

Abstract
Sustained or spontaneous hyperventilation has been associated with a variety of physical symptoms and has been linked to a number of organic illnesses and mental disorders. Theories of panic disorder hold that hyperventilation either produces feared symptoms of hypocapnia or protects against feared suffocation symptoms of hypercapnia. Although the evidence for both theories is inconclusive, findings from observational, experimental, and therapeutic studies suggest an important role of low carbon dioxide (CO2) levels in this disorder. Similarly, hypocapnia and associated hyperpnia are linked to bronchoconstriction, symptom exacerbation, and lower quality of life in patients with asthma. Raising CO2 levels by means of therapeutic capnometry has proven beneficial effects in both disorders, and the reversing of hyperventilation has emerged as a potent mediator for reductions in panic symptom severity and treatment success.
Keywords: hyperventilation, anxiety, panic, asthma, respiration, partial pressure of carbon dioxide, biofeedback therapy
1. The Study of Hyperventilation in Health and Disease
Hyperventilation, or hypocapnia, has been a pervasive topic in the general psychophysiology of emotion and performance (Wientjes, 1992; Ley & Yelich, 1998) as well as the clinical psychophysiology of anxiety disorders (e.g., Ley, 1992; Roth et al., 2005) and asthma (Herxheimer, 1946; Clarke & Gibson, 1980; Bruton & Holgate, 2005). Hyperventilation is caused by increased alveolar ventilation relative to metabolic carbon dioxide production. Consequently, alveolar carbon dioxide pressure tends to fall below normal levels (McDonough, 1994). Functionally, hyperventilation involves either fast or deeper breathing, or it may be the combination of both, resulting in an increase in minute ventilation above what is required by the organism’s metabolic demand (Gardner, 1996; Wientjes, 1992). Hyperventilation differs from hyperpnea, which is increased minute ventilation without change in carbon dioxide partial pressure (PCO2). Levels of PCO2 falling below 35 mmHg typically indicate that breathing is in the hypocapnic range (Oakes, 1996), and levels around 30 mmHg or lower on repeated occasions and across longer measurements periods have been proposed as being indicative of “unequivocal chronic hypocapnia” (Bass & Gardner, 1985). PCO2 is commonly measured in three ways: 1) directly from arterial or venous blood, 2) from expired air as end-tidal partial pressure of CO2 (PetCO2), or 3) transcutaneously, from the skin’s surface (PtCO2). While arterial or venous measurements are often impractical for psychophysiology due to their invasive nature, PtCO2 measurements are limited in detecting acute arterial PCO2 changes due to the slow detection time (approximately 2 min) that is caused by the slow diffusion of CO2 through the skin (Sanders et al., 1994; Wilhelm & Roth, 2001).
Acute hyperventilation with low levels of PCO2 is accompanied by disturbance of the acid-base balance (high pH levels, acute respiratory alkalosis). However, in chronic hyperventilation, low levels of PCO2 are typically accompanied by near-normal pH levels due to the release of hydrogen ions from protein and blood buffers and the reduction of bicarbonate levels by the kidneys (Fried, 1993). Determination of acid-base status by blood gas analysis is necessary for the correct diagnosis of the latter condition. Jack et al. (2004) observed arterial pH within the normal range and a significant base excess, consistent with compensated respiratory alkalosis in patients with chronic idiopathic hyperventilation.
Hypocapnia can be observed in a variety of organic illnesses, psychological disorders, and negative affective states and traits (Gardner, 1996; Grossman, 1983; Laffey & Kavanagh, 2002; Meuret, in press). It also has been linked to a variety of adverse health outcomes. Although hypocapnia is sometimes viewed as therapeutic by clinicians, for example in enhancing the effects of general anesthesia, reducing intracranial pressure due to head injury, or relieving pulmonary hypertension in neonatal respiratory failure, evidence for its adverse short- and long-lasting effects is increasingly well documented (Laffey & Kavanagh, 2002). In the central nervous system, detrimental effects include increases in seizure activity, cerebral ischemia with negative consequences for neonatal or traumatic brain injury, and postoperative impairments in cognitive function. In the periphery, hypocapnic alkalosis may also contribute to acute lung injury; worsen peripheral vascular disorders, myocardial ischemia, or thrombosis by increases in vasoconstriction and platelet aggregation; or may precipitate cardiac dysrhythmias.
The aim of this review is to a) describe the evidence on the impact of hypocapnia on symptom development as well as biological and psychological states, including quality of life, and b) discuss clinical implications and treatment considerations based on findings related to hypocapnia. We will include examples of the successful application of capnometry-assisted respiratory training in hypocapnic patients that has lead to successful and lasting elevation/correction of PCO2 into the eucapnic range.
We will focus on two conditions, asthma and panic disorder, as the role of sustained levels of hypocapnia have been studied most frequently in these disorders and may play a particularly crucial role in disease progression. In addition, an elevated comorbidity exists between both types of disorders (Carr, 1998) and hyperventilation may provide an interesting link between them. Other conditions such as epilepsy (Fried et al., 1984), neonatal brain injury (Greisen et al., 1987), or cardiac dysrhythmias (Mazzara et al., 1974) will not be considered here. Complications in another anxiety disorder, the specific phobia of blood, injections, and injuries, have also been associated with hyperventilation more recently (Ritz et al., 2005; 2009) and will be discussed separately in this issue (Ritz et al., this issue).
Historically, the 1980s and 90s have seen a controversial discussion surrounding hyperventilation as an illness syndrome (Lum, 1987). Agreement about criteria for the hyperventilation syndrome was never reached (Bass, 1997), and research has called into question whether symptoms elicited by hyperventilation were sufficiently specific (e.g., Hornsveld et al., 1996)1. While the evidence for such a nosological category remained weak, the sometimes acrimonious tone of the debate has discouraged parts of the research community from continuing their inquiry into potentially detrimental effects of hypocapnia in health and disease. At this critical juncture, the laboratory at Stanford University and the VA Palo Alto led by Walton T. Roth was among those who recognized the need for more empirical research in this area.
2. Hypocapnia in Panic Disorder
2.1. Symptom experience of panic patients and respiratory theories of panic disorder
Abnormalities in respiration have been postulated to play a central role in the development and maintenance of panic disorder. The clinical literature abounds with observations of panic patients presenting with a variety of physical complaints for which no organic origin is apparent. Among the most frequent and distressing symptoms reported by panic patients are sensations of shortness of breath, together with palpitations and faintness (McNally et al., 1995, Meuret et al., 2006). Other physical symptoms include dizziness and light-headedness, sensations of chest pain or pressure, as well as tingling sensations in the extremities. Respiratory symptoms specifically best distinguish the panic attacks of individuals with panic disorder from those of individuals without panic (Vickers & McNally, 2005). It has been further suggested that indices of respiratory parameters (e.g., PCO2, tidal volume, respiratory frequency) may better correlate with feelings of anxiety compared to other physiological functions, including heart rate (Meuret et al., 2009; Meuret et al., in press; Alpers et al., 2005, in patients with driving phobia).
It has been proposed that the underlying origin of these respiratory symptoms in various patient groups may be attributed to a disturbance in the acid-base balance (Lum, 1987). In earlier research, the hyperventilation syndrome had become a common designation for the constellation of complaints of these patients and the diagnosis had been reported to be present in at least 5 to 10% of general medical outpatients (Magarian, 1982). The breathing pattern of these patients were typically described as disorganized, with lower than normal PCO2 levels, rapid respiration rates, frequent sighing, and predominately thoracic rather than abdominal breathing. Additionally, these patients were often described as feeling anxious and depressed (Howell, 1997).
These observations had led to the formulation of two respiratory theories proposing a causal relationship between respiratory regulation, particularly related to PCO2, and panic: Ley’s hyperventilation theory (1986) and Klein’s suffocation false alarm theory (1993). In the former, the basic assumption is that panic attacks are caused by acute states of hypocapnia. In addition, hyperventilation may not be limited to the attack itself, but may precede and follow it, giving rise to moderate sustained hypocapnia. According to this hypothesis, the cause of seemingly spontaneous panic attacks is sustained through episodic periods of hyperventilation that often occur outside of the patient’s awareness. Hypocapnia also plays a role in Klein’s suffocation false alarm theory (Klein, 1993), but not as the primary cause of panic. Rather, hyperventilation is viewed as a compensatory or secondary reaction to an overly sensitive “suffocation alarm system” in these patients2. When a patient’s PCO2 rises, the system starts firing at an abnormally low threshold and/or responds with greater sensitivity to increments in CO2. This leads to disproportional dyspnea (sensations of air hunger, breathlessness, suffocation), which due to its distressing nature, initiates a cascade of panic symptoms. In this context, chronic hyperventilation is interpreted as an adaptation to a lowered suffocation alarm threshold, in that it keeps PCO2 sufficiently low to avoid triggering the suffocation alarm.
From a cognitive viewpoint, bodily sensations, including hyperventilation symptoms, are thought to trigger panic attacks (Clark, 1986; McNally, 1994). However, it is the fearful interpretation of these sensations, not the sensation itself that triggers the attack (for example, “shortness of breath means I am having an asthma attack and will suffocate”). According to Clark (1986), alleviating the physical symptoms is not sufficient for treatment success unless this is accompanied by reductions in catastrophic interpretations. Consequently, patients undergoing training in cognitive therapy are told that hyperventilation, like a variety of other sources of physiological symptoms, is harmless and constitutes no threat to the individual’s well-being. The importance of appraisal of bodily sensations associated with arousal in panic disorder has found strong support in past and recent literature (Clark, 1986; Barlow, 2002; Hofmann et al., 2007; Schmidt et al., 1997; Kroeze et al., 2005) and represents a significant source of influence in determining psychophysiological associations in this disorder.
2.2 Baseline levels of PCO2: evidence for prolonged hypocapnic states?
As noted earlier, the accurate assessment of chronic states of hyperventilation requires the assessment of acid-base status by means of analysis of blood samples. Such assessment has been done by very few studies in panic disorder and findings have been mixed. Evidence for chronic hyperventilation using measurements of acid-base balance was found in studies by Gorman et al. (1986) and Papp et al. (1989), but not Zandbergen et al. (1993). Studies assessing end-tidal measures of PCO2 are more numerous and provide evidence for differences in baseline levels between patients suffering from panic disorder compared to non-panic patients and healthy controls. For example, in a study by Papp et al. (1997), respiratory psychophysiology was examined in patients with panic disorder compared to healthy control volunteers undergoing challenge tests (see below). The authors also examined baseline respiratory characteristics between the two groups. They found that levels of baseline end-tidal PCO2 were significantly lower for patients compared to healthy controls. However, baseline levels among the panic patients did not differentiate those who panicked from those who did not during the challenge tests. Other respiratory parameters (respiratory rate, tidal volume, and minute ventilation) also showed higher levels in patients compared to controls, but the differences did not reach significance. Other studies found lower end-tidal PCO2 in panic patients but not controls prior to a lactate infusion challenge (Coplan et al., 1998; Liebowitz et al., 1985) or voluntary hyperventilation (Wilhelm et al., 2001). Regarding disorder specificity, lower end-tidal PCO2 levels were observed in panic patients compared to patients with posttraumatic stress disorder (PTSD) and healthy controls (Blechert et al., 2008). Lower end-tidal (Hegel & Ferguson, 1997) or venous CO2 levels (Munjack et al., 1993) were reported in panic patients compared to patients with generalized anxiety disorder and healthy controls. Lower end-tidal PCO2 was also observed in panic patients compared to controls just before and after a breath holding challenge test, whereas patients with generalized anxiety disorder showed intermediate levels (Roth et al., 1998). Van den Hout and colleagues (1992) observed hypocapnia at baseline (assessed via end-tidal PCO2) in both individuals with panic disorder and non-panic anxiety disorder patients compared to healthy controls. Levels decreased further during fearful imagery, which corresponded to increases in distress experience, but no group differences were observed in this response. The authors interpreted the changes in PCO2 as a nonspecific concomitant of fear or excitement rather than their cause. In our own studies, patients with panic disorder consistently displayed hypocapnic levels during baseline recordings of end-tidal PCO2 (e.g., Meuret et al., 2008, in press), but normalized when levels were therapeutically targeted (see below 4.1.3).
Thus, there is some evidence that both baseline end-tidal and venous PCO2 levels are lower in patients afflicted by panic disorder. However, since the majority of studies assessed PCO2 in proximity to a fear provoking challenge test, it is unclear whether the reduced levels were due to anticipatory anxiety or in some cases delayed recovery. In contrast with this body of evidence, other studies have not found evidence of hypocapnia in individuals with panic disorder during baselines (e.g., Holt & Andrews, 1989; Woods, et al., 1986).
Among the studies that have recorded baseline levels of PCO2 in absence of an anticipated stress test, hypocapnic levels were evident. For example, Salkovskis et al. (1986) found resting PCO2 levels to be significantly lower than normal before receiving breathing training. In other intervention studies, patients’ resting levels averaged around 33 mmHg prior to receiving a treatment aimed at reducing hyperventilation (Meuret et al., 2008) and/or cognitive therapy (Meuret et al., in press).
A number of studies have observed other respiratory abnormalities in panic patients that have been linked to sustained hypocapnia. In particular, breathing at variable tidal volume (“tidal volume instability”) or sigh breathing have been observed under baseline conditions (Wilhelm, Trabert, et al., 2001) or in REM sleep phases (Stein et al., 1995). Intermittent deep breaths can lower PCO2 levels and may be instrumental in helping to sustain lower PCO2 levels in panic patients (Papp et al., 1993). Wilhelm et al. (2001) also presented evidence for a specificity of stronger sigh breathing in panic compared to generalized anxiety disorder patients and healthy controls, although PCO2 levels did not distinguish between both patient groups in this study. Sigh breathing appears to be a stable respiratory characteristic that is not affected by cognitive strategies or doxapram-induced hyperventilation (Abelson et al., 2001), or by cognitive behavior or pharmacological therapy (Martinez et al., 2001). However, more recent findings question the specificity of volume variability for panic, as it has also been observed in blood-injection-injury patients (Ritz et al., 2009; Ayala et al., 2010) and in patients with PTSD but not in panic patients (Blechert et al., 2007). In addition, Pfaltz et al. (this issue) reported that in ambulatory monitoring of breathing patterns across two days, tidal volume variability was only elevated in stages of mild to moderate physical activity, but not under sedentary conditions, in panic patients compared to healthy controls. Sigh breathing did not differentiate between groups.
2.3. Response to respiratory challenge tests in panic patients
Respiratory theories, as described above, propose a direct connection between changes in PCO2 and the experience of anxiety and panic (Roth et al., 2005). This has motivated researchers to utilize a variety of experimental tests to examine the effect of artificially induced hypo- or hypercapnia.
The induction of hypocapnia is most often achieved through voluntary hyperventilation (VH). Despite its widespread use in studies of panic disorder, little consensus exists on standards of a VH test (for a review, Meuret et al., 2005). Patients are typically instructed to breathe faster than normal for a certain period of time but beyond this very general feature, studies vary greatly with regard to procedural parameters and outcome assessment. It often remains unclear whether actual decreases in PCO2 to moderate or severe levels of hypocapnia (30 to 20 mmHg) are achieved, because capnographic assessment is not reported. Some studies have relied on respiration rate measurements exclusively, or even on simple counting of breaths through observation, but this does not ensure that the patient is hyperventilating as increases in minute ventilation leading to hyperventilation have often been shown to be due to increases in tidal volume but not respiration rate (Gorman & Uy, 1987; Ritz et al., 2009; Meuret et al., 2005).
Figure 1 shows the progression of a VH challenge performed at the Stanford Anxiety Laboratory with a panic patient undergoing the provocation test (Meuret et al., 2005). The patient was successful in achieving the target level of 20 mmHg. Such a procedure most often elicits symptoms of shortness of breath, dizziness, heart racing, trembling, and tingling or numbness in the extremities. Feelings of unreality or fear of losing control are also reported. Some, but not all patients, report the occurrence of a panic attack. While the majority of symptoms subside by the end of a recovery period (in the case of this test, after 8 min), some patients continue to experience physical and cognitive symptoms (e.g., feelings of unreality) and/or show slower recovery from such a challenge (Wilhelm et al., 2001). Compared to other anxiety disorders or healthy controls, the physiological and psychological response to VH seems to be relatively specific to panic disorder (e.g., Antony, et al., 1997; Gorman, et al., 1994; Holt & Andrews, 1989; Gorman et al., 1988; Maddock & Carter, 1991; Wilhelm et al., 2001) and thus supports some basic assumptions of the above mentioned hyperventilation theory of Ley (1986). However, not all patients experience a panic attack or even experience anxiety, which questions theoretical models that view transient hypocapnia as a causal mechanism for panic (for further review, see Roth et al., 2005; Roth, 2005).
Figure 1.

Changes in PCO2 and respiration rate during a standardized voluntary hyperventilation test. Upper line represents end-tidal PCO2 and lower line represents respiration.
Exogenous CO2 can serve as a panicogen (Klein, 1989), and its effect has been widely tested in patients with PD. Here, the experimental procedure involves the inhalation of a higher than normal concentration of CO2 (typically ranging between 5–65%). Depending on the inhaled concentration, the test can elicit suffocation-like sensations of dyspnea and mild to pronounced states of anxiety or panic, with the latter often resembling naturally occurring panic attacks (Sanderson & Wetzler, 1990). The normal response to inhalation of elevated levels of CO2 also includes substantial increases in minute ventilation, respiration rate, and tidal volume (e.g., Alexander et al., 1960). Studies are equivocal with respect to the ventilatory response in panic patients, with some showing stronger increases in minute ventilation and/or inspiratory drive to CO2 inhalation than in healthy controls (e.g., Fishman et al., 1994; Gorman et al., 1988; Gorman et al., 2001; Lousberg et al., 1988; Papp et al., 1989; Rassovsky et al., 2006), and others showing no differences (Katzman et al., 2002; Papp et al., 1995, Papp et al., 1997; Woods et al., 1986; Zandbergen et al., 1991). Beyond minute ventilation, studies have shown differences between panic patients and healthy controls in aspects of respiratory adaptation to CO2 challenge, such as stronger increases in respiration rate (Beck et al., 1999; Papp et al., 1995; Papp et al., 1997; Pain et al., 1988; Sasaki et al., 1996), or reduced habituation of the tidal volume response across repeated challenges (Blechert et al., 2010). Some studies have also documented reduced tidal volume response in panic patients (Beck et al., 1999; Pain et al., 1988; Papp et al., 1995). A number of factors could account for this pattern of findings and discrepancies between observations, such as varying rates of panic in patients and control groups or response sets in patients (e.g., shallow breathing to avoid exposure). The response of healthy controls to various forms of CO2 challenge has been shown to be more variable, with a minority also responding with panic symptoms and stronger ventilatory changes (e.g., Gorman et al., 2001).
The stronger response of panic patients to CO2 challenge appears to have a trait component with a strong inheritability. In accordance are observations of asymptomatic first-degree relatives of patients with panic disorder who responded more fearfully to a 35% CO2 inhalation compared to healthy participants (Coryell, 1997; Perna et al., 1995).
While the hypersensitive response to hypercapnia has been well established in panic patients, the nature of the specific respiratory abnormalities in panic disorder remains controversial. Several reports have questioned the causal role of hypercapnia in eliciting panic or distinguishing panic patients from other anxiety patients or healthy controls (Roth et al., 1998; Beck et al., 1999; Schmidt et al., 1996). A general criticism of these inhalation studies is that the CO2 concentrations given are higher than those occurring naturally (McNally et al., 1995). The evidence on hypersensitivity of chemoreflexes in panic disorder has also remained equivocal (Katzman et al., 2002).
Additionally, it has been speculated that catastrophic cognitions, not biological responding, are the primary cause for why patients panic during these procedures. For instance, Rapee et al. (1986) administered single inhalations of a 50% CO2, with patients either receiving no explanation or detailed information on psychophysiological symptoms associated with the inhalation. Because the patients who had received no explanation responded with greater levels of panic-related symptoms, cognitions rather than physiological factors were thought to have mediated the symptoms. Sanderson et al. (1989) provide patients with a dial that supposedly controlled the amount of CO2 to be inhaled, but which in fact was ineffective. Patients in this condition were less likely to panic than patients who were not given the illusion of control. However, other studies have failed to replicate the finding that panic tendencies are dependent on patients’ cognitive sets (Welkowitz et al., 1999; Papp et al., 1995). Welkowitz et al. (1999) devised a stronger test of the perceived control hypothesis by providing patients with a functional control dial and blinded ratings of panic behavior. They were not able to find differences in panic rates when compared to two other conditions, standard instructions and reassurance of safety instructions. Evidence of at least partial influence of cognitive set variables on respiratory challenge responses also comes from treatment studies. Abelson et al. (1996) found that a cognitive intervention reduced panic attacks to doxapram challenge and substantially reduced the respiratory response. However, slight elevations in minute ventilation and reductions in PCO2 persisted despite treatment3.
Authors have also explored heterogeneity of the panic patient population with respect to a “respiratory subtype.” Analyzing retrospective reports of panic attacks, Briggs et al. (1993) identified a subtype of patients characterized by a symptom constellation that included respiratory symptoms such as shortness of breath, chest pain/discomfort, and choking/smothering sensations. However, it also included non-respiratory symptoms such as fear of dying. The symptom cluster has not been fully replicated (Shioiri et al., 1996; Meuret at al., 2006), but identified symptoms have been used in some studies to explore characteristics of respiratory subgroups of patients. For CO2 challenge, higher panic rates were found for respiratory compared to non-respiratory subtypes (Biber & Alkin, 1999; Freire et., 2008; Nardi et al., 2002). No differences in panic rates but stronger suffocation sensations were also found in the respiratory subtype (Abrams et al., 2006). For VH challenge, Freire et al. (2008) reported higher panic rates, but Meuret et al. (2008) only observed a tendency for slower recovery in PCO2 levels in the respiratory subgroup. Additional differences were found in some aspects of disease manifestation and baseline respiratory parameters across studies, but replications have remained rare. Although promising, more work on diagnostic criteria for this subtype is needed before stronger conclusions can be drawn.
2.4. Respiratory patterns during naturally occurring panic attacks
Based on the respiratory theories of panic, naturally occurring panic attacks should be preceded by sudden decreases in PCO2 (Ley, 1986) or increases (Klein, 1993). While such processes, if observed, would lend substantial face validity to the respective theories, the assessment is undoubtedly challenging, in part due to the sudden nature of the panic attacks themselves. Capturing the biological profile of real-life panic attacks not only requires extended recording times, but also advanced ambulatory technology that does not greatly interfere with patients’ daily life activities.
To date, only a few published studies report the assessment of real-life panic attacks, with the majority descriptive; measures of respiratory function, in particular PCO2, have been lacking. The two studies that have assessed changes in respiration during panic attacks yielded mixed results. Both used transcutaneous assessment of PCO2 (PtcCO2), which is not sufficiently sensitive to sudden changes in PCO2 levels. Decreases in PtcCO2 were found in some patients during the panic attacks in one study (Hibbert & Pilsbury, 1988), whereas hardly any changes, either before or during the panic attack, were found in another study (Garssen, Buikhuisen, & van Dyck, 1996). A third study (Martinez et al., 1996) monitored the respiratory pattern of panic patients for 24 hours and found elevated tidal volume instability in patients compared to controls.
A more recent study (Meuret et al., 2010; Rosenfield et al., 2010) successfully captured 13 panic attacks in eleven patients during repeated 24-hr ambulatory monitoring. Figure 2 illustrates the ambulatory set-up for assessing respiratory and other autonomic functions outside the laboratory using the Vitaport (Becker, Mannheim) ambulatory monitoring system combined with capnometry (see also Wilhelm et al., 2001). Central respiratory function parameters, such as tidal volume, respiratory rate, minute ventilation, and sigh rate, were measured by way of respiratory inductive plethysmography bands (Ritz et al., 2002) placed around the thorax and abdomen [4]. End-tidal PCO2 was assessed using a portable, battery-operated capnometry device (Weinmann, Karlsruhe, Germany) [9] that samples exhaled gas through a nasal cannula [1]. Other autonomic functions included cardiac activity [3] and electrodermal activity [7]. To control for sound, physical activity, and temperature, a sound sensor were placed on the throat [2], three accelerometers were attached to the arm, leg, and trunk [5], and external and finger temperature sensors [6] were also attached. An event button [8] was available to mark special occurrences (e.g., onset of panic attack, test periods).
Figure 2.
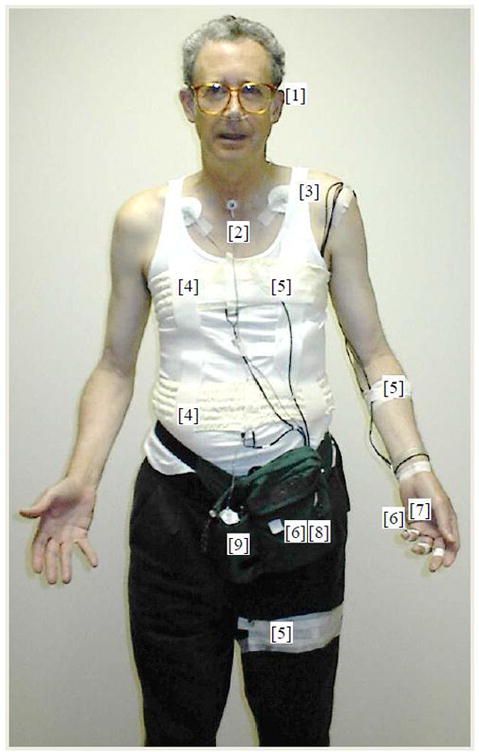
Illustration of the ambulatory set-up for 24-h monitoring with panic disorder patients. Capnometry device [9] with attached nasal cannula [1], sound sensor [2], EKG [3], thoracic and abdominal plethysmography bands [4], accelerometers [5], external and finger temperature sensors [6], electrodermal activity [7].
To determine whether panic attacks were preceded by autonomic activity or changes in PCO2, we adapted the method of change point analysis (Rosenfield et al., 2010) to detect the presence, sequence, and duration of unknown changes in these highly variable data sets. Compared to duration-matched control periods, the hour prior to the onset of a reported panic attack was marked by significant instability in cardiorespiratory function. Most intriguingly, levels of end-tidal PCO2 were significantly elevated (relative to initial levels) just prior to the onset of the panic attacks, which was remarkable given the applied Bonferroni correction of 4*50 to the standard p level of .05. The results were in line with the basic assumption of Klein’s (1993) suffocation alarm theory.
2.5. Conclusion
Taken together, a substantial body of literature suggests an involvement of respiratory processes in panic disorder, in particular those linked to hyperventilation. Although empirical findings supporting respiratory theories of panic are not always unequivocal, a great advantage over other theories of panic is that they are in fact falsifiable (Roth et al., 2005). Ultimately, one indicator of their value to the scientific community will lie in their potential to inform behavioral interventions for treatment of panic disorder. Below (see 4.1) we will exemplify one approach to panic disorder treatment that has its basis in respiratory theories of panic and that has shown promising results in reducing panic symptomatology.
3. Hypocapnia in Asthma
In the following, we will review the evidence for hypocapnia in asthma. As with studies examining the prevalence of hypocapnia in panic disorder, studies have reported a heightened prevalence of hypocapnia symptoms, reduced PCO2 levels, and an exaggerated increase in ventilation in response to a variety of stimuli in asthma. Experimental evidence that demonstrates adverse effects of hyperventilation in asthma will be reviewed. Furthermore, we will discuss circumstantial evidence linking hypocapnia in asthma to psychopathology (in particular panic), emotions, and stress.
3. 1. Hyperventilation symptom reporting in asthma
There are indications that symptoms of hyperventilation are relatively common in asthma. One survey of primary care patients in the UK suggests that symptoms of overbreathing’ can be found in 29% of asthma patients (Thomas et al., 2001), a larger percentage than in other primary care patients (Thomas et al., 2005). However, this survey was based on a questionnaire that included items that are common to both anxiety and asthma (shortness of breath, chest tightness) (Ritz, Bobb, et al., 2001; Bruton & Holgate, 2005). Earlier extensive research on asthmatic symptom reports using the Asthma Symptom Checklist (ASC) uncovered evidence that symptoms exclusively found in hyperventilation, such as tingling sensations, pins and needle feelings, dizziness, or numbness, form a separate cluster among asthma inpatients (Kinsman et al., 1973). Other studies with ambulatory outpatients or primary care populations confirmed the validity of this dimension (Belloch et al., 1997; Brooks et al., 1989; DePeuter et al., 2005; Ritz, Bobb, et al., 2001), although not all of them (Lebowitz et al., 1981). Authors of the latter study speculated that the lower asthma severity of outpatients was the reason for a failure to identify a hyperventilation symptom cluster; however, other outpatient studies with a larger range of asthma severities have identified this symptom cluster and did not find it to be associated with severity (Belloch et al., 1997).
In our own research, we found that the ASC hyperventilation symptom subscale was significantly associated with a lower general perceived health in asthma patients (Ritz, Rosenfield, et al., 2008). The findings also suggested that this relationship was partially mediated by the extent to which patients felt they were in control of their asthma management. Hyperventilation symptoms are typically not targeted by common anti-asthmatic medication, therefore, it could be speculated that the experience of such residual symptoms impacts perceived well-being through patients’ inability to control them.
3.2. Baseline PCO2 levels in asthma patients
Studies have found a high percentage of asthma cases among patients initially diagnosed with the hyperventilation syndrome (Gardner et al., 1992; Saisch et al., 1996; Demeter & Cordasco, 1986). In addition, compared with matched healthy controls, Osborne et al. (2000) reported statistically significant reductions in PCO2 in mild chronic asthmatics with no accompanying symptoms of hyperventilation. Hormbrey et al. (1988) observed lower levels of end-tidal PCO2 in a group of 27 asthma patients compared with 30 healthy controls and 29 patients previously diagnosed with “symptomatic hyperventilation,” although mean levels were still within the range of normocapnia for all three groups (37.2–42.4 mmHg). In an early study by Herxheimer (1946), 4 out of a total of 19 patients showed signs of chronic hyperventilation or a tendency to respond with strong increases in volume and breathing irregularity following minor stimulation. McFadden and Lyons (1968) observed drastic reductions in PCO2 associated with asthma attacks in asthma patients, often far below the threshold of 30mmHg defined for hypocapnia by Bass and Gardner (1985). These reductions in PCO2 can occur despite only moderate reductions in lung function. Furthermore, in acute asthma, increases in ventilation are beyond the level that is experimentally achieved by equivalent methacholine provocation (Gardner, 1996). In our own research (Ritz et al., in press), we found significantly lower PCO2 levels in a smaller sample of 15 asthma patients (33.8 mmHg) during neutral film viewing compared to blood-injection-injury phobics (n=12; 39.9 mmHg), with healthy controls (n=14) taking an intermediate position (37.4 mmHg).
3.3 Respiratory response of asthma patients to physical challenge
Compared to healthy controls, asthmatics have also been shown to respond with stronger increases in minute ventilation and/or respiratory drive to challenges such as brief static muscle tension of the forearm (Ritz et al., 1998), dynamic exercise (Varray & Prefaut, 1992), added resistive loads (Kelsen et al., 1979), conditioned responses to an innocuous inhaler device (after association with CO2 inhalation; DePeuter et al., 2005), or methacholine-induced bronchoconstriction (Fujimori et al., 1996). The latter study also found that PCO2 levels were lower for asthma patients than controls following challenge despite comparable bronchoconstriction. Thus, asthma patients demonstrate an exaggerated respiratory response to physical activity, airway obstruction, and potentially threatening situations, which makes them susceptible to further bronchoconstriction. An increase in respiratory drive through excessive deep breathing can also lead to subjective experience of dyspnea (Mahler et al., 1991).
3.4 Effects of hypocapnia in asthma
Herxheimer (1946) reported observations on five patients in which asthma symptoms were elicited by voluntary hyperventilation and prevented by breathing CO2 with comparable minute ventilation. Various triggers of spontaneous hyperventilation were identified in these patients, including physical exercise, excitement, and infections. Experimental studies have demonstrated that hypocapnia leads to a decline in lung function in asthma patients as well as sometimes in healthy controls (Butler et al., 1960; Newhouse et al., 1964; O’Cain et al., 1979; van den Elshout et al., 1991). Both autonomic (vagal) and local airway effects have been discussed as relevant mechanisms in these studies. Furthermore, a correlational study of mild asymptomatic asthma patients with airway hyperreactivity found an association between lower PCO2 and greater hyperresponsiveness of the airways to methacholine provocation (Osborne et al., 2000).
3.5 Effects of hyperpnea in asthma
Without leading to hypocapnia, increase in ventilation alone, as indicated by deep inspirations, high minute ventilation, or high respiratory drive, has been linked to asthma symptoms and airway obstruction, (Ritz, Dahme, et al., 2002). Thus, deep inspirations and fast expirations associated with spirometric measurements of lung function are known to lead to bronchoconstriction (Gayrard et al., 1975) and stronger nonspecific airway hyperreactivity (Orehek et al., 1975) in asthma. Similarly, while healthy airways dilate after deep inspirations, this mechanism may be deficient and even bronchoconstriction may occur with more severe asthma (e.g., Fish et al., 1981; Fredberg, 1998; Lim et al., 1987). Bronchoconstriction through isocapnic hyperventilation (hyperpnea with PCO2 levels experimentally compensated) is well documented in asthma and has become a standard challenge procedure (Solway, 1997). Indeed, one of the key mechanisms in exercise-induced asthma is linked to patients’ mode of ventilation, in particular airway cooling and/or drying (McFadden & Gilbert, 1994). Some authors attribute these effects to drying of the airways alone (Anderson, 1984). Animal models also indicate that repeated excessive ventilation with cold dry air results in elevated airway hyperresponsiveness, eosinophilic airway inflammation, and in impairments in response to β-adrenergic bronchodilators (Davis & Freed, 1999; 2001; Davis et al., 2003; Suzuki & Freed, 2002).
These adverse effects may occur independently from changes in PCO2. However, higher respiratory drive or minute ventilation puts patients at risk of becoming hypocapnic, which would add to the adverse effects of cooling and/or drying (McFadden & Gilbert, 1994). Thus, a deep breathing pattern with high minute volume and/or lowered PCO2 can lead to physiological changes contributing to exacerbations of asthma. This research also indicated that hyperventilation is a complex activity pattern that can affect the individual in ways separate from the disturbance in the acid-base balance it creates.
3.6 The role of emotions and panic in asthmatic hypocapnia
Clinical and experimental studies have linked reductions in PCO2 levels or hypocapnia to emotional states such as overwhelming stress (Boiten et al., 1994; Wientjes, 1992) or panic (see B2.1). A wide range of patients with psychiatric disorders involving elevated negative affect (neuroticism, anxiety) has typically been found to have low PCO2 values, which generally normalize after therapy (Grossman, 1983). To the extent that hypocapnic breathing is involved in the etiology, maintenance, or clinical manifestation of panic disorder, the well-documented comorbidity of asthma and panic disorder (Carr, 1998; Goodwin, 2003; Hasler et al., 2005) can be expected to increase the likelihood of observing hyperventilation in asthma. Emotional expressions that include stronger recruitment of the respiratory system such as laughing and shouting can indeed reduce PCO2 levels. Patients described by Herxheimer (1946) demonstrating chronic hyperventilation had reported a history of asthma attacks after “prolonged excitement (expectation of a thrilling event, laughter, prolonged argument, sexual intercourse)” (p. 86). In one study of emotional induction by brief 2.5 to 5-min film clips, we found that in healthy control participants, the lowest (though still normocapnic) PCO2 levels were reached during amusing films (Ritz, Wilhelm et al., 2005). It has been assumed that hyperventilation is also the mediator for asthma exacerbations induced by stress and anxiety states (e.g., Knapp, 1989). In a recent self-report study (Ritz, Kullowatz, et al., 2008), we found that reports of psychological triggers of asthma explained 4.3–11.5% of the variance in ASC hyperventilation symptoms over and above all other asthma trigger factors (allergens, air pollution, physical activity, infection) across two samples of British and German asthma patients with intermittent to moderate persistent severity of disease. However, observational and experimental evidence for this pathway in emotion- or stress-induced asthma remains scarce. Clarke and Gibson (1980) found drastic increases in minute ventilation in asthma patients during imagery of asthma-relevant scenes, but no PCO2 measurements were reported. While subsequent experimental emotion induction studies and longitudinal observational studies have provided ample evidence for bronchoconstriction due to negative and also positive emotional states (for reviews see Isenberg et al., 1992; Ritz & Kullowatz, 2005), little evidence points to the actual involvement of ventilatory changes, such as minute ventilation or PCO2, in emotion-induced airway obstruction (Ritz, 2004; Ritz et al., in press). Among longitudinal studies, only one case study of an asthma patient with a history of anxiety- and arousal-induced attacks was reported by Hibbert and Pilsbury (1988) in which PtcCO2, lung function (by peak flow), and anxiety were recorded continuously in a laboratory protocol before and after 5 treatment sessions of breathing training. Although reductions in hyperventilation were demonstrated through training, the report did not adequately test the association of anxiety with hyperventilation and subsequent lung function decline.
Thus, more evidence from systematic observations and experimental studies is needed to determine the role of emotions as a cause for asthmatic hyperventilation. It is possible that the emotional component is more visible in acute exacerbations of asthma, when patients may develop feelings of panic over perceived obstructions. Stimulus generalization or interoceptive conditioning may then account for sustained hypocapnia beyond the immediate exacerbation context.
3.7. Conclusion
Overall, there is good evidence that symptoms of hypocapnia are problematic for at least some asthma patients, as reduced PCO2 levels and symptoms suggestive of hyperventilation have been observed repeatedly. Both hypocapnia and the hyperpnea that often accompanies it have adverse effects on asthma and can lead to symptom exacerbations. Beyond its initial face validity, anecdotal and clinical reports, and the higher comorbidity of asthma with panic disorder (patients who often show lower PCO2 levels), the evidence for an emotional origin of hypocapnia in asthma is not conclusive. More research is needed on emotion and hyperventilation in asthma patients’ daily lives and in periods of symptom exacerbation. At this point, it is more adequate to address hyperventilation in asthma simply as a nonadaptive breathing behavior that can be targeted by adequate behavioral training.
4. Therapeutic Capnography
Reversing hypocapnia with the goal of achieving normocapnic levels has long been hypothesized to be beneficial (e.g., Laffey & Kavanagh, 2002). Although it seems palpable that interventions aimed at reversing hypocapnic states would validate their efficacy by means of objective measurements of CO2, this has rarely been done (Meuret et al., 2003). Thus, evaluating the effectiveness of most breathing trainings is greatly complicated by the lack of the most central measure, PCO2. One of the reasons for this obvious limitation was likely the lack of ecological devices. However, recent technological advances in light, user-friendly ambulatory capnometry equipment have opened up new avenues for the development and implementation of therapeutic capnography. In the following, we review the methodology, clinical application, and efficacy of outcome studies aimed at normalizing hypocapnic breathing.
4.1 Therapeutic Capnography for Panic Disorder
4. 1.1. Traditional breathing training for panic disorder
Given that respiratory dysregulation appears to be central and perhaps an etiologic feature in a considerable percentage of patients suffering from panic disorder, interventions specifically targeting respiratory dysregulation may be particularly effective. However, the few studies aimed at testing the efficacy of traditional breathing training (Craske et al., 1997; Schmidt et al., 2000) have neither targeted nor assessed PCO2 as a key indicator of dysregulation. In contrast, the respiratory instructions taught in these studies, such as teaching patients to breathe slower (e.g., Craske et al., 1997; Schmidt et al., 2000), have been shown to perpetuate hyperventilation due to compensatory deeper breathing and thus intensify panic symptoms (e.g., Conrad et al., 2007; Meuret et al., 2003). Likewise, instructions such as “Take a deep breath!” or “Breathe deeply!” can only exacerbate hypocapnia and related symptoms. Not surprisingly, results on the efficacy of breathing training as the sole treatment or as a combined intervention are mixed. While some reports suggest clear benefits of traditional breathing training (Franklin, 1989; Bonn et al., 1984; Hibbert & Chan, 1989), no additive benefits were found in other studies (Craske et al., 1997; Schmidt et al., 2000) (see Meuret et al., 2003 for a detailed review).
4. 1.2. Early approaches to treating hypocapnia
Until recently, systematic research on the implementation and evaluation of therapeutic capnometry for PD or other conditions affected by hypocapnia has been largely absent from the literature. A number of early studies that have considered the utility of measuring or changing PCO2 levels during breathing training demonstrated therapeutic benefits. Among the first to use feedback of PCO2 as a therapeutic tool were Folgering and colleagues in the early 1980s (Folgering et al., 1980; van Doorn et al., 1982). Over the course of 7 weeks, patients who suffered from hyperventilation syndrome were taught to increase hypocapnic PCO2 levels during their treatment session using a two-channel chart feedback recorder. Significant and sustained increases in PCO2, from approximately 32 to 39 mmHg, were observed in patients undergoing breathing training plus PCO2 feedback as compared to patients only received training in regulating their respiration. Similarly, Grossman and colleagues (Grossman et al., 1985) provided PCO2 feedback for in-session training to patients suffering from chronic hyperventilation, demonstrating significant improvements in both symptoms and respiration. The debate surrounding the hyperventilation syndrome may have contributed to the lack of replication of these promising early attempts in treating chronic hypocapnic breathing.
In an early study with panic patients, hypocapnic levels were assessed but not modified before and following respiratory training (Salkovskis, Jones, & Clark, 1986). The authors reported notable normalizations in PCO2 (mean 41.5 mm Hg) from initially hypocapnic levels (mean 35 mmHg).
4. 1.3. Capnometry-assisted breathing training for panic
CART was developed to address the shortcoming of traditional breathing training (see above, 4.1.1). In such, CART directly targets respiratory dysregulations, in particular hypocapnia (Meuret et al., 2001; 2008; in press). This biobehavioral intervention is a brief, four-week training that uses immediate feedback of end-tidal PCO2 (portable capnometry) to teach patients how to raise hypocapnic levels of PCO2 and thereby gain control over dysfunctional respiratory patterns and associated panic symptoms (e.g., shortness of breath, dizziness).
Feedback methodolology
CART takes advantage of recent developments in ambulatory capnography. The direct feedback of the core parameter, PCO2, in addition to measures such as respiratory rate and oxygen saturation, provides both asthma and anxiety patients with a unique insight into their physiology at different times of day, emotional states, and situations. The latter appears crucial as it allows patients to directly test whether fears such as suffocating are indeed a reflection of their physiological status or rather a catastrophic misconception. Furthermore, while panic patients tend to be hypersensitive to bodily sensations and interpret them in a catastrophic fashion (Clark, 1986), the opposite can be true for patients with asthma. Introspective awareness may be altered and patients are no longer able to detect deteriorations in their physiological state.
Another beneficial aspect of portable capnometry is the assessment of treatment compliance. Most behavioral interventions build on the premise that between-session exercises are a fundamental ingredient to treatment success. Yet compliance and progress have been rarely measured outside the therapist’s office. However, self-modification of physiological parameters, in particular, require more than in-session “snap-shots.” Thus, monitoring throughout therapy can help health professionals tailor the treatment to the patient’s individual needs.
Intervention components
Techniques for normalizing PCO2 levels and regularizing respiration rate and rhythm comprise twice daily, 15-minute between-session exercises. Each exercise consists of three parts: (A) a baseline period during which patients sit quietly and relaxed with their eyes closed for two minutes, (B) a 10-minute paced breathing period during which patients monitor their PCO2 and respiratory rate, and (C) a five-minute transfer phase without pacing tones but with feedback of their PCO2 and respiratory rate. Audio recordings announce timing and instructions of these phases as well as present the pacing tones, which are modulated to correspond to a respiratory rate of 13 breaths per minute in the first treatment week, and rates of 11, 9, and 6 breaths per minute in successive weeks.
Evidence for efficacy and modality-specific mediation from clinical trials
In two randomized controlled studies, 4 weeks of CART led to sustained increases in PCO2 levels and significant reductions in panic symptom severity and frequency (Meuret et al., 2008; Meuret et al., in press). These reductions were comparable to 13 sessions of CBT (Barlow et al., 2000) or brief cognitive skill training (Meuret et al., in press). Furthermore, longitudinal mediation analyses indicated that changes in PCO2 mediated and preceded changes in fear of bodily sensations (Meuret et al., 2009) and cognitive reappraisal (Meuret et al., in press). In addition, bi-directional relations were found for cardio-respiratory changes to mediate changes in self-reported symptoms during in-vivo exposure and vice versa (Seidel et al., 2009). Mediational and temporal analyses further demonstrated that in patients who received CART, changes in PCO2 unidirectionally mediated and preceded changes in perceived emotional control. Strikingly, similar processes were also observed in patients undergoing treatment in cognitive training, in that PCO2 mediated changes in panic symptom severity (Meuret et al., in press).
Hyper- or hypocapnia training?
Following Klein’s (1993) argument that panic patients hyperventilate to avoid the experience of the CO2 increases that trigger their low- threshold or hypersensitive suffocation alarm system, it could be speculated whether hypocapnia training may actually be beneficial for these patients (Roth, 2010). Preliminary findings of a study testing hypercapnic versus hypocapnic breathing training indeed indicate similar reductions in panic symptom severity for both trainings. This may be viewed as questioning the idea of increases in PCO2 levels mediating panic severity improvement. However, outcome equality is not indicative of the same underlying mechanism, as demonstrated in our recent study showing equivalence in outcome for hypoventilation versus cognitive training (Meuret et al., in press). Both hypo- and hyperventilation training could be interpreted as beneficial in light of the suffocation alarm theory: While hyperventilation could help patients avoid the feared suffocation symptoms, hypoventilation may serve to desensitize a hypersensitive suffocation alarm system. Thus, speculations about expectancy as the common underlying mechanism (Roth, 2010) are probably premature. Tests of mediation and temporal precedence among the proposed mediators and outcome would be needed to establish more concrete evidence (Kazdin, 2007).
4.2. Therapeutic Capnography for Asthma
Breathing training and biofeedback have long been advocated as an adjunctive treatment in asthma (Ritz & Roth, 2003; Ritz et al., 2004). The Buteyko breathing technique has been proposed as an intervention to improve asthma pathophysiology and patients’ quality of life (Stalmatzki, 1999). The aim is to train slower and shallower breathing to increase PCO2 levels with the assumption that low levels are the cause of a number of autonomic, endocrine and metabolic disturbances, which contribute to asthma pathophysiology. In three controlled trials, improvements in quality of life and/or reduced bronchodilator use were observed (Bowler et al., 1998; Cooper, et al., 2003; Opat, et al., 2000). Only one study included PCO2 measurements, but was only able to demonstrate decreases in minute ventilation in the Buteyko breathing training group. Thus, no evidence for the main treatment rationale of the technique has been presented as of yet.
Therefore, we recently adapted the CART training for asthma patients (Meuret, et al., 2007; Ritz et al., 2009). Patients with predominantly mild persistent to moderate asthma volunteered in a pilot study, which was presented as an adjunctive breathing training supplementing their existing medical treatment. They were encouraged to reduce their bronchodilator use, but to keep their other asthma medication constant. The techniques and protocol largely followed those outlined for panic patients (see 4.1.3), but in contrast to the application for panic, the therapy rationale outlined general as well as asthma-specific adverse effects of overbreathing or hypocapnia. In addition to using the capnometer, patients monitored their lung function and symptoms using a hand-held electronic spirometer with diary functions for ratings of symptoms and mood. Measurements of lung function and symptoms were scheduled before and after each exercise, and during the five therapist-guided sessions.
Twelve asthma patients were randomly assigned to an immediate 4-week treatment group or waiting list control. Following the 4-week training, patients in the treatment group (n=8) showed stable increases in PCO2 and reductions in respiration rate. These changes were sustained at a 2-month follow-up visit. Symptom frequency and distress reduced, reported asthma control increased, and mean diurnal peak expiratory flow variability (as a distal marker of airway hyperreactivity) decreased significantly in the treatment group. Little change was found in parameters of basal lung function. In control patients (N=4), symptoms and physiological parameters remained stable during the 4-week wait period. Credibility and acceptance of the training was very high for the treatment group. Patients reported that the training gave them greater voluntary control over their asthma symptoms, particularly over coughing. In a further analysis of this data set (Ritz et al., 2009), we found that the improvements in PCO2, respiration rate, and symptoms were gradual across the four weeks of training, suggesting that the full 4-week training should be applied for best effects.
We are currently testing the benefits of this training for asthma patients in a larger clinical trial sponsored by the National Heart, Lung and Blood Institute (NHLBI). This will include meditational and temporal analyses similar to the clinical trials in panic patients (see 4.1.3). A particular focus will be on changes in PCO2 and inflammation as mediators of control of asthma.4
5. General conclusion
Since its first introduction to panic and asthma treatment, breathing training has continued to evolve. However, lay conceptions about the benefits of individual breathing techniques (“deep breathing”) and a lack of mechanistic studies have impeded progress in this area for some time. The recently developed therapeutic capnometry for panic and asthma offer the advantage of a plausible and testable psychophysiological rationale for the expected treatment effects. For panic treatment, this is a clear advantage over cognitive-behavior therapy, a more established intervention that is plausible in its rationale, but cannot be falsified (Roth et al., 2005). Initial findings in patients with panic disorder suggest a specific effect of raising CO2 levels by therapeutic capnometry. On the other hand, mechanistic studies in asthma are still underway. The potential contribution of breathing training to psychological interventions in PD/A could be determined in dismantling studies. Alternatively, capnometry-assisted breathing training could also serve as a stand-alone treatment for PD, as suggested by the effect sizes of the first studies. Differential suitability of the techniques for various subgroups of panic patients needs to be determined. Similarly, given that the pathophysiology of asthma is heterogeneous, future research needs to determine whether CART could serve as a general adjunctive treatment for asthma patients or would be more suitable for patient subgroups. However, in contrast to panic disorder treatment, the biofeedback technique cannot be recommended as a stand-alone treatment at this point, because state-of-the art treatment of asthma currently requires anti-inflammatory medication in most cases (NHLBI, 2007).
As with any other behavioral treatment, the question of specificity vs. nonspecificity of the training will be an enduring concern. A case could be made that nonspecific effects such as therapeutic attention or persuasive treatment rationales inducing optimistic expectancies, perceptions of control, and feelings of empowerment drive most of the patients’ improvements (Roth, 2010). While this assumption could be rigorously tested in asthma patients by incorporating indicators of change in airway pathophysiology and management behaviors, demonstrating specificity in panic disorder as a psychological disorder might be a more difficult task. However, good progress has been made in testing mediators of improvement in panic disorder for CART versus cognitive training. As discussed in 4.1.3, for CART training, PCO2 unidirectionally mediated and preceded changes in fear of bodily sensations (Meuret et al., 2009), cognitive reappraisal, and perceived emotional control (Meuret et al., in press). While the capnometry biofeedback technique implies conscious processing of core respiratory values, patients’ perceptions of success also could have driven some of these associations. However, changes in PCO2 that occurred in cognitive skills training unsystematically also mediated changes in panic symptom severity. Because these patients were unaware of their PCO2 levels, the effects of CART seem unlikely to be explained by simple nonspecific expectancy effects.
This review focused on the empirical evidence on hypocapnia and the therapeutic application of capnometry to the treatment of panic and asthma. Speculations about central nervous system pathways involved in the adverse effects of hypocapnia in these disorders and in the therapeutic effects of CART would go beyond the scope of this review. Suffice to say that the literature offers a number of points of departure for such an endeavor. For example, Gorman et al. (2000) and Abelson et al. (2001) attempted to understand panic as a special case of activation of a general “fear-network” including hypothalamic sites, as well as the amygdala, hippocampus, and medial prefrontal cortex. Klein (2002) speculated about a specific role of the cerebellum as a structure involved in activation of primal affects such as air hunger, thirst, hunger, and satiety. The cerebellum may be particularly interesting for the paced-breathing based CART, given its role in assisting guided movements (Jueptner & Weiller, 1998). Without doubt, recent findings and advances in the methodology of brain imaging of respiratory regulation and dyspnea (Evans, 2010) will be critical in the further exploration of such pathways in both panic disorder and asthma.
In conclusion, therapeutic capnometry offers new approaches to the behavioral treatment of panic and asthma, and a focus on breathing-related parameters such as PCO2 may offer novel insights into psychophysiological pathways to treatment success in these debilitating disorders.
Acknowledgments
Preparation of this manuscript was partly funded by a National Institutes of Health/National Heart, Lung and Blood Institute grant, R01 HL-089761 (to both authors), and the generous support of the Beth and Russell Siegelman Foundation (Meuret).
We gratefully acknowledge the role of Dr. Walton T. Roth in inspiring and mentoring the authors’ pursuit of respiratory psychophysiology in clinical psychology research. We thank Dr. Karleyton Evans for valuable suggestions on an earlier version of this manuscript and Erica S. Ayala and Ashton Jeter for their help in the manuscript preparation.
Footnotes
It should be noted that there are caveats associated with the study of Hornsveld et al. (1996), among which are the experimental methodology of titrating CO2 manually, exclusive reliance on self report, and transcutaneous monitoring of PCO2 levels. As mentioned above, PtCO2 is not sufficiently precise for assessing momentary PCO2 changes (Sanders et al., 1994). Moreover, the study lacked acid-base balance assessments to classify any of the enrolled subjects as chronic hyperventilators (Jack et al., 2004).
Klein (1993) did not directly identify chemoreceptors as one major component of the proposed suffocation alarm system. Rather, he employed the term detector, which implies an earlier level of sensory processing, if not the initial transduction process at the receptor level. He also alluded to the medulla as the anatomical location most likely implicated. More specifically, in work leading up to the suffocation alarm theory, Klein, Gorman and colleagues (Gorman et al., 1988; Papp et al., 1993) clearly speculated about the involvement of hypersensitive chemoreceptors in panic patients’ response to CO2. Thus, the theory has been commonly interpreted as identifying chemoreceptors as the crucial site of derangement (Roth et al., 2005; Smoller et al., 1996). Consequently, experimental studies have explored chemoreceptor sensitivities or thresholds (Pain et al., 1988; Papp et al., 1995; Katzman et al., 2002). The lack of distinction between low threshold and high sensitivity points to an additional vagueness in the conceptualization of the derangements of the proposed system. More recently, Klein (2002) explicitly takes a wider perspective on the suffocation alarm system by stating: “this theory goes well beyond a theory of a sole abnormality in peripheral, afferent, CO2-responsive pathways to hypothesize that a hyper-reactivity of a common human adaptive mechanism—the suffocation alarm system” (p.567). This formulation is more in line with recent research demonstrating an overlap of cortico-limbic circuitries with those processing dyspnea (e.g., Evans et al., 2002).
Gorman et al. (2004) also found that cognitive behavior therapy reduced the anxiety response to CO2 challenge and panic incidence, but respiratory responses were reported unchanged by treatment. However, when inspecting the physiological challenge responses of healthy controls that were used as a comparison group, they show strong increases in minute ventilation closely resembling those of panic patients, or those of panicking patients and healthy controls in other studies (e.g., Gorman et al., 2001). The healthy controls thus closely resembled panic patients in that they showed a substantial respiratory response to CO2 challenge. Anxiety levels were lower on average in this group, but no panic rates were reported. In addition, significant (or almost significant, p=.051) decreases in all respiratory parameters were observed in both groups from initial to post-treatment 7% CO2 challenges (or at challenge repetition in controls). Nevertheless, the authors interpret their findings as a clear indication of a change in the perception but not in respiratory physiology.
Heart rate variability (HRV) biofeedback as a different breathing-base approach to treating asthma has been proposed by Lehrer et al. (2004). Patients learn to breathe slower than normal (around 6 breaths/min), leading to an overlap of high-frequency HRV, which is respiration-related, and low-frequency HRV, which is thought to be driven particularly by activity of the baroreflex. The authors have demonstrated reduced asthma symptomatology, medication needs, and respiratory resistance in a larger clinical trial. The mechanism of action of such changes is not well explored (Ritz et al., 2004). Although the training aims to entrain the baroreflex, and increases in baroreflex sensitivity have been postulated as a key to general improvements in the autonomic regulation, this clinical trial was not able to demonstrate lasting increases in this parameter. Also, because blood gas levels had not been assessed, a potential role of CO2 changes during this training could not be explored.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abelson JL, Nesse RM, Weg JG, Curtis GC. Respiratory psychophysiology and anxiety: cognitive intervention in the doxapram model of panic. Psychosomatic Medicine. 1996;58:302–313. doi: 10.1097/00006842-199607000-00002. [DOI] [PubMed] [Google Scholar]
- Abelson JL, Weg JG, Nesse RM, Curtis GC. Persistent respiratory irregularity in patients with panic disorder. Biological Psychiatry. 2001;49:588–595. doi: 10.1016/s0006-3223(00)01078-7. [DOI] [PubMed] [Google Scholar]
- Alexander JK, West JR, Wood JA, Richards DW. Journal of Clinical Investigation. 1955;34:511–32. doi: 10.1172/JCI103100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abrams K, Rassovsky Y, Kushner MG. Evidence for respiratory and nonrespiratory subtypes in panic disorder. Depression and Anxiety. 2006;23:474–81. doi: 10.1002/da.20179. [DOI] [PubMed] [Google Scholar]
- Alpers HW, Wilhelm FH, Roth WT. Psychophysiological measures during exposure in driving phobics. Journal of Abnormal Psychology. 2005;114:126–139. doi: 10.1037/0021-843X.114.1.126. [DOI] [PubMed] [Google Scholar]
- Anderson SD. Is there a unifying hypothesis for exercise-induced asthma? The Journal of Allergy and Clinical Immunology. 1984;73:660–665. doi: 10.1016/0091-6749(84)90301-4. [DOI] [PubMed] [Google Scholar]
- Antony MM, Brown TA, Barlow DH. Response to hyperventilation and 5.5% CO2 inhalation of subjects with types of specific phobia, panic disorder, or no mental disorder. The American Journal of Psychiatry. 1997;154:1089–1095. doi: 10.1176/ajp.154.8.1089. [DOI] [PubMed] [Google Scholar]
- Ayala ES, Meuret AE, Ritz T. Confrontation with blood and disgust stimuli precipitates respiratory dysregulation in blood-injection-injury phobia. Biological Psychology. 2010;84:88–97. doi: 10.1016/j.biopsycho.2010.02.004. [DOI] [PubMed] [Google Scholar]
- Barlow DH. Anxiety and its disorders: The nature and treatment of anxiety and panic. 2. Guilford Press; New York: 2002. [Google Scholar]
- Barlow DH, Gorman JM, Shear MK, Woods SW. Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: A randomized controlled trial. Journal of the American Medical Association. 2000;283:2573–2574. doi: 10.1001/jama.283.19.2529. [DOI] [PubMed] [Google Scholar]
- Bass C. Hyperventilation syndrome: a chimera? Journal of Psychosomatic Research. 1997;42:421–426. doi: 10.1016/s0022-3999(96)00365-0. [DOI] [PubMed] [Google Scholar]
- Bass C, Gardner WN. Respiratory and psychiatric abnormalities in chronic symptomatic hyperventilation. BMJ. 1985;290:1387–1390. doi: 10.1136/bmj.290.6479.1387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck JG, Ohtake PJ, Shipherd JC. Exaggerated anxiety is not unique to CO2 in panic disorder: a comparison of hypercapnic and hypoxic challenges. Journal of Abnormal Psychology. 1999;108:473–482. doi: 10.1037//0021-843x.108.3.473. [DOI] [PubMed] [Google Scholar]
- Belloch A, Perpiñá MJ, Pascual LM, Martinez M, De Diego A. Subjective symptomatology of asthma: validation of the asthma symptom checklist in an outpatient Spanish population. Journal of Asthma. 1997;34:509–519. doi: 10.3109/02770909709055395. [DOI] [PubMed] [Google Scholar]
- Biber B, Alkin T. Panic disorder subtypes: differential responses to CO2 challenge. Am J Psychiatry. 1999;156:739–44. doi: 10.1176/ajp.156.5.739. [DOI] [PubMed] [Google Scholar]
- Blechert J, Michael T, Grossman P, Lajtman M, Wilhelm FH. Autonomic and respiratory characteristics of posttraumatic stress disorder and panic disorder. Psychosomatic Medicine. 2007;69:935–943. doi: 10.1097/PSY.0b013e31815a8f6b. [DOI] [PubMed] [Google Scholar]
- Blechert J, Wilhelm FH, Meuret AE, Wilhelm EM, Roth WT. Respiratory, autonomic, and experiential responses to repeated inhalations of 20% CO2 enriched air in panic disorder, social phobia, and healthy controls. Biological Psychology. 2010;84:204–111. doi: 10.1016/j.biopsycho.2010.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boiten FA, Frijda NH, Wientjes CJ. Emotions and respiratory patters: Review and critical analysis. International Journal of Psychophysiology. 1994;17:103–128. doi: 10.1016/0167-8760(94)90027-2. [DOI] [PubMed] [Google Scholar]
- Bonn JA, Readhead CP, Timmons BH. Enhanced adaptive behavioural response in agoraphobic patients pretreated with breathing retraining. Lancet. 1984;2:665–669. doi: 10.1016/s0140-6736(84)91226-1. [DOI] [PubMed] [Google Scholar]
- Briggs AC, Strech DD, Brandon S. Subtyping of panic disorder by symptom profile. Br J Psychiatry. 1993;163:201–209. doi: 10.1192/bjp.163.2.201. [DOI] [PubMed] [Google Scholar]
- Bowler SD, Green AG, Mitchell CA. Buteyko breathing techniques in asthma: A blinded randomised controlled trial. The Medical Journal of Australia. 1998;169:575–578. doi: 10.5694/j.1326-5377.1998.tb123422.x. [DOI] [PubMed] [Google Scholar]
- Brooks CM, Richards JM, Jr, Bailey WC, Martin B, Windsor RA, Soong SJ. Subjective symptomatology of asthma in an outpatient population. Psychosomatic Medicine. 1989;51:102–108. doi: 10.1097/00006842-198901000-00010. [DOI] [PubMed] [Google Scholar]
- Bruton A, Holgate ST. Hypocapnia and asthma: A mechanism for breathing retraining? Chest. 2005;127:1808–1811. doi: 10.1378/chest.127.5.1808. [DOI] [PubMed] [Google Scholar]
- Butler J, Caro CG, Alcala R, Dubois AB. Physiological factors affecting airway resistance in normal subjects and in patients with obstructive respiratory disease. The Journal of Clinical Investigation. 1960;39:584–591. doi: 10.1172/JCI104071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr RE. Panic disorder and asthma: Causes, effects and research implications. Journal of Psychosomatic Research. 1998;44:43–52. doi: 10.1016/s0022-3999(97)00137-2. [DOI] [PubMed] [Google Scholar]
- Clark DM. A cognitive approach to panic. Behaviour Research and Therapy. 1986;24:461–470. doi: 10.1016/0005-7967(86)90011-2. [DOI] [PubMed] [Google Scholar]
- Clarke PS, Gibson JR. Asthma hyperventilation and emotion. Australian Family Physician. 1980;9:715–719. [PubMed] [Google Scholar]
- Conrad A, Müller A, Doberenz S, Kim S, Meuret AE, Wollburg E, Roth WT. Psychophysiological effects of breathing instructions for stress management. Applied Psychophysiology and Biofeedback. 2007;32:89–98. doi: 10.1007/s10484-007-9034-x. [DOI] [PubMed] [Google Scholar]
- Cooper S, Oborne J, Newton S, et al. Effects of two breathing exercises (Buteyko and Pranayama) in asthma: A randomized controlled trial. Thorax. 2003;58:674–679. doi: 10.1136/thorax.58.8.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coplan JD, Goetz R, Klein DF, Papp LA, Fyer AJ, Liebowitz MR, Davies SO, Gorman JM. Plasma cortisol concentrations preceding lactate-induced panic. Psychological, biochemical, and physiological correlates. Archives of General Psychiatry. 1998;55:130–136. doi: 10.1001/archpsyc.55.2.130. [DOI] [PubMed] [Google Scholar]
- Coryell W. Hypersensitivity to carbon dioxide as a disease-specific trait marker. Biological Psychiatry. 1997;41:259–263. doi: 10.1016/s0006-3223(97)87457-4. [DOI] [PubMed] [Google Scholar]
- Craske MG, Rowe M, Lewin M, Noriega-Dimitri R. Interoceptive exposure versus breathing retraining within cognitive-behavioural therapy for panic disorder with agoraphobia. British Journal of Clinical Psychology. 1997;36:85–99. doi: 10.1111/j.2044-8260.1997.tb01233.x. [DOI] [PubMed] [Google Scholar]
- Davis MS, Freed AN. Repetitive hyperpnoea causes peripheral airway obstruction and eosinophillia. The European Respiratory Journal. 1999;14:57–62. doi: 10.1034/j.1399-3003.1999.14a11.x. [DOI] [PubMed] [Google Scholar]
- Davis MS, Freed AN. Repeated hyperventilation causes peripheral airways inflammation, hyperreactivity, and impaired bronchodilation in dogs. American Journal of Respiratory and Critical Care Medicine. 2001;164:785–789. doi: 10.1164/ajrccm.164.5.2003081. [DOI] [PubMed] [Google Scholar]
- Davis MS, Schofield B, Freed AN. Repeated peripheral airway hypernea causes inflammation and remodeling in dogs. Medicine and Science in Sports and Exercise. 2003;35:608–616. doi: 10.1249/01.MSS.0000058660.88987.A0. [DOI] [PubMed] [Google Scholar]
- De Peuter S, Van Diest I, Lemaigre V, Li W, Verleden G, Demedts M, Van den Bergh O. Can subjective asthma symptoms be learned? Psychosomatic Medicine. 2005;67:454–461. doi: 10.1097/01.psy.0000160470.43167.e2. [DOI] [PubMed] [Google Scholar]
- Demeter SL, Cordasco EM. Hyperventilation syndrome and asthma. American Journal of Medicine. 1986;81:989–994. doi: 10.1016/0002-9343(86)90393-1. [DOI] [PubMed] [Google Scholar]
- Evans K. Cortico-limbic circuitry and the airways: Insights from functional neuroimaging of respiratory afferents and efferents. Biological Psychology. 2010;84:13–25. doi: 10.1016/j.biopsycho.2010.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans KC, Banzett RB, Adams L, McKay L, Frackowiak RS, Corfield DR. BOLD fMRI identifies limbic, paralimbic, and cerebellar activation during air hunger. J Neurophysiol. 2002;88:1500–11. doi: 10.1152/jn.2002.88.3.1500. [DOI] [PubMed] [Google Scholar]
- Fish JE, Ankin MG, Kelly JF, Peterman VI. Regulation of bronchomotor tone by lung inflation in asthmatic and nonasthmatic subjects. Journal of Applied Physiology. 1981;50:1079–1086. doi: 10.1152/jappl.1981.50.5.1079. [DOI] [PubMed] [Google Scholar]
- Fishman SM, Carr DB, Beckett A, Rosenbaum JF. Hypercapneic ventilatory response in patients with panic disorder before and after alprazolam treatment and in pre- and postmenstrual women. J Psychiatr Res. 1994;28:65–70. doi: 10.1016/0022-3956(94)90027-2. [DOI] [PubMed] [Google Scholar]
- Folgering H, Lenders J, Rosier I. Biofeedback control of Paco2, a prospective therapy in hyperventilation. In: Herzog H, et al., editors. Progress in respiratory research, vol. 14: Asthma. Karger; Basel: 1980. pp. 26–30. [Google Scholar]
- Franklin JA. A 6-year follow-up of the effectiveness of respiratory retraining, in-situ isometric relaxation, and cognitive modification in the treatment of agoraphobia. Behavior Modification. 1989;13:139–167. doi: 10.1177/01454455890132001. [DOI] [PubMed] [Google Scholar]
- Fredberg JJ. Airway smooth muscle in asthma: flirting with disaster. European Respiratory Journal. 1998;12:1252–1256. doi: 10.1183/09031936.98.12061252. [DOI] [PubMed] [Google Scholar]
- Freire RC, Lopes FL, Valença AM, Nascimento I, Veras AB, Mezzasalma MA, de-Melo-Neto VL, Zin WA, Nardi AE. Panic disorder respiratory subtype: a comparison between responses to hyperventilation and CO2 challenge tests. Psychiatry Research. 2008;15:307–10. doi: 10.1016/j.psychres.2007.07.015. [DOI] [PubMed] [Google Scholar]
- Fried R, Rubin SR, Carlton RM, Fox MC. Behavioral control of intractable idiopathic seizures: Self-regulation of end-tidal carbon dioxide. Psychosomatic Medicine. 1984;46:315–331. doi: 10.1097/00006842-198407000-00002. [DOI] [PubMed] [Google Scholar]
- Fried R. The Psychology and Physiology of Breathing. New York: Plenum Press; 1993. [Google Scholar]; Meuret AE. Therapeutic use of ambulatory capnography. In: Gravenstein J, Jaffe M, Paulus D, editors. Capnography, Clinical Aspects. 2. Cambridge: Cambridge University Press; (in press) [Google Scholar]
- Fujimori K, Satoh M, Arakawa M. Ventilatory response to continuous incremental changes in respiratory resistance in patients with mild asthma. Chest. 1996;109:1525–1531. doi: 10.1378/chest.109.6.1525. [DOI] [PubMed] [Google Scholar]
- Gardner WN. The pathophysiology of hyperventilation disorders. Chest. 1996;109:516–534. doi: 10.1378/chest.109.2.516. [DOI] [PubMed] [Google Scholar]
- Gardner WN, Bass C, Moxham J. Recurrent hyperventilation tetany due to mild asthma. Respiratory Medicine. 1992;86:349–351. doi: 10.1016/s0954-6111(06)80036-3. [DOI] [PubMed] [Google Scholar]
- Garssen B, Buikhuisen M, van Dyck R. Hyperventilation and panic attacks. The American Journal of Psychiatry. 1996;153:513–518. doi: 10.1176/ajp.153.4.513. [DOI] [PubMed] [Google Scholar]
- Gayrard P, Orehek J, Grimaud C, Charpin J. Bronchoconstrictor effects of a deep inspiration in patients with asthma. The American Review of Respiratory Disease. 1975;111:433–439. doi: 10.1164/arrd.1975.111.4.433. [DOI] [PubMed] [Google Scholar]
- Goodwin RD. Asthma and anxiety disorders. Advances in Psychosomatic Medicine. 2003;24:51–71. doi: 10.1159/000073780. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Martinez J, Coplan JD, Kent J, Kleber M. The effect of successful treatment on the emotional and physiological response to carbon dioxide inhalation in patients with panic disorder. Biol Psychiatry. 2004;56:862–7. doi: 10.1016/j.biopsych.2004.08.016. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Fyer MR, Goetz R, Askanazi J, Liebowitz MR, Fyer AJ, Kinney J, Klein DF. Ventilatory physiology of patients with panic disorder. Archives of General Psychiatry. 1988;45:31–39. doi: 10.1001/archpsyc.1988.01800250035006. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Papp LA, Coplan JD, Martinez JM, Lennon S, Goetz RR, Ross D, Klein DF. Anxiogenic effects of CO2 and hyperventilation in patients with panic disorder. The American Journal of Psychiatry. 1994;151:547–553. doi: 10.1176/ajp.151.4.547. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Uy J. Respiratory physiology and pathological anxiety. General Hospital Psychiatry. 1987;9:410–419. doi: 10.1016/0163-8343(87)90050-8. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Cohen BS, Liebowitz MR, Fyer AJ, Ross D, Davies SO, Klein DF. Blood gas changes and hypophosphatemia in lactate-induced panic. Archives of General Psychiatry. 1986;43:1067–1071. doi: 10.1001/archpsyc.1986.01800110053007. [DOI] [PubMed] [Google Scholar]
- Gorman JM, Kent J, Martinez J, Browne S, Coplan J, Papp LA. Physiological changes during carbon dioxide inhalation in patients with panic disorder, major depression, and premenstrual dysphoric disorder: evidence for a central fear mechanism. Archives of General Psychiatry. 2001;8:125–31. doi: 10.1001/archpsyc.58.2.125. [DOI] [PubMed] [Google Scholar]
- Greisen G, Munck H, Lou H. Severe hypocarbia in preterm infants and neurodevelopmental deficit. Acta Paediatrica Scandinavica. 1987;76:401–404. doi: 10.1111/j.1651-2227.1987.tb10489.x. [DOI] [PubMed] [Google Scholar]
- Grossman P. Respiration, stress, and cardiovascular function. Psychophysiology. 1983;20:284–300. doi: 10.1111/j.1469-8986.1983.tb02156.x. [DOI] [PubMed] [Google Scholar]
- Grossman P, de Swart JC, Defares PB. A controlled study of a breathing therapy for treatment of hyperventilation syndrome. Journal of Psychosomatic Research. 1985;29:49–58. doi: 10.1016/0022-3999(85)90008-x. [DOI] [PubMed] [Google Scholar]
- Hasler G, Gergen PJ, Kleinbaum DG, Ajdacic V, Gamma A, Eich D, Rössler W, Angst J. Asthma and panic in young adults: a 20-year prospective community study. American Journal of Respiratory and Critical Care Medicine. 2005;171:1224–1230. doi: 10.1164/rccm.200412-1669OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hegel MT, Ferguson RJ. Psychophysiological assessment of respiratory function in panic disorder: evidence for a hyperventilation subtype. Psychosomatic Medicine. 1997;59:224–30. doi: 10.1097/00006842-199705000-00003. [DOI] [PubMed] [Google Scholar]
- Herxheimer H. Hyperventilation asthma. Lancet. 1946;1:83–87. doi: 10.1016/s0140-6736(46)91225-1. [DOI] [PubMed] [Google Scholar]
- Hibbert GA, Chan M. Respiratory control: its contribution to the treatment of panic attacks. A controlled study. British Journal of Psychiatry. 1989;154:232–236. doi: 10.1192/bjp.154.2.232. [DOI] [PubMed] [Google Scholar]
- Hibbert G, Pilsbury D. Hyperventilation in panic attacks. Ambulant monitoring of transcutaneous carbon dioxide. British Journal of Psychiatry. 1988;153:76–80. doi: 10.1192/bjp.153.1.76. [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Meuret AE, Rosenfield D, Suvak MK, Barlow DH, Gorman JM, Shear MK, Woods SW. Preliminary evidence for cognitive mediation during cognitive-behavioral therapy of panic disorder. Journal of Consulting and Clinical Psychology. 2007;75:374–379. doi: 10.1037/0022-006X.75.3.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt PE, Andrews G. Hyperventilation and anxiety in panic disorder, social phobia, GAD, and normal controls. Behaviour Research and Therapy. 1989;27:453–460. doi: 10.1016/0005-7967(89)90016-8. [DOI] [PubMed] [Google Scholar]
- Hormbrey J, Jacobi MS, Patil CP, Saunders KB. CO2 response and pattern of breathing in patients with symptomatic hyperventilation, compared to asthmatic and normal subjects. The European Respiratory Journal. 1988;1:846–851. [PubMed] [Google Scholar]
- Hornsveld HK, Garssen B, Dop MJ, van Spiegel PI, de Haes JC. Double-blind placebo-controlled study of the hyperventilation provocation test and the validity of the hyperventilation syndrome. Lancet. 1996;348:154–158. doi: 10.1016/s0140-6736(96)02024-7. [DOI] [PubMed] [Google Scholar]
- Howell JBL. The hyperventilation syndrome: a syndrome under threat? Thorax. 1997;52(Suppl 3):S30–34. doi: 10.1136/thx.52.2008.s30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isenberg SA, Lehrer PM, Hochron S. The effects of suggestion and emotional arousal on pulmonary function in asthma: A review and a hypothesis regarding vagal mediation. Psychosomatic Medicine. 1992;54:192–216. doi: 10.1097/00006842-199203000-00006. [DOI] [PubMed] [Google Scholar]
- Jack S, Rossiter HB, Pearson MG, Ward SA, Warburton CJ, Whipp BJ. Ventilatory responses to inhaled carbon dioxide, hypoxia, and exercise in idiopathic hyperventilation. American Journal of Respiratory and Critical Care Medicine. 2004;170:118–25. doi: 10.1164/rccm.200207-720OC. [DOI] [PubMed] [Google Scholar]
- Jain N, Puranik M, Lodha R, Kabra SK. Long-term management of asthma. Indian Journal of Pediatrics. 2001;68(Suppl 4):S31–41. [PubMed] [Google Scholar]
- Jueptner M, Weiller C. A review of differences between basal ganglia and cerebellar control of movements as revealed by functional imaging studies. Brain. 1998;121:1437–49. doi: 10.1093/brain/121.8.1437. [DOI] [PubMed] [Google Scholar]
- Katzman MA, Struzik L, Vijay N, Coonerty-Femiano A, Mahamed S, Duffin J. Central and peripheral chemoreflexes in panic disorder. Psychiatry Research. 2002;113:181–192. doi: 10.1016/s0165-1781(02)00238-x. [DOI] [PubMed] [Google Scholar]
- Kazdin AE. Mediators and mechanisms of change in psychotherapy research. Annual Review of Clinical Psychology. 2007;3:1–27. doi: 10.1146/annurev.clinpsy.3.022806.091432. [DOI] [PubMed] [Google Scholar]
- Kelsen SG, Fleegler B, Altose MD. The respiratory neuromuscular response to hypoxia, hypercapnia, and obstruction to airflow in asthma. American Review of Respiratory Disease. 1979;120:517–27. doi: 10.1164/arrd.1979.120.3.517. [DOI] [PubMed] [Google Scholar]
- Kinsman RA, Luparello T, O’Banion K, Spector S. Multidimensional analysis of the subjective symptomatology of asthma. Psychosomatic Medicine. 1973;35:250–267. doi: 10.1097/00006842-197305000-00008. [DOI] [PubMed] [Google Scholar]
- Klein DF. Prodromal symptoms in agoraphobia and panic disorder. American Journal of Psychiatry. 1989;146:812–814. doi: 10.1176/ajp.146.6.aj1466812. [DOI] [PubMed] [Google Scholar]
- Klein DF. False suffocation alarms, spontaneous panics, and related conditions. An integrative hypothesis. Archives of General Psychiatry. 1993;50:306–317. doi: 10.1001/archpsyc.1993.01820160076009. [DOI] [PubMed] [Google Scholar]
- Klein DF. Response differences of spontaneous panic and fear. Archives of General Psychiatry. 2002;59:567–569. doi: 10.1001/archpsyc.59.6.567. [DOI] [PubMed] [Google Scholar]
- Knapp PH. Psychosomatic aspects of bronchial asthma: A review. In: Cheren S, editor. Psychosomatic medicine: Theory, physiology, and practice. Vol. 2. International University Press; Innocence: 1989. pp. 503–564. [Google Scholar]
- Kroeze S, Van der Does AJ, Spinhoven P, Schot R, Sterk PJ, Van den Aardweg JG. Automatic negative evaluation of suffocation sensations in individuals with suffocation fear. Journal of Abnormal Psychology. 2005;114:466–470. doi: 10.1037/0021-843X.114.3.466. [DOI] [PubMed] [Google Scholar]
- Laffey JG, Kavanagh BP. Hypocapnia. New England Journal of Medicine. 2002;347:43–53. doi: 10.1056/NEJMra012457. [DOI] [PubMed] [Google Scholar]
- Lebowitz MD, Thompson HC, Strunk RC. Subjective psychological symptoms in outpatient asthmatic adolescents. Journal of Behavioral Medicine. 1981;4:439–449. doi: 10.1007/BF00846152. [DOI] [PubMed] [Google Scholar]
- Lehrer PM, Vaschillo E, Vaschillo B, Lu SE, Scardella A, Siddique M, Habib RH. Biofeedback treatment for asthma. Chest. 2004;126:352–61. doi: 10.1378/chest.126.2.352. [DOI] [PubMed] [Google Scholar]
- Ley R. Blood, breath and fears: A hyperventilation theory of panic attacks and agoraphobia. Clinical Psychology Review. 1986;5:271–285. [Google Scholar]
- Ley R. The many faces of Pan: psychological and physiological differences among three types of panic attacks. Behaviour Research and Therapy. 1992;30:347–357. doi: 10.1016/0005-7967(92)90046-j. [DOI] [PubMed] [Google Scholar]
- Ley R, Yelich G. Fractional end-tidal CO2 as an index of the effects of stress on math performance and verbal memory of test-anxious adolescents. Biological Psychology. 1998;49:83–94. doi: 10.1016/s0301-0511(98)00028-3. [DOI] [PubMed] [Google Scholar]
- Liebowitz MR, Gorman JM, Fyer AJ, Levitt M, Dillon D, Levy G, Appleby IL, Anderson S, Palij M, Davies SO, et al. Lactate provocation of panic attacks. II. Biochemical and physiological findings. Archives of General Psychiatry. 1985;42:709–719. doi: 10.1001/archpsyc.1985.01790300077010. [DOI] [PubMed] [Google Scholar]
- Lim TK, Pride NB, Ingram RH., Jr Effects of volume history during spontaneous and acutely induced air-flow obstruction in asthma. American Review of Respiratory Disease. 1987;135:591–596. doi: 10.1164/arrd.1987.135.3.591. [DOI] [PubMed] [Google Scholar]
- Lousberg H, Griez E, van den Hout MA. Carbon dioxide chemosensitivity in panic disorder. Acta Psychiatr Scand. 1988;77:214–8. doi: 10.1111/j.1600-0447.1988.tb05103.x. [DOI] [PubMed] [Google Scholar]
- Lum LC. Hyperventilation syndromes in medicine and psychiatry: A review. Journal of the Royal Society of Medicine. 1987;80:229–231. doi: 10.1177/014107688708000413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maddock RJ, Carter CS. Hyperventilation-induced panic attacks in panic disorder with agoraphobia. Biological Psychiatry. 1991;29:843–854. doi: 10.1016/0006-3223(91)90051-m. [DOI] [PubMed] [Google Scholar]
- Magarian GJ. Hyperventilation syndrome: infrequently recognized common expression of anxiety and stress. Medicine (Baltimore) 1982;61:219–236. [PubMed] [Google Scholar]
- Mahler DA, Faryniarz K, Lentine T, Ward J, Olmstead EM, O’Connor GT. Measurement of breathlessness during exercise in asthmatics. Predictor variables, reliability, and responsiveness. American Review of Respiratory Disease. 1991;144:39–44. doi: 10.1164/ajrccm/144.1.39. [DOI] [PubMed] [Google Scholar]
- Martinez JM, Kent JM, Coplan JD, Browne ST, Papp LA, Sullivan GM, Kleber M, Perepletchikova F, Fyer AJ, Klein DF. Respiratory variability in panic disorder. Depression and Anxiety. 2001;14:232–237. doi: 10.1002/da.1072. [DOI] [PubMed] [Google Scholar]
- Martinez JM, Papp LA, Coplan JD, Anderson DE, Mueller CM, Klein DF, Gorman JM. Ambulatory monitoring of respiration in anxiety. Anxiety. 1996;2:296–302. [PubMed] [Google Scholar]
- Mazzara JT, Ayres SM, Grace WJ. Extreme hypocapnia in the critically ill patient. American Journal of Medicine. 1974;56:450–456. doi: 10.1016/0002-9343(74)90475-6. [DOI] [PubMed] [Google Scholar]
- McDonough JT. Stedman’s Concise Medical Dictionary. Williams and Wilkins; Baltimore: 1994. [Google Scholar]
- McFadden ER, Jr, Gilbert IA. Exercise-induced asthma. New England Journal of Medicine. 1994;330:1362–1367. doi: 10.1056/NEJM199405123301907. [DOI] [PubMed] [Google Scholar]
- McFadden ER, Jr, Lyons HA. Arterial-blood gas tension in asthma. New England Journal of Medicine. 1968;278:1027–32. doi: 10.1056/NEJM196805092781901. [DOI] [PubMed] [Google Scholar]
- McNally RJ. Panic Disorder: A Critical Analysis. Guilford Press; New York: 1994. [Google Scholar]
- McNally RJ, Hornig CD, Donnell CD. Clinical versus nonclinical panic: A test of suffocation false alarm theory. Behaviour Research and Therapy. 1995;33:127–131. doi: 10.1016/0005-7967(94)00037-k. [DOI] [PubMed] [Google Scholar]
- Meuret AE. Therapeutic use of ambulatory capnography. In: Gravenstein J, Jaffe M, Paulus D, editors. Capnography, Clinical Aspects. 2. Cambridge: Cambridge University Press; (in press) [Google Scholar]
- Meuret AE. Hyperventilation. In: Weiner I, Craighead E, editors. Corsini’s Encyclopedia of Psychology. 4. Vol. 2. John Wiley and Sons; 2010. [Google Scholar]
- Meuret AE, Ritz T, Wilhelm FH, Roth WT. Voluntary hyperventilation in the treatment of panic disorder--functions of hyperventilation, their implications for breathing training, and recommendations for standardization. Clinical Psychology Review. 2005;25:285–306. doi: 10.1016/j.cpr.2005.01.002. [DOI] [PubMed] [Google Scholar]
- Meuret AE, Ritz T, Wilhelm FH, Roth WT. Targeting pCO(2) in asthma: pilot evaluation of a capnometry-assisted breathing training. Applied Psychophysiology and Biofeedback. 2007;32:99–109. doi: 10.1007/s10484-007-9036-8. [DOI] [PubMed] [Google Scholar]
- Meuret AE, Rosenfield D, Hofmann SG, Suvak MK, Roth WT. Changes in respiration mediate changes in fear of bodily sensations in panic disorder. Journal of Psychiatric Research. 2009;43:634–641. doi: 10.1016/j.jpsychires.2008.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meuret AE, Rosenfield D, Seidel A, Bhaskara L, Hofmann SG. Respiratory and cognitive mediators of treatment change in panic disorder: Evidence for intervention specificity. Journal of Consulting and Clinical Psychology. doi: 10.1037/a0019552. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meuret AE, Wilhelm FH, Ritz T, Roth WT. Breathing training for treating panic disorder. Useful intervention or impediment? Behavior Modification. 2003;27:731–754. doi: 10.1177/0145445503256324. [DOI] [PubMed] [Google Scholar]
- Meuret AE, Wilhelm FH, Ritz T, Roth WT. Feedback of end-tidal pCO2 as a therapeutic approach for panic disorder. Journal of Psychiatric Research. 2008;42:560–568. doi: 10.1016/j.jpsychires.2007.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meuret AE, Wilhelm FH, Roth WT. Respiratory biofeedback-assisted therapy in panic disorder. Behavior Modification. 2001;25:584–605. doi: 10.1177/0145445501254006. [DOI] [PubMed] [Google Scholar]
- Meuret AE, White KS, Ritz T, Roth WT, Hofmann SG, Brown TA. Panic attack symptom dimensions and their relationship to illness characteristics in panic disorder. Journal of Psychiatric Research. 2006;40:520–527. doi: 10.1016/j.jpsychires.2005.09.006. [DOI] [PubMed] [Google Scholar]
- Meuret AE, Rosenfield D, Zhou E, Conrad A, Wilhelm FH, Roth WT. Cardio- respiratory instabilities precede the onset of naturally-occurring panic attacks; Poster presented at the 30th Annual Conference of the Anxiety Disorders Association of America. Baltimore, MA. March 4-7-15.2010. [Google Scholar]
- Munjack DJ, Brown RA, McDowell DE. Existence of hyperventilation in panic disorder with and without agoraphobia, GAD, and normals: Implications for the cognitive theory of panic. Journal of Anxiety Disorders. 1993;7:37–48. [Google Scholar]
- Nardi AE, Valença AM, Nascimento I, Zin WA, Versiani M. Carbon dioxide test in respiratory panic disorder subtype. Canadia Journal of Psychiatry. 2002;47:685–686. doi: 10.1177/070674370204700719. [DOI] [PubMed] [Google Scholar]
- National Heart, Lung, and Blood Institute/National Asthma Education and Prevention Program. Full report 2007. National Institutes of Health; Bethesda, MD: 2007. Expert panel report: Guidelines for the diagnosis and management of asthma. NIH Publication No. 07-4051. [Google Scholar]
- Newhouse MT, Becklake MR, Macklem PT, Mcgregor M. Effect of alterations in end-tidal co2 tension on flow resistance. Journal of Applied Physiology. 1964;19:745–749. doi: 10.1152/jappl.1964.19.4.745. [DOI] [PubMed] [Google Scholar]
- Oakes DF. Clinical practitioner’s pocket guide to respiratory care. 4. Health Educator Publications Inc; Old Town, MN: 1996. [Google Scholar]
- O’Cain CF, Hensley MJ, McFadden ER, Jr, Ingram RH., Jr Pattern and mechanism of airway response to hypocapnia in normal subjects. Journal of Applied Physiology. 1979;47:8–12. doi: 10.1152/jappl.1979.47.1.8. [DOI] [PubMed] [Google Scholar]
- Opat AJ, Cohen MM, Bailey MJ, Abramson MJ. A clinical trial of the buteyko breathing technique in asthma as taught by video. The Journal of Asthma. 2000;37:557–564. doi: 10.3109/02770900009090810. [DOI] [PubMed] [Google Scholar]
- Orehek J, Gayrard P, Grimaud C, Charpin J. Effect of maximal respiratory manoeuvres on bronchial sensitivity of asthmatic patients as compared to normal people. British Medical Journal. 1975;1:123–125. doi: 10.1136/bmj.1.5950.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osborne CA, O’Connor BJ, Lewis A, Kanabar V, Gardner WN. Hyperventilation and asymptomatic chronic asthma. Thorax. 2000;55:1016–1022. doi: 10.1136/thorax.55.12.1016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pain MC, Biddle N, Tiller JW. Panic disorder, the ventilatory response to carbon dioxide and respiratory variables. Psychosom Med. 1988;50:541–8. doi: 10.1097/00006842-198809000-00010. [DOI] [PubMed] [Google Scholar]
- Papp LA, Goetz R, Cole R, Klein DF, Jordan F, Liebowitz MR, Fyer AJ, Hollander E, Gorman JM. Hypersensitivity to carbon dioxide in panic disorder. Am J Psychiatry. 1989 Jun;146(6):779–81. doi: 10.1176/ajp.146.6.779. [DOI] [PubMed] [Google Scholar]
- Papp LA, Martinez JM, Klein DF, Ross D, Liebowitz MR, Fyer AJ, Hollander E, et al. Arterial blood gas changes in panic disorder and lactate-induced panic. Psychiatry Res. 1989;28:171–80. doi: 10.1016/0165-1781(89)90045-0. [DOI] [PubMed] [Google Scholar]
- Papp LA, Klein DF, Gorman JM. Carbon dioxide hypersensitivity, hyperventilation, and panic disorder. American Journal of Psychiatry. 1993;150:1149–1157. doi: 10.1176/ajp.150.8.1149. [DOI] [PubMed] [Google Scholar]
- Papp LA, Martinez JM, Klein DF, Coplan JD, Gorman JM. Rebreathing tests in panic disorder. Biol Psychiatry. 1995 Aug 15;38(4):240–5. doi: 10.1016/0006-3223(94)00296-F. [DOI] [PubMed] [Google Scholar]
- Papp LA, Martinez JM, Klein DF, Coplan JD, Norman RG, Cole R, de Jesus MF, Ross D, Goetz R, Gorman JM. Respiratory psychophysiology of panic disorder: Three respiratory challenges in 98 subjects. American Journal of Psychiatry. 1997;156:667–668. doi: 10.1176/ajp.154.11.1557. [DOI] [PubMed] [Google Scholar]
- Papp LA, Welkowitz LA, Martinez JM, Klein DF, Browne S, Gorman JM. Instructional set does not alter outcome of respiratory challenges in panic disorder. Biological Psychiatry. 1995;38:826–830. doi: 10.1016/0006-3223(95)00047-X. [DOI] [PubMed] [Google Scholar]
- Perna G, Cocchi S, Bertani A, Arancio C, Bellodi L. Sensitivity to 35% CO2 in healthy first-degree relatives of patients with panic disorder. The American Journal of Psychiatry. 1995;152:623–625. doi: 10.1176/ajp.152.4.623. [DOI] [PubMed] [Google Scholar]
- Rassovsky Y, Abrams K, Kushner MG. Suffocation and respiratory responses to carbon dioxide and breath holding challenges in individuals with panic disorder. 2006;60:291–8. doi: 10.1016/j.jpsychores.2005.08.005. [DOI] [PubMed] [Google Scholar]
- Rapee R, Mattick R, Murrell E. Cognitive mediation in the affective component of spontaneous panic attacks. Journal of Behavior Therapy and Experimental Psychiatry. 1986;17:245–53. doi: 10.1016/0005-7916(86)90059-5. [DOI] [PubMed] [Google Scholar]
- Ritz T. Probing the psychophysiology of the airways: physical activity, experienced emotion, and facially expressed emotion. Psychophysiology. 2004;41:809–821. doi: 10.1111/j.1469-8986.2004.00247.x. [DOI] [PubMed] [Google Scholar]
- Ritz T, Ayala ES, Meuret AE. The psychophysiology of the vasovagal syncope and blood phobia treatment: Looking beyond the diphasic response paradigm. International Journal of Psychophysiology. doi: 10.1016/j.ijpsycho.2010.05.007. this issue. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ritz T, Bobb C, Edwards M, Steptoe A. The structure of symptom report in asthma: a reevaluation. Journal of Psychosomatic Research. 2001;51:639–645. doi: 10.1016/s0022-3999(01)00271-9. [DOI] [PubMed] [Google Scholar]
- Ritz T, Dahme B, Wagner C. Effects of static forehead and forearm muscle tension on total respiratory resistance in healthy and asthmatic participants. Psychophysiology. 1998;35:549–562. doi: 10.1017/s0048577298961492. [DOI] [PubMed] [Google Scholar]
- Ritz T, Dahme B, Dubois AB, Folgering H, Fritz GK, Harver A, Kotses H, Lehrer PM, Ring C, Steptoe A, Van de Woestijne KP. Guidelines for mechanical lung function measurements in psychophysiology. Psychophysiology. 2002;39:546–67. doi: 10.1017/S0048577202010715. [DOI] [PubMed] [Google Scholar]
- Ritz T, Dahme B, Roth WT. Behavioral interventions in asthma. Biofeedback techniques. Journal of Psychosomatic Research. 2004;56:711–720. doi: 10.1016/S0022-3999(03)00131-4. [DOI] [PubMed] [Google Scholar]
- Ritz T, Kullowatz A. Effects of stress and emotion on lung function in health and asthma. Current Respiratory Medicine Reviews. 2005;1:209–218. [Google Scholar]
- Ritz T, Kullowatz A, Bobb C, Dahme B, Magnussen H, Kanniess F, Steptoe A. Psychological triggers and hyperventilation symptoms in asthma. Annals of Allergy, Asthma, & Immunology. 2008;100:426–432. doi: 10.1016/S1081-1206(10)60466-8. [DOI] [PubMed] [Google Scholar]
- Ritz T, Meuret AE, Roth WT. Weekly Changes in pCO2 and lung function of asthma patients by paced breathing and capnometry-assisted breathing training in asthma. Applied Psychophysiology and Biofeedback. 2009 doi: 10.1007/s10484-008-9070-1. [DOI] [PubMed] [Google Scholar]
- Ritz T, Rosenfield D, Meuret AE, Bobb C, Steptoe A. Hyperventilation symptoms are linked to a lower perceived health in asthma patients. Annals of Behavioral Medicine. 2008;35:97–104. doi: 10.1007/s12160-007-9014-7. [DOI] [PubMed] [Google Scholar]
- Ritz T, Roth WT. Behavioral interventions in asthma. Breathing training Behavior Modification. 2003;27:710–730. doi: 10.1177/0145445503256323. [DOI] [PubMed] [Google Scholar]
- Ritz T, Wilhelm FH, Gerlach AL, Kullowatz A, Roth WT. End-tidal pCO2 in blood phobics during viewing of emotion- and disease-related films. Psychosomatic Medicine. 2005;67:661–668. doi: 10.1097/01.psy.0000170339.06281.07. [DOI] [PubMed] [Google Scholar]
- Ritz T, Wilhelm FH, Meuret AE, Gerlach AL, Roth WT. Do blood phobia patients hyperventilate during exposure by breathing faster, deeper, or both? Depression and Anxiety. 2009;26:E60–7. doi: 10.1002/da.20466. [DOI] [PubMed] [Google Scholar]
- Rosenfield D, Zhou E, Wilhelm FH, Conrad A, Roth WT, Meuret AE. Change point analysis for longitudinal physiological data: Detection of cardiorespiratory changes preceding panic attacks. Biological Psychology. 2010;84:112–120. doi: 10.1016/j.biopsycho.2010.01.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roth WT. Physiological markers for anxiety: Panic disorder and phobias. International Journal of Psychophysiology. 2005;58:190–8. doi: 10.1016/j.ijpsycho.2005.01.015. [DOI] [PubMed] [Google Scholar]
- Roth WT. Translational research for panic disorder. Am J Psychiatry. 2008;165:796–798. doi: 10.1176/appi.ajp.2008.08040533. [DOI] [PubMed] [Google Scholar]
- Roth WT. Diversity of effective treatments of panic attacks: What do they have in common? Depression and Anxiety. 2010;27:5–11. doi: 10.1002/da.20601. [DOI] [PubMed] [Google Scholar]
- Roth WT, Wilhelm FH, Trabert W. Voluntary breath holding in panic and generalized anxiety disorders. Psychosomatic Medicine. 1998;60:671–679. doi: 10.1097/00006842-199811000-00004. [DOI] [PubMed] [Google Scholar]
- Roth WT, Wilhelm FH, Pettit D. Are current theories of panic falsifiable? Psychological Bulletin. 2005;131:171–192. doi: 10.1037/0033-2909.131.2.171. [DOI] [PubMed] [Google Scholar]
- Roth WT. Diversity of effective treatments of panic attacks: what do they have in common? Depression and Anxiety. 2010;27:5–11. doi: 10.1002/da.20601. [DOI] [PubMed] [Google Scholar]
- Salkovskis PM, Jones DR, Clark DM. Respiratory control in the treatment of panic attacks: Replication and extension with concurrent measurement of behaviour and PCO2. The British Journal of Psychiatry. 1986;148:526–532. doi: 10.1192/bjp.148.5.526. [DOI] [PubMed] [Google Scholar]
- Saisch SG, Wessely S, Gardner WN. Patients with acute hyperventilation presenting to an inner-city emergency department. Chest. 1996;110:952–957. doi: 10.1378/chest.110.4.952. [DOI] [PubMed] [Google Scholar]
- Sanders MH, Kern NB, Costantino JP, Stiller RA, Strollo PJ, Studnicki KA, Coates JA, et al. Accuracy of end-tidal and transcutaneous PCO2 monitoring during sleep. Chest. 1994;106:472–83. doi: 10.1378/chest.106.2.472. [DOI] [PubMed] [Google Scholar]
- Sanderson WC, Rapee RM, Barlow DH. The influence of an illusion of control on panic attacks induced via inhalation of 5.5% carbon dioxide-enriched air. Archives of General Psychiatry. 1989;46:157–62. doi: 10.1001/archpsyc.1989.01810020059010. [DOI] [PubMed] [Google Scholar]
- Sanderson WC, Wetzler S. Five percent carbon dioxide challenge: Valid analogue and maker of panic disorder? Biological Psychiatry. 1990;27:689–701. doi: 10.1016/0006-3223(90)90584-o. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Telch MJ, Jaimez TL. Biological challenge manipulation of PCO2 levels: a test of Klein’s (1993) suffocation alarm theory of panic. Journal of Abnormal Psychology. 1996;105:446–454. doi: 10.1037//0021-843x.105.3.446. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Trakowski JH, Staab JP. Extinction of panicogenic effects of a 35% CO2 challenge in patients with panic disorder. Journal of Abnormal Psychology. 1997;106:630–638. doi: 10.1037//0021-843x.106.4.630. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Woolaway-Bickel K, Trakowski J, Santiago H, Storey J, Koselka M, Cook J. Dismantling cognitive-behavioral treatment for panic disorder: Questioning the utility of breathing retraining. Journal of Consulting and Clinical Psychology. 2000;68:417–424. doi: 10.1037//0022-006x.68.3.417. [DOI] [PubMed] [Google Scholar]
- Seidel A, Rosenfield D, Bhaskara L, Hofmann SG, Meuret AE. Pathways of biobehavioral change in exposure therapy of panic Disorder. Paper presented at the 43nd Annual Convention of Association of Advancement of the Behavior and Cognitive Therapy; New York, NY. November 19–22.2009. [Google Scholar]
- Shioiri T, Someya T, Murashita J, Takahashi S. The symptom structure of panic disorder: a trial using factor and cluster analysis. Acta Psychiatrica Scandinavia. 1996;93:80–86. doi: 10.1111/j.1600-0447.1996.tb09806.x. [DOI] [PubMed] [Google Scholar]
- Smoller JW, Pollack MH, Otto MW, Rosenbaum JF, Kradin RL. Panic anxiety, dyspnea, and respiratory disease. Theoretical and clinical considerations. American Journal of Respiratory and Critical Care Medicine. 1996:6–17. doi: 10.1164/ajrccm.154.1.8680700. [DOI] [PubMed] [Google Scholar]
- Solway J. Hyperpnea-induced bronchoconstriction. In: Barnes PJ, Grunstein MM, Leff AR, Woolcock AJ, editors. Asthma. Lippincott-Raven; Philadelphia, PA: 1997. pp. 1121–1134. [Google Scholar]
- Stalmatski A. Buteyko’s revolutionary treatment. London: Kyle Cathie; 1999. Freedom from asthma. [Google Scholar]
- Stein MB, Millar TW, Larsen DK, Kryger MH. Irregular breathing during sleep in patients with panic disorder. The American Journal of Psychiatry. 1995;152:1168–1173. doi: 10.1176/ajp.152.8.1168. [DOI] [PubMed] [Google Scholar]
- Suzuki R, Freed AN. Heparin inhibits hyperventilation-induced late-phase hyperreactivity in dogs. The American Journal of Respiratory and Critical Care Medicine. 2002;165:27–33. doi: 10.1164/ajrccm.165.1.2010084. [DOI] [PubMed] [Google Scholar]
- Thomas M, McKinley RK, Freeman E, Foy C. Prevalence of dysfunctional breathing in patients treated for asthma in primary care: cross sectional survey. BMJ. 2001;322:1098–1100. doi: 10.1136/bmj.322.7294.1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas M, McKinley RK, Freeman E, Foy C, Price D. The prevalence of dysfunctional breathing in adults in the community with and without asthma. Primary Care Respiratory Journal. 2005;14:78–82. doi: 10.1016/j.pcrj.2004.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van den Elshout FJ, van Herwaarden CL, Folgering HT. Effects of hypercapnia and hypocapnia on respiratory resistance in normal and asthmatic subjects. Thorax. 1991;46:28–32. doi: 10.1136/thx.46.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van den Hout MA, Hoekstra R, Arntz A, Christiaanse M, Ranschaert W, Schouten E. Hyperventilation is not diagnostically specific to panic patients. Psychosomatic Medicine. 1992;53:182–191. doi: 10.1097/00006842-199203000-00005. [DOI] [PubMed] [Google Scholar]
- van Doorn P, Folgering H, Colla P. Control of the end-tidal PCO2 in the hyperventilation syndrome: effects of biofeedback and breathing instructions compared. Bulletin Europeen de Physiopathologie Respiratoire. 1982;18:829–836. [PubMed] [Google Scholar]
- Varray A, Préfaut C. Importance of physical exercise training in asthmatics [see comment] Journal of Asthma. 1992;29:229–234. doi: 10.3109/02770909209048936. [DOI] [PubMed] [Google Scholar]
- Veltman DJ, van Zijderveld GA, van Dyck R, Bakker A. Predictability, controllability, and fear of symptoms of anxiety in epinephrine-induced panic. Biological Psychiatry. 1998;44:1017–1026. doi: 10.1016/s0006-3223(98)00022-5. [DOI] [PubMed] [Google Scholar]
- Vickers K, McNally RJ. Respiratory symptoms and panic in the National Comorbidity Survey: a test of Klein’s suffocation false alarm theory. Behaviour Research and Therapy. 2005;43:1011–1018. doi: 10.1016/j.brat.2004.06.019. [DOI] [PubMed] [Google Scholar]
- Welkowitz LA, Papp L, Martinez J, Browne S, Gorman JM. Instructional set and physiological response to CO2 inhalation. The American Journal of Psychiatry. 1999;156:745–748. doi: 10.1176/ajp.156.5.745. [DOI] [PubMed] [Google Scholar]
- Wientjes CJ. Respiration in psychophysiology: Methods and applications. Biological Psychology. 1992;34:179–203. doi: 10.1016/0301-0511(92)90015-m. [DOI] [PubMed] [Google Scholar]
- Wilhelm FH, Alpers GW, Meuret AE, Roth WT. Respiratory pathophysiology of clinical anxiety outside the laboratory: Assessment of end-tidal pCO2, respiratory pattern variability, and transfer function RSA. In: Fahrenberg J, editor. Progress in Ambulatory Assessment. Hogrefe & Huber; Göttingen: 2001. [Google Scholar]
- Wilhelm FH, Gerlach AL, Roth WT. Slow recovery from voluntary hyperventilation in panic disorder. Psychosomatic Medicine. 2001;63:638–649. doi: 10.1097/00006842-200107000-00017. [DOI] [PubMed] [Google Scholar]
- Wilhelm FH, Trabert W, Roth WT. Characteristics of sighing in panic disorder. Biological Psychiatry. 2001;49:606–614. doi: 10.1016/s0006-3223(00)01014-3. [DOI] [PubMed] [Google Scholar]
- Wilhelm FH, Roth WT. The somatic symptom paradox in DSM-IV anxiety disorders: suggestions for a clinical focus in psychophysiology. Biological Psychology. 2001;57:105–40. doi: 10.1016/s0301-0511(01)00091-6. [DOI] [PubMed] [Google Scholar]
- Woods SW, Charney DS, Loke J, Goodman WK, Redmond DE, Jr, Heninger GR. Carbon dioxide sensitivity in panic anxiety. Ventilatory and anxiogenic response to carbon dioxide in healthy subjects and patients with panic anxiety before and after alprazolam treatment. Archives of General Psychiatry. 1986;43:900–909. doi: 10.1001/archpsyc.1986.01800090090013. [DOI] [PubMed] [Google Scholar]
- Zandbergen J, van Aalst V, de Loof C, Pols H, Griez E. No chronic hyperventilation in panic disorder patients. Psychiatry Research. 1993;47:1–6. doi: 10.1016/0165-1781(93)90050-q. [DOI] [PubMed] [Google Scholar]