated in the previous related study, it has not been possible until now to investigate these gender relationships across extended years of the CMHI. Increased knowledge of any differences will inform future program and policy direction and contribute to federal data driven decision making, quality monitoring, and efforts toward ensuring that programs are developed and tailored to provide service access to populations in need. To that end, this paper aims to: 1) extend – through a multi-group latent class analysis framework15, 16 – previous research and examine the risk characteristics of boys and girls entering mental health systems of care, and 2) determine whether those characteristics changed (or remained constant) across funding phases of the CMHI. Specifically, this paper addresses the following questions:
Have the nature of risk patterns, the relative prevalence of each risk pattern, or both remained constant (or changed) across funding phases for boys and girls?
What is the relationship between risk patterns and age for both boys and girls; and to what extent has this relationship remained constant (or changed) across funding phases?
What is the relationship between risk patterns and impairment for both boys and girls; and to what extent has this relationship remained constant (or changed) across funding phases?
Method
Data Source
The data for this study derives from information collected on children with serious emotional disturbance at intake into service as part of the national evaluation of the Children's Mental Health Initiative from 63 communities across the United States initially funded between 1993 and 2000. These funding years encompass three funding phases of the national evaluation and corresponding evaluation protocols. Phase I communities were initially funded in 1993 and 1994, Phase II communities in 1997 and 1998, and Phase III communities in 1999 and 2000. After the initial year of funding, communities typically enrolled children for 6 years. As a consequence, information encompasses children entering into service between 1994 and 2005. All of these communities completed their federal funding cycles and hence the data represent the final samples in these communities.
As part of the CMHI national evaluation, grantees were asked to provide descriptive information on all children entering service. A subset of children and families were recruited for the longitudinal outcome study. The national evaluation team recommended enrolling approximately 100 children per year, for three years, into the study. In most communities all willing families were recruited; however, communities serving larger populations could develop sampling strategies to select a sufficient number of participants. Severity of functional impairment or clinical symptoms was not used as a criterion for outcome study enrollment. The current study uses measures which were collected from all children enrolled in services in Phase I, but due to a change in study protocol these measures were included in the longitudinal study in Phases II-III (and thus collected only on the children and families who participated in the longitudinal study).
Sample Selection
Children served by the CMHI had to meet the criteria for serious emotional disturbance, which typically required that a child had a diagnosable DSM–IV disorder, exhibited functional impairments, and was in or at risk for out-of-home placement. The program targeted children with serious emotional disturbance ages birth to 22 years. Children were included in the current sample (N= 18,437) if they were between 5 and 22 years old and had data on gender, referral source, race/ethnicity and the six child risk factors described below.
Table 1 describes the characteristics of the sample. Overall, average age was 12.2 years; children from Phase I were somewhat younger than children from Phases II and III, and boys were younger than girls in all phases. More than half of the children were Caucasian, nearly one fourth were African American, and a tenth had Hispanic origin. The racial/ethnic composition remains fairly similar between Phases I and II; in Phase III, however, both African American children and children from other race/ethnicities increased. Children were referred into the system of care from mental health agencies, school systems, juvenile justice, child welfare, and family and self-referrals. Source of referral changed noticeably in Phase III; children referred from mental health agencies shifted from nearly 25% to almost 50% of the sample.
Table 1. Study sample characteristics.
| Phase I | Phase II | Phase III | ||||
|---|---|---|---|---|---|---|
| Boys (n=4,507) |
Girls (n=2,279) |
Boys (n=4,291) |
Girls (n=2,100) |
Boys (n=3,488) |
Girls (n=1,772) |
|
| Age | ||||||
| Mean | 11.4 | 12.2 | 12.4 | 12.9 | 12.0 | 12.9 |
| SD | 3.5 | 3.4 | 3.4 | 3.1 | 3.3 | 3.3 |
| Race/ethnicity | ||||||
| Caucasian | 55.2% | 57.1% | 55.9% | 57.2% | 46.0% | 45.2% |
| African American | 21.7% | 21.9% | 22.4% | 19.9% | 30.8% | 26.4% |
| Hispanic | 13.2% | 11.1% | 12.0% | 11.0% | 9.1% | 8.5% |
| Other | 9.9% | 9.9% | 9.6% | 11.9% | 14.1% | 19.9% |
| Referral source | ||||||
| Mental health | 24.2% | 25.0% | 23.1% | 24.0% | 43.3% | 45.7% |
| Education | 22.9% | 15.5% | 23.0% | 17.9% | 17.3% | 12.0% |
| Family | 15.9% | 19.0% | 9.9% | 10.8% | 11.1% | 13.3% |
| Child welfare | 11.7% | 17.0% | 9.5% | 16.8% | 8.8% | 10.8% |
| Juvenile justice | 14.0% | 9.3% | 22.2% | 19.3% | 12.0% | 9.8% |
| Other | 11.4% | 14.1% | 12.3% | 11.4% | 7.6% | 8.4% |
| Risk factors | ||||||
| Physically abused | 25.4% | 29.8% | 23.9% | 29.3% | 22.3% | 26.5% |
| Sexually abused | 13.8% | 34.4% | 13.8% | 35.0% | 14.6% | 32.1% |
| Runaway | 19.1% | 29.0% | 29.2% | 42.7% | 25.2% | 34.1% |
| Suicide attempt | 10.9% | 20.5% | 11.1% | 22.0% | 11.4% | 21.0% |
| Drug use/alcohol | 18.5% | 21.2% | 22.8% | 26.4% | 15.2% | 19.8% |
| Sexually abusive | 7.0% | 5.3% | 8.0% | 5.3% | 8.2% | 4.9% |
| CAFAS | ||||||
| Mean | 88.2 | 80.1 | 106.3 | 106.8 | 116.1 | 112.1 |
| SD | 43.4 | 44.2 | 43.6 | 49.2 | 48.0 | 49.6 |
| Missing | 24.7% | 20.7% | 51.7% | 49.9% | 49.6% | 56.7% |
Measures and indicators
Demographic information
Child age (years), gender, race/ethnicity and referral source were collected from caregivers at the time of the child's intake into services. In this study, race/ethnicity was categorized as Caucasian, African American, Hispanic, and Other.
Risk Factors
History of physical or sexual abuse, substance abuse, running away from home, suicide attempt, and sexually abusing another individual were obtained from caregivers at the time of intake. The prevalence of the risk factors is shown in Table 1. Across the phases, sexually abusing others was more prevalent among boys, whereas all the other risk factors were more prevalent among girls.
Functional impairment
Functional impairment was assessed using the Child and Adolescent Functional Assessment Scale (CAFAS), which rates functional impairment across 8 life domains: home role performance, community role performance, school role performance, behavior towards others, mood and emotions, self-harmful behavior, substance use or abuse, and thinking.17 Trained clinicians or interviewers, who had been established as reliable raters, completed the CAFAS using all available information (e.g. agency case records, intake assessment information, interviews with the caregiver, etc.) on the child to rate level of impairment. The total CAFAS score ranges from 0 to 240, with a higher score indicating greater impairment. Acceptable reliability and validity of the CAFAS has been documented and the scale has demonstrated good inter-rater reliability with a variety of raters, including mental health intake workers, direct service providers, paraprofessionals, and graduate students.18-21
Due to a change in the evaluation protocol, missing CAFAS data increases substantially between Phase I and Phases II and III. In Phase I, CAFAS information was collected from all children entering the CMHI. Beginning in Phase II, CAFAS information was only collected among the children who participated in the longitudinal study. Average impairment increases across phases, especially between Phase I and Phase II (Table 1). Average impairment scores are somewhat higher among boys than among girls in Phases I and III, and similar for boys and girls in Phase II.
Analysis
A multi-group latent class framework15, 16 was used to extend previous research14 and examine risk classes among boys and girls entering the CMHI across three funding phases. Multi-group LCA can be used to compare latent class characteristics across groups. In this study there are the six gender-by-funding phase groups. A completely unrestricted multi-group LC model is equivalent to the estimation of a separate model for each group, with the same number of classes.
The same 4-class solution proposed in the original CMHI study14 was compared to 3- and 5-class models. A single class model (i.e., a model of independence among risk factors) was used as a reference model. Overall measures of model fit were obtained, e.g., the likelihood ratio chi-square can be obtained by summing the values of each separate group model. Fit statistics used in the current study include the Akaike's information criterion (AIC), Bayesian information criterion (BIC), and the likelihood ratio chi-square (L2) test. Lower AIC and BIC values suggest better fit. There is not always agreement among the various fit statistics as to the best fitting model. In this study, greater importance was given to parsimoniousness, which is better captured by the BIC. The equivalence of the measurement portion of the model (i.e., the probabilities of endorsing each risk factor by class) between girls and boys and across phases within gender was tested by applying appropriate constraints and testing the difference in L2.
To test the association between age and latent class membership for boys and girls, across phases, the model was refitted to include age as a predictor of class membership. For each group, the log odds of belonging to one class compared with a base class (i.e., a class chosen arbitrarily to allow the comparison) was modeled as a linear function of age.
To test the association between functional impairment and latent class membership, mean total impairment scores and variances were estimated for each class and group. A Wald test was used to evaluate equivalence of means and variances across classes. As mentioned earlier, there was an increase in missingness on functional impairment across funding phases. Parameters were estimated using maximum likelihood under the ‘missing at random’ assumption. All analyses were performed using Mplus Version 5.22
Results
Latent Class Model Selection
Table 2 presents the fit statistics from the multi-group latent class analysis. Latent class models with 1 (H0), 3 (H3C), 4 (H4C) and 5 (H5C) classes were fitted simultaneously to the six groups (i.e., Phase I boys, Phase I girls, Phase II boys, Phase II girls, Phase III boys, Phase III girls).a The 5-class model should be interpreted cautiously since it was not possible to rule out a local maxima solution. b The fit statistics suggest that either a 4- or 5-class model best fits the data for both boys and girls, across phases. The L2 and AIC suggest that the 4-class model falls somewhat short of providing an adequate fit; however, the BIC, suggests that the 4-class model best fits the data. The percent reduction in the L2, when compared with the single class model, shows that almost all of the original association among the risk factors is explained in the 4-class model.
Table 2. Latent Class Models of Child Risk Factors: Model Fit.
| Model | AIC | BIC | L2 | DF | P | % Reduction in L2 (H0) |
|---|---|---|---|---|---|---|
| H0 | 166503.4 | 166824.1 | 7669.6 | 342 | 0.0000 | |
| H3C | 159770.7 | 160748.5 | 769.0 | 258 | 0.0000 | 90% |
| H4C | 159349.5 | 160655.8 | 263.7 | 216 | 0.0147 | 97% |
| H5C | 159347.9 | 160982.7 | 178.2 | 174 | 0.3988 | 98% |
AIC is the Akaike's information criterion and BIC stands for Bayesian information criterion.
Latent Class Analysis for Boys and Girls
Figure 1 shows the fitted probabilities of reporting each risk factor by class and the estimated probability of class membership, separately for each gender and phase. Based on the probability of endorsing each risk factor, the classes can be characterized as high-risk, abuse, status-offense, and low-risk classes for both boys and girls.
Figure 1. Four-class conditional probabilities of child risk factors by gender and phase.
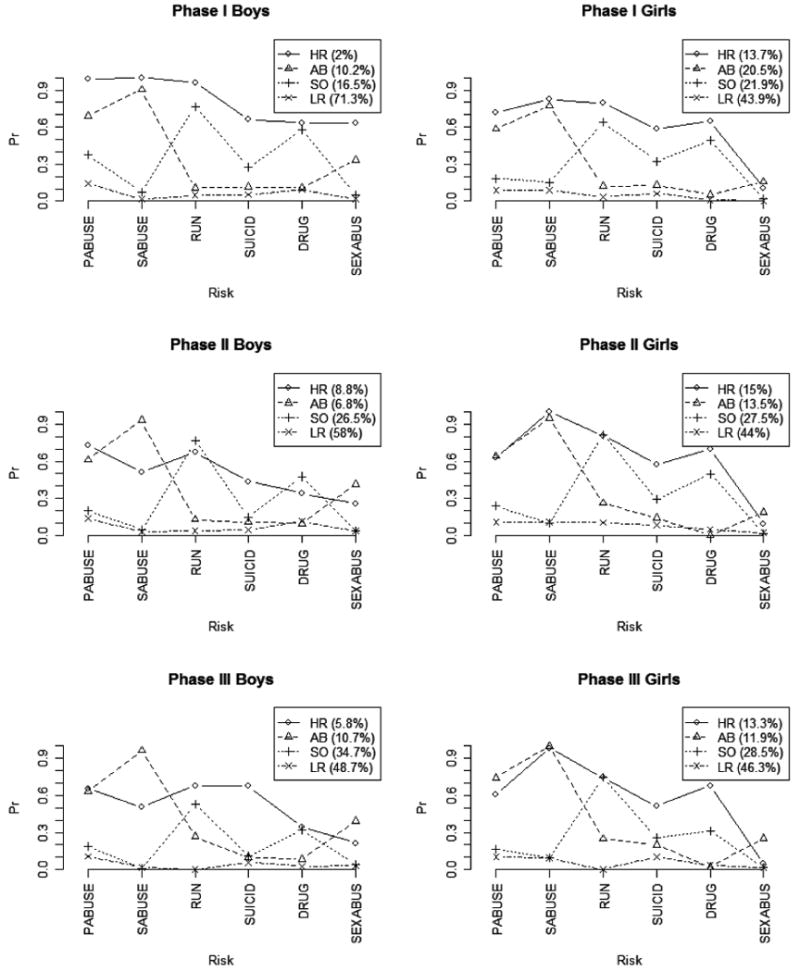
HR= high-risk, AB= abuse, SO= status-offense, and LR= low-risk. PABUSSE=physically abused, SABUSE= sexually abused, RUN= runaway from home, SUICIDE=suicide attempt, DRUGS= substance use and SEXABUS= sexually abusive.
Boys
The high-risk class includes boys who were most likely to endorse most of the child risk factors. In particular, the probability of physical abuse and running away were greater than 50% in each phase (ranges from 65.4%-98.8% and 67.1%-95.8%, respectively), and the probability of attempting suicide (43.7%-67.5%) was greater than in any other class. Membership into this class ranges from 2%-5.8% across the three phases. The abuse class reflects boys who were likely to endorse sexual abuse (90.4-96.3), physical abuse (61.2%-68.9%) and, to some extent, sexually abusing others (33.5%-41.5%), but less likely to endorse the other risk factors. Class membership ranges from 6.8%-10.7%. The status-offense class reflects boys who had high probabilities of reporting running away (52.8%-76.5%) and, to a lesser extent, substance abuse (32%-57.7%) and lower probabilities of reporting the other risk factors. The low-risk class, which the majority of boys belonged to, reflects boys who were unlikely to endorse any of the child risk factors.
While the four classes just described were identified across each of the funding phases, there were significant differences among item endorsement between phases; the change in the fit chi-square when item endorsement probabilities were constrained to be the same across phases is 186.2 for boys and 92.5 for girls, both with 48 df. Among boys in the high-risk class the conditional probabilities for physical abuse, sexual abuse, and running away decreased from very high in Phase I to moderately high in Phase III.
Girls
A 4-class model for girls was also identified (Figure 1). The high-risk class encompassed girls who were the most likely to report all of the risk factors (with a probability greater than 50% across phases) with the exception of sexually abusive to others. A larger proportion of girls belonged to the high-risk group compared to the proportion of boys in the high-risk group (e.g., 13.7% vs 2% in Phase I); however, this difference decreased across funding phase (e.g. 13.3% vs. 5.8% in Phase III). The abuse class includes girls who were likely to report sexual and physical abuse (77.2%-100% and 58.6%-74.4%, respectively) and unlikely to report any other child risk factors. Across phases, class membership in the abuse class ranged from 11.9%-20.5%. In Phases I and II twice as many girls belonged to the abuse class than boys; however similar proportions of girls and boys belonged to this class in Phase III. The status-offense class includes girls (21.9%-28.5%) who were most likely to endorse running away (63.7%-81.7%) and drug use (31.3%-49.7%), and less likely to endorse the remainder of risk factors. The low-risk class represents the largest proportion of girls and represents girls who were unlikely to endorse any of the risk factors (estimated probabilities range from 0%-10.8%). In Phases I and II, a lower proportion of girls belonged to the low-risk class compared to the proportion of boys in the low-risk class; in Phase III, similar proportions of boys and girls belonged to this class.
Despite the similarities, item endorsement in each class varied across phases. The probability of being sexually abused, for instance, increases among both high-risk and abuse girls between Phases I and III (from 82.6% to 98.3% and from 77.2% to 100.0%, respectively).
Association Between Class Membership and Age
Age significantly predicted the probability of belonging to the high-risk and status-offense classes compared to the low-risk class for both boys and girls, and in all phases (Table 3), except for high-risk boys in Phase III. Re-estimated conditional probabilities for each class were generally consistent with the original interpretation and are available upon request from the authors.
Table 3. Odds ratios between each class and low-risk class as a function of age.
| Phase I | Phase II | Phase III | ||||
|---|---|---|---|---|---|---|
| Estimate | 95%CI | Estimate | 95%CI | Estimate | 95%CI | |
| Boys | ||||||
| HR | 1.60 | 1.39-1.84 | 2.00 | 1.28-3.13 | 1.65 | 0.93-2.93 |
| AB | 0.96 | 0.9-1.01 | 1.04 | 0.94-1.14 | 1.00 | 0.92-1.08 |
| SO | 1.97 | 1.8-2.16 | 2.51 | 1.98-3.17 | 1.87 | 1.65-2.13 |
| Girls | ||||||
| HR | 2.32 | 1.78-3.03 | 2.39 | 1.89-3.02 | 2.30 | 1.83-2.90 |
| AB | 1.02 | 0.92-1.12 | 1.07 | 0.9-1.26 | 0.93 | 0.83-1.03 |
| SO | 2.30 | 1.78-2.96 | 2.32 | 2.00-2.69 | 2.10 | 1.73-2.54 |
Class label HR refers to high-risk, AB to abuse and SO to status-offense and LR to low-risk. Significantly different odds can be identified using odds ratios confidence intervals, i.e. those that do not include 1.
Boys
Figure 2 shows the fitted values, for each gender/phase group, of the probability of belonging to each class, as a function of age. In general, boys less than 11 years had a high probability of being in the low-risk class, a much lower probability of being in the abuse class, and almost no probability of being in the status-offense or high-risk classes. These patterns reversed for older boys who exhibited a higher probability of belonging to the status-offense class and the high-risk class.
Figure 2. Class membership probabilities as a function of age for boys and girls and across phases.
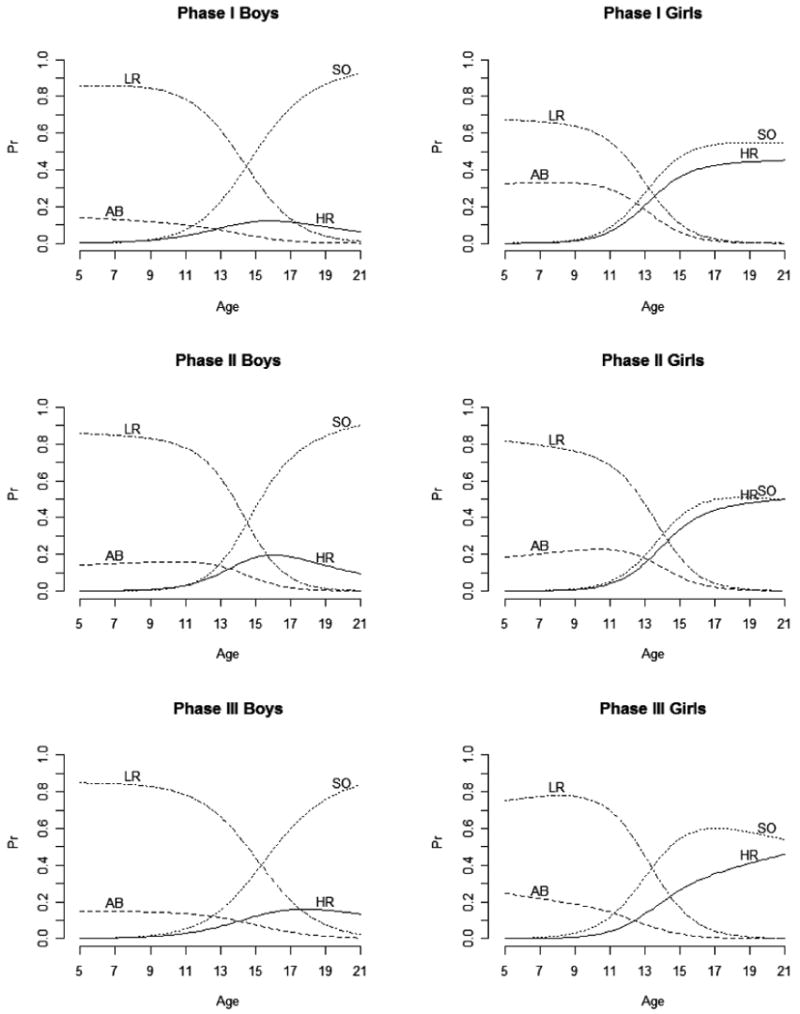
HR= high-risk, AB=abuse, SO= status-offense and LR= low-risk
Girls
A similar relationship between class membership and age was found for girls (Figure 2). Younger girls had a higher probability of belonging in the low-risk and abuse classes than older girls. Compared to younger boys, younger girls were more likely to belong to the abuse class, although this difference decreased across funding phase. Older girls had a higher probability of belonging to the high-risk and status-offense classes than younger girls. The proportion of older girls in the high-risk class was greater than the proportion of older boys in the high-risk class. Conversely, the proportion of older girls in the status-offense class was less than the proportion of boys in the status-offense class.
Latent Class Regression: Impairment
To examine the relation between class membership and functional impairment, the complete set of parameters, which describe the nature and prevalence of classes, as well as their relationship with age, were re-estimated. The relationship between class membership and functional impairment was then examined by gender and phase. Mean impairment scores and variances differed significantly by latent class (Wald tests of equal means (181.8 with 18 df) and of equal variances (1077.0 with 18 df) across classes), for both boys and girls and across phases. With the exception of Phase III boys in the high-risk class, the four-class conditional probabilities for boys and girls across phases (results available upon request from the authors) were generally consistent with the previously described high-risk, status-offense, abuse, and low-risk classes. The differences among the Phase III boys in the high-risk class are described below.
Boys
Table 4 presents mean functional impairment scores for each class by gender and phase. While there are some similarities among boys in the high-risk class across phases, there are substantive differences worthy of further description. Across all phases, boys in the high-risk class had the highest impairment scores and boys in the low-risk class had the lowest impairment scores. The Phase I estimated mean impairment for boys in the abuse class was lower than the impairment for boys in the status-offense class, a difference that largely disappears in Phases II and III. Similar to previous phases, high-risk boys in Phase III presented the highest probability of suicide attempt. Unlike previous phases, however, the probabilities of presenting any other risk factors were rather low (lower than 50% in all cases).
Table 4. Estimated mean CAFAS total score.
| Phase I | Phase II | Phase III | ||||
|---|---|---|---|---|---|---|
| Estimate | 95%CI | Estimate | 95%CI | Estimate | 95%CI | |
| Boys | ||||||
| HR | 135.5 | 125.2-145.8 | 139.1 | 124.4-153.8 | 157.0 | 146.2-167.9 |
| AB | 92.2 | 82.2-102.2 | 117.4 | 109.6-125.3 | 130.6 | 120.1-141.1 |
| SO | 109.9 | 105.2-114.5 | 109.7 | 89.6-129.9 | 120.4 | 113.1-127.8 |
| LR | 74.9 | 72.7-77.1 | 95.6 | 90.3-100.9 | 98.9 | 93.1-104.6 |
| Girls | ||||||
| HR | 113.6 | 106.9-120.3 | 132.2 | 122.1-142.2 | 134.5 | 122.4-146.5 |
| AB | 71.3 | 63.5-79.1 | 99.4 | 80.3-118.5 | 121.7 | 103.4-139.9 |
| SO | 92.2 | 85.1-99.4 | 119.4 | 106.9-131.9 | 118.1 | 109.6-126.6 |
| LR | 51.4 | 45.8-57.1 | 88.6 | 79.0-98.2 | 95.0 | 88.4-101.7 |
HR= high-risk, AB=abuse, SO=status-offense and LR= low-risk.
Girls
A similar pattern was found for girls (Table 4). Girls in the high-risk class had the highest impairment scores and girls in the low-risk class had the lowest impairment scores. In Phase I, the estimated mean impairment for girls in the abuse class was lower than mean impairment for girls in the status-offense class, but this difference also largely disappeared in Phases II and III.
Discussion
Multigroup latent class analysis was used to identify groups of children with similar patterns of risk entering into mental health service systems over three programmatic funding phases of the Children's Mental Health Initiative. Four latent classes offer, overall, the best explanation for the risk patterns observed across gender and phases. These four classes exhibit similarities across the groups and an interpretation consistent with the earlier CMHI study14 was proposed (e.g. low-risk, status-offense, abuse, and high-risk classes).
Specifically and largely consistent with the similar LCA investigation into risk class membership,14 this study found that the proportion of girls in the high-risk class was greater than the proportion of boys in the same class. These “high-risk” girls enter services having experienced significant adverse events in their lifetime, particularly physical and sexual abuse, running away, attempting suicide, and substance use. Girls entering systems of care with these histories may need differential services to address these specific risks. While a greater proportion of girls than boys were in the high-risk class across each of the program funding periods, the difference between boys and girls diminished across funding periods. The proportion of boys in the low-risk class decreased with each successive funding period, and consequently, greater proportions of boys fell in the status-offense, abuse, and high-risk classes. This shift is partially explained by a change in the age composition of boys served and, in fact, is less marked in the models which include age as a predictor of class membership. It may also reflect the priorities and characteristics of the sites that were funded in the later phases. Perhaps these later sites made efforts to identify and enroll boys with more complex problems into services and/or emphasized partnerships with agencies that prioritized boys with different risk profiles for service receipt.
While there were similarities in the four-class structure across each of the funding periods, there were also differences in the probability of endorsing risk items across phases. For example, in the first phase, boys in the high-risk group had a high probability of physical abuse, sexual abuse, and running away. The probability of endorsing these risk factors decreased in the subsequent phases, even after controlling for age. Furthermore, when impairment was included in the model, the nature of the high-risk class for boys varied markedly across phases. While the conditional probabilities were generally more constant for girls, there were also significant differences across phases. In particular, the conditional probability of being sexually abused increased among both high-risk and abuse girls between Phases I and III.
These findings should be considered in light of study limitations. Caregivers provided information on the child risk factors and caregivers' responses may have been influenced by a desire to provide socially acceptable answers. The investigation into patterns of child risk was limited to the six child risk factors assessed in the study. The inclusion of other child risk factors could alter the patterns found. Alternative statistical models could provide plausible explanations for the observed data. For example, relaxing the local independence restriction of the standard LCA could result in more parsimonious models and open a promising line of research. There were changes to the national evaluation study protocol between Phase I and Phase II, which could explain some of the differences found across phases. This is particularly the case for the CAFAS, which was only administered to a sub-sample of children (i.e., those participating in the longitudinal outcome study) in Phases II and III.
Implications for Behavioral Health
This study has implications for systems of care and service planning. The study identified groups of children entering systems of care with similar exposures to child risk factors. Clinicians and service providers can use this information to better develop individualized treatment plans for children and their families. For example, boys and girls in the high-risk group may need intensive and specialized services that children in the low-risk class may not need. Also, in a climate of limited resources, program planners can utilize this information to direct resources to those children in greatest need.
Across funding phases, the Children's Mental Health Initiative has enrolled an increasing proportion of boys with complex histories of child risk. This shift includes a greater proportion of boys with a history of drug use and running away, behaviors that often result in contact with service sectors such as juvenile justice. This raises the increasing importance of ongoing coordination and collaboration between sectors that serve children and their families. Such collaboration will enhance service providers' abilities to anticipate the needs of and develop treatment plans for boys who enter systems of care having experienced multiple child risk factors, which could ultimately prevent or mitigate their involvement with more restrictive and potentially more costly service systems, such as juvenile justice.
Across funding phases, a greater proportion of girls than boys entered systems of care with a history of multiple child risk factors. Previous studies related to gender suggest that girls enter into system of care services with more severe problems than boys.14, 3-25 Taken together, these findings suggest that there is a higher threshold or tolerance level for problems in girls. This raises questions concerning how mental health problems in girls are perceived and identified, and whether resources should be focused to increase awareness regarding behaviors in girls that suggest need for mental health services.
In addition to the above-mentioned implications, the study findings also have implications for future research. In addition to child-level risk factors, there are also family-, community-, and societal-level factors that place children at risk for mental health problems. Research that takes into account these multiple types of risk factors and identifies groups of children with similar risk histories will further enhance a service system's ability to provide services tailored to the individual needs of children and their families. A better understanding of the relation between the risk classes, gender, and how children enter into services could also provide useful information to agencies collaborating together to address the mental health needs of children. Finally, the Children's Mental Health Initiative and the national evaluation are ongoing efforts that provide continued opportunity to examine whether the changing trend in the types of children enrolling in systems of care programs continues into the future.
Acknowledgments
This research was supported by National Institute of Mental Health Grant # 1R01MH075828. The views expressed are the opinions of the authors and not those of the Substance Abuse and Mental Health Services Agency, the National Institute of Mental Health, the National Institute of Health, or the federal government.
Footnotes
As noted in the Analysis section, this unrestricted multi-group LC model is equivalent to the estimation of a separate model for each group but overall measures of fit are presented.
Iterative optimization techniques such as the one used in LCA may reach solutions, called local maxima, that do not represent the Maximum Likelihood Estimation. To minimize this possibility, the estimation process is repeated with different starting values (chosen at random) until the results are replicated several times. It was not possible, however, to replicate the results from H5C.
References
- 1.Pires SA. Building Systems of Care: A Primer. Washington, D.C.: National Technical Assistance Center for Children's Mental Health, Georgetown University Child Development Center; 2002. [Google Scholar]
- 2.Center for Mental Health Services. Atlanta, GA: ORC Macro; 2003. Comprehensive Community Mental Health Services for Children and Their Families program, evaluation findings–Annual report to congress, 2002–2003. DHHS SMA-CB-E2002/03. Available at: http://download.ncadi.samhsa.gov/ken/pdf/SMA03-CBE2002/CongReport20022003FINALPUBLICATION.pdf. [Google Scholar]
- 3.Manteuffel B, Stephens R, Santiago R. Overview of the national evaluation of the Comprehensive Community Mental Health Services for Children and Their Families program. Children's Services: Social Policy, Research, and Practice. 2002;5:3–20. [Google Scholar]
- 4.Schilling EA, Aseltine RH, Jr, Gore S. Adverse childhood experiences and mental health in young adults: A longitudinal survey. BMC Public Health. 2007;7:30. doi: 10.1186/1471-2458-7-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shanahan L, Copeland W, Costello EJ, et al. Specificity of putative psychosocial risk factors for psychiatric disorders in children and adolescents. Journal of Child Psychology and Psychiatry. 2008;49:34–42. doi: 10.1111/j.1469-7610.2007.01822.x. [DOI] [PubMed] [Google Scholar]
- 6.Cabiya JJ, Canino G, Chavez L, et al. Gender disparities in mental health service use of Puerto Rican children and adolescents. Journal of Child Psychology and Psychiatry. 2006;47:840–848. doi: 10.1111/j.1469-7610.2006.01623.x. [DOI] [PubMed] [Google Scholar]
- 7.Zimmerman FJ. Social and economic determinants of disparities in professional help-seeking for child mental health problems: Evidence from a national sample. Health Services Research. 2005;40:1514–1533. doi: 10.1111/j.1475-6773.2005.00411.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.D'Oosterlinck F, Broekaert E, De Wilde J, et al. Characteristics and profile of boys and girls with emotional and behavioural disorders in Flanders mental health institutes: A quantitative study. Child: Care, Health and Development. 2006;32:213–224. doi: 10.1111/j.1365-2214.2006.00607.x. [DOI] [PubMed] [Google Scholar]
- 9.Barksdale CL, Azur MJ, Leaf PJ. Racial disparities in mental health service sector utilization among youth entering systems of care programs. Journal of Behavioral Health Services & Research. 2009 February 14; doi: 10.1007/s11414-009-9166-2. published online. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hazen AL, Hough RL, Landsverk JA, et al. Use of mental health services by youths in public sectors of care. Mental Health Services Administration. 2004;6:213–226. doi: 10.1023/b:mhsr.0000044747.54525.36. [DOI] [PubMed] [Google Scholar]
- 11.Garland AF, Hough RL, McCabe KM, et al. Prevalence of psychiatric disorders in youths across five sectors of care. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40:409. doi: 10.1097/00004583-200104000-00009. [DOI] [PubMed] [Google Scholar]
- 12.Handwerk ML, Clopton K, Huefner JC, et al. Gender differences in adolescents in residential treatment. American Journal of Orthopsychiatry. 2006;76:312–324. doi: 10.1037/0002-9432.76.3.312. [DOI] [PubMed] [Google Scholar]
- 13.Hussey DL, Drinkard AM, Falletta L, et al. Understanding clinical complexity in delinquent youth: Comorbidities, service utilization, cost, and outcomes. Journal of Psychoactive Drugs. 2008;40:85–95. doi: 10.1080/02791072.2008.10399764. [DOI] [PubMed] [Google Scholar]
- 14.Walrath CM, Petras H, Mandell DS, et al. Gender differences in patterns of risk factors among children receiving mental health services: Latent class analyses. Journal of Behavioral Health Services and Research. 2004;31:297–311. doi: 10.1007/BF02287292. [DOI] [PubMed] [Google Scholar]
- 15.Clogg CC, Goodman LA. Latent structure analysis of a set of multidimensional contingency tables. Journal of the American Statistical Association. 1984;79:762–771. [Google Scholar]
- 16.McCutcheon AL. Basic concepts and procedures in single- and multiple-group latent class analysis. In: Hagenaars JA, McCutcheon AL, editors. Applied Latent Class Analysis. Cambridge, U.K.: Cambridge University Press; 2002. pp. 56–85. [Google Scholar]
- 17.Hodges K, Lambert W, Summerfelt WT. Validity of a measure to assess impairment: The child and adolescent functional assessment scale (CAFAS) 1994. February-March., [Google Scholar]
- 18.Hodges K, Wong MM. Psychometric characteristics of a multidimensional measure to assess impairment: The Child and Adolescent Functional Assessment Scale. Journal of Child and Family Studies. 1996;5:445–467. [Google Scholar]
- 19.Hodges K, Wong MM. Use of the child and adolescent functional assessment scale to predict service utilization and cost. Journal of Mental Health Administration. 1997;24:278–290. doi: 10.1007/BF02832662. [DOI] [PubMed] [Google Scholar]
- 20.Hodges K, Kim CS. Psychometric study of the Child and Adolescent Functional Assessment Scale: Prediction of contact with the law and poor school attendance. Journal of Abnormal Child Psychology. 2000;28:287–2997. doi: 10.1023/a:1005100521818. [DOI] [PubMed] [Google Scholar]
- 21.Hodges K. CAFAS self-training manual and blank scoring forms. Ypsilanti, MI: Eastern Michigan University, Department of Psychology; 1990. [Google Scholar]
- 22.Muthén BO, Muthén LK. Mplus User's Guide. Los Angeles, CA: Muthén&Muthén; 2007. [Google Scholar]
- 23.Walrath C, Godoy Garraza L, Stephens R, et al. The CMHI 14 Years Later: Who has been Served and How have their Characteristics Changed?. The 21st Annual Research Conference Proceedings, A System of Care for Children's Mental Health: Expanding the Research Base; Tampa, FL: University of South Florida, The Louis de la Parte Florida Mental Health Institute, Research and Training Center for Children's Mental Health; 2008. pp. 103–104. [Google Scholar]
- 24.Walrath C, Ybarra M, Holden EW, et al. Children with reported histories of sexual abuse: Utilizing multiple perspectives to understand clinical and psychosocial profiles. Child Abuse and Neglect. 2003;1370:1–16. doi: 10.1016/s0145-2134(03)00035-8. [DOI] [PubMed] [Google Scholar]
- 25.Walrath C, Mandell DS, Holden EW, et al. Assessing the strengths of children referred for community-based mental health services. Mental Health Services Research. 2004;6:1–8. doi: 10.1023/b:mhsr.0000011252.84719.f2. [DOI] [PubMed] [Google Scholar]